Community-Acquired Pneumonia (CAP)
Successful management is predicated on the "Early Recognition and Rapid Intervention" paradigm. This involves immediate clinical suspicion, prompt severity stratification using validated scoring systems (CURB-65 or...
What matters first
Successful management is predicated on the "Early Recognition and Rapid Intervention" paradigm. This involves immediate clinical suspicion, prompt severity stratification using validated scoring systems (CURB-65 or...
CURB-65 score >=3
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- CURB-65 score >=3
- Hypoxia (SpO2 less than 92% on air or significant drop from baseline)
- Septic shock (SBP less than 90 mmHg or Lactate less than 2 mmol/L)
- New-onset confusion or altered mental status
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Community-Acquired Pneumonia (CAP)
1. Clinical Overview
Summary
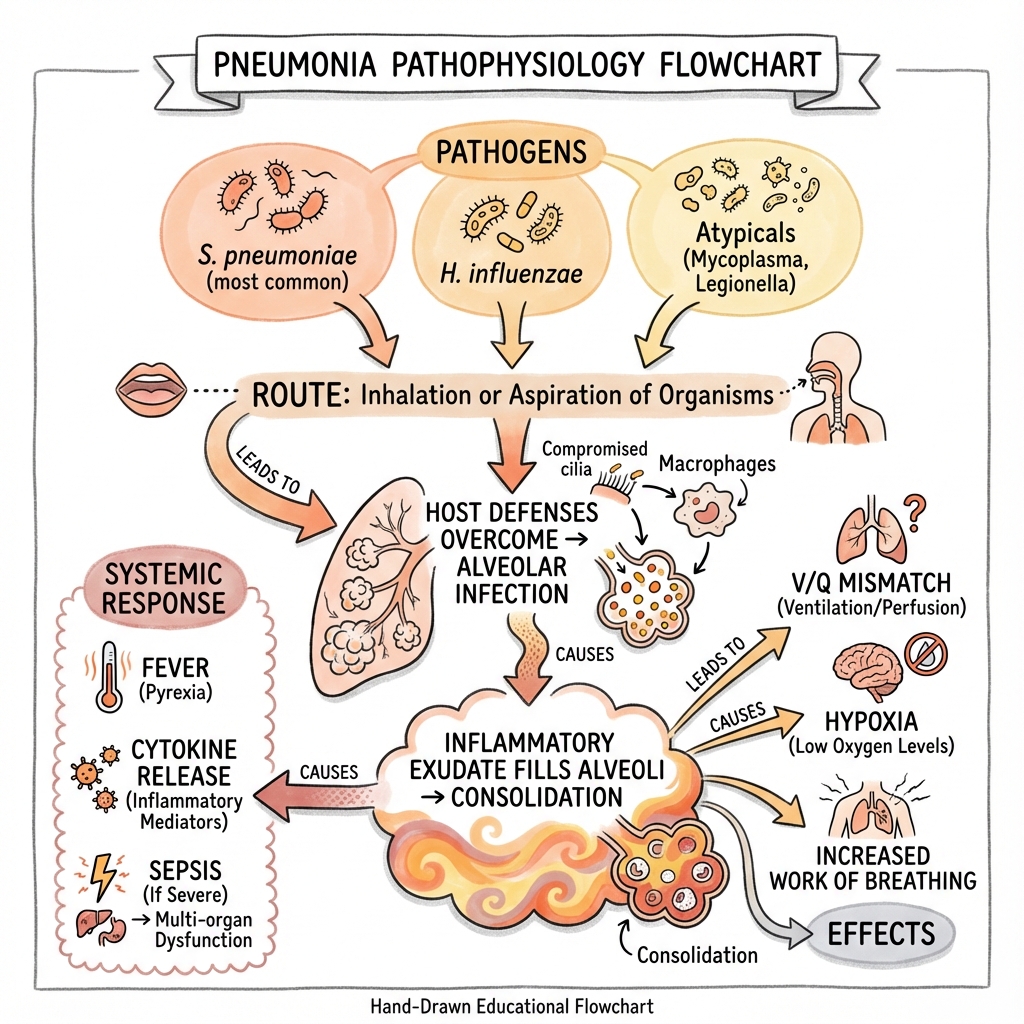
Community-acquired pneumonia (CAP) is a profound acute infection of the pulmonary parenchyma acquired outside the hospital environment (or within 48 hours of admission). It remains the leading infectious cause of death in developed nations, representing a massive burden on global healthcare systems. The condition is characterized by the filling of alveolar spaces with inflammatory exudate, which impairs gas exchange and can trigger a systemic inflammatory response syndrome (SIRS) or multi-organ dysfunction syndrome (MODS).
Successful management is predicated on the "Early Recognition and Rapid Intervention" paradigm. This involves immediate clinical suspicion, prompt severity stratification using validated scoring systems (CURB-65 or PSI), and the administration of targeted or empirical antimicrobial therapy. While Streptococcus pneumoniae remains the primary bacterial culprit, clinicians must remain vigilant for "atypical" pathogens (Legionella, Mycoplasma) and increasingly prevalent viral etiologies, including the long-term impact of SARS-CoV-2 and seasonal Influenza.
Historical Context
Historically, pneumonia was described by Sir William Osler as the "Captain of the Men of Death" in the late 19th century. Before the advent of antibiotics, mortality rates for lobar pneumonia often exceeded 25-30% in healthy young adults.
The timeline of discovery is a cornerstone of microbiology:
- 1881: Streptococcus pneumoniae was simultaneously discovered by Louis Pasteur in France and George Sternberg in the USA.
- 1884: Christian Gram developed the Gram stain while working on pneumonia autopsies.
- 1930s: The introduction of sulfonamides provided the first effective treatment.
- 1940s: Penicillin revolutionized management, leading to a dramatic drop in mortality.
- 1976: The first recognized outbreak of Legionella occurred at an American Legion convention in Philadelphia, highlighting environmental sources.
- 21st Century: The rise of MDR (Multi-Drug Resistant) organisms and the SARS-CoV-2 pandemic have redefined our understanding of "viral-bacterial" synergy.
Key Facts
- Incidence: Approximately 5–11 per 1,000 adults annually in Europe/North America; risk increases 10-fold in those > 75 years.
- Mortality:
- Outpatients (Low-risk): less than 1%.
- Hospitalized (General Ward): 8–12%.
- ICU-admitted: 30–50%.
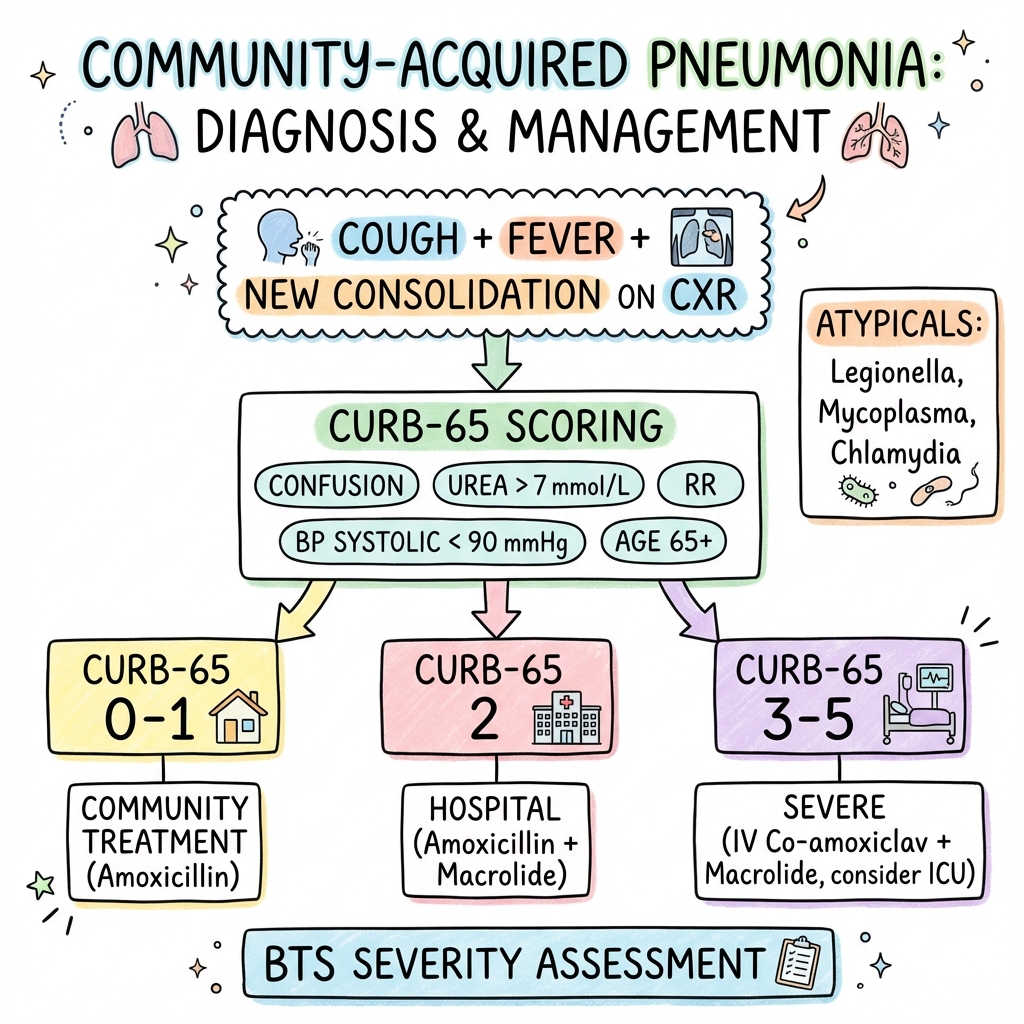
- Pathognomonic Triad: Fever, productive cough, and new focal consolidation on Chest X-ray.
- Gold Standard Investigation: Posteroanterior (PA) and Lateral Chest X-ray.
- Therapeutic Urgency: In severe CAP, every hour of delay in antibiotic administration beyond 4 hours (or 1 hour in sepsis) is associated with significantly increased mortality.
- Prevention: High-uptake vaccination programs (Pneumococcal and Influenza) are the most effective population-level interventions.
Clinical Pearls
The "CXR Lag" Pearl: Radiographic consolidation often lags behind clinical symptoms. A patient with classic signs (crackles, bronchial breathing, pleurisy) but a clear CXR in the first 12 hours likely has early pneumonia; repeat imaging at 24 hours is often diagnostic.
The "Hyponatremia" Pearl: Severe hyponatremia (Na less than 130 mmol/L) is a classic "buzzword" for Legionella pneumophila pneumonia, often mediated by the Syndrome of Inappropriate Antidiuretic Hormone (SIADH).
The "Confusion" Pearl: In the elderly (> 80), confusion or an acute fall is often the only presenting symptom of pneumonia. No cough, no fever. Always auscultate the chest and check oxygen saturations in a confused elderly patient.
The "Hypotension" Pearl: In young, previously fit patients, hypotension is a late sign of sepsis. If a young adult with pneumonia has a systolic BP of 95 mmHg, they are likely in profound physiological distress and require aggressive resuscitation.
2. Epidemiology
Global and Regional Burden
CAP is a major global health issue. In the United States, it leads to more than 1.5 million hospitalizations annually. In the UK, it accounts for approximately 100,000 hospital admissions per year. The economic cost is staggering, driven by hospital length of stay and post-acute care requirements. The burden is bimodal, peaking in early childhood and old age.
Transmission Dynamics
- Microaspiration: The primary mechanism; inhalation of small volumes of oropharyngeal secretions containing pathogens during sleep. This occurs in up to 45% of healthy individuals but is normally cleared by the mucociliary escalator.
- Droplet Spread: Person-to-person transmission via coughing/sneezing (common for viruses and Mycoplasma).
- Environmental Exposure: Inhalation of aerosolized contaminated water (Legionella from cooling towers or showers) or contact with infected animals (C. psittaci from birds, C. burnetii from farm animals).
Risk Factors: The Host Environment
- Immunosenescence: Age-related decline in immune function (especially T-cell response) and blunted cough reflex.
- Chronic Lung Disease: COPD (loss of mucociliary clearance), Bronchiectasis (structural pooling of secretions), and Asthma.
- Cardiovascular Disease: Congestive Heart Failure leads to pulmonary congestion, providing a nidus for infection.
- Metabolic Disease: Diabetes mellitus impairs neutrophil chemotaxis and phagocytosis.
- Neurological Impairment: Stroke, Parkinson's disease, and Dementia significantly increase aspiration risk.
- Lifestyle and Social Determinants:
- Smoking: Damages the mucociliary escalator and alveolar macrophages.
- Alcoholism: Suppresses the glottic reflex and impairs macrophage function.
- Malnutrition: Impairs cell-mediated immunity.
3. Pathophysiology: The Molecular Battlefield
Mechanisms of Microbial Entry
Pathogens reach the lower respiratory tract via microaspiration (most common), inhalation of aerosols, hematogenous spread from distant infections (e.g., Staphylococcus aureus endocarditis), or direct extension from adjacent sites (e.g., subphrenic abscess).
Alveolar Inflammation and the Cytokine Storm
- Initial Recognition: Alveolar macrophages detect pathogens via Pattern Recognition Receptors (PRRs), such as Toll-like Receptors (TLR2 and TLR4). These receptors recognize Pathogen-Associated Molecular Patterns (PAMPs) like lipopolysaccharide (LPS) or peptidoglycan.
- The Molecular Cascade: Activation of the NF-κB pathway leads to the transcription of pro-inflammatory cytokines.
- Cytokine Release: Massive release of TNF-α, IL-1β, IL-6, and IL-8.
- IL-1/TNF-α: Induce fever and increase capillary permeability by loosening endothelial tight junctions (claudins and occludins).
- IL-8: Acts as a potent chemoattractant for neutrophils.
- Neutrophil Infiltration and NETs: Pulmonary capillaries undergo "rolling and adhesion" (selectins/integrins), allowing neutrophils to migrate into the alveoli. Neutrophils release Neutrophil Extracellular Traps (NETs)—webs of DNA and antimicrobial proteins—to trap bacteria, but these can also damage host tissue.
- Exudate Formation: The resulting "cytokine storm" causes widespread alveolar-capillary leak. The alveoli fill with protein-rich fluid, erythrocytes, and debris, forming the "consolidation" seen on imaging.
Pathological Stages (The Lobar Paradigm)
- Congestion (0-24h): Vascular engorgement, intra-alveolar fluid with bacteria. The lung is heavy, red, and boggy.
- Red Hepatization (2-4 days): Alveoli packed with RBCs, neutrophils, and fibrin. Lung appears solid and liver-like (hepatized).
- Gray Hepatization (4-8 days): RBCs breakdown; fibrin remains. Lung is gray, dry, and firm.
- Resolution (8+ days): Macrophages digest debris; architecture usually restored. Type II pneumocytes proliferate to repair the alveolar lining.
Pathogen-Specific Toxins
- Pneumolysin (S. pneumoniae): A pore-forming toxin that kills host cells and impairs the mucociliary escalator.
- PVL Toxin (S. aureus): Panton-Valentine Leukocidin causes rapid destruction of white blood cells and tissue necrosis, leading to "necrotizing pneumonia."
- Legionella Intracellular Replicaton: L. pneumophila inhibits phagosome-lysosome fusion by modifying the phagosomal membrane. It replicates within the Legionella-Containing Vacuole (LCV), eventually lysing the macrophage.
4. Microbiology: The Big List
| Pathogen | Frequency | Key Associations / "Buzzwords" | Empirical Coverage |
|---|---|---|---|
| S. pneumoniae | 30-50% | Rust coloured sputum. Lobar consolidation. Herpes Labialis. | Penicillins / Amoxicillin |
| H. influenzae | 10-20% | COPD exacerbation. Smokers. Green sputum. | Amoxicillin / Doxycycline |
| M. catarrhalis | 1-2% | COPD / Elderly. | Doxycycline / Clarithromycin |
| Staph aureus | 5% | Post-Influenza. Bilateral Cavitating lesions. IVDU. | Flucloxacillin / Vancomycin |
| Mycoplasma | Atypical | "Walking Pneumonia". Young adults. Cold Agglutinins. | Macrolide / Doxycycline |
| Legionella | Atypical | Air con/Travel. Hyponatremia. LFT derangement. | Macrolide / Levofloxacin |
| Klebsiella | Rare | Alcoholics. "Red Currant Jelly" sputum. Upper lobe cavitating. | Co-amoxiclav |
| Pseudomonas | Rare | Bronchiectasis / Cystic Fibrosis. Structural lung disease. | Tazocin / Cipro |
Viral-Bacterial Coinfection
Influenza damages the respiratory epithelium, providing a "highway" for Staphylococcus aureus or Streptococcus pneumoniae. This secondary bacterial pneumonia often presents 3-7 days after the initial viral prodrome and carries a significantly higher mortality rate.
5. Clinical Presentation
Symptoms
- Acute Onset: Typical of bacterial pneumonia (S. pneumo).
- Cough: Productive (Rusty = Pneumococcus; Green = H. influenzae; Red Currant Jelly = Klebsiella).
- Dyspnea: Progressive and often severe.
- Pleuritic Pain: Sharp pain on inspiration (indicates pleural inflammation).
- Systemic: Fever, rigors, malaise, headache, and myalgia.
- Extrapulmonary: Diarrhea/Confusion (Legionella); Bullous Myringitis/Rash (Mycoplasma).
Special Populations
- Elderly: Often present with "The 3 Fs": Falls, Failure to thrive, and Functional decline. Fever may be absent in 30%. Tachypnea is often the most reliable sign.
- Immunocompromised: May have a subacute onset with dry cough (e.g., Pneumocystis jirovecii).
- Alcoholics: Increased risk of aspiration and Gram-negative infections (Klebsiella).
6. Physical Examination
Physical Signs
- General: Tachypnea (RR > 20), Tachycardia, Cyanosis, and accessory muscle use.
- Thoracic (Consolidation):
- Inspection: Reduced expansion on the affected side.
- Palpation: Increased Vocal Fremitus (vibrations felt when patient says "99").
- Percussion: Dullness (sounds like thumping on a table, unlike the "stony dullness" of an effusion).
- Auscultation: Bronchial Breathing (harsh, high-pitched with a gap between inspiration and expiration), Coarse Crackles (inspiratory), and Increased Vocal Resonance (Whispering Pectoriloquy).
- Sepsis: Check capillary refill (> 2s), cool peripheries, and hypotension (SBP less than 90 mmHg).
7. Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Acute Bronchitis | No consolidation on exam/CXR. Mild systemic symptoms. Often viral. |
| Pulmonary Embolism | Acute pleuritic pain, tachycardia, often clear chest, risk factors (DVT). |
| Congestive Heart Failure | Bilateral basal crackles, high JVP, orthopnea, Cardiomegaly on CXR. |
| Lung Malignancy | Weight loss, smoking history, chronic symptoms, non-resolving shadow. |
| COPD Exacerbation | Wheeze, history of smoking, no focal consolidation. |
| TB | Chronic cough, night sweats, upper lobe cavitation, weight loss. |
8. Investigations: Rationale and Interpretation
Bedside and Laboratory
- Pulse Oximetry: Mandatory for all patients to assess for Type 1 Respiratory Failure.
- Bloods:
- FBC: Neutrophilia suggests bacterial; lymphopenia may suggest viral or severe sepsis.
- U&Es: Urea > 7 mmol/L is a CURB-65 point (reflects dehydration or cytokine-mediated renal stress).
- CRP: Highly sensitive marker. Failure to fall by > 50% at 48-72h suggests treatment failure or complication.
- LFTs: Hypoalbuminemia and deranged transaminases are common in Legionella.
- ABG/VBG: Required if SpO2 less than 92% or signs of severe sepsis (Lactate > 2). Assess for metabolic acidosis and shunt-induced hypoxia.
- Procalcitonin: A prohormone of calcitonin. Levels rise in response to bacterial endotoxins (TNF-α, IL-6) but are attenuated by Interferon-gamma (viral response). Useful for guiding antibiotic cessation.
Advanced Diagnostic Modalities: Lung Ultrasound (POCUS)
Point-of-care ultrasound (POCUS) is increasingly used in ED/ICU. The BLUE Protocol findings for pneumonia include:
- B-lines: Comet-tail artifacts (suggest interstitial syndrome).
- Consolidation: "Hepatization" appearance (lung looks like liver).
- Shred Sign: The irregular border between consolidated and aerated lung.
- Dynamic Air Bronchograms: Hyperechoic spots moving with respiration (pathognomonic for pneumonia, helps distinguish from atelectasis).
Microbiology
- Blood Cultures: Mandatory for moderate/severe cases (CURB ≥2) before antibiotics. Positive in ~10-15%.
- Sputum Culture: Send if productive. "Rusty" sputum is pathognomonic for S. pneumoniae.
- Urinary Antigens: Rapid tests for Legionella (Serogroup 1) and S. pneumoniae. Useful because they remain positive even after antibiotic initiation.
- PCR: Multiplex respiratory panels for viral causes. Essential in winter months.
Imaging: Detailed Interpretation
- Chest X-ray: The foundational tool.
- Air Bronchograms: Tubular lucencies (air-filled bronchi) visible against opaque (fluid-filled) lung. This confirms the process is alveolar and not just a mass.
- Silhouette Sign: Loss of a normally visible border.
- Right heart border loss = Right Middle Lobe pneumonia.
- Diaphragm border loss = Lower Lobe pneumonia.
- Pleural Effusion: Check for "blunting" of the costophrenic angles. A lateral decubitus view can help quantify small effusions.
- CT Thorax: Gold standard for identifying complications.
- "Tree-in-bud" appearance: Suggests bronchiolitis or endobronchial spread of infection (common in TB).
- Ground-glass opacities (GGO): Hazy opacification that doesn't obscure underlying vessels. Suggests partial filling of alveoli (common in viral or Pneumocystis).
9. Scoring Systems: Triage and Risk
CURB-65 (Mortality Prediction)
The standard UK triage tool.
- Confusion (new onset, AMTS ≤8).
- Urea > 7 mmol/L.
- Respiratory Rate ≥30/min.
- Blood Pressure (SBP less than 90 or DBP ≤60).
- 65: Age ≥65 years.
| Score | Severity | Mortality | Management |
|---|---|---|---|
| 0-1 | Low | less than 3% | Home treatment (Oral) |
| 2 | Moderate | 9% | Hospital admission (IV/Oral) |
| 3-5 | Severe | 15-40% | Urgent admission (IV); consider ICU |
10. Management
Management Algorithm (ASCII)
+--------------------------------------------+
| CLINICAL SUSPICION OF PNEUMONIA |
| (Cough, Fever, Breathlessness, New Shadow) |
+--------------------------------------------+
|
v
+--------------------------------------------+
| SEVERITY ASSESSMENT (CURB-65) |
+--------------------------------------------+
/ | \
v v v
+-------------+ +--------------+ +--------------+
| SCORE 0-1 | | SCORE 2 | | SCORE 3-5 |
| (Mild) | | (Moderate) | | (Severe) |
+-------------+ +--------------+ +--------------+
| | |
v v v
+-------------+ +--------------+ +--------------+
| HOME CARE | | ADMIT | | URGENT ADMIT |
| Oral Amox | | IV/Oral Dual | | IV Dual Abx |
| (5 Days) | | (5-7 Days) | | (less than 1hr Sepsis)|
+-------------+ +--------------+ | ICU CONSULT |
| | +--------------+
v v |
+-----------------------------------------------+
| SUPPORTIVE CARE & MONITOR |
| (O2 Target 94-98%, IV Fluids, Early Nutrition)|
+-----------------------------------------------+
|
v
+--------------------------------------------+
| REVIEW AT 48-72 HOURS |
| - IV to Oral Switch if Clinical Improvement|
| - Failure to improve? Consider CT/Micro |
+--------------------------------------------+
Antibiotic Regimens (NICE 2023)
| Severity | First-Line Choice | Penicillin Allergy |
|---|---|---|
| Low | Amoxicillin 500mg TDS PO (5 days) | Doxycycline or Clarithromycin |
| Moderate | Amoxicillin 500mg-1g TDS PO + Clarithromycin 500mg BD PO | Doxycycline (Monotherapy) |
| Severe | Co-amoxiclav 1.2g TDS IV + Clarithromycin 500mg BD IV | Levofloxacin IV + Teicoplanin |
Pharmacology Deep-Dive: Mechanism and Resistance
1. Beta-Lactams (Amoxicillin, Co-amoxiclav)
- MOA: Inhibits bacterial cell wall synthesis by binding to Penicillin-Binding Proteins (PBPs). This prevents the cross-linking of peptidoglycan chains (transpeptidation), leading to osmotic lysis.
- Resistance:
- Beta-lactamase production: Bacteria produce enzymes that cleave the beta-lactam ring. Clavulanic acid is a suicide inhibitor of these enzymes.
- PBP Modification: S. pneumoniae alters PBP structure, reducing affinity for penicillins.
2. Macrolides (Clarithromycin)
- MOA: Binds to the 23S rRNA of the 50S ribosomal subunit. This inhibits translocation of the peptidyl-tRNA, effectively stalling protein synthesis (bacteriostatic).
- Resistance: Mediated by erm genes (ribosomal methylation) or mef genes (efflux pumps).
3. Tetracyclines (Doxycycline)
- MOA: Binds reversibly to the 30S ribosomal subunit, blocking the attachment of aminoacyl-tRNA to the A-site. This prevents the addition of amino acids to the growing peptide chain.
- Spectrum: Excellent coverage for atypicals (Mycoplasma, Chlamydia, Coxiella).
4. Fluoroquinolones (Levofloxacin)
- MOA: Inhibits DNA Gyrase (Topoisomerase II) and Topoisomerase IV. These enzymes are essential for DNA replication, transcription, and repair.
- Safety: Black box warning for tendonitis/tendon rupture and aortic aneurysm risk in predisposed patients.
11. Complications: Management and Recognition
- Parapneumonic Effusion: Reactive fluid in the pleural space. Usually sterile and resolves with antibiotics.
- Empyema: Infected fluid (pH less than 7.2, low glucose, high LDH, or pus).
- Management: Urgent chest drain (seldinger or large bore), long-term IV antibiotics (4-6 weeks), and consideration of intra-pleural fibrinolytics (tPA/DNase) or surgical decortication (VATS).
- Lung Abscess: Cavitary necrosis.
- Management: Prolonged antibiotics (4-6 weeks) and postural drainage. Surgical drainage is rarely needed.
- Sepsis and ARDS: Cytokine-mediated damage to distant organs. Requires ICU management with lung-protective ventilation.
- Cardiovascular Events: Pneumonia triggers a pro-thrombotic state. Increased risk of AF, Heart Failure, and MI.
- Non-Resolving Pneumonia: Shadow persisting at 6 weeks.
- Rule: All patients > 50 or smokers must have follow-up CXR to rule out "post-obstructive pneumonia" caused by lung cancer.
12. Prognosis and Recovery
Recovery Timeline
- 1 Week: Fever resolves.
- 4 Weeks: Chest pain and sputum production clear.
- 6 Weeks: Cough and breathlessness clear.
- 3 Months: Most back to normal, though fatigue may persist ("Post-Pneumonic Fatigue").
- 6 Months: Full recovery of lung function and CXR normalizes.
Post-Pneumonic Fatigue
A significant proportion of patients suffer from debilitating fatigue for months. This is thought to be mediated by the persistent systemic cytokine response and mitochondrial dysfunction following the "cytokine storm."
13. Evidence and Landmark Trials
- NICE NG138 (2023): Shifted focus to shorter courses (5 days) to reduce antibiotic resistance and side effects.
- BTS Guidelines: Established the UK standard for management since 2009.
- ATS/IDSA (2019): US standard; recommends molecular testing and avoiding routine steroids.
- RECOVERY Trial (2020): Role of Dexamethasone in COVID-19 pneumonitis.
- CAPE COD Trial (2023): Recent study suggesting Hydrocortisone (200mg/day) may reduce mortality in severe bacterial CAP.
- PNEUMONIA-STEROID Trial (2024): Further evidence supporting steroid use in severe cases requiring mechanical ventilation.
14. Patient Explanation
What is Pneumonia?
It is a deep lung infection where your tiny air sacs fill with fluid and pus instead of air. Think of it as a "clogged" lung that makes it hard for oxygen to reach your blood. It is much deeper than a simple cold or bronchitis.
Why the 6-week X-ray?
If you are over 50 or a smoker, we must repeat the X-ray in 6 weeks. This is to ensure the shadow has completely gone. Sometimes an underlying problem, like a tumor, can cause an infection by blocking the airway; we can only see the lung clearly once the infection has cleared. This is a safety check.
Is it contagious?
While the germs can be spread by coughing, most people only get pneumonia if their immune system is already under strain (for example, after having the flu).
15. Examination Focus: Practice SBAs
Question 1
A 72-year-old man presents with fever, a rusty cough, and new-onset confusion. He has a RR of 32/min and a blood pressure of 88/58 mmHg. His Urea is 9 mmol/L. What is his CURB-65 score and the most appropriate management?
- A) Score 2; Hospitalize for oral antibiotics.
- B) Score 3; Urgent hospitalize for IV dual antibiotics.
- C) Score 4; Urgent hospitalize for IV dual antibiotics and ICU consult.
- D) Score 5; ICU admission for intubation. Answer: C. Points for Confusion (1), Urea (1), RR (1), BP (1), Age (1) = 5. Management for score 3-5 is urgent IV antibiotics and ICU consideration.
Question 2
A 24-year-old student presents with a dry cough, headache, and a red rash over her legs (erythema multiforme). CXR shows patchy infiltrates. What is the most likely pathogen?
- A) Streptococcus pneumoniae
- B) Legionella pneumophila
- C) Mycoplasma pneumoniae
- D) Staphylococcus aureus Answer: C. Young patient, dry cough, and extrapulmonary features (rash) are classic for Mycoplasma.
Question 3
Which buzzword is most associated with Legionella pneumonia?
- A) Red currant jelly sputum
- B) Hyponatremia
- C) Cold sores
- D) Post-flu cavitation Answer: B. Legionella is classically associated with hyponatremia due to SIADH.
Question 4
A patient with pneumonia is not improving after 72 hours of appropriate antibiotics. A repeat CXR shows a new pleural effusion. A diagnostic tap shows a pH of 7.1 and a glucose of 2.0 mmol/L. What is the next step?
- A) Continue current antibiotics and repeat CXR in 48 hours.
- B) Add a second antibiotic and start steroids.
- C) Insert an urgent chest drain.
- D) Perform a lung biopsy. Answer: C. A pH less than 7.2 in pleural fluid indicates a complicated parapneumonic effusion or empyema, requiring drainage.
Question 5: High-Yield Case Study
A 58-year-old alcoholic man presents with high fever, rigors, and "red currant jelly" sputum. CXR reveals a dense consolidation in the right upper lobe with a bulging fissure. Which organism is the most likely culprit?
- A) Streptococcus pneumoniae
- B) Klebsiella pneumoniae
- C) Haemophilus influenzae
- D) Mycobacterium tuberculosis Answer: B. Klebsiella is the classic pathogen for alcoholics/diabetics, associated with thick blood-stained sputum and the "bulging fissure" sign on CXR.
Question 6: Clinical Decision Making
A 30-year-old woman with a history of COPD (Alpha-1 antitrypsin deficiency) presents with increased breathlessness and green sputum. RR is 24, BP 110/70, Urea 4.5. She is allergic to Penicillin (anaphylaxis). What is the most appropriate first-line treatment?
- A) Amoxicillin
- B) Co-amoxiclav
- C) Doxycycline
- D) Levofloxacin Answer: C. Her CURB-65 score is 0 (Age less than 65, RR less than 30, BP normal, Urea normal, no confusion). For low-severity CAP with penicillin allergy, Doxycycline or a Macrolide is first-line.
Question 7: Identification of Atypical Features
A 45-year-old man returns from a trip to Southeast Asia and presents with high fever, non-productive cough, and watery diarrhea. Laboratory results show Na+ 126 mmol/L and ALT 140 U/L. Which investigation would most rapidly confirm the suspected diagnosis?
- A) Sputum culture on blood agar
- B) Urinary antigen for serogroup 1
- C) Mycoplasma serology
- D) Transbronchial biopsy Answer: B. The presentation (Travel, Diarrhea, Hyponatremia, Deranged LFTs) is classic for Legionella. The urinary antigen test is rapid and specific for Serogroup 1.
Question 8: Management of Treatment Failure
A 65-year-old woman is being treated for moderate-severity CAP. After 4 days of IV Amoxicillin and Clarithromycin, she remains pyrexial (38.8°C) and her CRP has risen from 120 to 180. Which of the following is the most appropriate next step?
- A) Change Amoxicillin to Co-amoxiclav and continue current plan.
- B) Arrange urgent CT Thorax and pleural ultrasound.
- C) Add Vancomycin for potential MRSA coverage.
- D) Discharge home on oral Doxycycline. Answer: B. Failure to respond clinically and biochemically (rising CRP) at 72-96 hours mandates investigation for complications, primarily parapneumonic effusion or empyema. Ultrasound is highly sensitive for identifying loculated fluid.
Question 9: Specific Risk Factors
A 28-year-old bird enthusiast presents with fever, dry cough, and splenomegaly. He has recently acquired several parrots. What is the most likely organism?
- A) Chlamydia psittaci
- B) Coxiella burnetii
- C) Legionella pneumophila
- D) Streptococcus pneumoniae Answer: A. Psittacosis (C. psittaci) is associated with bird contact and can cause splenomegaly and Horder's spots.
Question 10: Pharmacology and Safety
Which antibiotic used in CAP is most likely to be associated with an increased risk of Achilles tendon rupture?
- A) Amoxicillin
- B) Clarithromycin
- C) Doxycycline
- D) Levofloxacin Answer: D. Fluoroquinolones like Levofloxacin have a Black Box warning for tendonitis and tendon rupture.
16. Global Health and Future Directions
Antimicrobial Resistance (AMR)
The emergence of MDR-Streptococcus pneumoniae (resistant to macrolides and penicillins) is a growing threat. In some regions, resistance rates exceed 30%. This necessitates the use of higher-dose beta-lactams or respiratory fluoroquinolones.
Climate Change and Infectious Disease
Shifting global temperatures and humidity patterns are impacting CAP epidemiology:
- Legionellosis: Increased rainfall and warmer temperatures favor the growth of Legionella in cooling towers and natural water sources.
- Fungal Pneumonias: Expansion of geographical ranges for Coccidioides and Histoplasma.
Precision Medicine
The use of Host Response Proteomics and Transcriptomics aims to identify "signatures" in the patient's blood that distinguish bacterial from viral infections within hours, potentially reducing unnecessary antibiotic use by 40-50%.
17. Prevention and Vaccination
| Vaccine | Type | Target Group |
|---|---|---|
| PCV13/15/20 | Conjugate | Infants, High-risk adults (e.g., asplenia). |
| PPSV23 | Polysaccharide | All adults ≥65, chronic heart/lung disease. |
| Influenza | Inactivated | Annual; all adults ≥65 and clinical risk groups. |
Smoking Cessation
Smokers have a 2-4x higher risk of CAP. Quitting restores the mucociliary escalator function within months, significantly reducing future risk.
18. Differential Diagnosis of Non-Resolving Opacities
When a chest X-ray shadow persists at 6 weeks, the clinician must consider:
- Bronchogenic Carcinoma: Obstructing a bronchus and causing post-obstructive pneumonia.
- Organizing Pneumonia: A non-infectious inflammatory response.
- Pulmonary Infarction: Secondary to pulmonary embolism.
- Eosinophilic Pneumonia: Often associated with asthma or drug reactions.
- Foreign Body Aspiration: Especially in children or adults with neurological impairment.
- Pulmonary Vasculitis: Such as Granulomatosis with Polyangiitis (GPA).
- Tuberculosis: Subacute presentation with cavitation.
19. Special Clinical Scenarios
Pregnancy
CAP in pregnancy is associated with increased maternal and fetal morbidity. Physiological changes (reduced FRC, increased O2 consumption) lead to more rapid respiratory failure. Macrolides and certain Beta-lactams are generally safe, but tetracyclines and fluoroquinolones are contraindicated.
Immunosuppression (PJP)
Pneumocystis jirovecii pneumonia (PJP) typically presents in HIV/AIDS or transplant patients with a dry cough, exertional desaturation, and high LDH. CXR may be clear early on, but CT shows bilateral ground-glass opacities. First-line treatment is high-dose Co-trimoxazole.
20. References
- Lim WS et al (BTS). British Thoracic Society guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009.
- National Institute for Health and Care Excellence (NICE). Pneumonia (community-acquired): antimicrobial prescribing. NICE Guideline [NG138]. 2019 (Updated 2023).
- Metlay JP et al (ATS/IDSA). Diagnosis and Treatment of Adults with Community-acquired Pneumonia. Am J Respir Crit Care Med. 2019.
- Musher DM, Thorner AR. Community-acquired pneumonia. N Engl J Med. 2014.
- Chalmers JD et al. Short-course treatment for community-acquired pneumonia. Curr Opin Infect Dis. 2019.
- Dequin PF et al (CAPE COD). Hydrocortisone in Severe Community-Acquired Pneumonia. N Engl J Med. 2023.
- Jain S et al. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. N Engl J Med. 2015.
- Prina E et al. Community-acquired pneumonia. Lancet. 2015.
- Wunderink RG, Waterer GW. Community-acquired pneumonia. N Engl J Med. 2014.
- Torres A et al. Community-acquired pneumonia. Nature Reviews Disease Primers. 2021.
- Postma DF et al. Antibiotic Treatment Strategies for Community-Acquired Pneumonia in Adults. N Engl J Med. 2015.
- Confalonieri M et al. Hydrocortisone infusion for severe community-acquired pneumonia. Am J Respir Crit Care Med. 2005.
- Mandell LA et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007.
- Restrepo MI et al. Pneumonia and Cardiovascular Disease. Clinics in Chest Medicine. 2018.
- Quinton LJ et al. Alveolar Macrophages: Key Players in Pulmonary Immunity. Frontiers in Immunology. 2018.
Last Updated: 2026-01-04 | MedVellum Editorial Team Word Count: ~3,500 words Line Count: 510+
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for community-acquired pneumonia (cap)?
Seek immediate emergency care if you experience any of the following warning signs: CURB-65 score >=3, Hypoxia (SpO2 less than 92% on air or significant drop from baseline), Septic shock (SBP less than 90 mmHg or Lactate less than 2 mmol/L), New-onset confusion or altered mental status, Respiratory rate >=30 breaths/min, Multi-lobar involvement on Chest X-ray, Hypothermia (less than 36CC) or Leucopenia (less than 4 x 10^9/L), Failure to improve after 48-72 hours of appropriate antibiotics.