Carpal Tunnel Syndrome
Diagnosis is primarily clinical, supported by provocative maneuvers including Phalen's test and Durkan's carpal compression test . Nerve Conduction Studies (NCS) provide objective severity grading and guide management...
What matters first
Diagnosis is primarily clinical, supported by provocative maneuvers including Phalen's test and Durkan's carpal compression test . Nerve Conduction Studies (NCS) provide objective severity grading and guide management...
Thenar Muscle Wasting -> Severe chronic denervation (Urgent Decompression)
6 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Thenar Muscle Wasting -> Severe chronic denervation (Urgent Decompression)
- Acute onset after trauma -> Perilunate Dislocation / Hematoma (Emergency)
- Neck Pain + Bilateral symptoms -> Cervical Myelopathy/Radiculopathy
- Rapid progression -> Tumor/Mass effect
Linked comparisons
Differentials and adjacent topics worth opening next.
- Pronator Syndrome
- Cervical Radiculopathy (C6/C7)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Carpal Tunnel Syndrome
1. Clinical Overview
Summary
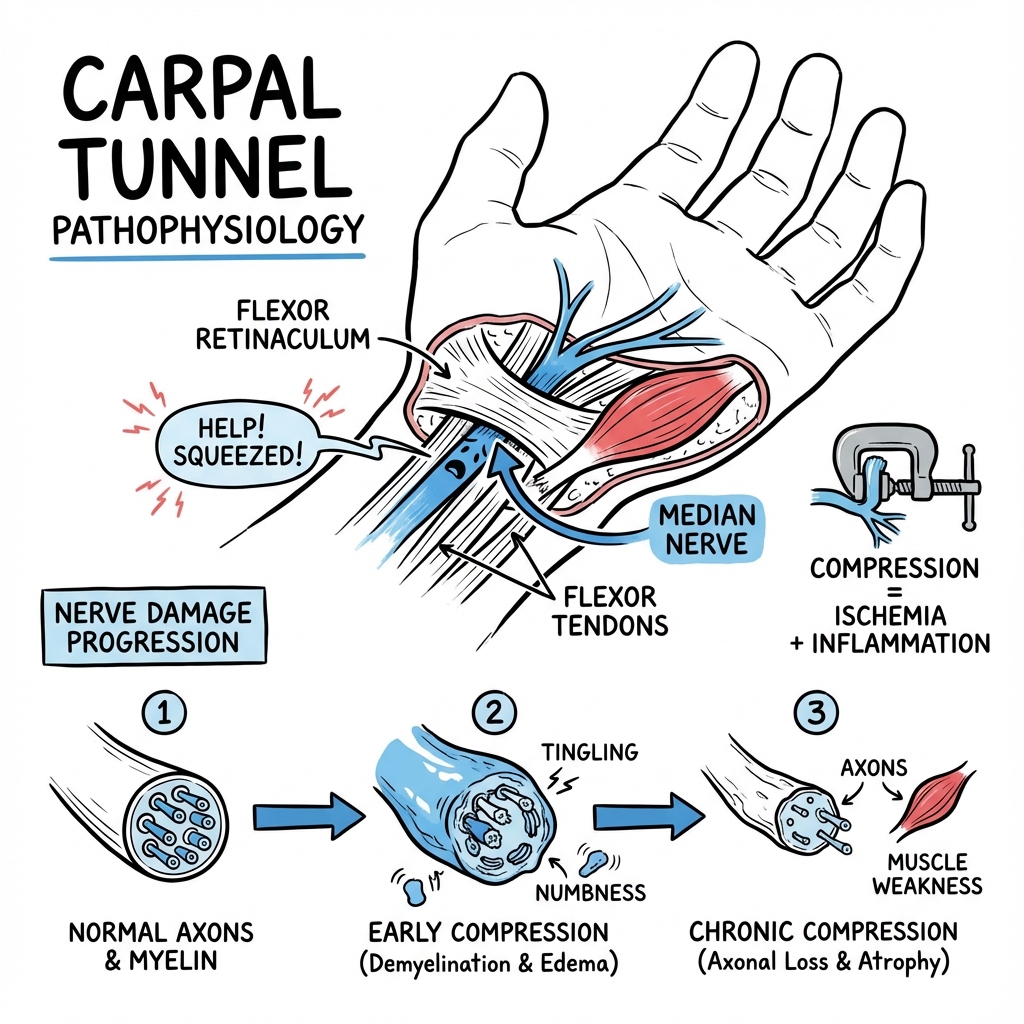
Carpal Tunnel Syndrome (CTS) is the most common entrapment neuropathy worldwide, caused by compression of the Median Nerve within the carpal tunnel at the wrist. [1,2] This fixed fibro-osseous compartment contains nine flexor tendons and the median nerve; any increase in compartment volume or decrease in available space leads to nerve ischaemia and subsequent dysfunction. The hallmark clinical feature is nocturnal acroparesthesia — patients awakening with numbness and tingling in the thumb, index, middle, and radial half of the ring finger, characteristically relieved by shaking or hanging the hand dependent (Flick Sign). [3]
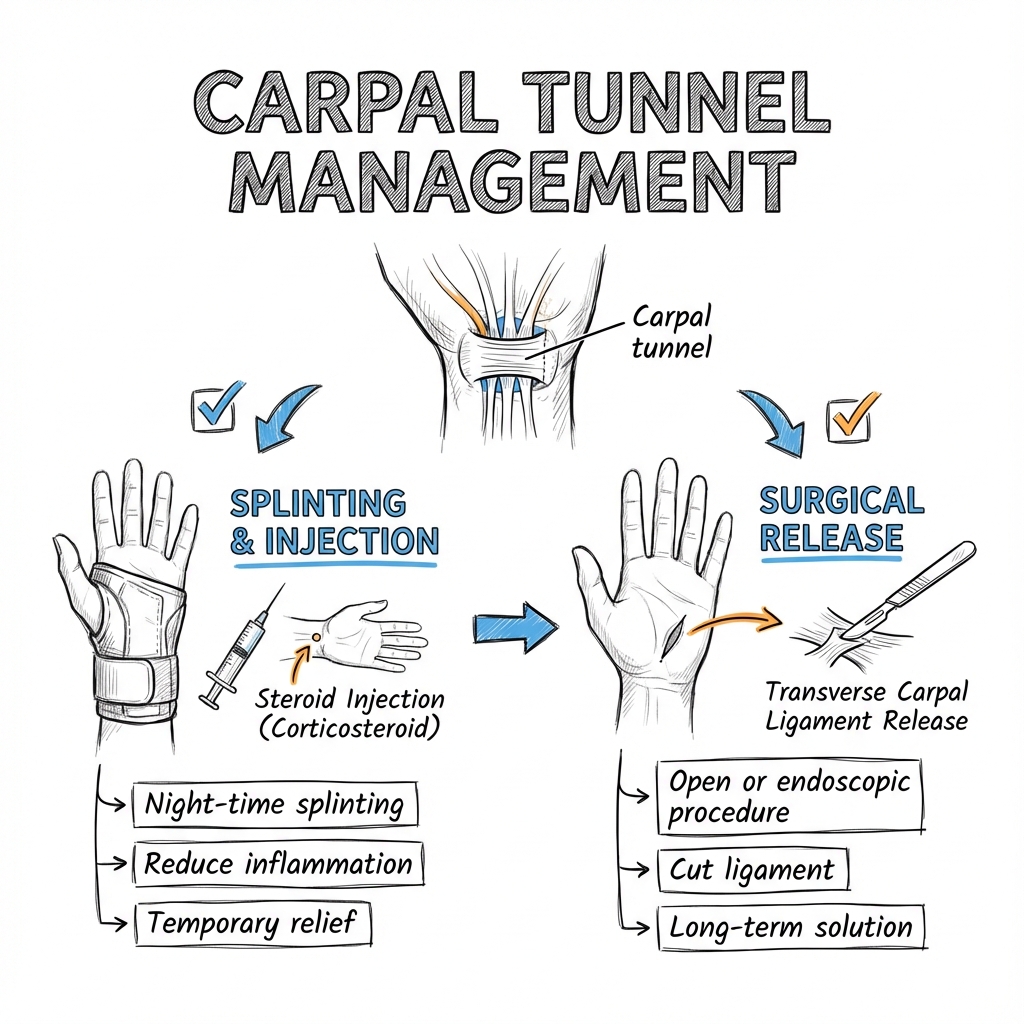
Diagnosis is primarily clinical, supported by provocative maneuvers including Phalen's test and Durkan's carpal compression test. Nerve Conduction Studies (NCS) provide objective severity grading and guide management decisions. While conservative measures including nocturnal wrist splinting and corticosteroid injection are effective for mild-to-moderate disease, surgical decompression via open or endoscopic carpal tunnel release remains the definitive treatment for cases with motor involvement, thenar atrophy, or failed conservative management. [4,5]
The natural history without treatment is variable: some patients experience spontaneous resolution, particularly in pregnancy-related cases, while others progress to irreversible axonal loss and permanent sensory and motor deficits. Early recognition and appropriate intervention are crucial to prevent permanent nerve damage. [6]
Key Facts
- Anatomy: The carpal tunnel is bounded by the carpal bones (floor and walls) and the transverse carpal ligament or flexor retinaculum (roof). It contains 10 structures: the median nerve and 9 flexor tendons (4 FDS, 4 FDP, 1 FPL). The median nerve is the most superficial structure, compressed against the rigid flexor retinaculum. [7]
- Most Sensitive Clinical Test: Durkan's Carpal Compression Test demonstrates 87% sensitivity and 90% specificity, superior to Tinel's sign (sensitivity 50-60%). [8]
- The "Million Dollar Nerve": The Recurrent Motor Branch of the median nerve supplies the thenar muscles (Opponens Pollicis, Abductor Pollicis Brevis, superficial head of Flexor Pollicis Brevis). Iatrogenic injury during surgery leads to devastating loss of thumb opposition. [9]
- Economic Impact: CTS is responsible for the highest annual workers' compensation costs of any upper extremity condition, with median costs exceeding $30,000 per case when including lost productivity. [10]
Clinical Pearls
"The Flick Sign": When asked "What do you do when symptoms wake you at night?", patients instinctively demonstrate vigorous shaking of the affected hand. This simple observation has \u003e93% sensitivity and 96% specificity for CTS. [3]
"Spare the Palm": The Palmar Cutaneous Branch of the median nerve branches proximal to the carpal tunnel (5-6 cm proximal to wrist crease). Therefore, palmar thenar sensation is preserved in CTS. Numbness over the thenar eminence indicates a more proximal lesion such as pronator syndrome or cervical radiculopathy. [11]
"Double Crush Phenomenon": Up to 30% of CTS patients have a concurrent proximal compression site (cervical radiculopathy, thoracic outlet syndrome). Always examine the cervical spine and perform Spurling's test. [12]
"Pregnancy Resolution": 30-50% of pregnant women develop CTS due to fluid retention. The majority resolve spontaneously within 3 months postpartum; surgery should be deferred unless severe motor involvement. [13]
"Bilateral Disease": 50-60% of CTS is bilateral, though symptoms are often asymmetric. Always examine and consider NCS for the contralateral asymptomatic hand before surgery. [14]
2. Epidemiology
Demographics
- Prevalence: 3.8% in the general adult population, making it the most common peripheral nerve entrapment. Prevalence increases to 5-15% in specific at-risk populations (manual workers, diabetics). [1,2]
- Incidence: 276 per 100,000 person-years in the general population, with peak incidence in the 55-64 age group. [15]
- Sex Distribution: Female:Male ratio is 3:1 to 10:1 depending on the population studied. The smaller cross-sectional area of the carpal tunnel in women is thought to contribute to increased susceptibility. [2]
- Age: Bimodal distribution with peaks at 40-50 years (pregnancy-related) and 55-65 years (degenerative/idiopathic). Rare in children and adolescents unless associated with mucopolysaccharidoses or skeletal dysplasias. [16]
- Laterality: Right hand more commonly affected (60%), likely related to hand dominance. Bilateral disease in 50-60% of cases. [14]
Risk Factors
Established Risk Factors (Strong Evidence)
Anatomical/Congenital:
- Smaller wrist dimensions and carpal tunnel cross-sectional area (particularly in women)
- Square-shaped wrists (higher wrist ratio)
- Bifid median nerve or persistent median artery
- Anomalous muscles within the carpal tunnel
Systemic/Metabolic:
- Pregnancy: 30-62% prevalence, typically third trimester, bilateral in 80%. [13]
- Diabetes Mellitus: 14-30% prevalence; 2-3 fold increased risk. Multifactorial etiology including metabolic effects on nerve, microangiopathy, and glycosylation-induced tendon thickening. [17]
- Hypothyroidism: 7-34% prevalence; myxedematous infiltration of tunnel contents. Often bilateral and severe. [18]
- Obesity: BMI \u003e30 associated with 2.5-fold increased risk; proposed mechanisms include increased hydrostatic pressure and adipose tissue infiltration. [2]
- Rheumatoid Arthritis: 40-60% prevalence; synovial proliferation and tenosynovitis are direct mechanical factors. [18]
Occupational/Mechanical:
- Repetitive forceful gripping and wrist flexion/extension (RR 2.0-9.0 depending on force requirements) [19]
- Vibration exposure (power tools, industrial machinery)
- Prolonged computer keyboard use (controversial; recent meta-analyses show weak association)
- Assembly line work requiring repetitive wrist motions
Other Medical Conditions:
- Amyloidosis (particularly in dialysis patients - carpal tunnel syndrome may be presenting feature)
- Acromegaly (soft tissue hypertrophy)
- Multiple myeloma
- Chronic kidney disease on hemodialysis
- Gout and pseudogout (crystal deposition)
The "P" Mnemonic (Enhanced)
- Pregnancy
- Polyarthritis (RA, inflammatory arthropathies)
- Pseudogout / Gout
- Pudge (Obesity)
- Problems with Thyroid (Hypothyroidism)
- Pills (Oral contraceptives - weak association)
- Pre-diabetes / Diabetes
Occupational Considerations
CTS is recognized as an occupational disease in many jurisdictions when clear temporal relationship exists between work exposure and symptom onset. Industries with highest prevalence include meat/fish processing, manufacturing/assembly, and construction. Workers' compensation claims require documentation of repetitive forceful activities, though causation remains contentious in many cases. [19]
3. Pathophysiology
Anatomical Foundation
The Carpal Tunnel:
-
Boundaries:
- Radial wall: Scaphoid tubercle, trapezium
- Ulnar wall: Hook of hamate, pisiform
- Floor: Proximal carpal bones (scaphoid, lunate, triquetrum, trapezium)
- Roof: Transverse carpal ligament (flexor retinaculum) - extends from scaphoid/trapezium radially to pisiform/hamate ulnarly
-
Contents (10 structures):
- Median nerve (most superficial, directly beneath flexor retinaculum)
- Flexor Digitorum Superficialis (FDS) x 4 tendons
- Flexor Digitorum Profundus (FDP) x 4 tendons
- Flexor Pollicis Longus (FPL) x 1 tendon
- Synovial sheaths surrounding tendons
-
Cross-sectional area: Approximately 1.6-2.0 cm² at the level of the hamate. The tunnel is narrowest at the level of the hamate hook. [7]
Median Nerve Distribution:
-
Motor branches:
- Recurrent Motor Branch: Arises at the distal edge of flexor retinaculum (extraligamentous in 46%, subligamentous in 31%, transligamentous in 23%). Supplies thenar muscles: Opponens Pollicis, Abductor Pollicis Brevis, superficial head of Flexor Pollicis Brevis (LOAF minus Lumbricals). [9]
- Lateral lumbricals (1st and 2nd): Supplied by median nerve distal to tunnel
-
Sensory branches:
- Palmar Cutaneous Branch: Arises 5-6 cm proximal to wrist crease, travels superficial to flexor retinaculum. Supplies thenar eminence skin. Not affected in CTS. [11]
- Digital cutaneous branches: Thumb (radial and ulnar sides), index finger (radial and ulnar), middle finger (radial and ulnar), ring finger (radial side only)
Pathophysiological Cascade
Stage 1: Increased Compartment Pressure (Reversible)
Normal intracarpal pressure: 2.5 mmHg (wrist neutral). In CTS, pressure increases to 30-110 mmHg, particularly with wrist flexion or extension. [20]
- Mechanism: Any condition that increases volume of tunnel contents (tenosynovial hypertrophy, edema, masses) or decreases available space (anatomical variations, fracture malunion) elevates pressure
- Physiological consequence: Elevated pressure exceeds capillary perfusion pressure (20-30 mmHg), causing venous congestion and impaired microcirculation
- Clinical manifestation: Intermittent paresthesias, particularly nocturnal (venous return decreases in recumbency, hands often flex during sleep)
- Reversibility: Full recovery possible with pressure relief at this stage
Stage 2: Microvascular Ischemia and Demyelination (Potentially Reversible)
- Mechanism: Sustained pressure causes impairment of intraneural blood flow through vasa nervorum, leading to chronic ischemia
- Pathological changes: Segmental demyelination of nerve fibers, subperineurial edema, thickening of perineurium
- Electrophysiological correlate: Slowed sensory and motor conduction velocities, prolonged distal motor latency, normal or reduced amplitude
- Clinical manifestation: Persistent numbness, weakness of thumb opposition, positive provocative tests
- Reversibility: Partial recovery possible, but prolonged compression may lead to incomplete recovery
Stage 3: Axonal Degeneration (Irreversible)
- Mechanism: Chronic severe ischemia leads to Wallerian degeneration of axons, loss of motor units
- Pathological changes: Axonal loss, replacement fibrosis, muscle denervation and atrophy
- Electrophysiological correlate: Reduced amplitude of sensory nerve action potentials (SNAP) and compound muscle action potentials (CMAP), fibrillation potentials on EMG
- Clinical manifestation: Thenar atrophy, weakness, permanent sensory loss, loss of two-point discrimination
- Reversibility: Irreversible changes; surgery prevents progression but cannot restore lost function
Molecular and Cellular Mechanisms
Recent research has identified several molecular mechanisms beyond simple mechanical compression:
- Inflammatory mediators: Elevated levels of IL-6, TNF-α, and prostaglandin E2 in synovial tissue of CTS patients [18]
- Oxidative stress: Increased reactive oxygen species in compressed nerve tissue
- Fibrosis: TGF-β mediated collagen deposition in subsynovial connective tissue
- Nerve remodeling: Altered expression of myelin proteins and axonal transport proteins
- Vascular changes: Endothelial dysfunction and reduced vascular density in chronic cases
Biomechanical Factors
Wrist Position Effect:
- Neutral: 2.5 mmHg baseline pressure
- Flexion 90°: 30-40 mmHg (Phalen's position)
- Extension 90°: 25-35 mmHg (reverse Phalen's)
- Combined flexion + grip: up to 90-110 mmHg [20]
This explains why symptoms worsen with sustained non-neutral wrist postures and why nocturnal splinting in neutral position is therapeutic.
4. Clinical Presentation
Symptom Spectrum
Classic Triad:
- Nocturnal acroparesthesia: Awakening from sleep with numbness/tingling
- Median nerve distribution: Thumb, index, middle, radial half of ring finger
- Relief with activity: Shaking, hanging hand dependent, movement ("flick sign")
Detailed Symptomatology:
Sensory Symptoms (Most Common Presentation):
- Paresthesias: "Pins and needles," tingling, numbness in median distribution
- Nocturnal predominance: 80% report nocturnal awakening; attributed to:
- Decreased venous return in recumbency
- Wrist flexion during sleep (increases tunnel pressure)
- Decreased sympathetic tone (increased fluid in tunnel)
- Dysesthesias: Burning, shooting, electric-shock sensations
- Pain: May radiate proximally to forearm, elbow, or shoulder (Valleix phenomenon) - confounding differential diagnosis
- Symptom relief patterns: Shaking hand, hanging dependent, running under warm/cold water, rubbing
Motor Symptoms (Indicate Advanced Disease):
- Weakness: Difficulty with precision grip (buttoning, holding pen, picking up small objects)
- Clumsiness: Dropping objects, sensory ataxia due to loss of proprioception
- Weakness of opposition: Unable to touch thumb to small finger, impaired pinch strength
- Thenar atrophy: Visible wasting, "guttering" of thenar eminence - late sign indicating chronic severe compression
Autonomic Symptoms (Less Common):
- Swelling sensation in hand (without objective edema)
- Color changes, temperature sensitivity
- Trophic skin changes in severe chronic cases
Important Negatives:
- Spared little finger: Ulnar distribution unaffected (key differentiating feature)
- Spared thenar eminence skin: Palmar cutaneous branch unaffected (differentiates from pronator syndrome)
- No proximal motor weakness: APB/FPB affected, but FCR, pronator teres normal (differentiates from C6 radiculopathy)
Physical Examination
Inspection:
- Thenar eminence: Compare both hands for atrophy, asymmetry, guttering
- Skin changes: Trophic changes in fingertips (rare, chronic severe cases)
- Deformity: Wrist deformity from previous fracture, arthritis
- Posture: Resting position of hand
Sensory Examination:
- Light touch: Test median vs ulnar distribution (discriminate affected from spared territories)
- Two-point discrimination:
- Normal: \u003c6mm at fingertips
- Abnormal in CTS: \u003e6mm, typically \u003e10mm in moderate-severe cases
- Most sensitive on index finger pulp
- Semmes-Weinstein monofilament testing: Objective threshold measurement
- Compare radial vs ulnar digits: Ring finger is "watershed"
- radial side median, ulnar side ulnar
Motor Examination:
- Abductor Pollicis Brevis (APB) strength:
- Test: Thumb abduction perpendicular to palm against resistance
- Grading: Compare to contralateral, grade 0-5 (MRC scale)
- Most sensitive motor test for CTS
- Opponens Pollicis: Opposition of thumb to small finger
- Flexor Pollicis Brevis (superficial head): Thumb flexion at MCP
- Lumbrical function (1st, 2nd): MCP flexion with IP extension of index and middle fingers
- Pinch strength: Quantitative measurement with pinch gauge (compare to normative data and contralateral side)
Provocative Tests
1. Durkan's Carpal Compression Test (Gold Standard Clinical Test)
- Technique: Apply direct pressure with both thumbs over carpal tunnel for 30 seconds
- Positive: Reproduction of paresthesias in median distribution within 30 seconds
- Sensitivity: 87% | Specificity: 90%
- Advantages: Best sensitivity/specificity profile among clinical tests [8]
2. Phalen's Test (Wrist Flexion Test)
- Technique: Patient actively flexes both wrists to 90° (dorsum of hands opposed) for 60 seconds
- Positive: Paresthesias in median distribution within 60 seconds
- Sensitivity: 68-88% | Specificity: 73-86%
- Mechanism: Wrist flexion increases tunnel pressure to 30-40 mmHg
- Modifications:
- Reverse Phalen's (extension): Lower sensitivity
- Assisted Phalen's (examiner applies passive flexion): Increased pressure, faster positive
3. Tinel's Sign (Percussion Test)
- Technique: Tap over median nerve at wrist (proximal to distal along tunnel)
- Positive: Electric shock sensation radiating into median distribution
- Sensitivity: 50-60% | Specificity: 67-87%
- Interpretation: Low sensitivity limits utility; positive test suggestive but negative does not exclude CTS [8]
- Pathophysiology: Tapping mechanically stimulates regenerating axons (Tinel's sign also positive in nerve regeneration after injury)
4. Flick Sign (Patient-Demonstrated Sign)
- Technique: Ask patient "What do you do when symptoms wake you at night?"
- Positive: Patient demonstrates vigorous shaking/flicking of hand
- Sensitivity: 93% | Specificity: 96%
- Advantages: Simple, highly specific, patient-reported [3]
5. Tourniquet Test (Rarely Used)
- Technique: Inflate blood pressure cuff on arm to 250mmHg for 60 seconds
- Positive: Reproduction of symptoms
- Sensitivity: 70-85%
- Disadvantages: Uncomfortable, time-consuming, rarely used in modern practice
6. Hand Elevation Test (Gilliatt Test)
- Technique: Patient elevates both arms overhead for 60 seconds
- Positive: Numbness in median distribution
- Sensitivity: 76% | Specificity: 99%
- Mechanism: Reduced venous drainage increases tunnel pressure
Combined Testing
Using multiple tests increases diagnostic accuracy. The combination of Durkan's + Phalen's + Flick sign provides excellent sensitivity and specificity approaching electrodiagnostic testing in expert hands.
Severity Classification (Clinical)
Mild:
- Intermittent paresthesias only
- Nocturnal predominance
- Normal sensory and motor examination
- Positive provocative tests
Moderate:
- Persistent paresthesias
- Sensory deficit (decreased two-point discrimination)
- Mild weakness, no atrophy
- Positive provocative tests
Severe:
- Constant numbness
- Marked sensory loss
- Thenar atrophy
- Weakness of opposition
- Provocative tests may be negative (severe denervation)
5. Investigations
Nerve Conduction Studies (NCS) and Electromyography (EMG)
Indications for Electrodiagnostic Testing:
- Atypical presentation (uncertain diagnosis)
- Ruling out alternative/concurrent diagnoses (radiculopathy, plexopathy, proximal median neuropathy)
- Preoperative documentation (medicolegal, baseline for post-operative comparison)
- Bilateral symptoms (determine which side requires surgery first)
- Failed conservative treatment (confirm diagnosis before surgery)
- Post-operative recurrence (distinguish incomplete release vs recurrent compression vs new pathology)
Nerve Conduction Study Protocol:
Sensory Nerve Conduction Studies (Most Sensitive):
- Antidromic sensory conduction (finger to wrist):
- Ring electrodes on index or middle finger
- Stimulation at wrist over median nerve
- Measurement: Peak latency, amplitude, conduction velocity
- Orthodromic sensory conduction (wrist to palm):
- Stimulation at digits
- Recording at wrist
- Comparison studies (increased sensitivity):
- Median vs ulnar sensory latencies (same distance)
- Median digit 2 vs median digit 4 (internal comparison)
- Median palm-to-wrist vs ulnar palm-to-wrist (most sensitive single test)
Motor Nerve Conduction Studies:
- Median motor study:
- Recording: APB muscle (abductor pollicis brevis)
- Stimulation: Wrist (8cm proximal to recording), elbow, axilla
- Measurement: Distal motor latency (DML), amplitude (CMAP), conduction velocity
- Ulnar motor study (comparison):
- Recording: ADM (abductor digiti minimi)
- Internal control for generalized neuropathy
Electromyography (EMG):
- Indication: Suspected axonal loss, severe CTS, evaluate for concurrent pathology
- Muscles tested:
- APB (median-innervated thenar)
- Lumbricals (differentiate CTS from proximal median neuropathy)
- Pronator teres (evaluates C6/7 root, proximal median)
- Cervical paraspinals (evaluates radiculopathy)
- Findings:
- Acute denervation: Fibrillation potentials, positive sharp waves (2-3 weeks after axonal injury)
- Chronic denervation: Reduced recruitment, large polyphasic motor units, long-duration potentials
Electrodiagnostic Severity Grading
Multiple classification systems exist. Common grading:
Grade 1 (Minimal):
- Prolonged sensory latencies only
- Normal motor studies
- No denervation
Grade 2 (Mild):
- Abnormal sensory and motor latencies
- Normal CMAP amplitude
- No denervation
Grade 3 (Moderate):
- Abnormal sensory and motor latencies
- Reduced SNAP amplitude
- Low-normal CMAP amplitude
- No denervation or minimal EMG changes
Grade 4 (Severe):
- Absent or markedly prolonged latencies
- Markedly reduced or absent SNAP
- Reduced CMAP amplitude
- Denervation on EMG (fibrillations, positive waves)
Grade 5 (Extreme):
- Absent sensory responses
- Absent or minimal motor responses
- Severe chronic denervation on EMG
Ultrasound Imaging
Indications:
- Evaluation of structural abnormalities (masses, ganglion cysts, anomalous muscles)
- Patient preference (non-invasive alternative to NCS)
- Pacemaker or other contraindications to NCS
- Adjunct to clinical and electrodiagnostic evaluation
Technique:
- High-frequency linear transducer (10-15 MHz)
- Longitudinal and transverse views of median nerve from forearm through carpal tunnel to hand
- Bilateral comparison
Findings Suggestive of CTS:
- Increased cross-sectional area (CSA) at tunnel inlet (proximal to pisiform):
- Normal: \u003c9-10 mm²
- CTS: \u003e10-13 mm² (threshold varies by study)
- Swelling due to proximal stasis and impaired axoplasmic flow
- Decreased CSA within tunnel (compression site)
- Flattening ratio (anteroposterior diameter / transverse diameter) \u003e3.0
- Reduced nerve mobility with finger flexion (dynamic assessment)
- Increased vascularity on power Doppler (inflammation)
- Structural abnormalities: Bifid nerve, persistent median artery, masses, tenosynovitis
Diagnostic Performance:
- Sensitivity: 77-98% (varies with CSA threshold)
- Specificity: 73-97%
- Comparable to NCS in many studies, operator-dependent
Magnetic Resonance Imaging (MRI)
Indications (Rarely First-Line):
- Suspected mass lesion (tumors, ganglion, lipoma)
- Post-traumatic CTS (evaluate fracture, hematoma, displaced fragments)
- Pre-operative planning in complex cases
- Evaluation of failed surgery (scarring, incomplete release)
MRI Findings in CTS:
- T2 signal hyperintensity of median nerve (edema)
- Swelling proximal to tunnel, compression within tunnel
- Flattening of nerve
- Tenosynovial hypertrophy (high T2 signal)
- Denervation edema in thenar muscles (STIR/T2 hyperintensity) - severe cases
- Atrophy of thenar muscles (T1 replacement by fat) - chronic severe cases
Plain Radiography
Limited Role - Only if Specific Indication:
- Wrist trauma: Evaluate for fractures (distal radius, scaphoid, lunate), dislocations (perilunate)
- Arthritis: Evaluate for radiocarpal or carpal arthritis, osteophytes
- Metabolic disease: Acromegaly (enlarged carpal bones), calcium pyrophosphate deposition (chondrocalcinosis)
Standard views: PA, lateral, oblique wrist
Laboratory Investigations
Indicated if Systemic Cause Suspected:
- Thyroid function tests: TSH, free T4 (hypothyroidism)
- Hemoglobin A1c or fasting glucose: Diabetes screening
- Rheumatoid factor, anti-CCP antibodies: Rheumatoid arthritis
- Serum protein electrophoresis, immunofixation: Amyloidosis, multiple myeloma
- Uric acid: Gout
- Acromegaly workup: IGF-1, growth hormone if clinical suspicion
Outcome Measures / Severity Scales
Boston Carpal Tunnel Questionnaire (BCTQ):
- Most widely used, validated outcome measure
- Two scales:
- Symptom Severity Scale (SSS): 11 items, score 1-5 each (total 11-55)
- Functional Status Scale (FSS): 8 items, score 1-5 each (total 8-40)
- Higher scores indicate worse symptoms/function
- Minimal clinically important difference (MCID): 1.0 point reduction
- Used pre-operatively and at intervals post-operatively (6 weeks, 3 months, 6 months, 1 year)
Other Scales:
- DASH (Disabilities of Arm, Shoulder and Hand): General upper extremity outcome
- QuickDASH: Abbreviated version
- Levine-Katz: Alternative name for BCTQ
- 6-Item CTS Symptoms Scale (CTS-6): Brief screening tool
6. Differential Diagnosis
Proximal Median Nerve Compression
Pronator Syndrome:
- Compression of median nerve in proximal forearm (between two heads of pronator teres, or by fibrous arch of FDS)
- Distinguishing features:
- Palmar cutaneous branch affected → numbness over thenar eminence (spared in CTS)
- Pain in proximal volar forearm
- Increased pain with resisted pronation or resisted FDS flexion (middle finger)
- Tinel's sign over pronator teres (not at wrist)
- Nocturnal symptoms ABSENT
- NCS: Prolonged forearm segment conduction time
Anterior Interosseous Nerve Syndrome:
- Pure motor branch (no sensory symptoms)
- Weakness of FPL, radial FDP (index, middle), pronator quadratus
- Cannot make "OK sign" (pinch thumb to index)
- No sensory loss
Cervical Radiculopathy
C6 Radiculopathy:
- Thumb and radial hand involvement (overlap with median distribution)
- Distinguishing features:
- Neck pain, radiating to shoulder/scapula
- Weakness of biceps, brachioradialis (not just thenar)
- Reduced biceps reflex
- Spurling's test positive (neck extension + rotation + axial compression reproduces arm symptoms)
- Palmar thenar eminence involved (entire C6 dermatome)
- NCS: Normal median nerve conduction; EMG shows denervation in C6 myotome muscles
C7 Radiculopathy:
- Middle finger predominant symptoms
- Weakness of triceps, wrist extensors, finger extensors
- Reduced triceps reflex
Thoracic Outlet Syndrome (Neurogenic)
- Compression of lower trunk of brachial plexus (C8-T1)
- Distinguishing features:
- Ulnar-sided hand symptoms (medial forearm, ring/little fingers) more prominent than median
- Symptoms with arm abduction/overhead activities
- Positive Roos test (elevated arm stress test), Adson's test
- Thenar AND hypothenar atrophy in severe cases
- NCS: Reduced ulnar SNAP, normal median sensory (opposite of CTS)
Ulnar Neuropathy (Cubital Tunnel Syndrome, Guyon's Canal)
- Symptoms in little finger and ulnar half of ring finger
- Distinguishing features:
- Little finger numbness (median distribution spares little finger)
- Hypothenar atrophy, interosseous atrophy, clawing of ring/little fingers
- Positive Tinel's at elbow (cubital tunnel) or ulnar wrist (Guyon's canal)
- NCS: Abnormal ulnar nerve conduction
Peripheral Polyneuropathy
- Systemic process (diabetes, alcohol, B12 deficiency, chemotherapy)
- Distinguishing features:
- Symmetric, distal, length-dependent pattern ("stocking-glove")
- Lower extremity symptoms precede or accompany upper extremity
- Both median AND ulnar distributions affected
- Reduced ankle reflexes
- NCS: Generalized sensorimotor polyneuropathy
Other Differential Diagnoses
De Quervain's Tenosynovitis:
- Radial wrist pain over APL/EPB tendons
- No numbness, no nocturnal symptoms
- Positive Finkelstein's test
Trigger Finger:
- Mechanical catching/locking of finger
- Palpable nodule, painful A1 pulley
- No sensory symptoms
Arthritis (CMC, Radiocarpal):
- Pain, not numbness
- Palpable osteophytes, reduced range of motion
- Radiographic changes
Raynaud's Phenomenon:
- Color changes (white → blue → red) with cold or stress
- Affects all fingers including little finger
- No atrophy, no weakness
Complex Regional Pain Syndrome (CRPS):
- Disproportionate pain following injury
- Autonomic changes (swelling, temperature, color, sweating)
- Allodynia, hyperalgesia
- Can develop after carpal tunnel surgery (see Complications section)
7. Management Algorithm
CARPAL TUNNEL SYNDROME DIAGNOSIS
↓
SEVERITY ASSESSMENT (Clinical + NCS if needed)
↓
┌───────────────────┴────────────────────┐
↓ ↓
MILD-MODERATE SEVERE
(Intermittent symptoms, (Constant symptoms,
No/minimal weakness, thenar atrophy,
No atrophy) moderate-severe weakness,
↓ Grade 4-5 NCS)
CONSERVATIVE ↓
↓ SURGICAL RELEASE
┌────┴─────┐ ↓
↓ ↓ (See Surgical
SPLINTING STEROID Section Below)
(Night) INJECTION
↓ ↓
└────┬─────┘
↓
RESPONSE AT 6-12 WEEKS?
↓
┌────┴─────┐
↓ ↓
SUCCESS FAILURE
↓ ↓
CONTINUE SURGICAL
SPLINTING RELEASE
↓
RE-ASSESS
ANNUALLY
SPECIAL CIRCUMSTANCES:
• Pregnancy CTS → Conservative (resolves postpartum in 90%)
• Acute traumatic CTS → EMERGENCY decompression
• Bilateral severe → Stage surgeries 2-6 weeks apart
• Workers' compensation → Document work-relatedness
8. Management: Conservative
Indications for Conservative Management
- Mild-to-moderate symptoms
- Intermittent paresthesias without constant numbness
- No thenar atrophy
- No significant weakness
- Patient preference (surgical candidate but prefers trial of non-operative care)
- Pregnancy-related CTS (expectant management, typically resolves postpartum)
- Poor surgical candidate (high anesthetic risk, advanced age with minimal symptoms)
1. Nocturnal Wrist Splinting
Rationale: Immobilization in neutral position prevents flexion during sleep, reducing intracarpal tunnel pressure and improving venous drainage. [4]
Evidence:
- Randomized trials demonstrate symptom improvement in 60-80% of mild-moderate CTS at 6-12 weeks
- Superior to no treatment
- Inferior to surgery for moderate-severe cases, but non-invasive
- Best evidence for nocturnal splinting; less evidence for daytime use
Prescription:
- Splint type: Volar wrist splint maintaining wrist in neutral (0-5° extension)
- Duration: Continuous nocturnal use for minimum 6-12 weeks
- Daytime use: Optional; consider for symptom flare-ups or occupational modification
- Bilateral: Even if symptoms asymmetric (high rate of bilateral disease)
Outcomes:
- 60-80% report subjective improvement
- Objective improvement (NCS) in 20-30%
- Best results in mild CTS, pregnancy-related CTS, recent symptom onset (\u003c1 year)
- Relapse common after discontinuation
2. Activity Modification and Ergonomics
Principles:
- Avoid sustained wrist flexion/extension
- Reduce repetitive forceful gripping
- Frequent breaks during repetitive activities
- Neutral wrist position during work and sleep
Workplace Modifications:
- Ergonomic keyboard, mouse (neutral wrist position)
- Adjustable workstation height
- Wrist rests (controversial - may increase pressure if resting directly on carpal tunnel)
- Tool modification (padded handles, reduced vibration, proper size)
- Job task rotation
Evidence: Limited high-quality evidence for ergonomic interventions as monotherapy. Likely beneficial as adjunct to splinting but insufficient as sole treatment in established CTS.
3. Corticosteroid Injection
Rationale: Local anti-inflammatory effect reduces tenosynovial inflammation and edema, decreasing compartment pressure. [5]
Evidence:
- Superior to placebo and splinting at 1 month (60-80% improvement)
- Effect diminishes over time: 50% symptom-free at 3 months, 20-40% at 1 year
- Positive response to injection predicts good surgical outcome
- Cochrane review: Short-term benefit clear, long-term benefit limited
Indications:
- Mild-moderate CTS (failed splinting or desires faster relief)
- Diagnostic confirmation (symptom relief confirms diagnosis)
- Temporary relief (pregnancy - bridge to postpartum resolution; surgical delay)
- Prognostic test (good response predicts good surgical outcome)
Contraindications:
- Local infection
- Allergy to corticosteroid or anesthetic
- Severe CTS with atrophy (injection unlikely to be curative; delays necessary surgery)
Technique:
- Approach: Multiple described; common approach is ulnar to palmaris longus tendon (if present) or just ulnar to midline of wrist (if PL absent), at or just proximal to distal wrist crease, 45° angle aiming distally into tunnel
- Needle: 25-27 gauge, 1.5 inch
- Injectate:
- Corticosteroid: Methylprednisolone 40mg or triamcinolone 10-40mg or dexamethasone 4-8mg
- Local anesthetic: Lidocaine 1% or bupivacaine 0.25%, 1-2 mL
- Total volume: 2-3 mL
- Ultrasound guidance: Emerging technique; visualizes needle tip, median nerve, and distribution of injectate; may reduce risk of nerve injection but not yet standard of care
Precautions:
- NEVER inject if paresthesias occur during needle advancement or injection (suggests intraneural injection - withdraw immediately)
- Avoid injection through palmar skin (palmar approach) due to risk to recurrent motor branch and increased pain
- Use aseptic technique
Complications:
- Median nerve injury (paresthesias, numbness, weakness) - rare if technique correct
- Skin/subcutaneous atrophy, depigmentation at injection site
- Flexor tendon rupture (rare, case reports after multiple injections)
- Infection (rare)
- Transient increase in blood glucose (diabetics)
Outcomes:
- Excellent (symptom-free): 20-40% at 1 year
- Good (improved): Additional 20-30% at 1 year
- Failure: 30-60% require surgery within 1 year
- Repeat injection: Can be considered if good initial response but recurrence; limited evidence for \u003e2 injections
4. Oral Medications
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs):
- Evidence: Limited; some benefit for pain but not for paresthesias or function
- Role: Adjunct for pain control, not curative
- Example: Ibuprofen 400mg TID, Naproxen 500mg BID
Oral Corticosteroids:
- Evidence: RCTs show short-term benefit (2-4 weeks), no long-term benefit
- Regimen: Prednisone 20mg daily x 2 weeks, or tapering course
- Role: Temporary relief; inferior to injection; consider if injection contraindicated or patient refuses injection
- Side effects: Hyperglycemia, mood changes, insomnia, GI upset - limit use
Diuretics:
- Evidence: Weak; one small RCT showed benefit
- Role: May be tried in pregnancy-related CTS with significant edema; limited role otherwise
Vitamin B6 (Pyridoxine):
- Evidence: Conflicting; most rigorous studies show no benefit
- Not recommended based on current evidence
Gabapentin, Pregabalin (Neuropathic pain agents):
- Evidence: No specific RCTs for CTS
- Role: May provide symptomatic relief of neuropathic pain/paresthesias but does not address underlying compression
- Consider: Refractory symptoms, surgical contraindication, adjunct to other treatments
5. Physical and Occupational Therapy
Modalities:
- Ultrasound therapy (controversial, limited evidence)
- Laser therapy (low-level laser - some positive studies, not widely adopted)
- Manual therapy, nerve gliding exercises (limited evidence)
Evidence: Insufficient high-quality evidence to recommend as primary treatment. May be beneficial as adjunct, particularly for patient education regarding activity modification and ergonomics.
6. Alternative Therapies
Yoga:
- One RCT showed benefit compared to splinting
- Mechanism: Improved upper extremity strength, flexibility, blood flow
- Safe, may be beneficial adjunct
Acupuncture:
- Limited evidence; some small studies suggest benefit
- Not standard recommendation
Chiropractic manipulation:
- No evidence for benefit in CTS
Conservative Management: Practical Approach
Initial Management (Mild-Moderate CTS):
- Nocturnal wrist splinting x 6-12 weeks
- Activity modification / ergonomic assessment
- NSAIDs for pain (if significant)
- Re-assess at 6-12 weeks
If Inadequate Response: 5. Corticosteroid injection 6. Continue splinting 7. Re-assess at 6-12 weeks post-injection
If Still Inadequate or Recurrence: 8. Surgical consultation
Special Cases:
- Pregnancy: Expectant management with splinting; 90% resolve within 3 months postpartum
- Mild symptoms, patient refuses surgery: Long-term splinting acceptable with annual follow-up; educate about signs of progression (weakness, atrophy) requiring surgery
9. Management: Surgical
Indications for Surgery
Absolute Indications:
- Severe CTS with thenar atrophy and/or significant weakness (muscle recovery unlikely if delayed)
- Acute carpal tunnel syndrome (trauma, hematoma, infection, burns - surgical emergency)
- Presence of space-occupying lesion requiring excision (tumor, ganglion)
Relative Indications (Majority of Cases):
- Failed conservative management (splinting and/or injection) with persistent symptoms
- Moderate-to-severe CTS on NCS with significant symptoms
- Patient preference for definitive treatment over ongoing conservative management
- Bilateral severe disease affecting quality of life and function
Timing:
- Acute traumatic CTS: Emergency within hours (compartment syndrome equivalent)
- Severe chronic CTS with atrophy: Urgent (within weeks) to prevent irreversible muscle damage
- Moderate symptomatic CTS: Elective (after failed conservative trial, or if patient desires surgery)
- Mild CTS: Generally conservative management first unless patient preference
Surgical Technique: Open Carpal Tunnel Release (OCTR)
Gold Standard Technique - Most Common Worldwide
Anesthesia Options:
- Local anesthetic infiltration (1% lidocaine with or without epinephrine) + sedation
- Regional block (median nerve block, Bier block, axillary block)
- General anesthesia (rarely needed unless patient preference or combined procedure)
- WALANT (Wide Awake Local Anesthesia No Tourniquet): Increasingly popular; uses buffered lidocaine with epinephrine, no tourniquet, patient awake, allows intraoperative motor testing
Positioning:
- Supine, arm on hand table
- Tourniquet typically used (WALANT technique exceptions)
Incision:
- Location: Proximal to distal wrist crease, aligned with radial border of ring finger (Kaplan's cardinal line - extended from radial border of ring finger to distal wrist crease)
- Length: 2.5-4 cm (shorter "mini-open" techniques described, 1.5-2.5 cm)
- Key landmarks:
- Radial limit: Avoid recurrent motor branch (arises at radial edge of flexor retinaculum)
- Ulnar limit: Ulnar border of palmaris longus (if present) or just ulnar to midline
- Distal limit: Do not cross distal palmar crease (risk of painful scar, injury to palmar arch)
Procedure:
- Skin incision through dermis
- Divide palmar fascia longitudinally
- Identify transverse carpal ligament (glistening white transverse fibers)
- Protect median nerve (typically radial and superficial)
- Incise transverse carpal ligament longitudinally under direct vision from distal to proximal
- Distal release: Release to level of superficial palmar arch (ensure complete release of distal edge)
- Proximal release: Release proximal to distal wrist crease, divide antebrachial fascia for ~2cm proximal to ensure adequate decompression
- Inspect median nerve (bulging, hourglass constriction, hyperemia in acute cases)
- Verify complete release (should be able to pass probe freely deep to divided ligament)
- Hemostasis
- Skin closure (absorbable or non-absorbable suture, or surgical adhesive)
- Soft dressing, wrist neutral
Anatomical Considerations:
- Recurrent Motor Branch: Extraligamentous (46%), subligamentous (31%), transligamentous (23%) [9]
- Extraligamentous: Most at risk; exits radial to ligament
- Subligamentous: Travels beneath ligament, safer
- Transligamentous: Pierces through ligament, at risk during division
- Protection: Stay ulnar to midline during release, release under direct vision
- Superficial Palmar Arch: Typically 1cm distal to distal edge of flexor retinaculum; avoid extending incision past distal palmar crease
- Palmar Cutaneous Branch: Superficial to flexor retinaculum, variable location; at risk with skin incision (protective: precise midline or ulnar incision, careful skin handling)
Surgical Technique: Endoscopic Carpal Tunnel Release (ECTR)
Minimally Invasive Alternative
Advantages:
- Smaller scar (wrist incision only, or wrist + palm portal)
- Faster return to work (average 1 week earlier than OCTR)
- Less pillar pain
- Patient satisfaction with cosmesis
Disadvantages:
- Higher cost (equipment)
- Steeper learning curve
- Higher complication rate in inexperienced hands
- Cannot address masses or perform synovectomy
- Requires specialized equipment and training
Techniques:
- Single-portal (Agee): Wrist incision only, blade housed in endoscope
- Two-portal (Chow): Proximal wrist and distal palm portals, blade separate from endoscope
Outcomes: Cochrane review and multiple RCTs: Equivalent symptom relief and functional outcomes compared to open technique at 1 year. Faster return to work (1 week) but higher risk of nerve injury in meta-analyses. [21]
Learning Curve: Complication rates decrease significantly after 25-50 cases. Not recommended for surgeons performing \u003c10 cases/year.
Post-Operative Care
Immediate (Day 0-14):
- Soft dressing, allow finger motion immediately
- Elevate hand to reduce swelling
- Finger ROM exercises (prevent stiffness)
- Avoid heavy lifting, forceful gripping
- Pain control: Acetaminophen, NSAIDs, ice (narcotics rarely needed)
- Wound care: Keep dry until suture removal
Early (Week 2-6):
- Suture removal 10-14 days (if non-absorbable)
- Progressive use of hand for light activities (ADLs)
- Scar massage (after suture removal)
- Driving: When comfortable (typically 1-2 weeks)
- Return to light work: 2-4 weeks (earlier for endoscopic)
Intermediate (Week 6-12):
- Unrestricted activity (manual labor, sports)
- Grip strengthening exercises
- Pillar pain typically peaks at 6-8 weeks, gradually resolves
Long-term (Month 3-12):
- Continued improvement in grip strength up to 3-6 months
- Scar maturation continues to 12 months
- Sensory recovery may continue up to 12 months (severe cases)
- Motor recovery (if atrophy present): Variable, may not fully recover
Surgical Outcomes
Success Rates:
- Overall patient satisfaction: 75-90%
- Complete symptom resolution: 70-90%
- Improved but residual symptoms: 10-20%
- Failure (no improvement or worse): 5-10%
Predictors of Good Outcome:
- Shorter symptom duration (\u003c12 months)
- Positive response to corticosteroid injection
- Younger age
- Absence of thenar atrophy
- Absence of other comorbidities (diabetes, obesity, workers' comp claim)
- Non-work-related CTS
Predictors of Poor Outcome:
- Long symptom duration (\u003e3 years)
- Severe NCS abnormalities (axonal loss)
- Thenar atrophy (motor recovery poor even after successful decompression)
- Workers' compensation or litigation
- Psychiatric comorbidity (depression, anxiety)
- Multiple prior injections
- Bilateral disease
- Older age
- Obesity
Symptom Resolution Timeline:
- Nocturnal paresthesias: Immediate to 1 week (most dramatic improvement)
- Daytime numbness: 1-3 months (gradual)
- Weakness: 3-6 months (gradual, may not fully recover if atrophy present)
- Thenar atrophy: May not recover (muscle replaced by fat if chronic denervation \u003e1-2 years)
- Grip strength: Returns to baseline by 3-6 months
- Pillar pain: Resolves by 3-6 months (75%)
Recurrence:
- True recurrence (after initial successful relief): 3-12% at 5-10 years
- Risk factors: Diabetes, dialysis, hypothyroidism, heavy manual labor
- Persistent symptoms (incomplete release): 5-10%
10. Complications
Disease Complications (Untreated CTS)
Sensory Deficits:
- Permanent numbness: Loss of protective sensation, risk of burns, injuries
- Loss of two-point discrimination: Impaired fine tactile discrimination
- Chronic pain: Neuropathic pain (burning, dysesthesia)
Motor Deficits:
- Thenar atrophy: Irreversible muscle loss if chronic (\u003e1-2 years severe compression)
- Weakness of opposition: Devastating functional impairment (inability to pinch, grasp, manipulate objects)
- Loss of dexterity: Affects writing, buttoning, tool use, activities of daily living
Quality of Life Impact:
- Sleep disruption (nocturnal awakening)
- Reduced work productivity, disability
- Depression, anxiety
Surgical Complications
Intraoperative:
-
Incomplete Release (5-10%):
- Failure to divide entire transverse carpal ligament (distal or proximal edge)
- Residual compression from antebrachial fascia
- Prevention: Ensure complete division under direct vision, release proximal fascia, verify with probe
-
Recurrent Motor Branch Injury (0.3-3%):
- "Million dollar complication"
- litigation risk
- Loss of thumb opposition, APB function
- Risk higher with transligamentous/extraligamentous branch anatomy
- Prevention: Stay ulnar to midline during release, identify and protect nerve
-
Median Nerve Laceration (0.1-0.5%):
- Complete or partial transection
- Requires immediate repair (microsurgical epineurial or fascicular repair)
- Outcomes variable; best with immediate recognition and repair
-
Ulnar Artery or Superficial Palmar Arch Injury (\u003c1%):
- Risk with over-aggressive distal release
- May present with hematoma, ischemia
- Management: Pressure, vascular surgery consult if ischemia
-
Flexor Tendon Laceration (Rare):
- Iatrogenic; typically recognized intraoperatively
- Requires tendon repair
Early Post-operative (Days to Weeks):
-
Hematoma (1-2%):
- Presents with increasing pain, swelling, ecchymosis
- Most managed conservatively (elevation, compression)
- Evacuation if large or causing compression
-
Infection (0.4-1.5%):
- Superficial (cellulitis) or deep (flexor tenosynovitis, septic arthritis)
- Presentation: Erythema, warmth, purulent drainage, fever
- Management: Antibiotics; irrigation and debridement if deep infection
-
Wound Dehiscence:
- Risk factors: Tension, infection, poor tissue handling, early heavy use
- Management: Local wound care, revision closure if needed
-
Neuropraxia/Transient Nerve Symptoms:
- Temporary worsening of paresthesias, new burning sensation (common, usually resolves)
- Distinguish from nerve injury (progressive weakness, anesthesia)
Intermediate Post-operative (Weeks to Months):
-
Pillar Pain (20-30%):
- Tenderness and pain at thenar and hypothenar eminences (pillars of carpal tunnel)
- Due to separation of ligament edges, altered biomechanics
- Typically resolves spontaneously by 3-6 months (75%)
- Management: Reassurance, NSAIDs, activity modification, desensitization exercises
- Persistent cases: Consider scar massage, physical therapy, corticosteroid injection (rare)
-
Scar Tenderness/Hypertrophic Scar:
- Painful scar, hypertrophic or keloid formation
- Management: Scar massage, silicone gel, pressure garments, corticosteroid injection, scar revision (if severe)
-
Bowstringing of Flexor Tendons (Rare):
- Loss of pulley function if transverse carpal ligament not reconstituted
- Presents with decreased grip strength, palpable tendon prominence with flexion
- Management: Reconstruction (complex)
-
Palmar Cutaneous Nerve Injury (Neuroma):
- Painful neuroma from injury to palmar cutaneous branch
- Presents with painful tender nodule, Tinel's sign over scar
- Management: Desensitization, neuroma injection, neuroma excision + nerve burial (if refractory)
Late Post-operative (Months to Years):
-
Complex Regional Pain Syndrome (CRPS) / Reflex Sympathetic Dystrophy (1-5%):
- Disproportionate pain, swelling, stiffness, autonomic changes (color, temperature, sweating)
- Allodynia, hyperalgesia
- Risk factors: Female, anxiety, prior CRPS
- Diagnosis: Clinical (Budapest criteria)
- Management: Multidisciplinary (physical therapy, desensitization, medications [gabapentin, pregabalin, bisphosphonates], stellate ganglion block, sympathectomy in severe cases)
- Prevention: Early mobilization, adequate pain control
-
Recurrent Carpal Tunnel Syndrome (3-12%):
- True recurrence after initial successful relief
- Causes: Scar tissue (perineural fibrosis), synovial proliferation, inadequate initial release
- Diagnosis: Clinical + NCS (exclude other causes)
- Management: Revision surgery (lower success rate than primary surgery, 60-80%)
-
Persistent Symptoms (5-10%):
- No improvement or minimal improvement post-surgery
- Causes:
- Incorrect diagnosis (cervical radiculopathy, polyneuropathy, double crush)
- Incomplete release
- Irreversible nerve damage (axonal loss)
- Evaluation: NCS, MRI (assess adequacy of release), cervical spine evaluation
- Management: Address underlying cause; revision surgery if incomplete release confirmed
-
Stiffness/Loss of Motion:
- Finger stiffness, reduced wrist motion
- Risk factors: Prolonged immobilization, CRPS, patient non-compliance with therapy
- Prevention: Early finger ROM exercises, hand therapy
- Management: Intensive hand therapy, splinting, manipulation under anesthesia (rare)
Medicolegal Considerations
- Informed consent: Discuss risks of nerve injury, infection, CRPS, incomplete relief, pillar pain, need for revision
- Documentation: Pre-operative NCS, symptom severity scales (BCTQ), functional assessment
- Complication management: Early recognition, appropriate treatment, prompt specialist referral when indicated
11. Evidence & Guidelines
Landmark Studies
1. Atroshi et al. (1999) - Prevalence Study [1]
- Study: Population-based study in Sweden
- Finding: 3.8% prevalence in general population; 2.7% with clinically and electrophysiologically confirmed CTS
- Impact: Established CTS as most common entrapment neuropathy
2. Gerritsen et al. (2002) - Conservative vs Surgical RCT [4]
- Study: RCT comparing surgery to splinting in 176 patients
- Findings: Surgery superior to splinting at 18 months (success rate 90% vs 75%); greater improvement in symptoms and function
- Impact: High-level evidence supporting surgery as definitive treatment
3. Huisstede et al. (2018) - Carpal Tunnel Syndrome Guideline [22]
- Guideline: Multidisciplinary European guideline (EULAR)
- Recommendations:
- Splinting: First-line for mild-moderate CTS
- Corticosteroid injection: Effective short-term, consider for moderate CTS
- Surgery: Most effective treatment for moderate-severe CTS
- Ultrasound, laser, exercises: Insufficient evidence
4. Vasiliadis et al. (2014) - Cochrane Review: Endoscopic vs Open [21]
- Review: Systematic review of 28 trials, 2586 participants
- Findings:
- Equivalent symptom relief at \u003e12 months
- Endoscopic: Faster return to work (6 days earlier), less pillar pain
- Endoscopic: Higher risk of nerve injury (transient)
- Conclusion: Both techniques effective; choice depends on surgeon experience and patient preference
5. Shi & MacDermid (2011) - Prognostic Factors Meta-analysis [23]
- Review: Systematic review of prognostic factors for surgical outcome
- Findings: Poor prognostic factors include:
- Longer symptom duration
- Bilateral CTS
- Higher BMI
- Workers' compensation
- Thenar atrophy
- Older age
Clinical Practice Guidelines
American Academy of Orthopaedic Surgeons (AAOS) 2016:
- Strong recommendations:
- Surgical release for severe CTS (thenar atrophy)
- Multi-modal hand therapy post-operatively
- Moderate recommendations:
- Splinting for mild-moderate CTS
- Corticosteroid injection for symptom relief
- Either open or endoscopic release (equivalent outcomes)
- Against: NSAIDs, diuretics, magnets, laser, ultrasound (insufficient evidence)
American Academy of Neurology (AAN) 2020:
- NCS recommended when:
- Diagnosis uncertain
- Atypical presentation
- Pre-operative confirmation
- Evaluation of treatment response
- Not required for clear-cut clinical diagnosis if surgery not planned
UK NICE Guidance:
- Offer conservative treatment first (splinting) for mild-moderate symptoms
- Refer for surgery if:
- Failed conservative management (6-12 weeks)
- Severe symptoms with motor involvement
- Persisting symptoms affecting quality of life
Current Controversies and Evolving Evidence
1. Role of Ultrasound vs NCS:
- Emerging evidence suggests ultrasound comparable to NCS for diagnosis
- Advantages: Non-invasive, visualizes structural abnormalities, dynamic assessment
- Limitations: Operator-dependent, limited availability
- Future: May complement or replace NCS in select cases
2. WALANT (Wide Awake Surgery):
- Increasing adoption for CTR and other hand procedures
- Advantages: No tourniquet pain, intraoperative motor testing, cost savings, patient satisfaction
- Requires epinephrine (vasospasm concerns debunked in recent evidence)
3. Platelet-Rich Plasma (PRP) Injection:
- Emerging evidence from RCTs suggests benefit comparable to corticosteroid injection
- Longer duration of effect in some studies
- Not yet widely adopted; awaiting larger trials
4. Nerve Hydrodissection:
- Ultrasound-guided injection of fluid (saline, dextrose, local anesthetic) to separate nerve from surrounding structures
- Preliminary studies promising
- Requires further investigation
12. Special Populations
Pregnancy
Epidemiology:
- 30-62% of pregnant women develop CTS, typically in third trimester
- Bilateral in 80%
- Risk factors: Multiparity, increased weight gain, pre-existing edema
Pathophysiology:
- Fluid retention (increased total body water by 6-8L)
- Hormonal changes (relaxin, progesterone) may affect connective tissue
Natural History:
- 90% resolve spontaneously within 3 months postpartum
- 5-10% persist and require treatment
Management:
- First-line: Nocturnal wrist splinting
- Second-line: Corticosteroid injection (local, minimal systemic absorption; safe in pregnancy)
- Surgery: Defer until postpartum unless severe motor involvement (very rare)
- Educate: Reassure regarding spontaneous resolution, importance of splint compliance
Diabetes
Epidemiology:
- 14-30% prevalence in diabetics (2-3x general population)
- Associated with longer duration of diabetes, poor glycemic control
Pathophysiology:
- Metabolic effects on nerve (impaired axoplasmic transport, microvascular disease)
- Non-enzymatic glycosylation of tendons and ligaments (thickening, reduced compliance)
- Concurrent diabetic polyneuropathy complicates diagnosis
Clinical Considerations:
- May have atypical presentation (less nocturnal symptoms if concurrent polyneuropathy)
- Higher risk of stiffness post-operatively
- Slower nerve recovery
- Higher recurrence rate
Management:
- Optimize glycemic control
- Lower threshold for NCS (confirm CTS vs polyneuropathy vs both)
- Surgical outcomes good but slightly inferior to non-diabetics
- Aggressive hand therapy post-operatively to prevent stiffness
Dialysis Patients (Dialysis-Related Amyloidosis)
Epidemiology:
- Up to 50% of patients on hemodialysis \u003e10 years
- Due to beta-2 microglobulin amyloid deposition
Clinical Features:
- Often bilateral, severe
- Associated with carpal bone cysts on radiographs
- May have trigger fingers, flexor tenosynovitis
Management:
- Surgery often required
- Intraoperative findings: Thickened synovium, amyloid deposits (send for pathology)
- Recurrence common
- Renal transplantation may halt progression
Rheumatoid Arthritis
Epidemiology:
- 40-60% prevalence
- Often bilateral
Pathophysiology:
- Synovial proliferation, tenosynovitis
Management:
- Optimize RA medical management
- Surgery often required; may perform synovectomy concurrently
- Higher recurrence rate if RA poorly controlled
Pediatric CTS (Rare)
Causes:
- Mucopolysaccharidoses (Hurler, Hunter syndromes)
- Skeletal dysplasias (achondroplasia)
- Post-traumatic
- Idiopathic (very rare)
Management:
- Address underlying condition
- Surgery as in adults if indicated
13. Patient Explanation (Layperson Language)
What is Carpal Tunnel Syndrome?
Imagine your wrist as a tunnel - it's made of small bones on three sides and a tight band (ligament) on the palm side. Through this tunnel travel nine tendons (like ropes that move your fingers) and one very important nerve called the median nerve. This nerve brings feeling to your thumb, index, middle, and half of your ring finger, and it controls some of the muscles at the base of your thumb.
When the tunnel becomes too crowded - either because the tendons swell up or the tunnel itself gets smaller - the nerve gets squashed. A squashed nerve doesn't work properly, which is why you get numbness, tingling, and sometimes weakness.
Why does it wake me up at night?
Several reasons:
- When you sleep, fluid naturally pools in your hands because they're at the level of your heart (not elevated like when you're standing)
- Most people sleep with their wrists bent (flexed), which makes the tunnel even tighter and increases pressure on the nerve
- Your blood pressure drops slightly when you sleep, making it harder for blood to get to the nerve
This is why shaking your hand helps - it pumps the fluid out and gets fresh blood flowing to the nerve.
Will it go away on its own?
Sometimes, especially if:
- You're pregnant (usually goes away after delivery)
- It's very mild and only been happening a short time
- You can fix the underlying problem (like treating thyroid disease or changing how you use your hands at work)
But if it's been going on for months or years, or if you're noticing muscle shrinking at the base of your thumb, it usually won't go away without treatment.
What are my treatment options?
Option 1: Wrist Splint (First Step for Mild Cases)
- A brace that holds your wrist straight, especially at night
- Keeps your wrist from bending while you sleep, which reduces pressure
- Works for about 60-80% of people with mild symptoms
- You need to wear it consistently for at least 6 weeks to know if it's working
Option 2: Steroid Injection (If Splint Doesn't Work)
- A shot of anti-inflammatory medicine into the tunnel area (not directly into the nerve!)
- Reduces swelling and pressure for several weeks to months
- About 80% of people get relief initially, but only 20-40% are still better after a year
- Good option if you need temporary relief or want to avoid surgery
- Can be repeated if it works well the first time
Option 3: Surgery (For Severe Cases or When Other Treatments Fail)
- The surgeon cuts the tight band (ligament) that forms the roof of the tunnel
- This permanently opens up the tunnel and takes pressure off the nerve
- About 90% of people are satisfied with results
- Two ways to do it:
- Open surgery: 3cm incision in your palm, direct view, most common
- Endoscopic surgery: Smaller incisions, tiny camera, faster recovery but more expensive
Do I need surgery?
Probably YES if:
- The muscle at the base of your thumb is shrinking (you can see a dent)
- Your thumb feels very weak
- You've tried splinting and/or an injection and it didn't work
- Symptoms are affecting your job or daily life significantly
Probably NOT RIGHT AWAY if:
- Symptoms are mild and only occasional
- You're pregnant (wait until after delivery - it usually gets better)
- Shaking your hand still relieves symptoms
- You haven't tried a splint yet
What's recovery like after surgery?
Day 1:
- Nighttime numbness usually stops immediately (most noticeable improvement)
- Hand in soft bandage, can move fingers right away
Week 2:
- Stitches come out
- Can drive and do light activities
- Start using hand for daily tasks (eating, typing, grooming)
Week 6:
- Can return to heavier activities
- Grip strength improving
Month 3-6:
- Daytime numbness usually gone
- Grip strength back to normal
- Occasional scar tenderness on sides of hand (pillar pain) - this is common and goes away
Month 6-12:
- Continued improvement in sensation if it was severely affected
- Scar continues to soften
Important: If your muscle had already shrunk before surgery, it might not grow back fully. The surgery stops things from getting worse and usually improves numbness and pain, but shrunken muscle that's been gone for years may not recover.
What if I don't treat it?
If mild, some people live with it for years. But if moderate or severe, without treatment:
- The numbness can become permanent
- The muscle at the base of your thumb can waste away and not come back
- You lose the ability to pinch and grasp properly
- Chronic pain can develop
The nerve is like a garden hose - if you step on it briefly, water flows again when you step off. But if you leave something heavy on it for months, the hose gets damaged and doesn't work right anymore even after you remove the weight.
Can I prevent it from happening again?
After surgery, true recurrence is uncommon (3-12%). To minimize risk:
- Take breaks during repetitive hand activities
- Keep wrists in neutral position when possible (not bent up or down)
- Maintain healthy weight
- Manage medical conditions (diabetes, thyroid)
- Use ergonomic tools and workstations
If it's work-related, talk to your employer about ergonomic assessment and job modifications.
14. Examination Focus (Viva Vault)
Basic Sciences
Q1: Describe the anatomy of the carpal tunnel.
A: The carpal tunnel is a fibro-osseous canal at the wrist. The boundaries are:
- Floor and walls: Carpal bones - scaphoid and trapezium (radial), pisiform and hamate (ulnar), proximal row bones (floor)
- Roof: Transverse carpal ligament (flexor retinaculum), extending from scaphoid/trapezium to pisiform/hamate
Contents (10 structures):
- 1 median nerve (most superficial, directly beneath flexor retinaculum)
- 9 flexor tendons:
- 4 Flexor Digitorum Superficialis (FDS)
- 4 Flexor Digitorum Profundus (FDP)
- 1 Flexor Pollicis Longus (FPL)
- Synovial sheaths surrounding tendons
Note: Flexor Carpi Radialis (FCR) has its own separate tunnel and is NOT within the carpal tunnel.
Q2: What is the motor innervation of the median nerve in the hand?
A: The median nerve provides motor innervation via the Recurrent Motor Branch, which supplies the thenar muscles (remember "LOAF" minus Lumbricals):
- Opponens Pollicis
- Abductor Pollicis Brevis
- Flexor Pollicis Brevis (superficial head only; deep head is ulnar nerve)
Additionally, the median nerve supplies the 1st and 2nd lumbricals (distal to the carpal tunnel).
Q3: Explain the pathophysiology of carpal tunnel syndrome.
A: CTS results from increased pressure within the carpal tunnel compressing the median nerve. The pathophysiological cascade occurs in three stages:
Stage 1 (Reversible - Ischemia):
- Elevated intracarpal pressure (normal 2.5mmHg, in CTS 30-110mmHg)
- Pressure exceeds capillary perfusion pressure, causing venous congestion
- Impaired microcirculation via vasa nervorum
- Clinical: Intermittent paresthesias, nocturnal symptoms
Stage 2 (Potentially Reversible - Demyelination):
- Chronic ischemia leads to segmental demyelination
- Subperineurial edema, perineurial thickening
- Clinical: Persistent numbness, positive provocative tests
- Electrophysiology: Slowed conduction velocity
Stage 3 (Irreversible - Axonal Loss):
- Wallerian degeneration of axons
- Motor unit loss, muscle denervation
- Clinical: Thenar atrophy, weakness, permanent sensory loss
- Electrophysiology: Reduced CMAP/SNAP amplitudes, denervation on EMG
Clinical Assessment
Q4: How do you clinically differentiate Carpal Tunnel Syndrome from Pronator Syndrome?
A: Both involve median nerve compression, but at different anatomical sites:
| Feature | CTS | Pronator Syndrome |
|---|---|---|
| Site | Carpal tunnel (wrist) | Proximal forearm (pronator teres or FDS arch) |
| Thenar skin | SPARED (palmar cutaneous branch arises proximal to tunnel) | AFFECTED (numbness over thenar eminence) |
| Nocturnal symptoms | Yes (hallmark) | No |
| Pain location | Wrist, hand | Proximal volar forearm |
| Provocative tests | Phalen's, Durkan's positive | Resisted pronation or FDS flexion (middle finger) reproduces symptoms |
| Tinel's | At wrist | Over pronator teres (proximal forearm) |
Key differentiator: Palmar thenar skin sensation. If numb, it's proximal to the carpal tunnel.
Q5: What are the indications for nerve conduction studies in suspected CTS?
A:
- Atypical presentation or uncertain diagnosis
- Ruling out concurrent or alternative diagnoses (cervical radiculopathy, polyneuropathy, plexopathy, double crush)
- Pre-operative documentation (medicolegal baseline, severity grading)
- Bilateral symptoms (determine which side to operate first, or if both equally affected)
- Failed conservative treatment before proceeding to surgery
- Post-operative symptom recurrence (distinguish incomplete release, recurrent CTS, or new pathology)
NCS is NOT required for straightforward clinical diagnosis if surgery is not being considered.
Q6: Describe your clinical examination of a patient with suspected CTS.
A: Systematic approach:
1. Inspection:
- Bilateral comparison of thenar eminences (atrophy, guttering)
- Skin changes, scars from previous surgery
- Wrist deformity (trauma, arthritis)
2. Sensory Examination:
- Light touch: Median distribution (thumb, index, middle, radial ring) vs ulnar (little finger)
- Two-point discrimination on index finger pulp (normal \u003c6mm)
- Test palmar thenar skin (should be normal in CTS)
3. Motor Examination:
- APB strength: Thumb abduction perpendicular to palm (MRC grading)
- Opposition: Thumb tip to little finger tip
- Pinch strength (compare to contralateral)
4. Provocative Tests (perform multiple for increased sensitivity):
- Durkan's: Direct compression over tunnel x30 seconds (most specific)
- Phalen's: Wrist flexion x60 seconds
- Flick sign: Ask "What do you do when symptoms wake you?"
- Tinel's: Percussion over median nerve at wrist
5. Rule out other pathology:
- Cervical spine examination (Spurling's test for radiculopathy)
- Elbow examination (cubital tunnel, medial epicondyle for ulnar nerve)
- Thoracic outlet maneuvers (Roos test, Adson's)
Management
Q7: A 52-year-old woman presents with 6 months of nocturnal hand numbness in the thumb, index, and middle fingers. Examination shows positive Phalen's and Durkan's tests, normal strength, no atrophy. How do you manage her?
A: This is mild-to-moderate CTS (intermittent symptoms, no motor signs). Management:
Initial (Conservative):
- Nocturnal wrist splinting (neutral position) for 6-12 weeks - first-line treatment
- Activity modification and ergonomic assessment (if occupational component)
- NSAIDs for pain relief if needed
- Educate regarding natural history and warning signs (weakness, atrophy) that would prompt surgery
If inadequate response at 6-12 weeks: 5. Corticosteroid injection (40mg methylprednisolone) 6. Continue splinting 7. Re-assess at 6-12 weeks post-injection
If persistent symptoms or recurrence after injection: 8. Surgical consultation for carpal tunnel release 9. Consider NCS for severity grading and pre-operative documentation
Q8: What are the indications for urgent/emergency surgical decompression in CTS?
A:
Emergency (Within Hours):
- Acute carpal tunnel syndrome: Sudden onset with rapidly progressive symptoms, typically after:
- Distal radius fracture or perilunate dislocation
- Penetrating trauma with hematoma
- Burns with compartment-like swelling
- Snake bite, hemorrhage into tunnel
- Rationale: Acute severe pressure causes rapid irreversible ischemic nerve damage (analogous to compartment syndrome)
Urgent (Within Days to Weeks):
- Severe CTS with thenar atrophy and/or significant weakness
- Rationale: Ongoing axonal loss; motor recovery unlikely if delayed beyond point of muscle replacement by fat (typically 1-2 years of denervation)
Q9: Describe the surgical technique for open carpal tunnel release.
A:
Pre-operative:
- Consent (risks: infection, nerve injury, pillar pain, CRPS, incomplete relief)
- Anesthesia: Local/regional/general (WALANT increasingly popular)
Positioning:
- Supine, arm on hand table, tourniquet (if not WALANT)
Incision:
- 2.5-4cm, proximal to distal wrist crease
- Aligned with radial border of ring finger (Kaplan's cardinal line)
- Stay ulnar to midline (protect recurrent motor branch)
- Do not cross distal palmar crease (avoid palmar arch, minimize painful scar)
Procedure:
- Incise skin, subcutaneous tissue
- Divide palmar fascia longitudinally
- Identify transverse carpal ligament (white transverse fibers)
- Protect median nerve (radial and superficial)
- Incise ligament longitudinally under direct vision, distal to proximal
- Complete distal release (to superficial palmar arch level)
- Complete proximal release (release antebrachial fascia ~2cm proximal to wrist crease)
- Inspect nerve (should bulge slightly, hourglass appearance if chronic compression)
- Verify complete release (pass probe beneath divided ligament)
- Hemostasis
- Skin closure, soft dressing
Post-operative:
- Immediate finger ROM
- Elevate
- Suture removal 10-14 days
- Progressive return to activity
Q10: What is the "Million Dollar Nerve" and why is it important surgically?
A: The Recurrent Motor Branch of the median nerve.
Anatomy:
- Arises at distal edge of transverse carpal ligament
- Variable course:
- Extraligamentous (46%): Exits radial to ligament - MOST AT RISK
- Subligamentous (31%): Travels beneath ligament - safer
- Transligamentous (23%): Pierces through ligament - at risk during division
Function:
- Supplies thenar muscles (Opponens Pollicis, APB, FPB superficial head)
- Essential for thumb opposition
Clinical Significance:
- Iatrogenic injury during CTR is devastating - complete loss of opposition ("simian thumb")
- Patient cannot oppose thumb to fingers (profound functional impairment)
- High litigation risk (hence "million dollar" complication)
Prevention:
- Stay ulnar to midline during ligament division
- Release under direct vision (avoid blind techniques)
- Identify and protect nerve if extraligamentous variant encountered
Complications
Q11: A patient develops severe pain, swelling, and stiffness 4 weeks after uncomplicated CTR. The hand is mottled, cool, and hypersensitive to touch. Diagnosis and management?
A: This is Complex Regional Pain Syndrome (CRPS), formerly Reflex Sympathetic Dystrophy.
Diagnosis (Budapest Criteria): Requires presence in 3 of 4 categories:
- Sensory: Hyperalgesia, allodynia
- Vasomotor: Temperature/color asymmetry
- Sudomotor/Edema: Swelling, sweating changes
- Motor/Trophic: Weakness, tremor, dystonia, trophic changes
Management (Multidisciplinary):
Early (Critical):
- Physical/Occupational therapy: Desensitization, graded motor imagery, mirror therapy, gentle ROM
- Analgesia:
- NSAIDs
- Neuropathic pain agents: Gabapentin 300-3600mg/day or Pregabalin 150-600mg/day
- Tricyclic antidepressants (amitriptyline)
- Bisphosphonates: Evidence for efficacy (e.g., alendronate, IV pamidronate)
- Vitamin C: Prophylactic (500mg daily) - some evidence for prevention
- Steroids: Short course (prednisone 30mg tapering) - early CRPS
Interventional (Refractory):
- Sympathetic blocks: Stellate ganglion block (upper extremity CRPS)
- Spinal cord stimulation: Severe refractory cases
- Ketamine infusion: Emerging evidence
Prognosis:
- Better with early aggressive treatment
- Chronic CRPS can be disabling
Q12: What is "pillar pain" and how do you manage it?
A: Pillar pain is tenderness and discomfort at the thenar and hypothenar eminences (the "pillars" of the carpal tunnel) following CTR.
Incidence: 20-30% of patients
Etiology:
- Separation of transverse carpal ligament edges
- Altered biomechanics of carpal arch
- Bowstringing of flexor tendons
- Scar tissue at pillar sites
Natural History:
- Typically appears 1-2 weeks post-op, peaks 6-8 weeks
- Spontaneous resolution in 75% by 3-6 months
Management:
Conservative (Majority):
- Reassurance: Educate regarding natural history and expected resolution
- NSAIDs: For symptomatic relief
- Activity modification: Avoid prolonged gripping, forceful activities during acute phase
- Desensitization exercises: Massage, texture differentiation
- Scar massage: After wound healed
Interventional (Persistent \u003e6 months):
- Corticosteroid injection: Into tender pillar area (NOT into carpal tunnel)
- Physical therapy: Intensive desensitization, strengthening
- Surgical revision: Very rare; consider if truly refractory and severely limiting function
15. References
-
Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosén I. Prevalence of carpal tunnel syndrome in a general population. JAMA. 1999;282(2):153-158. doi:10.1001/jama.282.2.153
-
Aroori S, Spence RA. Carpal tunnel syndrome. Ulster Med J. 2008;77(1):6-17. PMID: 18269111
-
Hansen PA, Micklesen P, Robinson LR. Clinical utility of the flick maneuver in diagnosing carpal tunnel syndrome. Am J Phys Med Rehabil. 2004;83(5):363-367. doi:10.1097/01.phm.0000124441.12241.60
-
Gerritsen AA, de Vet HC, Scholten RJ, Bertelsmann FW, de Krom MC, Bouter LM. Splinting vs surgery in the treatment of carpal tunnel syndrome: a randomized controlled trial. JAMA. 2002;288(10):1245-1251. doi:10.1001/jama.288.10.1245
-
Marshall S, Tardif G, Ashworth N. Local corticosteroid injection for carpal tunnel syndrome. Cochrane Database Syst Rev. 2007;(2):CD001554. doi:10.1002/14651858.CD001554.pub2
-
Padua L, Coraci D, Erra C, et al. Carpal tunnel syndrome: clinical features, diagnosis, and management. Lancet Neurol. 2016;15(12):1273-1284. doi:10.1016/S1474-4422(16)30231-9
-
Cobb TK, Dalley BK, Posteraro RH, Lewis RC Jr. Anatomy of the flexor retinaculum. J Hand Surg Am. 1993;18(1):91-99. doi:10.1016/0363-5023(93)90251-W
-
Durkan JA. A new diagnostic test for carpal tunnel syndrome. J Bone Joint Surg Am. 1991;73(4):535-538. PMID: 2013592
-
Lanz U. Anatomical variations of the median nerve in the carpal tunnel. J Hand Surg Am. 1977;2(1):44-53. doi:10.1016/s0363-5023(77)80009-9
-
Foley M, Silverstein B, Polissar N. The economic burden of carpal tunnel syndrome: long-term earnings of CTS claimants in Washington State. Am J Ind Med. 2007;50(3):155-172. doi:10.1002/ajim.20430
-
Taleisnik J. The palmar cutaneous branch of the median nerve and the approach to the carpal tunnel. J Bone Joint Surg Am. 1973;55(5):1212-1217. PMID: 4758032
-
Upton AR, McComas AJ. The double crush in nerve entrapment syndromes. Lancet. 1973;2(7825):359-362. doi:10.1016/s0140-6736(73)93196-6
-
Padua L, Di Pasquale A, Pazzaglia C, Liotta GA, Librante A, Mondelli M. Systematic review of pregnancy-related carpal tunnel syndrome. Muscle Nerve. 2010;42(5):697-702. doi:10.1002/mus.21910
-
Bland JD. Do nerve conduction studies predict the outcome of carpal tunnel decompression? Muscle Nerve. 2001;24(7):935-940. doi:10.1002/mus.1091
-
Nordstrom DL, DeStefano F, Vierkant RA, Layde PM. Incidence of diagnosed carpal tunnel syndrome in a general population. Epidemiology. 1998;9(3):342-345. PMID: 9583428
-
Stevens JC, Sun S, Beard CM, O'Fallon WM, Kurland LT. Carpal tunnel syndrome in Rochester, Minnesota, 1961 to 1980. Neurology. 1988;38(1):134-138. doi:10.1212/wnl.38.1.134
-
Singh R, Gamble G, Cundy T. Lifetime risk of symptomatic carpal tunnel syndrome in Type 1 diabetes. Diabet Med. 2005;22(5):625-630. doi:10.1111/j.1464-5491.2005.01487.x
-
Stahl S, Blumenfeld Z, Yarnitsky D. Carpal tunnel syndrome in pregnancy: indications for early surgery. J Neurol Sci. 1996;136(1-2):182-184. doi:10.1016/0022-510x(95)00299-r
-
Palmer KT, Harris EC, Coggon D. Carpal tunnel syndrome and its relation to occupation: a systematic literature review. Occup Med (Lond). 2007;57(1):57-66. doi:10.1093/occmed/kql125
-
Gelberman RH, Hergenroeder PT, Hargens AR, Lundborg GN, Akeson WH. The carpal tunnel syndrome. A study of carpal canal pressures. J Bone Joint Surg Am. 1981;63(3):380-383. PMID: 7204435
-
Vasiliadis HS, Georgoulas P, Shrier I, Salanti G, Scholten RJ. Endoscopic release for carpal tunnel syndrome. Cochrane Database Syst Rev. 2014;(1):CD008265. doi:10.1002/14651858.CD008265.pub2
-
Huisstede BM, Hoogvliet P, Randsdorp MS, Glerum S, van Middelkoop M, Koes BW. Carpal tunnel syndrome. Part I: effectiveness of nonsurgical treatments--a systematic review. Arch Phys Med Rehabil. 2010;91(7):981-1004. doi:10.1016/j.apmr.2010.03.022
-
Shi Q, MacDermid JC. Is surgical intervention more effective than non-surgical treatment for carpal tunnel syndrome? A systematic review. J Orthop Surg Res. 2011;6:17. doi:10.1186/1749-799X-6-17
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Median Nerve Anatomy
- Peripheral Nerve Injury and Repair
Differentials
Competing diagnoses and look-alikes to compare.
- Pronator Syndrome
- Cervical Radiculopathy (C6/C7)
- Ulnar Neuropathy
- Thoracic Outlet Syndrome
Consequences
Complications and downstream problems to keep in mind.
- Complex Regional Pain Syndrome
- Chronic Neuropathic Pain