Cellulitis and Erysipelas
Cellulitis is a common, spreading bacterial infection of the deep dermis and subcutaneous tissue, typically presenting with localised heat, redness (erythema), swelling (oedema), and pain. Erysipelas is a superficial...
What matters first
Cellulitis is a common, spreading bacterial infection of the deep dermis and subcutaneous tissue, typically presenting with localised heat, redness (erythema), swelling (oedema), and pain. Erysipelas is a superficial...
Pain out of proportion to clinical signs (Necrotising Fasciitis)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Pain out of proportion to clinical signs (Necrotising Fasciitis)
- Rapidly progressive erythema (approx less than 2cm/hour)
- Crepitus (Gas in soft tissue)
- Bullae (especially Haemorrhagic Bullae)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Cellulitis and Erysipelas
1. Clinical Overview
Summary
Cellulitis is a common, spreading bacterial infection of the deep dermis and subcutaneous tissue, typically presenting with localised heat, redness (erythema), swelling (oedema), and pain. Erysipelas is a superficial variant involving the upper dermis and superficial lymphatics, clinically distinguished by a sharply demarcated, raised border and "orange peel" (peau d'orange) texture. In practice, the terms are often overlapping, and management is broadly similar. [1]
The vast majority of cases (70-80%) are caused by Beta-haemolytic Streptococci (Groups A, B, C, G) rather than Staphylococcus aureus, a fact that influences empirical antibiotic choice (Penicillin/Flucloxacillin-based). [2] The portal of entry is often a breach in the skin barrier (e.g., Tinea pedis, eczema, trauma, or venous ulcers), although no entry point is found in ~50% of cases.
A critical clinical distinction is between "Simple Cellulitis" and "Cellulitis Mimics". The most common misdiagnosis (> 30% of referrals) is "Bilateral Cellulitis", which is almost invariably Venous Eczema / Lipodermatosclerosis or dependent oedema. As the aphorism goes: "Cellulitis is unilateral; Dermatitis is bilateral". [3]
Uncomplicated cellulitis responds rapidly to oral antibiotics. The challenge lies in identifying:
- Sepsis / Severe Infection: Requiring IV therapy (CREST Class III/IV).
- Necrotising Fasciitis: A surgical emergency requiring immediate debridement.
- Mimics: Preventing unnecessary antibiotic use.
Key Facts
- Pathogen: Streptococcus species (Group A Strep) are the #1 cause. Staph aureus is #2.
- Risk Factor: Lymphoedema is the strongest predisposing factor.
- Diagnostic Rule: "Bilateral Red Legs" = Venous Stasis (Red Legs), NOT Cellulitis.
- Emergency: Necrotising Fasciitis kills in hours. Look for "Pain out of proportion" and "Hard woody feel".
- Treatment: Flucloxacillin is the mainstay in the UK/Australia (covers Strep & MSSA). Penicillin V + Flucloxacillin is classic.
- Recurrence: High recurrence rate (20-50%) if underlying risk factors (Tinea pedis, oedema) are not managed. Prophylactic Penicillin V is evidentially supported. [4]
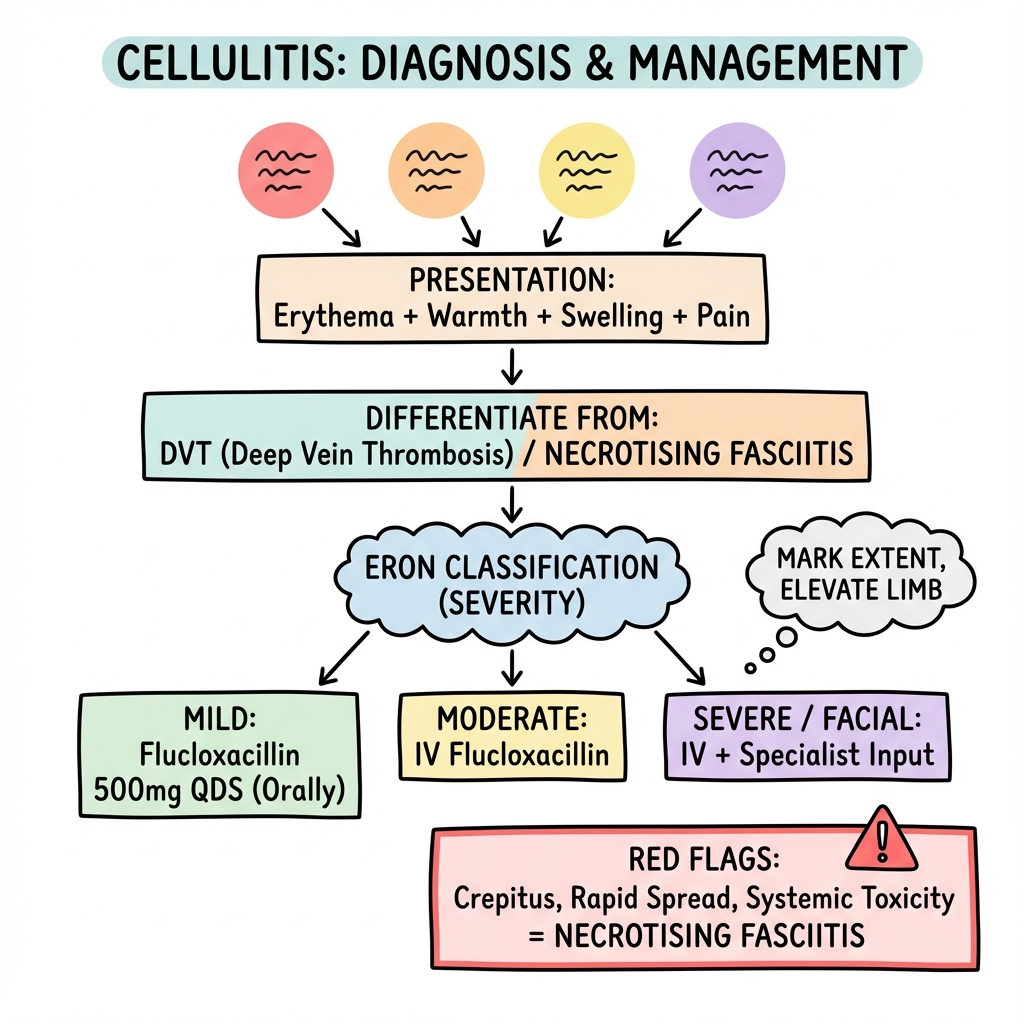
The Eron Classification (Severity Grading)
This guides the decision for Oral vs IV antibiotics and Admission vs Home.
| Class | Description | Management |
|---|---|---|
| I | No systemic toxicity. No comorbidities. | Oral antibiotics. Outpatient. |
| II | Systemic illness (Fever/Malaise) OR Comorbidity (DM/PVD). | IV or High dose Oral. Outpatient (OPAT) or Short Stay. |
| III | Significant systemic toxicity (Tachycardia, Tachypnoea) OR Unstable comorbidity. | IV antibiotics. Hospital Admission. |
| IV | Sepsis (Hypotension) OR Necrotising Fasciitis suspected. | Resuscitation. Urgent Surgical Consult. ICU. |
Clinical Pearls
The "Elevate" Pearl: Antibiotics kill the bug, but gravity kills the cure. You MUST elevate the limb higher than the hip to reduce oedema. Without elevation, antibiotics penetrate poorly into the waterlogged tissue, and the redness will not settle.
The "Marker" Pearl: Always draw a line around the erythema margin with a permanent marker on admission. This is the only objective way to track progression or regression over 24 hours.
The "Toe Web" Pearl: Always look between the toes. Tinea pedis (Athlete's foot) is the portal of entry in > 50% of leg cellulitis. Treating the fungal infection prevents recurrence.
The "Steroid" Pearl: In severe inflammation, once antibiotics are established (e.g., after 48h), a short course of Prednisolone can speed up recovery and reduce length of stay. (Evidence emerging).
2. Epidemiology
Incidence
- Common: Accounts for 2-3% of all emergency hospital admissions.
- Rate: Approx 200 cases per 100,000 patient-years.
- Trend: Increasing incidence due to rising ageing population, obesity, and diabetes.
Risk Factors (The "Portal of Entry")
Addressing these is key to prevention.
- Skin Barrier Breach:
- Tinea pedis (Fissures).
- Trauma / Abrasions / Insect bites.
- Ulcers (Venous/Arterial).
- Eczema / Psoriasis.
- Oedema:
- Lymphoedema (Mastectomy, previous cellulitis).
- Chronic Venous Insufficiency.
- Obesity (BMI > 30).
- Immune Status:
- Diabetes Mellitus.
- Immunosuppression (Chemo/Steroids).
- Cirrhosis.
- Surgical:
- Saphenous vein harvest sites (CABG).
Recurrent Cellulitis
- Approx 30% of patients will have a recurrence within 3 years.
- Each episode damages lymphatics further, predisposing to the next ("Vicious Cycle of Lymphoedema").
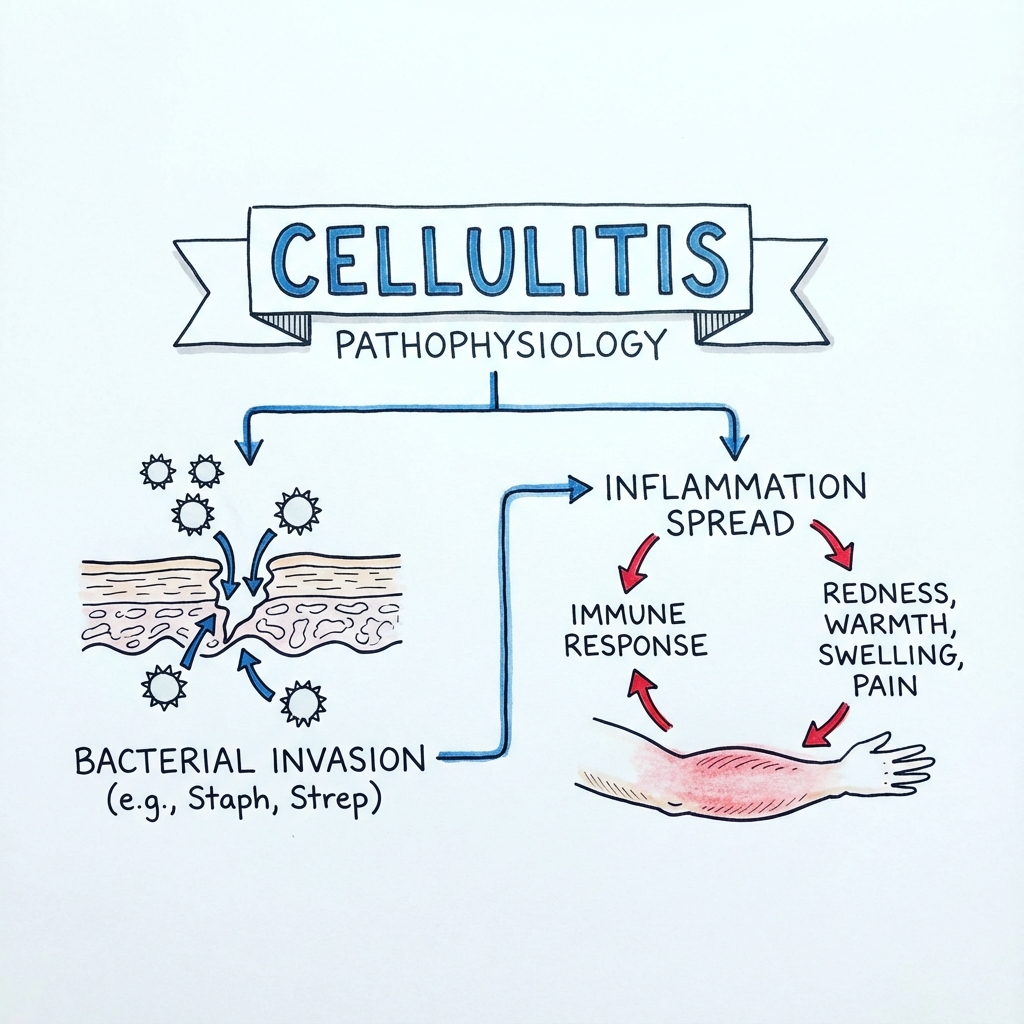
3. Pathophysiology
Mechanisms of Infection
1. Inoculation:
- Bacteria (usually commensals) breach the stratum corneum via a micro-abrasion (e.g., macerated toe web).
- They colonise the subcutaneous fat and dermis.
2. Proliferation:
- Streptococcus pyogenes (Group A): Produces hyaluronidase ("Spreading Factor") which breaks down connective tissue ground substance, allowing rapid spread along tissue planes. This typically causes the diffuse, non-purulent cellulitis/erysipelas.
- Staphylococcus aureus: Produces coagulase, which walls off infection. Typically causes localized, purulent infection (Abscess / Furuncle) with surrounding cellulitis.
3. Host Response & Inflammation:
- Release of cytokines (IL-1, IL-6, TNF-alpha) causes:
- Vasodilation (Erythema / Redness).
- Capillary Leak (Oedema / Swelling).
- Pain receptor sensitisation.
- Systemic fever.
- Clinical Note: The redness often worsens for 24 hours after starting antibiotics due to toxin release from dying bacteria (Jarisch-Herxheimer-like reaction).
Microbiology: The "Best Guess"
| Organism | Frequency | Clinical Context |
|---|---|---|
| Beta-haemolytic Strep (A, B, C, G) | 70-80% | Diffuse, non-purulent, rapid spread. Erysipelas. |
| Staphylococcus aureus (MSSA/MRSA) | 10-20% | Purulent, abscess associated, penetrating trauma, IVDU. |
| Pasteurella multocida | less than 5% | Cat or Dog bites. (Rapid onset less than 24h). |
| Pseudomonas aeruginosa | Rare | Nail puncture through rubber sole (sneaker). Hot tub folliculitis. |
| Aeromonas hydrophila | Rare | Fresh water exposure / Leech therapy. |
| Vibrio vulnificus | Rare | Sea water exposure (coral cut) + Liver disease. Lethal. |
| Eikenella corrodens | Rare | Human bites ("Fight bite"). |
Virulence Factors
- M Protein (Strep): Anti-phagocytic surface protein. Prevents opsonisation.
- Panton-Valentine Leukocidin (PVL): Produced by some Staph strains (especially CA-MRSA). Causes leukocyte destruction and tissue necrosis. Leads to recurrent, necrotic abscesses ("Spider bite" lesions).
- Superantigens: Pyrogenic exotoxins A-C. Cause Toxic Shock Syndrome (TSS).
4. Clinical Presentation
Symptoms
- Pain: Variable. Severe pain suggests deep involvement.
- Fever/Chills: Often precede the rash (especially in Strep erysipelas).
- Swelling: Tightness of the limb.
- Malaise: "Flu-like" prodrome.
Examination Signs
The Four Cardinal Signs of Inflammation:
- Rubor (Redness): Erythema.
- Erysipelas: Bright red, raised edge, sharp border. Face/Legs.
- Cellulitis: Darker red, indistinct border.
- Calor (Heat): Compare with contralateral limb using back of hand.
- Tumor (Swelling): Pitting oedema. Loss of skin wrinkles.
- Dolor (Pain): Tenderness on palpation.
Systemic Signs (SEPSIS ALERT): Look for end-organ dysfunction.
- Slurred speech or confusion.
- Extreme shivering or muscle pain.
- Passing no urine (in a day).
- Severe breathlessness.
- It feels like you might die.
- Skin mottled or discolored.
Red Flags for Necrotising Fasciitis
Seek immediate surgical opinion if:
- Pain out of proportion to physical illness (e.g., patient screaming but leg looks mildly pink).
- Anaesthesia: Numbness over the area (nerves destroyed).
- Rapid progression: Marking moves visibly over hours.
- Hard woody feel: Indurated subcutaneous tissue.
- Crepitus: Gas under skin (Late sign).
- Skin Necrosis: Grey/Purple patches or Dusky skin.
- Hemodynamic instability: Septic shock.
5. Differential Diagnosis (The Mimics)
"All that glistens is not gold; All that is red is not Cellulitis." Misdiagnosis rate is estimated at 30%.
| Condition | Distinguishing Features |
|---|---|
| Lipodermatosclerosis (Varicose Eczema) | Bilateral. Chronic. Hyperpigmentation (haemosiderin). Inverted "Champagne Bottle" legs. Itch prominent. Afebrile. |
| Deep Vein Thrombosis (DVT) | Unilateral. Swelling predominant. Redness is usually dusky/cyanotic, not bright red. Pain is deep cramp. No fever. |
| Gout (Acute) | Joint based (MTP/Ankle). Rapid onset (overnight). Exquisite tenderness. History of gout. |
| Contact Dermatitis | Itchy. Vesicles/weeping. Clear demarcation at allergen contact site (e.g., Elastoplast allergy). |
| Drug Reaction (Fixed Drug Eruption) | Recurrent round/oval patches. History of drug. |
| Erythema Nodosum | Tender, bruised nodules. Shins (bilateral). Associated with Sarcoid/IBD/Tb. |
| Lyme Disease (Erythema Migrans) | "Bullseye" target lesion. Tick bite history. Spreading ring. |
| Pyoderma Gangrenosum | Ulcer with purple, overhanging, undermined edge. Very painful. Assoc with IBD/RA. (often misdiagnosed as infected ulcer). |
6. Investigations
Do we need them?
Simple Class I Cellulitis: Clinical diagnosis. No investigations needed.
Laboratory
- FBC: Leukocytosis (Neutrophilia).
- CRP: Marker of severity and response. If > 200, suspect abscess or deep collection.
- Blood Cultures:
- Low yield in simple cellulitis (less than 5% positive).
- Mandatory in: Sepsis, Class III/IV, Immuno-compromised, Salt water exposure.
- Swabs:
- Intact skin: Useless (grows commensals). Do NOT swab.
- Broken skin/Ulcer: Swab base after cleaning with saline.
- Blister fluid: Aspirate (high yield).
- CK: To rule out Myositis / Nec Fasc.
- Lactate: Sepsis screen.
Imaging
- X-Ray: Look for gas (Nec Fasc), foreign body (glass/metal), or osteomyelitis (if chronic ulcer).
- Ultrasound:
- Rule out DVT (Compressibility).
- Identify Abscess (Hypoechoic collection) requiring drainage.
- MRI: Gold standard for Osteomyelitis or deep Necrotising Fasciitis if diagnosis unclear.
7. Management
Management Algorithm
PATIENT WITH RED LEG
↓
┌─────────────────────────────────────────────────────┐
│ EXCLUDE MIMICS (30% cases) │
│ - Is it bilateral? -> Venous Eczema (Steroids) │
│ - Is it DVT? -> Wells Score / D-Dimer │
└─────────────────────────────────────────────────────┘
↓
ASSESS SEVERITY (ERON)
↓
┌───────────────┬─────────────────┬───────────────────┐
│ CLASS I │ CLASS II │ CLASS III / IV │
│ (No Sepsis) │ (Systemic upset)│ (Unstable / Fast) │
└───────┬───────┴────────┬────────┴─────────┬─────────┘
│ │ │
│ │ │
┌───────▼───────┐ ┌──────▼────────┐ ┌───────▼───────┐
│ ORAL THERAPY │ │ IV OPTION / │ │ ADMIT HOSPITAL│
│ - Fluclox │ │ OPAT │ │ - IV Fluclox │
│ - Elevation │ │ - Ceftriaxone│ │ - BenPen │
│ - Review 48h │ │ - Once daily │ │ - Fluids │
└───────────────┘ └───────────────┘ └───────┬───────┘
│
SURGICAL R/V?
(If Nec Fasc)
1. Antibiotic Therapy
A. Standard Empirical Therapy (Staph/Strep) Guidance based on CREST / NICE.
Oral (Class I):
- First Line: Flucloxacillin 500mg-1g QDS. (Empty stomach).
- Penicillin Allergy:
- Mild: Clarithromycin 500mg BD or Erythromycin.
- Severe: Doxycycline 100mg BD or Clindamycin 300-450mg QDS.
Intravenous (Class III/IV):
- First Line: Flucloxacillin 2g QDS IV. (Often combined with Benzylpenicillin 1.2g QDS for synergistic Strep killing).
- Penicillin Allergy:
- Vancomycin (loading dose + levels) OR Teicoplanin.
- Clindamycin 600mg-1.2g IV QDS.
2. Renal Impairment Dosage Table
Dosing adjustment is critical to avoid neurotoxicity (Penicillins) or nephrotoxicity (Vancomycin).
| Antibiotic | eGFR > 50 | eGFR 10-50 | eGFR less than 10 |
|---|---|---|---|
| Flucloxacillin | 2g QDS | 2g QDS | 1g QDS |
| Benzylpenicillin | 1.2g QDS | 1.2g Q6H | 600mg Q6H |
| Clindamycin | No change | No change | No change |
| Doxycycline | No change | No change | No change |
| Vancomycin | 15-20mg/kg BD | By Levels | By Levels |
| Ciprofloxacin | 500mg BD | 500mg BD | 500mg Daily |
B. Specific Scenarios
- Facial Erysipelas: Penicillin V / IV Benzylpenicillin (pure Strep).
- Human/Animal Bite: Co-Amoxiclav (Augmentin) cover Anaerobes/Pasteurella.
- Diabetic Foot: Polymicrobial. Co-Amoxiclav or Pip-Taz.
- Water Exposure: Doxycycline / Ciprofloxacin (cover Vibrio/Aeromonas).
- MRSA History: Vancomycin / Doxycycline / Cotrimoxazole (check sensitivities).
3. Adjunctive Care (Crucial)
A. Elevation
- Line in the sand rule: The limb must be higher than the hip.
- Use a Bradford Sling or bed elevation.
- "Antibiotics don't swim upstream".
B. Marker Pen
- Mark the edge of erythema on admission. Date and time it.
- Review in 24 hours. Note: Redness may expand initially (toxin release) but fever/pain should settle.
C. Skin Care
- Treat the portal of entry.
- Tinea Pedis: Topical Terbinafine / Clotrimazole.
- Eczema: Emollient + Topical Steroid (yes, you can put steroid on infected skin IF covered by antibiotics - controversial but practiced by derm).
4. Recurrence Prevention
| Regimen | Indication | Dose |
|---|---|---|
| Penicillin V | Recurrent Strep Cellulitis | 250mg - 500mg BD |
| Erythromycin | Penicillin Allergic | 250mg BD |
| Azithromycin | Compliance poor | 250mg Daily (3x week) |
- Duration: Trial for 12 months. Review. If relapse after stopping, lifelong.
- Evidence: PATCH trial supports this.
5. Nursing & Wound Management
A. Wound Assessment (T.I.M.E Principle)
- Tissue: Is there viable pink granulating tissue or black necrotic slough?
- Infection: Signs of spreading redness/heat?
- Moisture: Is the wound highly exudative (wet) or dry?
- Edge: Are skin edges advancing (healing) or undermined?
B. Dressing Selection Guide
- High Exudate (Wet, Weeping legs):
- Use: Alginates (Kaltostat), Super-absorbents (Zetuvit), Foams.
- Risk: Maceration of surrounding skin if not absorbed.
- Dry Wounds:
- Use: Hydrogels (Intrasite) to rehydrate.
- Infected Wounds:
- Use: Silver dressings (Acticoat) or Iodine (Inadine) or Medical Honey.
- Note: Do not use Silver for > 2 weeks due to toxicity/resistance.
C. Compression Therapy
- Timing: NEVER compress acute cellulitis (too painful). Wait until infection resolves.
- Safety: MUST check ABPI (Ankle Brachial Pressure Index) first. If less than 0.8, compression is dangerous (Arterial Insufficiency).
- Type: Below knee Class 1 or 2 stockings.
8. Special Clinical Scenarios
(Expanded Section)
A. Necrotising Fasciitis (NSTI)
This is the differential you cannot miss. Infection spreads along the fascial planes, causing widespread necrosis with minimal external signs initially.
- Types:
- Type I: Polymicrobial (Aerobes + Anaerobes). Common in diabetics/post-surgical.
- Type II: Monomicrobial (Group A Strep). Young healthy patients. "Flesh eating bacteria".
- Management:
- Surgery is definitive. Antibiotics are secondary.
- "A cut is worth a thousand scans". If suspected, surgeon enters theatre for exploration.
- Finger Sweep Test: Under local anaesthetic, if finger passes easily along fascial plane with "dishwater pus", diagnosis is confirmed.
LRINEC Score (Laboratory Risk Indicator for Necrotising Fasciitis) Score > 6 suggests NSTI. Score > 8 strongly predictive.
| Parameter | Value | Points |
|---|---|---|
| CRP | > 150 mg/L | 4 |
| less than 150 | 0 | |
| WBC | > 25 | 2 |
| 15-25 | 1 | |
| Haemoglobin | less than 110 g/L | 2 |
| 110-135 | 1 | |
| Sodium | less than 135 mmol/L | 2 |
| Creatinine | > 141 umol/L | 2 |
| Glucose | > 10 mmol/L | 1 |
B. Periorbital vs Orbital Cellulitis
- Pre-septal (Periorbital): Eyelid swollen/red. Eye moves normally. Vision normal. Oral ABx.
- Orbital (Post-septal): Emergency. Pain on eye movement. Proptosis (bulging). Diplopia. RAPD.
- Risk: Cavernous Sinus Thrombosis, Blindness, Meningitis.
- Action: CT Orbits + IV Ceftriaxone + ENT/Ophthalmology urgent r/v.
C. Cellulitis in IVDU (Intravenous Drug Users)
- Risks: Abscess common. "Skin popping". DVT co-existence ("Groin hit").
- Pathogens: MRSA high risk. Anaerobes (licking needle).
- Management: Ultra-low threshold for Ultrasound (to find abscess/DVT). Vancomycin empirical often needed.
9. Complications
Local
- Abscess Formation: Collection of pus. Requires Incision & Drainage (I&D). Antibiotics alone cannot penetrate pus.
- Gangrene / Necrosis: Pressure on microvasculature.
- Bullae: Blistering due to epidermal oedema OR toxin effect.
- Clear fluid: Likely severe oedema / Strep.
- Haemorrhagic (Blood fill): Red Flag for Necrotising Fasciitis or severe Staph.
- Management: Leave intact if possible, or aspirate sterilely. Do not de-roof (pain/infection risk).
Systemic
- Sepsis: Hypotension, AKI.
- Endocarditis: Staph aureus bacteraemia has high seeding risk (10-20%). Check Echo in all Staph bacteraemias.
- Post-Streptococcal Glomerulonephritis: Renal failure weeks after Strep infection.
Long Term
- Chronic Lymphoedema: Infection destroys lymphatics -> Lymphoedema -> More Infection.
- Elephantiasis Nostra Verrucosa: Chronic non-pitting oedema with warty hyperkeratotic skin changes.
10. Prognosis & Outcomes
- Response Time:
- Fever/Pain settle in 24-48 hours.
- Redness/Swelling take 7-10 days to resolve. Warn the patient the leg will peel and remain discoloured for weeks.
- Slow Response: Look for Abscess, Osteomyelitis, or Resistant organism.
- Mortality: Low for uncomplicated cases (less than 1%). Increases to 50% for Necrotising Fasciitis or Sepsis in elderly.
- Recurrence: 20-50% recur locally without prophylaxis.
11. Evidence & Guidelines
Guidelines
- CREST Guidelines (2005): Guidelines on the management of cellulitis in adults. (Seminal N.Ireland paper establishing the grading system).
- IDSA Guidelines (2014): Diagnosis and Management of Skin and Soft Tissue Infections. (US Standard). Includes MRSA coverage algorithm.
- NICE CKS (2019): Cellulitis - acute. (UK Primary Care). Flucloxacillin 500mg-1g First line.
- BSAC (British Society for Antimicrobial Chemotherapy): Advice on OPAT (Outpatient Parenteral Antibiotic Therapy) for cellulitis.
Key Trials
-
PATCH I & II Trials (2013): Prophylactic antibiotics for prevention of recurrent cellulitis.
- RCT. Penicillin V 250mg BD vs Placebo.
- Result: Reduced recurrence by 50% while taking drug. Effect lost after stopping.
- Clinical Impact: Supports long-term prophylaxis for recurrent cases. PMID: 23633173.
-
O'Cannon et al (ER visits): showed 30% of "Cellulitis" diagnoses were misdiagnosed (Dermatitis).
- Impact: Emphasis on "Bilateral Red Legs = Dermatology".
-
Examination of Lymphoedema (Soo et al): Demonstrated that compression therapy REDUCES cellulitis recurrence by improving lymphatic drainage (reversing the stagnant pool).
12. Patient Explanation
What is Cellulitis?
It is a bacterial infection of the deeper layers of your skin and fat. The bacteria (usually Strep or Staph) get in through a tiny crack - like athlete's foot, a scratch, or an insect bite.
Why is my leg red and swollen?
Your body enters "war mode" to fight the bacteria. It widens blood vessels (redness) and sends fluid and white blood cells (swelling) to kill the germs. Even after the germs are dead, the fluid takes time to drain away.
Why do I need to keep it up?
Gravity pulls fluid down. If your leg is down, the fluid pools, and the antibiotics can't get to the bugs. You must keep your heel higher than your hip (on a stack of pillows or a sofa arm) for the next 48 hours.
Is it contagious?
No. You cannot catch cellulitis from someone else. It is your own skin bacteria getting into the wrong place.
The Do's and Don'ts of Recovery
- ✅ DO draw a line around the red area to track it.
- ✅ DO keep the leg elevated whenever possible.
- ✅ DO treat the athlete's foot between your toes (cream).
- ❌ DON'T wear compression stockings initially (too painful).
- ❌ DON'T worry if the redness spreads slightly in the first 24h (this is normal).
13. References
-
Phoenix G et al. Diagnosis and management of cellulitis. BMJ. 2012;344:e3951. PMID: 22674913
-
Thomas KS et al (PATCH Trial). Penicillin to prevent recurrent leg cellulitis. N Engl J Med. 2013 May 2;368(18):1695-703. PMID: 23633171
-
Stevens DL et al (IDSA). Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014 Jul 15;59(2):e10-52. PMID: 24973422
-
Hirschmann JV et al. Lower limb cellulitis and its mimics: part I. An overview. J Am Acad Dermatol. 2012 Aug;67(2):163.e1-12. PMID: 22794018 - The seminal paper on Mimics.
-
Eron LJ et al. Classifying the severity of nonpurulent skin and soft tissue infections. J Antimicrob Chemother. 2003;51 Suppl 1:i105-11. (CREST Classification).
-
Wong CH et al (LRINEC). The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004 Jul;32(7):1535-41. PMID: 15241098
14. Examination Focus
Common Questions
- "How to treat Cellulitis in a Penicillin Allergic patient?"
- Answer: Clarify allergy. If mild rash: Cephalosporin (low cross reactivity). If Anaphylaxis: Clarithromycin/Clindamycin or Doxycycline.
- "What is the most common mimic?"
- Answer: Varicose Eczema / Lipodermatosclerosis. (Look for bilateral, haemosiderin, normal CRP).
- "Patient with Cellulitis and new murmur?"
- Answer: Suspect Endocarditis (Staph Aureus). Order Echo and Blood Cultures.
- "What is the LRINEC score?"
- Answer: A scoring system using CRP, WBC, Hb, Na, Creatinine and Glucose to predict Necrotising Fasciitis. Note: Low sensitivity (can miss cases), but high specificity.
ASCII Algorithm: IV to Oral Switch
Day 1: IV Antibiotics + Mark leg
↓
Day 2: Fever resolved? Pain better?
Redness stable?
↙ ↘
YES NO
↓ ↓
Switch Oral Continue IV
Discharge Consider MRI / Escalate
Last Updated: 2026-01-04
Medical Disclaimer: MedVellum content is for educational purposes and clinical reference. Clinical decisions should account for individual patient circumstances. Always consult appropriate specialists and current guidelines.