Liver Cirrhosis
Liver Cirrhosis is the histological end-stage of diverse chronic liver insults, characterised by diffuse hepatic fibrosi... MRCP exam preparation.
What matters first
Liver Cirrhosis is the histological end-stage of diverse chronic liver insults, characterised by diffuse hepatic fibrosi... MRCP exam preparation.
Haematemesis or melaena (Variceal bleed)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Haematemesis or melaena (Variceal bleed)
- New-onset confusion or asterixis (Encephalopathy)
- Abdominal pain + fever (SBP)
- Rapidly rising creatinine (Hepatorenal Syndrome)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Budd-Chiari Syndrome
- Congestive Hepatopathy
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Liver Cirrhosis (Adult)
1. Overview
Liver Cirrhosis is the histological end-stage of diverse chronic liver insults, characterised by diffuse hepatic fibrosis, nodular regeneration, and the catastrophic distortion of normal vascular architecture. It represents a state of total system failure where the liver's biosynthetic, metabolic, and filtration capacities are progressively lost. [1]
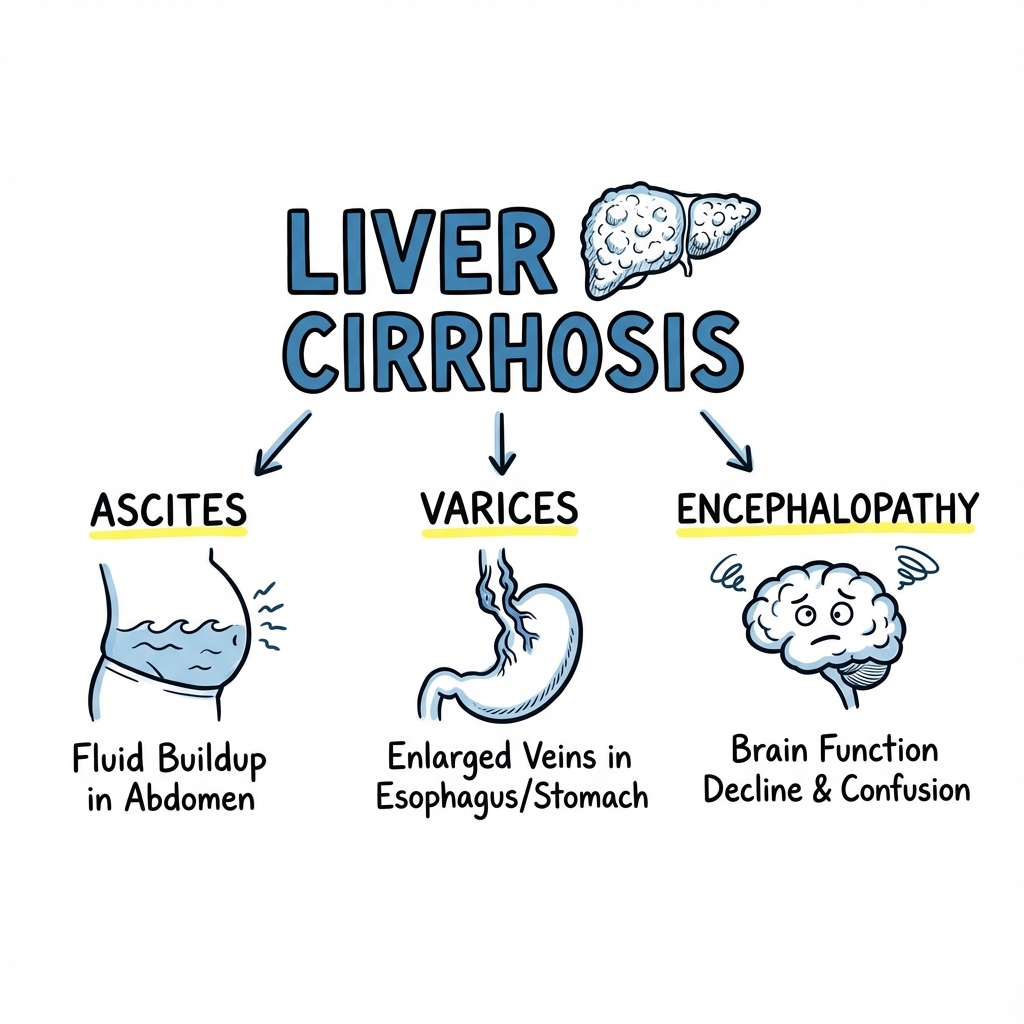
The 2023-2024 global consensus has shifted nomenclature from NAFLD to MASLD (Metabolic Dysfunction-Associated Steatotic Liver Disease), reflecting the underlying metabolic driver. Cirrhosis is no longer viewed as a static "scarred" state but as a dynamic condition: Compensated (median survival > 12 years) and Decompensated (median survival less than 2 years), defined by the onset of ascites, variceal haemorrhage, or encephalopathy. [2]
Management has been refined by the MELD-Na 3.0 score for transplant prioritisation and the aggressive use of Terlipressin and Albumin for renal protection. In suitable candidates, Liver Transplantation is the only definitive cure, offering 5-year survival rates exceeding 75%. [3]
2. Epidemiology
The Global Burden
- Mortality: Cirrhosis causes 1.3 million deaths annually (2.4% of global deaths).
- The "Rising Tide": While viral hepatitis (C) is declining due to DAA therapy, MASLD and Alcohol-related Liver Disease (ArLD) are rising rapidly, particularly post-COVID.
Geographic Variation
| Driver | Region | Clinical Note |
|---|---|---|
| Hepatitis B | Sub-Saharan Africa / SE Asia | High risk of early HCC. |
| Alcohol | Europe / North America | Acute-on-Chronic (ACLF) risk is high. |
| MASLD | Middle East / USA | Linked to BMI and Type 2 Diabetes. |
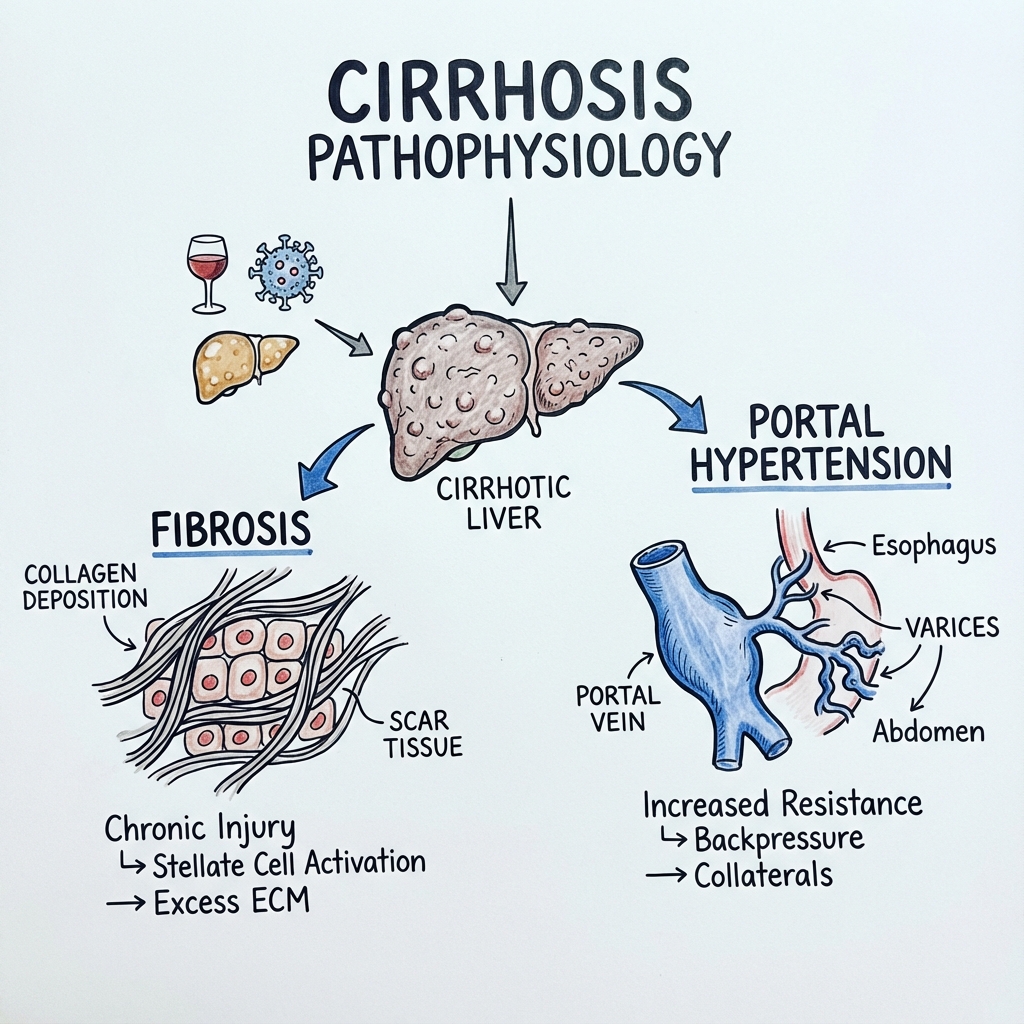
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- Hepatocyte Injury: Chronic insult (ethanol metabolites, viral proteins, or lipid peroxidation) causes hepatocyte apoptosis and the release of DAMPs (Damage-Associated Molecular Patterns).
- Kupffer Cell Activation: Resident macrophages (Kupffer cells) detect DAMPs and release pro-inflammatory cytokines, specifically TNF-α and TGF-β1.
- Stellate Cell Activation (The Key Switch): Quiescent Hepatic Stellate Cells (HSCs) in the Space of Disse transform into myofibroblast-like cells. This is driven by PDGF (migration) and TGF-β1 (fibrogenesis).
- Excessive ECM Deposition: Activated HSCs produce massive amounts of Type I and III collagen. This "caps off" the sinusoids (Sinusoidal Capillarisation), destroying the fenestrae that allow nutrient exchange.
- Vascular Distortion & Resistance: Fibrotic bands contract, compressing the portal venules and increasing intrahepatic resistance.
- Portal Hypertension: As intrahepatic resistance rises, portal pressure exceeds 10-12 mmHg. This leads to the opening of porto-systemic collaterals (Varices) and splenic sequestration (Splenomegaly).
- Systemic Vasodilation: Portal hypertension triggers the release of Nitric Oxide in the splanchnic circulation. This causes massive "Splanchnic Pooling," leading to effective arterial hypovolemia, which activates the RAAS and SNS, precipitating Ascites and Hepatorenal Syndrome. [4, 5, 6]
4. Clinical Presentation
Peripheral Stigmata (CLD Signs)
- Spider Naevi: > 5 in the SVC distribution (indicative of hyperoestrogenism).
- Leukonychia: White nails due to hypoalbuminaemia.
- Palmar Erythema: Blotchy redness of the thenar/hypothenar eminences.
- Gynaecomastia & Testicular Atrophy: In males, due to failure to clear oestrogens.
Decompensation Features
- Ascites: Abdominal distension with shifting dullness (> 1.5L fluid).
- Asterixis (Flapping Tremor): Inability to maintain wrist extension; a sign of Hepatic Encephalopathy.
- Jaundice: Scleral icterus indicates total bilirubin > 35-40 µmol/L.
- Caput Medusae: Dilated veins radiating from the umbilicus (Porto-systemic shunt).
5. Investigations
Laboratory Synthesis
- Synthetic Function: Prothrombin Time (PT/INR) and Albumin. (Note: LFTs/ALT are often normal in established cirrhosis).
- FBC: Thrombocytopenia is the most sensitive marker for portal hypertension (hypersplenism).
- Ascitic Tap: Neutrophil count > 250 cells/mm³ defines Spontaneous Bacterial Peritonitis (SBP).
Non-Invasive Fibrosis Assessment
- FibroScan (Transient Elastography): Measures liver stiffness (kPa). Values > 12-15 kPa strongly suggest cirrhosis.
- APRI / FIB-4 Scores: Validated blood-based calculations to avoid biopsy in many cases.
The Gold Standard
- Liver Biopsy: Shows bridging fibrosis and regenerative nodules. Reserved for cases where aetiology is uncertain.
6. Management: The Complication Algorithm
1. Ascites & SBP
- Ascites: Salt restriction + Spironolactone (target 100mg) ± Furosemide (target 40mg).
- SBP: Immediate IV Cefotaxime/Ceftriaxone + IV Albumin (to prevent HRS). [7]
2. Variceal Bleeding (Red Alert)
- Immediate: Terlipressin + Prophylactic Abx (Ceftriaxone) + Urgent OGD for Banding.
- Long-term: Carvedilol (Non-selective Beta-blocker) reduces portal pressure.
3. Hepatic Encephalopathy
- First-line: Lactulose (aim for 2-3 soft stools/day) to trap ammonia (NH4+).
- Second-line: Rifaximin (non-absorbable antibiotic) to reduce ammonia-producing gut flora.
7. Evidence: Landmark Trials
| Trial | Population | Result | Impact |
|---|---|---|---|
| STOPAH | Alcoholic Hepatitis | Prednisolone > Placebo | Standardised steroid use for AH (Maddrey > 32). |
| PREDESCI | Compensated Cirrhosis | NSBB > Placebo | Proved NSBB prevent decompensation. |
| ATTIRE | Acute Decomp. | Albumin vs. Standard | No benefit for routine albumin titration. |
| FRONTIER | Refractory HE | Rifaximin | Significant reduction in recurrences. |
| HALT-C | Hepatitis C | Maintenance Interferon | No benefit in preventing cirrhosis progression. |
8. Single Best Answer (SBA) Questions
Question 1
A 55-year-old male with cirrhosis and ascites is admitted with abdominal pain and confusion. Ascitic tap: Neutrophils 450/mm³. Creatinine is 180 (baseline 90). What is the most appropriate management?
- A) IV Furosemide
- B) Oral Spironolactone
- C) IV Ceftriaxone + IV Albumin
- D) Large Volume Paracentesis
- E) TIPS procedure
- Answer: C. The patient has SBP (Neutrophils > 250). In SBP, the risk of Hepatorenal Syndrome is high. IV Albumin (1.5g/kg on Day 1) is mandatory to reduce the risk of renal failure and mortality.
Question 2
Which molecular pathway is the primary target for preventing hepatic fibrosis during the transition from MASLD to Cirrhosis?
- A) Beta-oxidation of fatty acids
- B) TGF-β1 mediated Stellate Cell activation
- C) Viral replication of HBV
- D) Gastric acid production
- E) Platelet aggregation in the spleen
- Answer: B. TGF-β1 is the "master regulator" of fibrogenesis, driving quiescent Stellate cells to become collagen-producing myofibroblasts.
9. Viva Scenario: The "Variceal Bleed"
Examiner: "A known cirrhotic presents with massive haematemesis. Their BP is 85/50. Describe your immediate steps."
Candidate:
- Resuscitation: ABC approach. Airway protection (often needs intubation). Restricted volume resuscitation (Target SBP 90, Hb 70-80) to avoid increasing portal pressure.
- Vasoactive Therapy: Start IV Terlipressin or Octreotide immediately (before OGD).
- Infection Prophylaxis: IV Ceftriaxone (reduces mortality and re-bleeding risk).
- Endoscopy: Urgent OGD within 6-12 hours for variceal band ligation (VBL).
- Rescue: If bleeding is uncontrolled, consider a Sengstaken-Blakemore tube or TIPS.
10. Patient Explanation
"Cirrhosis is often called 'scarring of the liver.' Over many years of injury, the liver tissue becomes hard and lumpy, like a dry sponge. This hardness makes it very difficult for blood to flow through the liver, causing the blood to 'back up' into your stomach and spleen (Portal Hypertension). It also means the liver can't perform its 500+ jobs, like cleaning your blood or making important proteins. Our goal is to stop any further damage by avoiding alcohol/treating viruses, and to manage the 'leaks' (fluid in the belly) using water tablets."
11. References
- EASL. Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018. [PMID: 29653741]
- Rinella ME, et al. A multi-society Delphi consensus on steatotic liver disease nomenclature. Hepatology. 2023. [PMID: 37363822]
- Kim WR, et al. MELD-Na 3.0: Refinement of the MELD score for liver transplant allocation. Gastroenterology. 2021. [PMID: 34144043]
- Thursz MR, et al. Prednisolone or Pentoxifylline for Alcoholic Hepatitis (STOPAH). N Engl J Med. 2015. [PMID: 25901427]
- Villanueva C, et al. Beta-blockers to prevent decompensation of cirrhosis (PREDESCI). Lancet. 2019. [PMID: 30935736]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for liver cirrhosis?
Seek immediate emergency care if you experience any of the following warning signs: Haematemesis or melaena (Variceal bleed), New-onset confusion or asterixis (Encephalopathy), Abdominal pain + fever (SBP), Rapidly rising creatinine (Hepatorenal Syndrome), Acute jaundice in a known cirrhotic (ACLF).
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Budd-Chiari Syndrome
- Congestive Hepatopathy
Consequences
Complications and downstream problems to keep in mind.