COPD Exacerbation
An Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) is defined by the GOLD 2024 Report as an event c... MRCP exam preparation.
What matters first
An Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) is defined by the GOLD 2024 Report as an event c... MRCP exam preparation.
Respiratory acidosis (pH less than 7.35)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Respiratory acidosis (pH less than 7.35)
- New-onset confusion or drowsy (CO2 narcosis)
- Silent chest or very poor air entry
- Sudden unilateral chest pain (Pneumothorax)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Congestive Heart Failure
- Pneumonia
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
COPD Exacerbation (Adult)
1. Overview
An Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) is defined by the GOLD 2024 Report as an event characterised by increased dyspnoea and/or cough and sputum that worsens in less than 14 days, which may be accompanied by tachypnoea and/or tachycardia and is often associated with increased local and systemic inflammation caused by infection, pollution, or other insults to the airways. [1]
AECOPD is a major driver of mortality and healthcare costs, accounting for over 130,000 hospital admissions annually in the UK. The prognosis after a severe exacerbation remains poor, with 1-year mortality rates approaching 25%, a figure higher than that for many common cancers. [2]
The paradigm of management centres on the rapid reversal of airflow obstruction, suppression of airway inflammation, and, critically, the identification and management of Type 2 Respiratory Failure (T2RF). The introduction of Non-Invasive Ventilation (NIV) as a standard of care for acidotic exacerbations has reduced mortality by 50% in this cohort. [3]
2. Epidemiology
Incidence & Distribution
- Frequency: On average, COPD patients experience 1-2 exacerbations per year. The "frequent exacerbator" phenotype (≥2 per year) is associated with worse quality of life and faster FEV1 decline. [4]
- Seasonality: Marked winter peak, correlating with the prevalence of viral respiratory infections (Rhinovirus, Influenza, RSV).
- Mortality: In-hospital mortality is 3-10%. For those requiring ICU admission, mortality exceeds 15-20%.
Risk Factors for Frequent Exacerbations
| Factor | Relative Risk | Clinical Significance |
|---|---|---|
| History of Exacerbations | Best Predictor | A history of ≥2 exacerbations in the prior year is the strongest predictor of future events. |
| FEV1 less than 50% Predicted | High | Severe airflow obstruction increases vulnerability. |
| Eosinophilia (> 300 cells/µL) | Moderate | Suggests an asthma-COPD overlap or Th2-mediated inflammation; predicts ICS response. |
| Gastroesophageal Reflux | Moderate | Micro-aspiration triggers airway inflammation. |
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- The Trigger: An external insult (Viral/Bacterial infection or Particulate Matter) interacts with the airway epithelium.
- Innate Immune Amplification: Epithelial cells and alveolar macrophages release "alarmins" (IL-1, IL-33) and chemokines (CXCL8/IL-8), which potently recruit Neutrophils and CD8+ T-lymphocytes.
- Neutrophilic Burst: Activated neutrophils release Neutrophil Elastase (NE) and Matrix Metalloproteinases (MMPs), which overwhelm the body's antiprotease defences (Alpha-1 Antitrypsin).
- Mucus Hypersecretion: NE stimulates Goblet Cell Hyperplasia and activates the MUC5AC gene, leading to the production of thick, tenacious mucus that causes widespread "mucus plugging."
- Dynamic Hyperinflation: Worsening airflow obstruction and mucus plugging reduce the time available for exhalation. Air is trapped (Auto-PEEP), forcing the patient to breathe at higher lung volumes, which increases the work of breathing and places the diaphragm at a mechanical disadvantage.
- V/Q Mismatch & Shunt: Inflammation-induced edema and plugging lead to areas of low ventilation relative to perfusion, causing hypoxaemia.
- Muscle Fatigue & T2RF: The combination of high work of breathing, poor gas exchange, and dynamic hyperinflation leads to respiratory muscle exhaustion. This precipitates a fall in alveolar ventilation and a rise in PaCO2 (Respiratory Acidosis). [5, 6]
4. Clinical Presentation
Symptoms (The Cardinal Triad)
- Increased Dyspnoea: Rapidly worsening breathlessness.
- Increased Sputum Volume: Worsening productive cough.
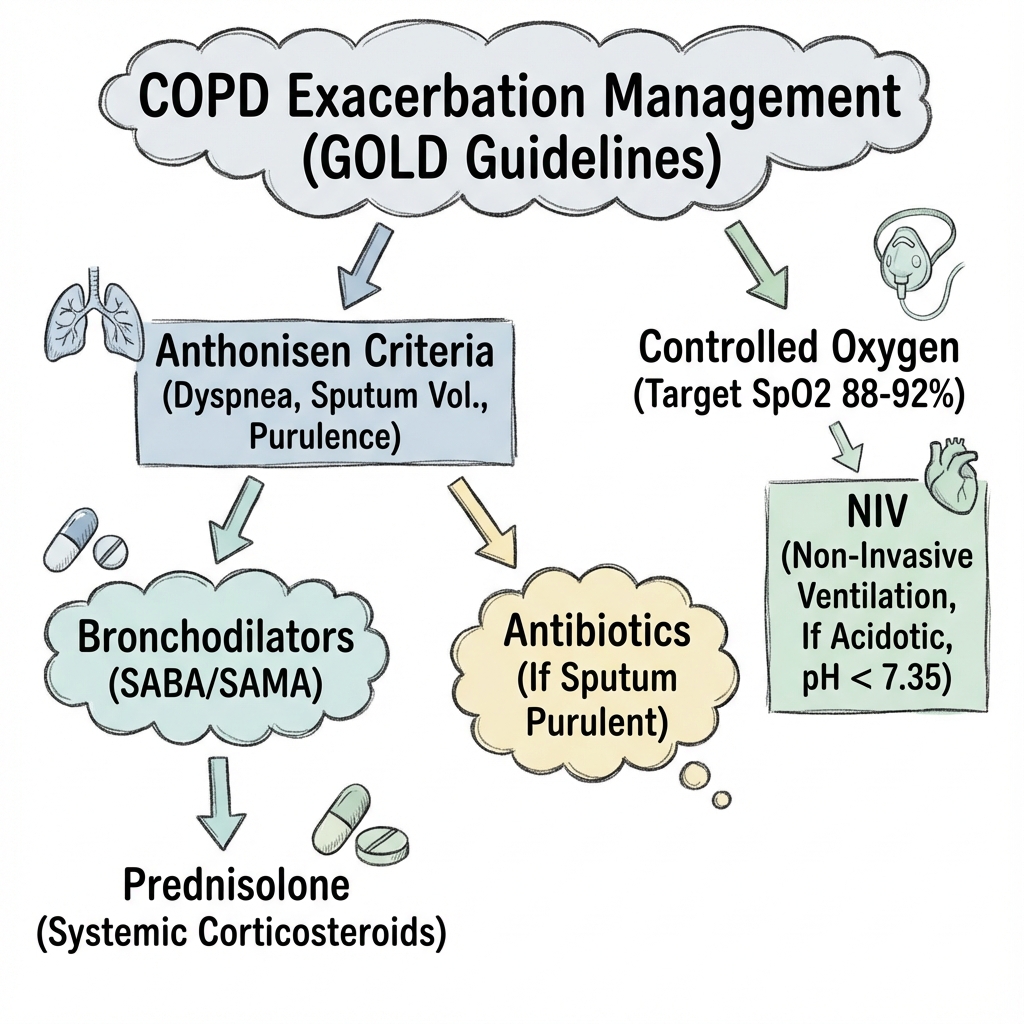
- Increased Sputum Purulence: Change in colour (yellow/green), suggesting bacterial involvement (Anthonisen Criteria). [7]
Physical Signs
- Respiratory: Tachypnoea (> 25/min), accessory muscle use, pursed-lip breathing, widespread expiratory wheeze.
- Life-Threatening Signs: "Silent chest," cyanosis, inability to complete sentences, paradoxical chest wall movement.
- Systemic: Tachycardia, signs of right heart failure (Cor Pulmonale - raised JVP, peripheral oedema).
- Neurological: Drowsiness, flapping tremor (asterixis), and miosis (signs of CO2 narcosis).
5. Investigations
The Gold Standard: Arterial Blood Gas (ABG)
Mandatory in all hospital presentations.
- pH less than 7.35 + PaCO2 > 6.0 kPa: Decompensated T2RF (Respiratory Acidosis) → Urgent NIV indicated.
- pH > 7.35 + PaCO2 > 6.0 kPa: Compensated T2RF (Chronic CO2 retention).
Imaging & Laboratory
- Chest X-Ray: Essential to exclude pneumonia, pneumothorax, or pulmonary oedema. (COPD signs: Hyperinflation, flat diaphragms, bullae).
- ECG: Look for Right Axis Deviation or P-Pulmonale (Right atrial enlargement). Rule out ACS/Arrhythmia.
- FBC: Look for neutrophilia (infection) or eosinophilia (ICS response predictor).
- CRP: Values > 20 mg/L increase the probability of bacterial infection.
6. Management: The Acute Algorithm
Immediate Medical Therapy
- Oxygen: Controlled oxygen via Venturi mask. Target 88-92% (to prevent hyperoxia-induced V/Q mismatch and loss of hypoxic drive).
- Bronchodilators: Salbutamol 5mg + Ipratropium 500mcg nebulised. (Avoid oxygen-driven nebs if CO2 retainer; use air-driven).
- Corticosteroids: Prednisolone 30mg PO daily (or 100mg Hydrocortisone IV) for 5 days. (The REDUCE trial proved 5 days is non-inferior to 14 days). [8]
- Antibiotics: Only if purulent sputum or raised CRP (> 20).
- 1st line: Amoxicillin, Doxycycline, or Clarithromycin.
- Duration: 5 days.
Non-Invasive Ventilation (NIV) - The Life-Saver
Indications (NICE/BTS): Respiratory acidosis (pH 7.25-7.35) despite 1 hour of medical therapy. [9]
- Settings:
- IPAP: Start 10-12 cmH2O (titrate up to 20 to clear CO2).
- EPAP: Start 4-5 cmH2O (splints airways open).
- Success: pH should improve within 1-2 hours. If not, consider escalation to Intubation.
7. Complications
- Pneumothorax: High mortality in COPD. Requires urgent drainage.
- Pulmonary Embolism: Present in up to 15% of AECOPD admissions. Consider if breathlessness is out of proportion to signs.
- Arrhythmias: Multifocal Atrial Tachycardia (MAT) and AF are common due to hypoxia and β-agonist use.
- Myocardial Infarction: Stress of exacerbation triggers Type 2 MI.
8. Evidence: Landmark Trials
| Trial | Population | Intervention | Result | Impact |
|---|---|---|---|---|
| REDUCE (2013) | AECOPD | 5 days vs. 14 days Pred | Non-inferior | Standardised short-course steroids (5 days). |
| Ram Meta-Analysis | AECOPD | NIV vs. Standard Care | Mortality ↓50% | Established NIV as first-line for acidotic AECOPD. |
| DISARM | AECOPD | CRP-guided Antibiotics | Reduced Abx use | Encouraged CRP use to avoid over-prescribing. |
| ETHOS (2020) | Stable COPD | Triple vs. Dual Therapy | Reduced Exacerb. | Established Triple therapy as exacerbation-prevention. |
9. Single Best Answer (SBA) Questions
Question 1
A 68-year-old male with COPD presents with worsening breathlessness. ABG on air: pH 7.28, PaCO2 8.2 kPa, PaO2 6.1 kPa, HCO3 29 mmol/L. He has received nebulisers and steroids. What is the most appropriate next step?
- A) Start high-flow oxygen (15L/min)
- B) Increase Prednisolone to 60mg
- C) Initiate Non-Invasive Ventilation (NIV)
- D) Give 1.2g Co-amoxiclav IV
- E) Arrange urgent Intubation
- Answer: C. The patient has decompensated respiratory acidosis (pH less than 7.35). NIV is the standard of care for this presentation.
Question 2
According to the REDUCE trial, what is the recommended duration of corticosteroid therapy for an acute exacerbation of COPD?
- A) 3 days
- B) 5 days
- C) 10 days
- D) 14 days
- E) 21 days
- Answer: B. 5 days was proven non-inferior to longer courses and reduces steroid-related side effects.
10. Viva Scenario: The "Normal" SpO2 Trap
Examiner: "A patient with COPD is brought in by paramedics with SpO2 of 100% on a non-rebreath mask. They are very drowsy. What is happening and what are your first actions?"
Candidate:
- Diagnosis: This is Oxygen-induced Hypercapnia. High FiO2 has caused V/Q mismatch (loss of hypoxic vasoconstriction), the Haldane effect (CO2 displacement from Hb), and reduced minute ventilation, leading to CO2 narcosis.
- Immediate Actions:
- Reduce FiO2 immediately (aim for 88-92% via Venturi mask).
- Perform an urgent ABG to assess pH and PaCO2.
- Prepare for NIV if acidosis is present.
- Exclude other causes of coma (Glucose, CT Head).
11. Patient Explanation
"A COPD flare-up is like having a blockage in your breathing tubes. Not only are the tubes tighter, but they are also filled with thick mucus, making it very hard to push air out. Think of it like trying to breathe through a straw that's partially clogged. The 'steroid' tablets we give you act like a sponge to soak up the inflammation, and the 'nebulisers' help relax the muscles around the tubes. If your carbon dioxide levels get too high, we use a special tight mask (NIV) to help your lungs do the hard work of pumping air while you recover."
12. References
- GOLD 2024 Report. Global Strategy for the Diagnosis, Management, and Prevention of COPD. GOLD
- Leuppi JD, et al. Short-term vs conventional glucocorticoid therapy in acute exacerbations of COPD (REDUCE). JAMA. 2013. [PMID: 23695200]
- Ram FS, et al. Non-invasive positive pressure ventilation for COPD exacerbations. Cochrane Database Syst Rev. 2004. [PMID: 15266518]
- Wedzicha JA, et al. Mechanisms and impact of the frequent exacerbator phenotype in COPD. BMC Med. 2013. [PMID: 23938011]
- O'Driscoll BR, et al. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax. 2017. [PMID: 28507176]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for copd exacerbation?
Seek immediate emergency care if you experience any of the following warning signs: Respiratory acidosis (pH less than 7.35), New-onset confusion or drowsy (CO2 narcosis), Silent chest or very poor air entry, Sudden unilateral chest pain (Pneumothorax), Haemodynamic instability (Shock).
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Congestive Heart Failure
- Pneumonia
- Pulmonary Embolism
Consequences
Complications and downstream problems to keep in mind.
- Type 2 Respiratory Failure
- Cor Pulmonale