Deep Vein Thrombosis (DVT)
Deep Vein Thrombosis (DVT) is a common and potentially life-threatening condition involving the formation of a thrombus ... MRCP exam preparation.
What matters first
Deep Vein Thrombosis (DVT) is a common and potentially life-threatening condition involving the formation of a thrombus ... MRCP exam preparation.
Sudden dyspnoea or pleuritic pain (PE)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Sudden dyspnoea or pleuritic pain (PE)
- Phlegmasia cerulea dolens (cyanosis, ischaemia)
- Phlegmasia alba dolens (pallor, pulselessness)
- Massive swelling extending to the groin
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Cellulitis
- Ruptured Baker's Cyst
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Deep Vein Thrombosis (Adult)
1. Overview
Deep Vein Thrombosis (DVT) is a common and potentially life-threatening condition involving the formation of a thrombus within the deep venous system, most frequently in the lower extremities. It constitutes one end of the Venous Thromboembolism (VTE) spectrum, with Pulmonary Embolism (PE) being the most feared acute complication. [1]
The clinical significance of DVT resides in its "dual threat": acutely, it is the primary source of fatal PE (occurring in up to 50% of untreated proximal DVTs); chronically, it leads to Post-Thrombotic Syndrome (PTS) in 20-50% of patients, causing permanent venous hypertension, chronic pain, and ulceration. [2]
Management has been revolutionised by the DOAC (Direct Oral Anticoagulant) era, which has replaced Warfarin as the first-line therapy for most patients. The current standard of care emphasizes the use of validated clinical prediction rules (Wells Score) and the transition toward personalized durations of therapy based on the "Provoked vs. Unprovoked" paradigm. [3]
2. Epidemiology
Incidence and Burden
- Stats: Affects ~1 in 1,000 adults annually. The risk doubles with each decade after the age of 40.
- The "Preventable Death": VTE remains the leading cause of preventable hospital death worldwide.
- Cancer Association: Active malignancy increases VTE risk 4- to 7-fold. Cancer-Associated Thrombosis (CAT) now accounts for 20% of all VTE cases. [4]
Genetic Predisposition
| Condition | Prevalence (Caucasians) | Relative Risk (Heterozygous) |
|---|---|---|
| Factor V Leiden | 3-7% | 3x to 5x |
| Prothrombin G20210A | 2-3% | 2x to 3x |
| Protein C/S Deficiency | Rare | 7x to 10x |
| Antithrombin III Def. | Very Rare | 20x to 50x |
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- Endothelial Activation: Stasis in venous valve pockets leads to local hypoxia. This triggers the endothelium to express P-selectin and Von Willebrand Factor (vWF) instead of its usual anticoagulant proteins.
- Leukocyte Recruitment: Circulating monocytes and neutrophils bind to P-selectin. Monocytes express Tissue Factor (TF), initiating the extrinsic coagulation cascade.
- NETosis (The Scaffold): Neutrophils in the valve pocket undergo "NETosis," releasing Neutrophil Extracellular Traps—webs of DNA and histones. These provide a physical scaffold for platelet adhesion and activate the intrinsic pathway (Factor XII).
- Thrombin Burst: The convergence of the extrinsic and intrinsic pathways leads to a massive generation of Thrombin (Factor IIa), which converts soluble fibrinogen into a dense Fibrin mesh.
- Red Thrombus Formation: Unlike arterial "white" thrombi, the slow flow in veins allows for the massive entrapment of Erythrocytes within the fibrin mesh, creating the characteristic "Red Thrombus."
- Thrombus Propagation: The clot grows proximally. Mechanical stress can cause the "free-floating" proximal end to break loose, embolising through the right heart to the pulmonary arteries.
- Valve Destruction & Remodelling: As the thrombus "organises," it triggers an inflammatory surge. Matrix Metalloproteinases (MMPs) degrade the delicate venous valves, leading to permanent valvular incompetence and Chronic Venous Hypertension (the basis of PTS). [5, 6]
4. Clinical Presentation
Symptoms
- Unilateral Leg Swelling: The most common and sensitive sign.
- Dull Ache/Cramp: Often in the calf, worse on weight-bearing.
- Phlegmasia Cerulea Dolens: A "Blue, swollen, ischaemic" limb. This is a surgical emergency representing massive iliofemoral occlusion.
The Wells Score (DVT Likelihood)
| Feature | Points |
|---|---|
| Active Cancer | +1 |
| Paralysis/Immobilisation | +1 |
| Bedridden > 3 days / Major Surgery | +1 |
| Tenderness along deep veins | +1 |
| Entire leg swollen | +1 |
| Calf swelling > 3cm (10cm below tuberosity) | +1 |
| Pitting Oedema (symptomatic leg) | +1 |
| Collateral superficial veins | +1 |
| Alternative diagnosis more likely | -2 |
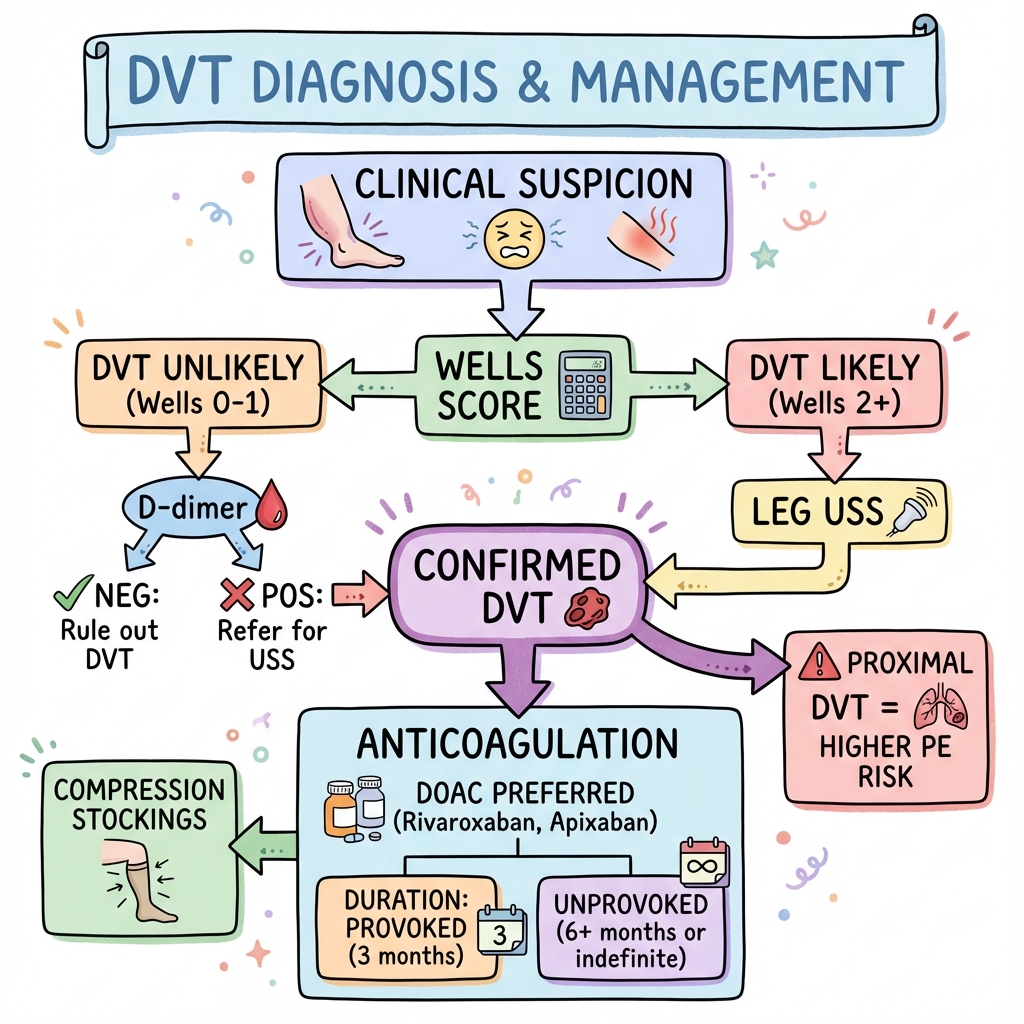
Interpretation: Score ≥2 = DVT Likely (Proceed directly to Ultrasound). Score less than 2 = Unlikely (Proceed to D-dimer). [7]
5. Investigations
The "Exclusion" Tool: D-dimer
- High Sensitivity: D-dimer has a negative predictive value (NPV) of > 99% in low-probability patients.
- The Age-Adjustment Rule: For patients > 50 years, use Age x 10 µg/L as the cut-off (reduces false positives). [8]
The Gold Standard: Duplex Ultrasound
- Criteria: Loss of compressibility of the vein is the primary diagnostic finding.
- The "Serial" Rule: If the Wells score is high but the initial US is negative, a repeat US in 5-7 days is mandatory to catch propagating distal clots. [9]
6. Management: The Anticoagulation Protocol
1. The DOAC Era (First-Line)
- Apixaban: 10mg BD for 7 days, then 5mg BD. (Lowest bleeding risk).
- Rivaroxaban: 15mg BD for 21 days, then 20mg OD.
- Dabigatran/Edoxaban: Requires a 5-day lead-in with LMWH before starting the oral drug. [10]
2. Cancer-Associated Thrombosis (CAT)
The CARAVAGGIO and SELECT-D trials have established DOACs (Apixaban/Rivaroxaban) as non-inferior to LMWH, except in luminal GI or GU cancers where bleeding risk is higher. [11]
3. Duration of Therapy
- Provoked (Transient risk factor): 3 months.
- Unprovoked (First episode): At least 6 months; then assess for Indefinite Anticoagulation based on the "HERDOO2" or "DASH" scores.
- The "EINSTEIN-CHOICE" Pearl: For long-term prevention, Rivaroxaban 10mg OD is as effective as 20mg but with less bleeding. [12]
7. Complications: Post-Thrombotic Syndrome (PTS)
PTS affects up to 50% of patients.
- Symptoms: Chronic heaviness, pain, and venous claudication.
- Signs: Hyperpigmentation (haemosiderin), Lipodermatosclerosis, and Venous Ulcers.
- Prevention: Early mobilisation and effective anticoagulation. The SOX trial proved that routine compression stockings do not prevent PTS, though they aid symptom control. [13]
8. Evidence: Landmark Trials
| Trial | Population | Intervention | Result | Impact |
|---|---|---|---|---|
| EINSTEIN-DVT | DVT | Rivaroxaban vs. VKA | Non-inferior | Validated DOACs for DVT treatment. |
| AMPLIFY | DVT/PE | Apixaban vs. VKA | ↓ 69% Major Bleed | Established Apixaban's safety profile. |
| CARAVAGGIO | Cancer VTE | Apixaban vs. Dalteparin | Non-inferior | Shifted CAT management to DOACs. |
| ATTRACT | Iliofemoral | Thrombolysis + AC | No ↓ in PTS | Limited lysis to limb-threatening cases. |
| EINSTEIN-CHOICE | Long-term | 10mg vs. 20mg Riva | 10mg Effective | Standardised low-dose long-term secondary prev. |
9. Single Best Answer (SBA) Questions
Question 1
A 65-year-old male with a recent knee replacement (2 weeks ago) presents with unilateral calf swelling. His Wells score is 3. An initial duplex ultrasound is negative. What is the most appropriate next step?
- A) Discharge with reassurance
- B) Perform a D-dimer
- C) Start Apixaban immediately
- D) Repeat duplex ultrasound in 5-7 days
- E) Perform a CT Venogram
- Answer: D. In high-probability patients (Wells ≥2) with a negative initial ultrasound, a repeat scan is mandatory to detect any distal (calf) thrombus that may have propagated proximally.
Question 2
A 40-year-old female with an unprovoked proximal DVT has completed 6 months of treatment. She is keen to stop anticoagulation. Which finding would most strongly support a decision for indefinite anticoagulation?
- A) Heterozygous Factor V Leiden
- B) Elevated D-dimer 1 month after stopping treatment
- C) Persistent clot on ultrasound at 6 months
- D) Negative family history
- E) Female sex
- Answer: B. A positive D-dimer after stopping anticoagulation for unprovoked VTE is the most powerful predictor of recurrence and warrants a discussion regarding indefinite therapy.
10. Viva Scenario: The "Cancer" Conundrum
Examiner: "Your patient has a new DVT and was recently diagnosed with a high-grade Gastric Adenocarcinoma. Which anticoagulant would you choose and why?"
Candidate:
- Guideline Shift: While DOACs are generally first-line for Cancer-Associated Thrombosis (CAT), they are associated with a higher risk of major GI bleeding in patients with intact luminal GI tumours.
- Choice: I would choose Low Molecular Weight Heparin (LMWH), such as Dalteparin (CLOT trial protocol).
- Rationale: LMWH avoids the mucosal bleeding risk seen with Rivaroxaban/Edoxaban in the SELECT-D and Hokusai VTE Cancer trials.
- Monitoring: I would monitor for thrombocytopenia (HIT) and check renal function, adjusting the dose if CrCl falls.
11. Patient Explanation
"A DVT is a blood clot that has formed in the deep veins of your leg, usually because the blood has slowed down or become 'sticky.' The danger is that a piece of this clot can break off and travel to your lungs, which is a life-threatening emergency. We use 'blood thinners' to stop the clot from getting bigger and to let your body's natural systems dissolve it over time. You will need to take these for at least 3 to 6 months. It is very important that you keep walking—moving your leg helps the blood flow and prevents the long-term 'heavy leg' syndrome."
12. References
- Kearon C, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline. Chest. 2016. [PMID: 26867832]
- Agnelli G, et al. Oral Apixaban for the Treatment of Acute VTE (AMPLIFY). N Engl J Med. 2013. [PMID: 23808929]
- Agnelli G, et al. Apixaban for the Treatment of VTE in Patients with Cancer (CARAVAGGIO). N Engl J Med. 2020. [PMID: 32223112]
- Weitz JI, et al. Rivaroxaban or Aspirin for Extended Treatment of VTE (EINSTEIN-CHOICE). N Engl J Med. 2017. [PMID: 28316319]
- Ortel TL, et al. American Society of Hematology 2020 guidelines for management of VTE. Blood Adv. 2020. [PMID: 33044451]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for deep vein thrombosis (dvt)?
Seek immediate emergency care if you experience any of the following warning signs: Sudden dyspnoea or pleuritic pain (PE), Phlegmasia cerulea dolens (cyanosis, ischaemia), Phlegmasia alba dolens (pallor, pulselessness), Massive swelling extending to the groin, Evidence of compartment syndrome.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Cellulitis
- Ruptured Baker's Cyst
Consequences
Complications and downstream problems to keep in mind.
- Post-Thrombotic Syndrome
- CTEPH