Hyperkalaemia (Emergency)
Hyperkalaemia is a life-threatening electrolyte emergency defined by a serum potassium concentration 5.5 mmol/L. It is... MRCP exam preparation.
What matters first
Hyperkalaemia is a life-threatening electrolyte emergency defined by a serum potassium concentration 5.5 mmol/L. It is... MRCP exam preparation.
Peaked T-waves or QRS widening on ECG
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Peaked T-waves or QRS widening on ECG
- Potassium less than 6.5 mmol/L (Severe)
- Ascending muscle weakness or paralysis
- Sustained bradycardia or high-grade AV block
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Pseudohyperkalaemia
- Hyperacute T-waves (STEMI)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Hyperkalaemia (Adult)
1. Overview
Hyperkalaemia is a life-threatening electrolyte emergency defined by a serum potassium concentration > 5.5 mmol/L. It is the most lethal metabolic disturbance in clinical medicine, capable of precipitating sudden cardiac arrest (asystole or VF) with little or no clinical warning. [1]
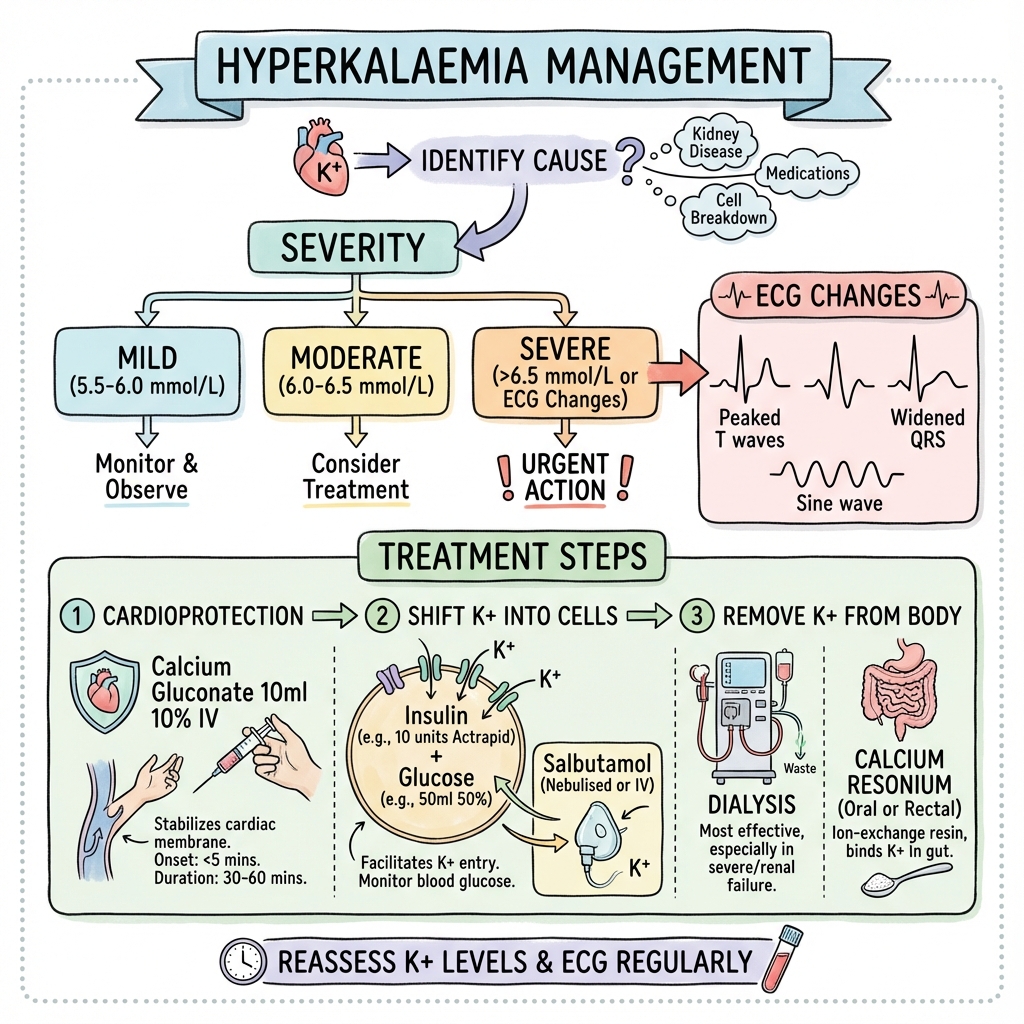
The condition is broadly categorized by severity:
- Mild: 5.5–5.9 mmol/L.
- Moderate: 6.0–6.4 mmol/L.
- Severe: ≥6.5 mmol/L (or any level with ECG changes). [2]
The paradigm of management follows the "Stabilize, Shift, and Eliminate" triad. The 2020-2024 guidelines from the Renal Association (UK) and ERC emphasize the importance of immediate cardiac stabilization with Calcium, the risk of iatrogenic hypoglycemia during insulin-glucose shifting, and the emergence of fast-acting oral binders like Sodium Zirconium Cyclosilicate (Lokelma). [3]
2. Epidemiology
The Hospital Context
- Prevalence: Found in up to 10% of all hospitalized patients.
- The "RAASi Trap": The rise in the use of ACE-inhibitors, ARBs, and MRAs for Heart Failure and CKD has led to a parallel rise in chronic and acute hyperkalaemia.
- Mortality: Severe hyperkalaemia carries a pre-hospital mortality of ~30% if untreated. [4]
Risk Factors for Spurious Results (Pseudohyperkalaemia)
Always exclude pseudohyperkalaemia if the patient is asymptomatic and the ECG is normal:
- Haemolysis: Traumatic venepuncture or "fist-clenching" during draw.
- Thrombocytosis (> 500): Potassium released from platelets during clotting in the tube.
- Leukocytosis (> 50): Leakage from white cells if the sample is delayed.
- Action: Repeat the sample via a lithium-heparin (green top) tube or check a VBG. [5]
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM (Cardiac Toxicity)
- Reduced Transmembrane Gradient: According to the Nernst Equation, the resting membrane potential ($V_m$) of cardiomyocytes is determined by the ratio of intracellular to extracellular K+.
- Depolarisation of Vm: High extracellular K+ makes the Vm less negative (moving from -90mV to -70mV). This brings the cell closer to the Threshold Potential (Vth).
- Sodium Channel Inactivation: Paradoxically, persistent mild depolarisation inactivates fast voltage-gated Na+ channels. This slows the Phase 0 upstroke of the action potential.
- Conduction Velocity Delay: Slowed Phase 0 results in delayed conduction through the specialized system and myocardium, manifesting as PR prolongation and QRS widening.
- Accelerated Repolarisation: High extracellular K+ increases the conductance of the IKr (Rapidly Activating Delayed Rectifier K+) channel. This results in the characteristic Tall, Peaked T-waves.
- Membrane Destabilisation: As Vm and Vth converge, the cell enters a state of persistent "refractoriness," leading to high-grade AV block and "Sine Wave" morphology.
- Cardiac Standstill: Eventually, the myocardium becomes totally inexcitable, resulting in ventricular standstill in diastole (Asystole) or fragmented VF. [6, 7]
4. Clinical Presentation
The "Great Pretender"
Hyperkalaemia is famously asymptomatic until the "pre-arrest" stage. When symptoms do occur, they are often non-specific:
- Muscle Weakness: Ascending flaccid paralysis (resembling Guillain-Barré).
- Paraesthesia: Perioral or limb-based.
- Nausea & Vomiting: Common in the context of AKI.
Physical Signs of Cause
- Crush Injuries: Signs of rhabdomyolysis or compartment syndrome.
- Addisonian Stigmata: Hyperpigmentation or postural hypotension.
- Renal Failure Signs: AV fistula, dialysis catheter, or uraemic rub. [8]
5. Investigations: ECG Mastery
The Progression of ECG Changes
- K+ 5.5-6.5: Tall, Peaked T-waves. (Narrow base, symmetric, "Eiffel Tower" shape).
- K+ 6.5-7.5: P-wave flattening, PR prolongation, and ST depression.
- K+ 7.5-8.5: QRS Widening. The QRS begins to merge with the T-wave.
- K+ > 8.5: Sine Wave pattern. Pre-terminal; impending VF/Asystole. [9]
Diagnostic Workup
- VBG (Venous Blood Gas): Mandatory for immediate K+ result within 5 minutes.
- U&Es: Gold standard lab confirmation.
- Creatine Kinase (CK): To rule out rhabdomyolysis.
- Cortisol/ACTH: If Addison's suspected.
6. Management: The Emergency Protocol
1. Membrane Stabilization (STABILIZE)
- Agent: Calcium Gluconate 10% 30mL IV over 10 minutes (or Calcium Chloride 10mL).
- Effect: Antagonizes the membrane effect of K+ by shifting the threshold potential. Does not lower K+.
- Onset: 1-3 minutes. Duration: 30-60 minutes.
2. Intracellular Shifting (SHIFT)
- Insulin-Glucose: 10 units Actrapid in 50mL 50% Dextrose.
- 2024 Safety Update: Monitor blood glucose at 0, 15, 30, 60, and 120 mins to catch delayed iatrogenic hypoglycemia (occurring in 15% of patients). [10]
- Salbutamol: 10-20mg via nebuliser. (Additive effect to insulin).
3. Removal from Body (ELIMINATE)
- Diuretics: IV Furosemide (if patient is producing urine).
- Oral Binders: Sodium Zirconium Cyclosilicate (Lokelma) 10g TDS. Onset within 1 hour; highly effective for non-life-threatening severe K+.
- Haemodialysis: The definitive treatment for refractory K+ or anuric AKI. [11]
7. Evidence: Landmark Trials
| Trial | Population | Intervention | Result | Impact |
|---|---|---|---|---|
| HARMONIZE | Hyperkalaemia | Lokelma (ZS-9) | Rapid ↓ in K+ | Established Lokelma as standard for acute/chronic. |
| AMETHYST | CKD + T2DM | Patiromer | Safe control | Validated long-term K+ management on RAASi. |
| DIAMOND | Heart Failure | Patiromer vs Plab | Permitted MRA use | Proved binders "enable" GDMT in HF patients. |
| Cochrane '15 | Acute HK | Salbutamol + Ins | Superior to mono | Standardised combination shifting therapy. |
8. Single Best Answer (SBA) Questions
Question 1
A 72-year-old male with anuria and AKI is found to have a potassium of 7.2 mmol/L. His ECG shows a widened QRS but he is currently stable. What is the single most important immediate step?
- A) Start a 10-unit insulin infusion
- B) Arrange for emergency haemodialysis
- C) Give 30mL of 10% Calcium Gluconate IV
- D) Administer 10g of Sodium Zirconium Cyclosilicate
- E) Give 20mg nebulised Salbutamol
- Answer: C. In the presence of QRS widening (ECG changes), immediate cardiac membrane stabilization with Calcium is the absolute priority to prevent cardiac arrest, preceding all other interventions.
Question 2
What is the primary mechanism by which hyperkalaemia causes "tented" T-waves on an ECG?
- A) Slowed conduction in the Bundle of His
- B) Delayed opening of Calcium channels
- C) Increased conductance of the IKr potassium channel
- D) Inactivation of the Na+/K+ ATPase pump
- E) Shortening of the PR interval
- Answer: C. High extracellular K+ paradoxically increases the efficiency of the IKr (rectifier) channel, leading to faster Phase 3 repolarisation and peaked T-waves.
9. Viva Scenario: The "Stone Heart" Myth
Examiner: "Your patient with severe hyperkalaemia is also taking Digoxin. Are you worried about giving IV Calcium?"
Candidate:
- The Myth: Historically, the "Stone Heart" theory suggested that IV calcium in digoxin-treated patients would cause irreversible cardiac contraction.
- Evidence: Modern systematic reviews have shown that this risk is largely theoretical and based on case reports from the early 20th century.
- Priority: The risk of death from hyperkalaemic cardiac arrest is far higher.
- Safe Action: I would still administer the Calcium Gluconate, but I would do so as a slow infusion over 20-30 minutes rather than a rapid bolus, while maintaining continuous ECG monitoring.
10. Patient Explanation
"Potassium is a salt in your blood that acts like a spark plug for your heart. When the level gets too high—usually because the kidneys are struggling—it interferes with the heart's electrical rhythm, which can be very dangerous. We are giving you three types of medicine: one to 'protect' the heart from the sparks, one to 'hide' the potassium inside your cells for a few hours, and one to 'flush' it out of your body for good. We will need to check your blood sugar frequently, as the treatment can sometimes cause it to drop."
11. References
- UK Kidney Association. Clinical Practice Guidelines: Treatment of Acute Hyperkalaemia in Adults. 2020. UKKA
- Packham DK, et al. Sodium Zirconium Cyclosilicate in Hyperkalemia (HARMONIZE). N Engl J Med. 2015. [PMID: 25415807]
- European Resuscitation Council (ERC). Guidelines for Resuscitation: Cardiac arrest in special circumstances. 2021. ERC
- Weir MR, et al. Patiromer in patients with kidney disease and hyperkalemia (AMETHYST-DN). JAMA. 2015. [PMID: 26172458]
- Palmer BF, Carrero JJ. Hyperkalemia in Chronic Kidney Disease. N Engl J Med. 2017. [PMID: 29211656]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for hyperkalaemia (emergency)?
Seek immediate emergency care if you experience any of the following warning signs: Peaked T-waves or QRS widening on ECG, Potassium less than 6.5 mmol/L (Severe), Ascending muscle weakness or paralysis, Sustained bradycardia or high-grade AV block, Oliguric AKI with metabolic acidosis.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Pseudohyperkalaemia
- Hyperacute T-waves (STEMI)
Consequences
Complications and downstream problems to keep in mind.
- Ventricular Fibrillation
- Cardiac Arrest