Hypertension
Hypertension (HTN) is a chronic medical condition characterised by persistently elevated systemic arterial blood pressur... MRCP exam preparation.
What matters first
Hypertension (HTN) is a chronic medical condition characterised by persistently elevated systemic arterial blood pressur... MRCP exam preparation.
SBP less than 180 or DBP less than 120 (Hypertensive Crisis)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- SBP less than 180 or DBP less than 120 (Hypertensive Crisis)
- New-onset confusion (Encephalopathy)
- Chest pain (MI or Aortic Dissection)
- Acute visual loss (Papilloedema)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- White Coat Hypertension
- Chronic Kidney Disease
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Hypertension (Adult)
1. Overview
Hypertension (HTN) is a chronic medical condition characterised by persistently elevated systemic arterial blood pressure. It is the single most important modifiable risk factor for cardiovascular disease (CVD), stroke, and end-stage renal disease (ESRD) worldwide. [1]
The definition of HTN has evolved: while the ACC/AHA (2017) guidelines lowered the threshold to ≥130/80 mmHg, the ESC/ESH (2024) guidelines maintain ≥140/90 mmHg for most adults while recommending a "treat-to-target" of less than 130/80 in those at high risk. [2, 3]
HTN is classified into Primary (Essential) (95%) — a polygenic and lifestyle-driven disorder — and Secondary (5%) — resulting from identifiable renal, endocrine, or vascular causes. Because it is often asymptomatic until a catastrophic vascular event occurs, it is famously known as the "Silent Killer." Management today focuses on early intensive control, the use of Single-Pill Combinations (SPC), and emerging procedural therapies like Renal Denervation. [4]
2. Epidemiology
The "Global Rule of Halves"
- Prevalence: ~1.3 billion people worldwide.
- The Paradox: Roughly half of those with HTN are unaware of their diagnosis; half of those diagnosed are not on treatment; and half of those on treatment are not at target. [5]
High-Risk Groups
- Age: Prevalence exceeds 75% in those > 75 years, primarily as Isolated Systolic Hypertension due to arterial stiffening.
- Ethnicity: Non-Hispanic Black populations have the highest rates of HTN globally, presenting earlier and with more severe target organ damage (TOD), specifically stroke and CKD. [6]
- The "Obesity-HTN" Axis: 60-70% of hypertension risk is directly attributable to excess adiposity.
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- Pressure-Natriuresis Resetting: In health, an increase in BP triggers renal sodium excretion. In HTN, the curve shifts; a higher BP is required to excrete the same amount of sodium, primarily due to increased distal tubular reabsorption (ENaC upregulation).
- Sympathetic Overdrive: Chronic stress or OSA activates the Rostral Ventrolateral Medulla (RVLM), leading to increased norepinephrine release. This causes vasoconstriction and triggers the release of Renin from the juxtaglomerular apparatus.
- RAAS Activation: Excessive Angiotensin II (AngII) acts on AT1 receptors, causing immediate vasoconstriction and stimulating Aldosterone-mediated volume expansion.
- Nitric Oxide (NO) Quenching: Chronic high shear stress activates NADPH oxidase, producing Superoxide (O2-). O2- reacts with NO to form Peroxynitrite, destroying the body's primary vasodilator and leading to endothelial dysfunction.
- Vascular Remodelling: Low-grade inflammation (recruitment of T-cells to the perivascular space) stimulates VSMC hypertrophy. The Media-to-Lumen ratio increases, permanently elevating Total Peripheral Resistance (TPR).
- Arterial Stiffening: Chronic pressure leads to the fragmentation of Elastin and the deposition of Collagen in the large arteries (Aorta), increasing Pulse Wave Velocity (PWV).
- Target Organ Damage (TOD): Sustained pressure causes Hyaline Arteriolosclerosis in the kidneys and Left Ventricular Hypertrophy (LVH) in the heart as a compensatory response to increased afterload. [7, 8]
4. Clinical Presentation
Asymptomatic Nature
The vast majority of patients are asymptomatic. Symptoms when they occur usually indicate Target Organ Damage or Hypertensive Crisis:
- Headache: Classically occipital and worse in the morning.
- Epistaxis: Recurrent spontaneous nosebleeds.
- Visual Blur: Grade 3-4 retinopathy.
Physical Signs of Secondary Causes
- Renal Bruit: Suggests Renal Artery Stenosis.
- Radio-Femoral Delay: Suggests Aortic Coarctation.
- Buffalo Hump/Striae: Suggests Cushing's Syndrome.
- Palpable Kidneys: Suggests ADPKD. [9]
5. Investigations
The Gold Standard: ABPM
Diagnosis should always be confirmed by Ambulatory Blood Pressure Monitoring (ABPM) or Home Monitoring (HBPM) to rule out "White Coat Hypertension" (high in clinic, normal at home) or "Masked Hypertension" (normal in clinic, high at home). [10]
Routine "TOD" Screen
- Urine ACR: To look for microalbuminuria (early renal damage).
- ECG: Look for Sokolow-Lyon criteria for LVH (S in V1 + R in V5/V6 > 35mm).
- Fundoscopy: Grade I (Silver wiring) to Grade IV (Papilloedema).
- U&Es / HbA1c / Lipids: Part of the cardiovascular risk calculation (QRISK3 or SCORE2).
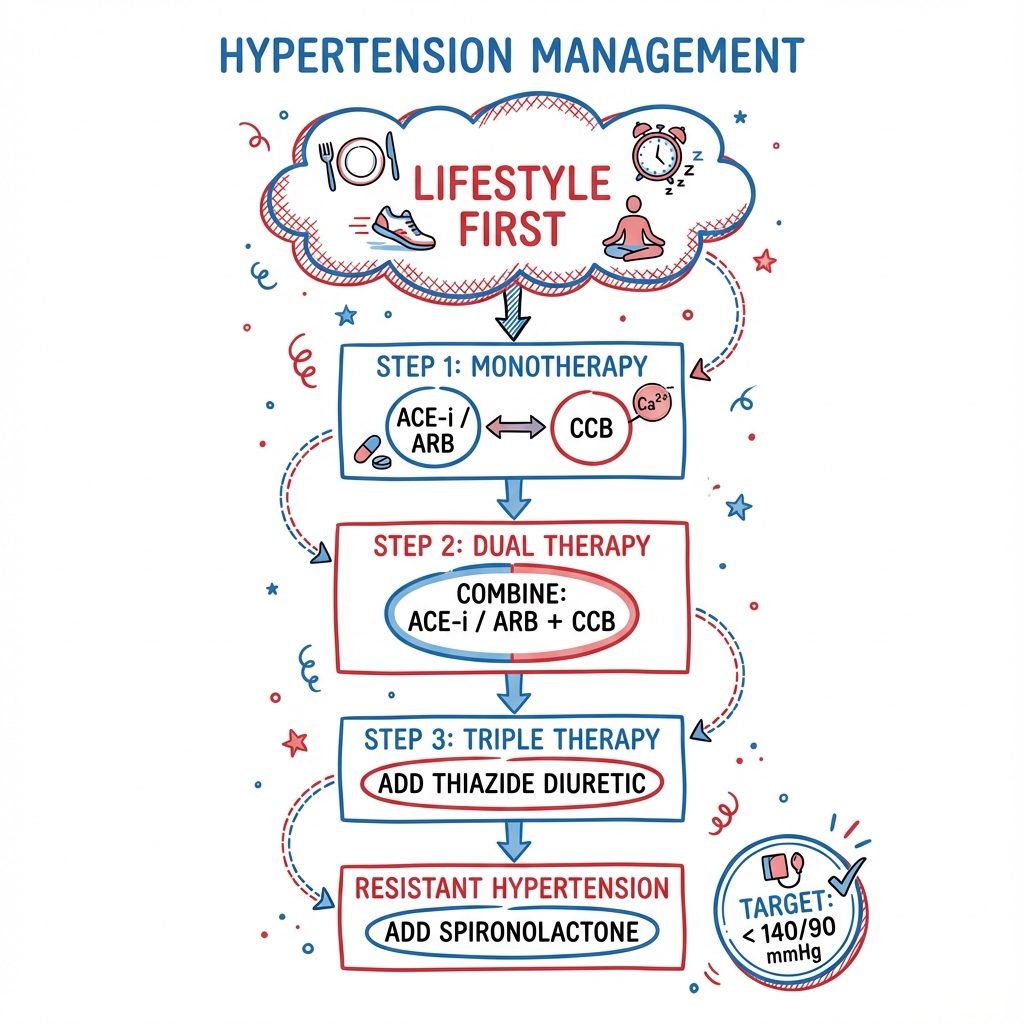
6. Management: The Modern Algorithm
1. Lifestyle First (The "Non-Drug" Pillars)
- Salt Restriction: less than 5g NaCl/day (SBP ↓5 mmHg).
- DASH Diet: High in fruit/veg, low in saturated fat (SBP ↓11 mmHg).
- Weight Loss: 1 mmHg SBP drop per 1 kg lost.
2. Pharmacotherapy (Single-Pill Combinations)
The 2024 ESC/ESH guidelines recommend starting with a Dual SPC for most patients:
- Step 1: ACEi/ARB + CCB or Thiazide-like diuretic (e.g. Indapamide).
- Step 2: Triple SPC (ACEi/ARB + CCB + Diuretic).
- Step 3 (Resistant HTN): Add Spironolactone (25-50mg OD). (Based on the PATHWAY-2 trial). [11]
3. Procedural: Renal Denervation (RDN)
Indicated for patients with uncontrolled resistant HTN or those who cannot tolerate medications. Ultrasound or RF energy is used to ablate the sympathetic nerves in the renal arteries. [12]
7. Evidence: Landmark Trials
| Trial | Population | Result | Impact |
|---|---|---|---|
| SPRINT | High-risk HTN | Target less than 120 vs. less than 140 | 25% ↓ Events; standard for high-risk pts. |
| ALLHAT | HTN | Chlorthalidone vs. ACEi/CCB | Diuretic superior in preventing HF. |
| ACCOMPLISH | High-risk HTN | ACEi+CCB vs. ACEi+Thiaz | ACEi+CCB superior for event reduction. |
| PATHWAY-2 | Resistant HTN | Spironolactone vs. others | Spiro is the clear 4th-line drug. |
| SPYRAL HTN | RDN | Sham-controlled RDN | BP reduction proven even without meds. |
8. Complications: The Vascular Harvest
- Stroke: 50% of all strokes (ICH and Ischaemic) are caused by HTN.
- Heart Failure: HTN is the primary cause of HFpEF (stiff heart).
- Aortic Dissection: HTN is the strongest risk factor for Type A and B dissection.
- Vascular Dementia: Mid-life HTN predicts cognitive decline 20 years later. [13]
9. Single Best Answer (SBA) Questions
Question 1
A 55-year-old Black male has a persistent clinic BP of 155/95. ABG confirms a mean of 148/92. He has no other comorbidities. What is the most appropriate first-line treatment?
- A) Ramipril 5mg
- B) Amlodipine 5mg
- C) Bisoprolol 2.5mg
- D) Losartan 50mg
- E) Spironolactone 25mg
- Answer: B. For patients of Black African/Caribbean descent, CCBs (Amlodipine) or Thiazide-like diuretics are superior to ACEi/ARBs as first-line therapy (NICE and ESC guidelines).
Question 2
A patient with HTN is found to have a serum potassium of 3.1 mmol/L. They are not on a diuretic. What is the most appropriate screening test for their secondary hypertension?
- A) 24-hour urinary metanephrines
- B) Renal Artery Doppler
- C) Plasma Aldosterone-to-Renin Ratio (ARR)
- D) Overnight Dexamethasone Suppression Test
- E) CT Head
- Answer: C. Hypertension + Hypokalaemia = Primary Hyperaldosteronism (Conn's) until proven otherwise. ARR is the mandatory screening test. [14]
10. Viva Scenario: The "Resistant" Patient
Examiner: "Your patient is on Ramipril, Amlodipine, and Indapamide at maximum doses, but their home BP is still 155/95. What is your systematic approach?"
Candidate:
- Rule out Pseudo-resistance: I would check medication adherence (urine assay if available) and rule out "White Coat Effect" via ABPM.
- Screen for Interfering Substances: I'd ask about NSAIDs, liquorice, herbal supplements, and decongestants.
- Secondary Screen: I'd screen for Conn's Syndrome (ARR) and Sleep Apnoea (Epworth scale).
- Treatment Escalation: If truly resistant, I would add Spironolactone 25mg as the 4th-line agent (based on PATHWAY-2 evidence).
11. Patient Explanation
"Hypertension is like having too much air in a tire. You can't feel it, but the extra pressure is slowly damaging the rubber and the rim. In your body, this pressure wears out your heart and damages the 'filters' in your kidneys. Most of the time, we don't find a single 'cause'—it's a mix of genetics, salt, and lifestyle. Our goal with these 'Single-Pill' combinations is to protect you from a future stroke or heart attack by bringing the pressure down to a safe level."
12. References
- Whelton PK, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Hypertension. 2018. [PMID: 29146535]
- Mancia G, et al. 2023 ESH Guidelines for the management of arterial hypertension. J Hypertens. 2023. [PMID: 37345492]
- The SPRINT Research Group. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2015. [PMID: 26551272]
- Williams B, et al. PATHWAY-2: Spironolactone versus placebo, bisoprolol, and doxazosin to determine the optimal treatment for drug-resistant hypertension. Lancet. 2015. [PMID: 26402272]
- Bhatt DL, et al. Renal denervation in patients with uncontrolled hypertension (SYMPLICITY HTN-3). N Engl J Med. 2014. [PMID: 24678160]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- White Coat Hypertension
- Chronic Kidney Disease
Consequences
Complications and downstream problems to keep in mind.
- Haemorrhagic Stroke
- Heart Failure (HFpEF)