Obsessive-Compulsive Disorder (Adult)
Obsessive-Compulsive Disorder (OCD) is a chronic, debilitating psychiatric condition characterised by the presence of obsessions (recurrent, intrusive, unwanted thoughts, images, or urges causing marked anxiety)...
What matters first
Obsessive-Compulsive Disorder (OCD) is a chronic, debilitating psychiatric condition characterised by the presence of obsessions (recurrent, intrusive, unwanted thoughts, images, or urges causing marked anxiety)...
Acute suicide risk (especially with severe OCD + depression)
7 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Acute suicide risk (especially with severe OCD + depression)
- Severe functional impairment (unable to work, leave house, self-care)
- Co-morbid severe depression with psychotic features
- Poor/absent insight approaching delusional intensity
Linked comparisons
Differentials and adjacent topics worth opening next.
- Body Dysmorphic Disorder
- Generalised Anxiety Disorder
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Obsessive-Compulsive Disorder (Adult)
1. Topic Overview
Summary
Obsessive-Compulsive Disorder (OCD) is a chronic, debilitating psychiatric condition characterised by the presence of obsessions (recurrent, intrusive, unwanted thoughts, images, or urges causing marked anxiety) and/or compulsions (repetitive behaviours or mental acts performed to reduce distress or prevent feared outcomes). [1,2] OCD affects approximately 1-2% of the population worldwide, with typical onset in adolescence or early adulthood. [3] The disorder is ego-dystonic — patients recognise thoughts as their own but distressing and inconsistent with their self-concept, distinguishing OCD from psychosis (in most cases). [4]
The phenomenology of OCD is highly heterogeneous: common obsessional themes include contamination fears, harm-related intrusive thoughts, forbidden sexual/religious imagery, symmetry/exactness preoccupations, and pathological doubt. [5] Corresponding compulsions include washing/cleaning, checking, counting, ordering/arranging, mental rituals (praying, neutralising thoughts), and reassurance-seeking. [5] Time spent on obsessions and compulsions typically exceeds 1 hour per day and causes significant functional impairment across occupational, social, and personal domains. [1]
OCD is conceptualised as arising from dysfunction in cortico-striato-thalamo-cortical (CSTC) circuits, with converging evidence from neuroimaging, neuropsychology, and neurosurgical interventions. [6] Serotonergic dysfunction is implicated by the therapeutic efficacy of selective serotonin reuptake inhibitors (SSRIs), while glutamatergic and dopaminergic systems also contribute. [7]
First-line psychological treatment is Cognitive Behavioural Therapy with Exposure and Response Prevention (CBT with ERP), which has the strongest evidence base for efficacy. [8,9] Pharmacologically, SSRIs at higher doses than those used for depression (e.g., fluoxetine 60-80mg, sertraline 150-200mg) are first-line, often requiring 10-12 weeks for therapeutic response. [10] Treatment-resistant cases may benefit from clomipramine (a tricyclic antidepressant with potent serotonergic action), augmentation with low-dose antipsychotics, or intensive/residential ERP programmes. [11,12] Severe refractory OCD may warrant consideration of neurosurgical interventions (deep brain stimulation, anterior capsulotomy). [13]
Key Facts
| Parameter | Value |
|---|---|
| Definition | Obsessions (intrusive thoughts) ± compulsions (repetitive behaviours) causing distress and functional impairment |
| Lifetime Prevalence | 1-3% (varies by diagnostic criteria and population) [3] |
| 12-Month Prevalence | 0.5-1.2% [3] |
| Age of Onset | Bimodal: childhood (ages 6-12, more common in males) and early adulthood (ages 18-25) [14] |
| Sex Ratio | Approximately 1:1 overall; slight male preponderance in childhood-onset |
| Heritability | 45-65% (higher in childhood-onset OCD) [15] |
| First-Line Psychological Treatment | CBT with Exposure and Response Prevention (ERP) |
| First-Line Pharmacotherapy | SSRI at high dose (e.g., fluoxetine 60-80mg, sertraline 150-200mg) [10] |
| Typical Time to Medication Response | 10-12 weeks (longer than for depression) [10] |
| Chronicity | Typically chronic/waxing-waning course; spontaneous remission rare without treatment [1] |
Clinical Pearls
"ERP is the Gold Standard for OCD": Exposure and Response Prevention — systematically confronting feared triggers while refraining from compulsions — has the strongest evidence base. Many patients achieve sustained improvement. [8,9]
"Higher Doses, Longer Trials": SSRIs for OCD require higher doses than for depression (e.g., fluoxetine 60-80mg vs 20mg for depression) and longer trials (10-12 weeks minimum). [10] Inadequate dosing or duration is a common reason for perceived "treatment resistance."
"Assess Insight — It Varies from Good to Absent": DSM-5 allows specifiers for insight: good/fair, poor, or absent/delusional. Poor insight (approaching delusional conviction) is associated with poorer treatment response and may be mistaken for psychosis. [4]
"OCD is Ego-Dystonic, Not Psychotic": Patients typically recognise obsessions as products of their own mind (not inserted) and distressing/inconsistent with values (not endorsed). This distinguishes OCD from psychosis, though overlap exists in poor-insight cases. [4]
"Comorbidity is the Rule, Not the Exception": 60-70% lifetime comorbidity with major depression; high rates of other anxiety disorders, tics, autism spectrum disorder, and personality disorders. [16] Comorbidity complicates treatment and worsens prognosis.
"Consider PANDAS in Acute Paediatric-Onset": Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections (PANDAS) presents with abrupt OCD/tic onset after streptococcal infection. Controversial but increasingly recognised. [17]
Why This Matters Clinically
OCD is often concealed due to shame and embarrassment, leading to diagnostic delays of 7-10 years from symptom onset to treatment initiation. [1] The World Health Organization ranks OCD among the top 10 most disabling conditions worldwide due to profound impairment in quality of life, occupational function, and relationships. [1] Early recognition and evidence-based treatment can prevent decades of suffering and disability. Without treatment, the natural course is typically chronic and unremitting. With appropriate CBT with ERP and/or pharmacotherapy, significant improvement is achievable in the majority of patients. [8,9,10]
2. Epidemiology
Prevalence and Incidence
| Measure | Value | Notes |
|---|---|---|
| Lifetime Prevalence | 1.6-2.3% | Meta-analysis of international studies [3] |
| 12-Month Prevalence | 0.7-1.2% | Varies by population and diagnostic criteria [3] |
| Point Prevalence | ~1% | Stable across cultures [3] |
| Male:Female Ratio | ~1:1 overall | Slight male preponderance in childhood-onset OCD |
Age of Onset
| Pattern | Peak Age | Details |
|---|---|---|
| Childhood-Onset | 6-12 years | More common in males; higher genetic loading [14] |
| Adult-Onset | 18-25 years | More equal sex distribution |
| Late-Onset | > 35 years | Less common; consider organic/neurological causes |
Clinical Note: Bimodal distribution with early peak in childhood (particularly boys) and second peak in early adulthood. [14] Mean age of onset is approximately 19.5 years. Childhood-onset OCD is associated with higher rates of tic disorders, ADHD, and family history of OCD. [14]
Geographic and Cultural Variation
OCD prevalence is remarkably consistent across cultures and countries (~1-2%), suggesting biological rather than purely cultural aetiology. [3] However, symptom content varies by culture:
- Western countries: contamination/washing themes common
- Religious cultures: heightened scrupulosity, blasphemous thoughts
- East Asian cultures: symmetry/ordering themes may predominate
Delay to Treatment
| Metric | Value | Clinical Implication |
|---|---|---|
| Mean Delay from Onset to Treatment | 7-10 years [1] | Prolonged untreated illness associated with worse outcomes |
| Proportion Seeking Treatment | less than 50% [1] | Shame, embarrassment, lack of recognition |
Exam Detail: High-Yield for Exams: OCD has a bimodal age distribution (childhood and early adulthood peaks), affects ~1-2% of the population, and has equal sex distribution overall but male preponderance in childhood-onset. The delay to treatment averages 7-10 years, emphasising the importance of active screening in primary care and mental health settings. OCD is transcultural — prevalence is similar worldwide, though symptom content varies by cultural context.
3. Aetiology and Pathophysiology
Genetic Factors
| Finding | Evidence | Source |
|---|---|---|
| Heritability | 45-65% | Twin and family studies [15] |
| Family Risk | 4-5x increased risk in first-degree relatives | Family studies [15] |
| Genetic Overlap | Shared genetic risk with Tourette syndrome, ADHD, autism spectrum disorder | Genomic studies [15] |
| Candidate Genes | SLC1A1 (glutamate transporter), SAPAP3, SLITRK5, HTR2A (serotonin receptor) | GWAS and candidate gene studies [15] |
Clinical Note: Childhood-onset OCD has higher heritability and greater family loading than adult-onset OCD. [15] Genetic architecture is polygenic (many genes of small effect), with no single "OCD gene."
Neurobiological Pathophysiology
Cortico-Striato-Thalamo-Cortical (CSTC) Circuit Dysfunction
The dominant neurobiological model of OCD implicates hyperactivity and dysregulation of CSTC circuits. [6]
Key Brain Regions:
- Orbitofrontal Cortex (OFC): Hyperactive in OCD; involved in error detection, threat appraisal, and assigning salience to intrusive thoughts. [6]
- Anterior Cingulate Cortex (ACC): Hyperactive; involved in conflict monitoring, error detection, and emotional regulation. [6]
- Caudate Nucleus (Striatum): Dysfunction leads to failure of "gating" or filtering of inappropriate behavioural responses. Normally suppresses unwanted motor/cognitive programs; in OCD, this suppression fails. [6]
- Thalamus: Relays signals between cortical and subcortical structures; hyperactive in OCD. [6]
Pathophysiological Model:
- OFC and ACC generate intrusive thoughts and assign excessive salience/threat value.
- Caudate fails to filter/suppress these intrusive thoughts and inappropriate responses.
- Thalamus relays signals back to cortex, creating a self-perpetuating loop.
- Result: persistent intrusive thoughts → anxiety → compulsive rituals to neutralise anxiety → temporary relief → reinforcement of cycle. [6]
Evidence:
- Neuroimaging (fMRI, PET): Hypermetabolism in OFC, ACC, caudate, and thalamus at rest and during symptom provocation. [6]
- Treatment Response: SSRI treatment and CBT with ERP both reduce hyperactivity in CSTC circuits. [6]
- Neurosurgery: Lesions interrupting CSTC circuits (anterior capsulotomy, cingulotomy) reduce OCD symptoms in refractory cases. [13]
Exam Detail: Examination Focus: The cortico-striato-thalamo-cortical (CSTC) circuit is the neuroanatomical substrate of OCD. Key components are orbitofrontal cortex (threat appraisal), anterior cingulate cortex (conflict monitoring), caudate nucleus (failure of gating/filtering), and thalamus (relay station). Neuroimaging shows hypermetabolism in these regions, which normalises with treatment (both pharmacological and psychological). Neurosurgical interventions targeting these circuits (e.g., anterior capsulotomy) are effective in severe, refractory OCD, providing converging evidence for the model.
Neurotransmitter Systems
| System | Role in OCD | Evidence |
|---|---|---|
| Serotonin (5-HT) | Dysregulation; SSRIs and clomipramine (potent 5-HT reuptake inhibitors) are effective [7,10] | Strong evidence from pharmacotherapy |
| Glutamate | Excess glutamatergic activity in CSTC circuits; glutamate modulators (e.g., memantine, N-acetylcysteine) show promise as augmentation [7] | Emerging evidence |
| Dopamine | Hyperactivity implicated; antipsychotic augmentation effective in treatment-resistant OCD [12] | Moderate evidence |
| GABA | Reduced GABA in ACC; potential role in anxiety and compulsions [7] | Preliminary evidence |
Clinical Implication: Serotonergic agents (SSRIs, clomipramine) remain first-line pharmacotherapy. Glutamatergic and dopaminergic systems represent targets for treatment-resistant cases. [7,12]
Psychological Models
Cognitive-Behavioural Model
OCD is maintained by maladaptive beliefs and cognitive distortions that amplify the significance of intrusive thoughts (which are universal experiences). [18]
Key Cognitive Distortions:
- Inflated Responsibility: "If I don't check, something terrible will happen and it will be my fault."
- Thought-Action Fusion: "Thinking about harming someone is morally equivalent to doing it" (moral TAF) or "Thinking about an event makes it more likely to occur" (likelihood TAF). [18]
- Overestimation of Threat: "Germs are everywhere and will definitely make me seriously ill."
- Intolerance of Uncertainty: "I must be 100% certain the door is locked."
- Perfectionism: "Things must be exactly right or something bad will happen."
- Overimportance of Thoughts: "Having this thought means I'm a bad person."
Behavioural Maintenance: Compulsions provide short-term anxiety reduction (negative reinforcement) but prevent extinction of the fear response and reinforce the belief that the compulsion is necessary. [18] This perpetuates the cycle.
Therapeutic Implication: CBT with ERP targets these beliefs and behaviours by:
- Exposure: Confronting feared situations/triggers to habituate and learn that feared outcomes do not occur.
- Response Prevention: Refraining from compulsions to break the reinforcement cycle and learn that anxiety naturally decreases without rituals. [8,9]
Immunological Factors (PANDAS/PANS)
PANDAS (Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections) is a controversial but increasingly recognised subtype of paediatric OCD characterised by:
- Abrupt onset of OCD and/or tics following Group A Streptococcal (GAS) infection (e.g., pharyngitis, scarlet fever). [17]
- Dramatic symptom exacerbations temporally related to GAS infections.
- Neurological abnormalities (choreiform movements, hyperactivity, emotional lability).
Mechanism: Molecular mimicry — anti-streptococcal antibodies cross-react with basal ganglia neurons (particularly caudate), leading to neuroinflammation and OCD/tic symptoms. [17]
PANS (Paediatric Acute-onset Neuropsychiatric Syndrome) is a broader category including PANDAS but also acute-onset OCD triggered by other infections (e.g., influenza, mycoplasma) or non-infectious causes.
Treatment: Controversial; options include antibiotics (penicillin prophylaxis), anti-inflammatory agents (NSAIDs, corticosteroids), and immunomodulatory therapies (IVIG, plasmapheresis) in severe cases. [17] Standard OCD treatments (CBT with ERP, SSRIs) remain important.
Exam Detail: Viva Scenario: "A 9-year-old boy develops sudden-onset severe OCD (contamination fears, excessive hand-washing) and motor tics 2 weeks after a sore throat. What is the differential diagnosis and management?"
Model Answer:
- Diagnosis: Consider PANDAS (Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections). Abrupt onset of OCD/tics following streptococcal infection is characteristic. Differential includes primary OCD, Tourette syndrome, Sydenham's chorea, autoimmune encephalitis.
- Investigations: Throat swab (if still symptomatic), anti-streptolysin O (ASO) titre, anti-DNase B titre (evidence of recent GAS infection); neurological examination (choreiform movements); consider brain MRI if atypical features. Consider anti-neuronal antibodies if broader autoimmune encephalitis suspected.
- Management:
- "Acute: Treat streptococcal infection if active (penicillin). Consider anti-inflammatory agents (NSAIDs, short course of corticosteroids) in severe cases; some evidence for IVIG/plasmapheresis in refractory cases (controversial). [17]"
- "Prophylaxis: Penicillin prophylaxis to prevent recurrent GAS infections (controversial; consider if multiple documented exacerbations)."
- "Psychiatric: Standard OCD treatment with CBT with ERP and SSRI (e.g., fluoxetine, sertraline) if OCD symptoms persist beyond acute phase."
- "Multidisciplinary: Paediatric neurology/rheumatology involvement; monitoring for recurrence."
Evidence: PANDAS remains controversial but increasingly recognised; molecular mimicry with basal ganglia is proposed mechanism. [17]
4. Clinical Presentation
Obsessions (Intrusive Thoughts, Images, or Urges)
Obsessions are recurrent, persistent, intrusive, unwanted thoughts, urges, or images causing marked anxiety or distress. [1] Key features:
- Ego-dystonic: Recognised as one's own thoughts but inconsistent with self-concept, values, or desires.
- Resisted: Patient attempts to ignore, suppress, or neutralise obsessions (though resistance may diminish over time).
- Time-consuming: Typically > 1 hour per day in clinically significant OCD. [1]
Common Obsessional Themes
| Theme | Examples | Associated Compulsions |
|---|---|---|
| Contamination | Fear of germs, bodily fluids, chemicals, "spiritual contamination" | Washing, cleaning, avoidance |
| Harm/Aggression | Intrusive thoughts/images of harming self or others (stabbing, pushing someone in front of train) | Checking, reassurance-seeking, avoidance of triggers (knives, heights) |
| Sexual | Unwanted intrusive sexual thoughts (paedophilic imagery, incest, sexual acts) | Mental rituals (neutralising thoughts), avoidance of children/triggers |
| Religious/Blasphemous | Intrusive blasphemous thoughts, images of Satan, fears of sin/damnation | Prayer, confession, reassurance from religious authority |
| Symmetry/Exactness | Need for things to be "just right," symmetrical, ordered | Ordering, arranging, repeating actions until "right" |
| Somatic | Obsessive focus on bodily sensations (breathing, blinking, swallowing) | Checking, reassurance-seeking |
| Pathological Doubt | "Did I lock the door? Turn off the oven? Hit someone with my car?" | Checking, retracing steps |
Clinical Note: Harm-related and sexual obsessions are particularly distressing and do not reflect actual desires or risk of acting. These are ego-dystonic intrusive thoughts; patients are horrified by them. This distinguishes OCD from psychopathy or paraphilia. [4]
Compulsions (Repetitive Behaviours or Mental Acts)
Compulsions are repetitive behaviours or mental acts performed in response to an obsession or according to rigid rules. [1] Key features:
- Aimed at reducing distress or preventing feared outcome (though often not realistically connected, or excessive).
- Not pleasurable (may provide temporary relief but not intrinsically enjoyable).
- Time-consuming and/or impairing: Interfere with daily functioning.
Common Compulsions
| Type | Examples | Associated Obsessions |
|---|---|---|
| Washing/Cleaning | Hand-washing (hours per day), showering rituals, cleaning household items | Contamination fears |
| Checking | Checking locks, appliances, switches; retracing driving route | Pathological doubt, harm fears |
| Counting | Counting to specific numbers, repeating actions in multiples | Symmetry, magical thinking |
| Ordering/Arranging | Items must be symmetrical, aligned, in specific order | Symmetry, "just right" feelings |
| Mental Rituals | Praying, repeating phrases silently, neutralising "bad" thoughts with "good" thoughts | Religious obsessions, harm/sexual intrusions |
| Reassurance-Seeking | Repeatedly asking others "Did I hurt anyone? Am I contaminated?" | Harm fears, contamination, doubt |
| Hoarding | Difficulty discarding items due to fear of loss/harm (now separate diagnosis: Hoarding Disorder) | Obsessions about loss, responsibility |
Clinical Note: Mental compulsions (e.g., silent counting, neutralising thoughts) are often overlooked but equally important to assess. Patients may present with purely obsessional OCD (obsessions without overt behavioural compulsions, though mental rituals are usually present). [5]
Subtypes and Symptom Dimensions
Factor-analytic studies identify relatively stable symptom dimensions:
- Contamination/Washing
- Harm/Checking (including pathological doubt)
- Symmetry/Ordering/Counting
- Hoarding (now a separate disorder: Hoarding Disorder)
- Forbidden Thoughts (sexual, religious, aggressive obsessions with mental rituals)
Clinical Implication: Most patients exhibit symptoms across multiple dimensions, though one or two typically predominate. Symptom dimensions may predict treatment response (e.g., hoarding symptoms respond poorly to SSRIs). [5]
Insight Specifiers (DSM-5)
DSM-5 requires specification of level of insight: [4]
| Specifier | Description | Prevalence | Clinical Significance |
|---|---|---|---|
| Good/Fair Insight | Recognises OCD beliefs are definitely/probably not true | ~70-80% | Better treatment response |
| Poor Insight | Thinks OCD beliefs are probably true | ~15-20% | Poorer treatment response; may require antipsychotic augmentation |
| Absent Insight/Delusional | Completely convinced OCD beliefs are true | ~5% | May be misdiagnosed as psychosis; poorest treatment response; antipsychotic augmentation often required [4] |
Clinical Note: Insight may fluctuate with anxiety levels (worse insight when highly anxious) and improve with treatment. [4]
Age of Onset and Course Patterns
| Pattern | Description | Prevalence |
|---|---|---|
| Childhood-Onset (less than 18 years) | Earlier onset; more males; higher genetic loading; more tics/ADHD comorbidity | ~50% of cases [14] |
| Adult-Onset (18-35 years) | Equal sex distribution; less family history | ~40% of cases |
| Late-Onset (> 35 years) | Less common; consider organic causes (e.g., basal ganglia lesions, autoimmune encephalitis) | ~10% of cases |
Course:
- Chronic/Waxing-Waning: Most common (~70-80%); symptoms fluctuate in response to stress.
- Episodic: Discrete episodes with periods of remission (~20%).
- Progressive/Deteriorating: Rare; consider comorbidity or organic causes. [1]
Red Flags Requiring Urgent Assessment
[!CAUTION] Red Flags in OCD:
- Acute suicide risk: Especially with severe OCD + comorbid depression (lifetime suicide attempt rate ~10-15%). [16]
- Severe functional impairment: Housebound, unable to work, unable to perform self-care (washing, eating) due to OCD.
- Severe skin damage: Infection risk from excessive washing; bleeding, ulceration.
- Extreme weight loss: Contamination fears preventing eating.
- Poor/absent insight approaching psychosis: Risk of misdiagnosis; may require antipsychotic treatment. [4]
- OCD in pregnancy: Risks of untreated OCD (harm to mother/infant) vs medication risks; specialist perinatal psychiatry input required.
- Safeguarding concerns: Parental OCD interfering with child care (e.g., excessive cleaning preventing feeding, fear of harming baby).
- Acute paediatric onset post-infection: Consider PANDAS/PANS. [17]
5. Clinical Examination and Assessment
History Taking
Obsessions
- "Do you experience unwanted, intrusive thoughts, images, or urges that you find distressing?"
- "What are these thoughts about?" (Screen for contamination, harm, sexual, religious themes.)
- "Do you recognise these thoughts as coming from your own mind?" (Distinguish from thought insertion in psychosis.)
- "How much time do you spend thinking about these thoughts each day?"
Compulsions
- "Do you feel you have to do certain things over and over to reduce anxiety or prevent something bad from happening?"
- "What do you do?" (Assess for washing, checking, counting, mental rituals.)
- "How long do these behaviours take each day?"
- "What happens if you try to resist or stop these behaviours?"
Functional Impairment
- "How does this affect your daily life — work, relationships, self-care?"
- "Are there places or situations you avoid because of these symptoms?"
Insight
- "Do you think these fears/concerns are realistic, or do you recognise they may be excessive?"
- "How certain are you that your fears are true?" (Good insight: "I know it's irrational"; Poor insight: "It's probably true"; Absent insight: "I'm completely certain.")
Comorbidity
- Screen for depression (PHQ-9), other anxiety disorders (GAD-7, social anxiety), tics, autism spectrum traits, substance use.
Mental State Examination
| Domain | Typical Findings in OCD |
|---|---|
| Appearance | May show effects of compulsions (dry/cracked hands from washing, unkempt if contamination fears prevent bathing) |
| Behaviour | May perform rituals during interview (checking, arranging objects, mental rituals); may be anxious, restless |
| Speech | Normal rate/volume; may show excessive detail (circumstantiality) when describing obsessions |
| Mood | Subjectively anxious, distressed; may be depressed if comorbid MDD |
| Affect | Anxious, constricted; may show distress when discussing obsessional content |
| Thought Form | Normal (OCD is not a thought disorder); may show rumination |
| Thought Content | Obsessional preoccupations; themes of contamination, harm, symmetry, etc.; ego-dystonic (distressing, unwanted) |
| Perception | Normal (no hallucinations) |
| Cognition | Usually normal; may show mild executive dysfunction (impaired cognitive flexibility, set-shifting) on neuropsychological testing |
| Insight | Variable: good/fair (recognises thoughts as excessive) to poor/absent (approaching delusional conviction) [4] |
Key Distinction: OCD is not a psychotic disorder. Obsessions are recognised as one's own thoughts (not inserted), and in most cases, patients have at least partial insight that fears are excessive. However, in poor/absent insight OCD, conviction may approach delusional intensity, leading to diagnostic confusion. [4]
Standardised Assessment Instruments
| Tool | Purpose | Scoring | Clinical Use |
|---|---|---|---|
| Yale-Brown Obsessive Compulsive Scale (Y-BOCS) | Gold standard severity rating | 0-40 (0-7 subclinical, 8-15 mild, 16-23 moderate, 24-31 severe, 32-40 extreme) | Baseline assessment, monitoring treatment response [1] |
| Obsessive-Compulsive Inventory-Revised (OCI-R) | Self-report symptom severity across dimensions | 0-72 (> 21 suggests OCD) | Screening, monitoring |
| Dimensional Y-BOCS (DY-BOCS) | Assesses severity across symptom dimensions | Separate scores for each dimension | Research, tailored treatment planning |
| Children's Y-BOCS (CY-BOCS) | Paediatric version of Y-BOCS | 0-40 (as per Y-BOCS) | Paediatric OCD assessment |
Clinical Pearl: Y-BOCS is the gold standard for assessing OCD severity and monitoring treatment response. It assesses time, interference, distress, resistance, and control for both obsessions and compulsions. A ≥35% reduction in Y-BOCS score is typically considered a clinically significant treatment response. [1]
6. Investigations
OCD is a clinical diagnosis based on history and mental state examination. Investigations are primarily to:
- Rule out organic causes (particularly in atypical presentations, e.g., late-onset, acute onset, neurological signs).
- Baseline assessments prior to medication (SSRIs, clomipramine).
- Screen for comorbidity (depression, anxiety).
Laboratory Investigations
| Test | Indication | Notes |
|---|---|---|
| Full Blood Count (FBC) | Baseline before clomipramine | Clomipramine: rare risk of agranulocytosis |
| Urea & Electrolytes (U&E) | Baseline if SSRI/clomipramine (hyponatraemia risk) | Especially in elderly |
| Liver Function Tests (LFTs) | Baseline before medication | SSRIs/clomipramine metabolised hepatically |
| Thyroid Function Tests (TFTs) | Rule out thyroid disorder (anxiety mimic) | If atypical presentation |
| Anti-Streptolysin O (ASO) Titre, Anti-DNase B | If PANDAS suspected (acute paediatric onset post-streptococcal infection) | Elevated titres suggest recent GAS infection [17] |
| Serum Copper, Caeruloplasmin | If Wilson's disease suspected (young patient, neuropsychiatric + movement disorder) | Rule out treatable metabolic disorder |
| Anti-neuronal Antibodies | If autoimmune encephalitis suspected (acute onset, neurological signs, cognitive change) | Anti-NMDA receptor, anti-LGI1, etc. |
Cardiac Investigations
| Test | Indication | Notes |
|---|---|---|
| Electrocardiogram (ECG) | Mandatory before clomipramine (TCA; risk of QTc prolongation, arrhythmia) | Repeat if dose escalation [10] |
Neuropsychological Testing
| Test | Purpose | Findings in OCD |
|---|---|---|
| Executive Function Battery | Assess cognitive flexibility, set-shifting, response inhibition | Impairments in set-shifting (Wisconsin Card Sorting Test), response inhibition (Stroop Task) common [6] |
Clinical Use: Research tool; not routinely required for clinical management but may inform cognitive remediation strategies.
Neuroimaging
| Modality | Indication | Findings in OCD |
|---|---|---|
| MRI Brain | Atypical features (late-onset, acute onset, neurological signs, poor response to treatment) | Structural abnormalities in caudate, OFC in some cases; exclude organic pathology (tumour, stroke, MS) [6] |
| Functional MRI (fMRI) | Research; not routine clinical use | Hyperactivity in OFC, ACC, caudate, thalamus during symptom provocation [6] |
| PET Scan | Research; pre-neurosurgical assessment | Hypermetabolism in CSTC circuits; normalises with treatment [6] |
Clinical Indication for Neuroimaging:
- Late-onset OCD (> 35 years, especially > 50 years).
- Acute onset with rapid deterioration.
- Neurological signs (movement disorder, cognitive impairment, seizures).
- Poor response to standard treatment (consider organic pathology). [6]
7. Differential Diagnosis
| Condition | Key Distinguishing Features | Overlap with OCD |
|---|---|---|
| Generalised Anxiety Disorder (GAD) | Worries are about real-life concerns (finances, health, family), not intrusive/irrational; no compulsions | Anxiety, rumination |
| Body Dysmorphic Disorder (BDD) | Obsessions limited to perceived defects in appearance; compulsions are mirror-checking, reassurance-seeking, cosmetic procedures | Previously part of OCD spectrum; now separate in DSM-5 |
| Illness Anxiety Disorder (Hypochondriasis) | Preoccupation with having a serious illness; reassurance-seeking from doctors; no contamination fears/washing | Health anxiety |
| Hoarding Disorder | Difficulty discarding possessions due to perceived need to save; cluttered living spaces; ego-syntonic (not distressing until consequences arise) | Previously considered OCD subtype; poor response to OCD treatments [5] |
| Autism Spectrum Disorder (ASD) | Repetitive behaviours/rituals are ego-syntonic (comforting, preferred), not distressing; broader social communication deficits | High comorbidity; ~25% of ASD patients have OCD [16] |
| Tourette Syndrome / Chronic Tic Disorder | Tics are sudden, rapid, non-rhythmic motor movements or vocalisations; preceded by premonitory urge; ego-dystonic but not anxiety-driven | High comorbidity (~30% of TS patients have OCD); may respond to similar treatments [16] |
| Psychotic Disorders (Schizophrenia, Delusional Disorder) | Delusions are ego-syntonic (believed to be true, not distressing as irrational); thought insertion (thoughts not recognised as own); hallucinations | Poor-insight OCD may mimic psychosis; ~10-15% of schizophrenia patients have comorbid OCD [4,16] |
| Major Depressive Disorder with Rumination | Rumination is mood-congruent (themes of worthlessness, guilt, hopelessness); no compulsions | 60-70% comorbidity; OCD often precedes depression [16] |
| Obsessive-Compulsive Personality Disorder (OCPD) | Ego-syntonic perfectionism, rigidity, control; no discrete obsessions/compulsions; pervasive personality pattern | Different disorder; OCPD is ego-syntonic ("I am right to be this way"), OCD is ego-dystonic ("This distresses me") |
| Post-Traumatic Stress Disorder (PTSD) | Intrusive thoughts are trauma-related memories/flashbacks; hyperarousal, avoidance, re-experiencing | Intrusive thoughts overlap; OCD thoughts are not trauma memories |
| Anorexia Nervosa | Obsessions limited to food, weight, shape; compulsions are restrictive eating, exercise, body-checking | Overlap in obsessionality, rigidity; ~10-40% of AN patients have comorbid OCD [16] |
| Organic Causes (basal ganglia lesions, autoimmune encephalitis, Wilson's disease, Sydenham's chorea) | Acute/subacute onset; neurological signs; abnormal neuroimaging or labs | Consider in atypical presentations [6] |
Exam Detail: Viva Scenario: "How do you distinguish OCD from psychosis in a patient with poor insight?"
Model Answer:
- Ego-dystonicity: In OCD, even with poor insight, the thoughts are recognised as one's own (not inserted) and are distressing/inconsistent with self-concept (ego-dystonic). In psychosis, delusions are ego-syntonic (believed to be true, not resisted). [4]
- Content: OCD obsessions typically involve common OCD themes (contamination, harm, symmetry, scrupulosity). Psychotic delusions may involve persecution, grandiosity, control, or bizarre content.
- Response to compulsions: In OCD, compulsions provide temporary anxiety relief. In psychosis, delusions persist regardless of behaviour.
- Insight fluctuation: In OCD, insight may fluctuate with anxiety (worse when anxious, better when calm); may improve with treatment. In psychosis, lack of insight is usually fixed. [4]
- Response to treatment: OCD responds to SSRIs and ERP; poor-insight OCD may require antipsychotic augmentation but typically lower doses than for primary psychosis. [12]
- Comorbidity: ~10-15% of schizophrenia patients have comorbid OCD; both can co-exist ("schizo-obsessive disorder"). [16]
Key Point: DSM-5 includes specifier "absent insight/delusional beliefs" for OCD, recognising that delusional-level conviction can occur in OCD and does not automatically indicate psychosis. [4]
8. Management
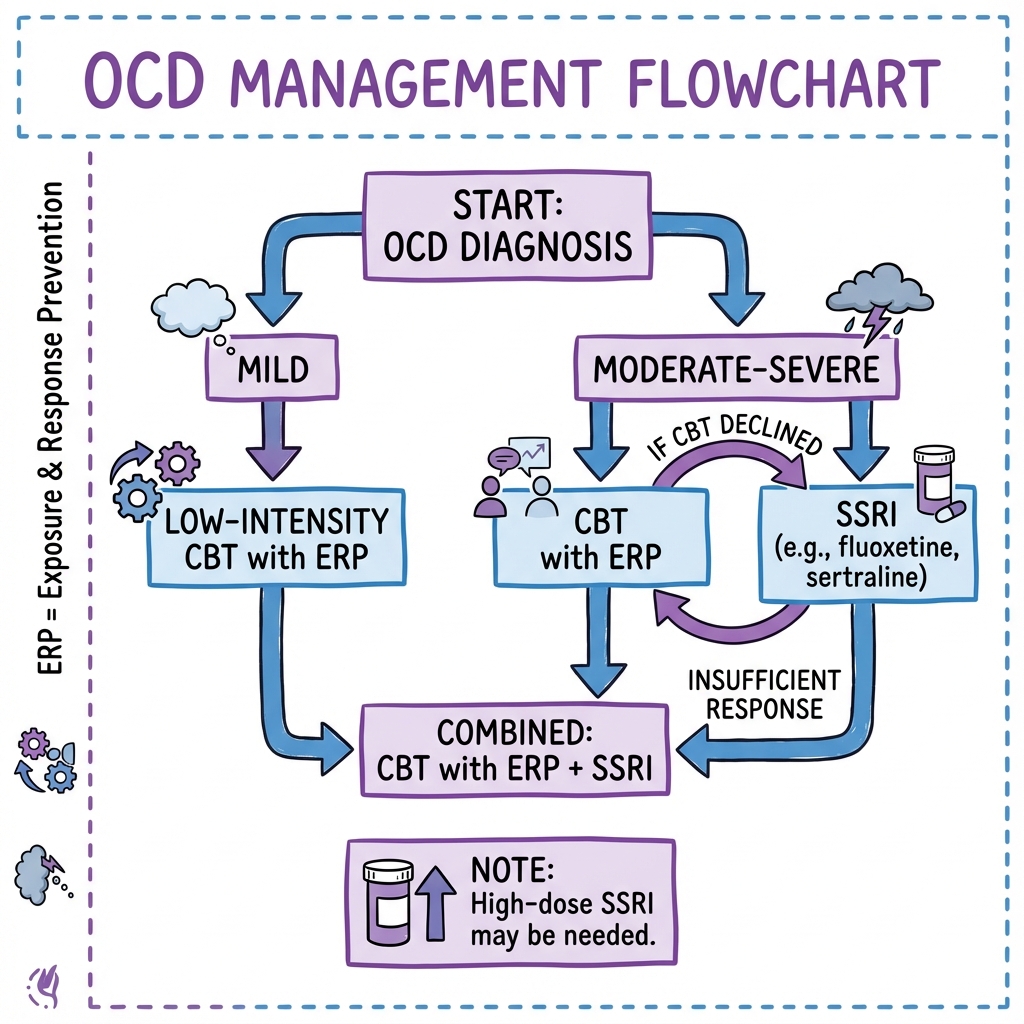
Overview: Stepped Care Approach
Management follows a stepped care model based on severity, functional impairment, and response to treatment. [10]
| Step | Severity | Treatment | Setting |
|---|---|---|---|
| Step 1 | Mild OCD (Y-BOCS less than 16, minimal impairment) | Psychoeducation, self-help materials (guided self-help, CBT-based workbooks), low-intensity CBT | Primary care, IAPT (Improving Access to Psychological Therapies) |
| Step 2 | Moderate OCD (Y-BOCS 16-23, moderate impairment) | CBT with ERP (10-20 sessions) OR SSRI (high dose) | Primary care, IAPT, secondary mental health services |
| Step 3 | Severe OCD (Y-BOCS 24-31, severe impairment) | CBT with ERP + SSRI (combination often superior), specialist OCD service | Secondary mental health services, specialist OCD clinic |
| Step 4 | Treatment-Resistant OCD | Clomipramine, SSRI augmentation (antipsychotics, glutamate modulators), intensive/residential ERP, neurosurgery (DBS, capsulotomy) | Tertiary specialist OCD services, neurosurgery centres |
Guiding Principle: CBT with Exposure and Response Prevention (ERP) is the gold standard psychological treatment and should be offered to all patients with OCD. [8,9] SSRIs are effective but generally less so than ERP; combination therapy is often optimal for moderate-severe OCD. [9]
Psychological Treatment: CBT with Exposure and Response Prevention (ERP)
Rationale
OCD is maintained by avoidance (of feared triggers) and compulsions (which provide short-term relief but prevent extinction of fear and reinforce the OCD cycle). [18] ERP breaks this cycle by:
- Exposure: Gradual, repeated confrontation with feared situations/triggers → habituation (anxiety naturally decreases with prolonged exposure).
- Response Prevention: Refraining from compulsions → extinction of conditioned fear response; learning that feared outcomes do not occur and anxiety decreases without rituals. [8,18]
Evidence Base
- Meta-analyses: ERP is highly effective; effect sizes 1.5-2.0 (large effect); 60-80% response rate (≥35% Y-BOCS reduction). [8,9]
- Superiority to other therapies: ERP superior to relaxation, anxiety management, non-ERP CBT. [8]
- Durability: Treatment gains maintained at 1-2 year follow-up; relapse rates lower than for medication alone. [9]
- Combination with SSRI: Combination of ERP + SSRI is superior to SSRI alone for moderate-severe OCD. [9]
Structure of ERP
Format: Typically 10-20 weekly sessions (60-90 minutes); may be individual or group-based. Intensive formats (daily sessions over 2-4 weeks) show excellent outcomes. [8]
Steps:
- Psychoeducation: Explain OCD cycle (intrusive thoughts → anxiety → compulsions → temporary relief → reinforcement).
- Hierarchy Construction: Collaboratively develop a fear hierarchy (list of feared situations ranked by difficulty, 0-100 SUDs [Subjective Units of Distress]).
- Graded Exposure: Start with moderately difficult items (SUDs 40-60); progress to more difficult. Exposure is prolonged (45-90 minutes) to allow habituation.
- Response Prevention: Refrain from compulsions during and after exposure. Patient learns anxiety decreases naturally without rituals.
- Homework: Daily ERP practice between sessions essential for success.
- Relapse Prevention: Identify high-risk situations; plan for setbacks; maintenance sessions.
Example Hierarchy (Contamination OCD):
- SUDs 20: Touch clean door handle without washing.
- SUDs 40: Touch communal door handle without washing.
- SUDs 60: Touch public toilet door handle without washing.
- SUDs 80: Touch public toilet seat without washing.
- SUDs 100: Touch toilet bowl and eat food without washing.
Clinical Pearl: Prolonged exposure (45-90 minutes) is critical to allow habituation. Brief exposures (less than 30 minutes) may increase anxiety without habituation and worsen symptoms (sensitisation). [8]
Predictors of ERP Response
| Factor | Association with Outcome |
|---|---|
| Good insight | Better response [4] |
| Higher motivation, treatment engagement | Better response |
| Homework completion | Strongly predicts success [8] |
| Comorbid depression | Poorer response (treat depression first/concurrently) [16] |
| Hoarding symptoms | Poor response to standard ERP (requires specialised hoarding treatment) [5] |
| Poor insight | Poorer response; consider SSRI + antipsychotic augmentation [4] |
Pharmacotherapy
First-Line: Selective Serotonin Reuptake Inhibitors (SSRIs)
SSRIs are first-line pharmacotherapy for OCD. [10] Key principles:
- Higher doses than for depression are required (e.g., fluoxetine 60-80mg vs 20mg for depression).
- Longer trial duration (10-12 weeks at therapeutic dose) before assessing response.
- Response is typically partial (~40-60% achieve ≥35% Y-BOCS reduction); complete remission uncommon. [10]
| SSRI | Starting Dose | Target Dose for OCD | Maximum Dose | Notes |
|---|---|---|---|---|
| Fluoxetine | 20mg daily | 60-80mg daily | 80mg daily | Long half-life (no withdrawal if miss dose); first-line |
| Sertraline | 50mg daily | 150-200mg daily | 200mg daily | Well-tolerated; first-line |
| Paroxetine | 20mg daily | 40-60mg daily | 60mg daily | Sedating; weight gain; severe withdrawal syndrome (avoid if possible) |
| Fluvoxamine | 50mg daily | 200-300mg daily | 300mg daily | Licensed for OCD in many countries; drug interactions (CYP1A2 inhibitor) |
| Citalopram | 20mg daily | 40mg daily | 40mg daily (60mg off-label) | QTc prolongation risk at > 40mg; less evidence for OCD |
| Escitalopram | 10mg daily | 20mg daily | 20mg daily (30mg off-label) | Less evidence for OCD than other SSRIs |
Clinical Pearls:
- Choice of SSRI: No consistent evidence of superiority of one SSRI over another; choice based on side-effect profile, patient preference, drug interactions. Fluoxetine and sertraline are most commonly first-line due to evidence base and tolerability. [10]
- Dose escalation: Start at low dose (to minimise initial anxiety/agitation); escalate to therapeutic dose over 2-4 weeks.
- Duration of trial: Minimum 10-12 weeks at therapeutic dose before concluding "treatment failure." [10]
- Response: Typically partial (25-40% reduction in Y-BOCS); rarely complete remission with medication alone.
- Duration of treatment: If effective, continue for at least 12 months after remission; consider longer (24+ months) for severe/recurrent OCD. Taper gradually (over 2-3 months) to minimise withdrawal and relapse. [10]
Side Effects:
- Common: Nausea, headache, insomnia/sedation, sexual dysfunction (delayed ejaculation, anorgasmia, reduced libido ~30-40%), weight gain (especially paroxetine).
- Serious (rare): Hyponatraemia (especially elderly), GI bleeding (especially if combined with NSAIDs; consider PPI), serotonin syndrome (if combined with other serotonergic drugs), suicidal ideation (monitor closely, especially in young adults less than 25 years).
Second-Line: Clomipramine (Tricyclic Antidepressant)
Clomipramine is a tricyclic antidepressant (TCA) with potent serotonin reuptake inhibition. It is highly effective for OCD (possibly more effective than SSRIs in some studies) but poorer tolerability limits first-line use. [10,11]
| Parameter | Details |
|---|---|
| Indication | Treatment-resistant OCD (failed ≥2 SSRIs at adequate dose/duration) [11] |
| Dose | Start 25mg daily; escalate to 150-250mg daily (in divided doses or once daily at night) |
| Evidence | Superior to placebo; possibly superior to SSRIs in some meta-analyses [10,11] |
| Side Effects | Anticholinergic (dry mouth, constipation, urinary retention, blurred vision), sedation, weight gain, orthostatic hypotension, cardiac effects (QTc prolongation, arrhythmia), seizure risk (dose-related; avoid > 250mg) |
| Contraindications | Recent MI, arrhythmia, severe heart disease, uncontrolled epilepsy, acute porphyria, MAOI use (wait 14 days) |
| Monitoring | ECG mandatory (baseline, after dose escalation, periodically); BP monitoring (orthostatic hypotension); plasma levels if poor response/toxicity suspected |
Clinical Pearl: Clomipramine is highly effective but poorly tolerated. Reserve for treatment-resistant OCD after ≥2 SSRI trials. [11]
Treatment-Resistant OCD
Definition: Failure to respond (≥35% Y-BOCS reduction) to:
- ≥2 SSRIs at adequate dose (high dose) for adequate duration (10-12 weeks).
- CBT with ERP (≥10 sessions with adequate homework compliance). [11]
Prevalence: ~30-40% of OCD patients are treatment-resistant. [11]
Step 1: Re-assess Diagnosis and Adherence
- Is it truly OCD? Re-evaluate for differential diagnoses (ASD, OCPD, psychosis, other anxiety disorders).
- Is insight poor? Consider poor-insight OCD (may require antipsychotic augmentation). [4]
- Is there comorbidity? Treat comorbid depression, substance use, PTSD.
- Was ERP adequate? Sufficient sessions (≥10)? Homework completion? Adequate exposure duration (45-90 minutes)?
- Was medication adequate? Sufficient dose? Sufficient duration (≥10-12 weeks)? Adherence?
Step 2: Switch or Augment Medication
Switch to Clomipramine
If not yet tried, switch to clomipramine 150-250mg. [11]
Augmentation Strategies
| Strategy | Evidence | Dose/Protocol | Notes |
|---|---|---|---|
| Antipsychotic Augmentation (add to SSRI) | Moderate-strong evidence; meta-analyses show benefit [12] | Risperidone 0.5-3mg, Aripiprazole 5-15mg, Quetiapine 150-300mg added to SSRI | Most evidence for risperidone, aripiprazole; particularly effective if comorbid tics or poor insight [12] |
| Glutamate Modulators | Emerging evidence; several small RCTs | N-acetylcysteine (NAC) 1200-2400mg daily, Memantine 10-20mg daily, Lamotrigine 100-200mg daily | NAC: antioxidant, modulates glutamate; memantine: NMDA antagonist; lamotrigine: glutamate release inhibitor [7] |
| SSRI + Clomipramine Combination | Limited evidence; expert opinion | Low-dose clomipramine (25-75mg) added to SSRI | Risk of serotonin syndrome; requires specialist supervision; monitor ECG |
| SSRI + Buspirone | Weak evidence | Buspirone 30-60mg daily added to SSRI | 5-HT1A partial agonist; inconsistent evidence |
| SSRI + Lithium | Weak evidence | Lithium 400-800mg (plasma level 0.6-0.8 mmol/L) | Monitor levels, renal function, thyroid function |
Clinical Pearl: Antipsychotic augmentation (risperidone, aripiprazole) is the best-evidenced augmentation strategy for treatment-resistant OCD, particularly if comorbid tics or poor insight. [12] Use low doses (much lower than for psychosis); monitor for extrapyramidal side effects, weight gain, metabolic syndrome.
Step 3: Intensive/Residential ERP
For severe treatment-resistant OCD, intensive ERP programmes (daily sessions over 2-4 weeks, residential/day-patient setting) show excellent outcomes. [8] These programmes provide:
- Daily therapist-assisted exposure (2-3 hours per day).
- 24-hour response prevention (residential setting prevents rituals).
- Peer support (group format).
Availability: Specialist OCD clinics/centres (e.g., Maudsley Hospital London, Bethlem Royal Hospital UK, McLean Hospital USA).
Step 4: Neurosurgical Interventions (Severe Refractory OCD)
For severe, chronic, disabling OCD refractory to all standard treatments (multiple medication trials, intensive ERP), neurosurgical interventions may be considered. [13]
| Procedure | Mechanism | Evidence | Selection Criteria |
|---|---|---|---|
| Deep Brain Stimulation (DBS) | Reversible; electrodes implanted in ventral capsule/ventral striatum (VC/VS) or subthalamic nucleus (STN); high-frequency stimulation modulates CSTC circuits [13] | RCTs show ~40-60% response; FDA/CE approved for refractory OCD [13] | Y-BOCS ≥28, duration > 5 years, failed all standard treatments, severe impairment |
| Anterior Capsulotomy | Irreversible lesion; interrupts anterior limb of internal capsule (part of CSTC circuit) | ~50-70% response in case series [13] | As per DBS; irreversible so reserved for extreme cases |
| Anterior Cingulotomy | Irreversible lesion; targets anterior cingulate cortex | ~30-50% response [13] | As per DBS |
Clinical Note: Neurosurgery is reserved for severe, chronic, disabling OCD after exhaustive trials of standard treatments. Requires multidisciplinary assessment (psychiatry, neurosurgery, ethics) and patient informed consent. DBS is reversible and increasingly preferred over ablative procedures. [13]
Special Populations
OCD in Pregnancy and Perinatal Period
Prevalence: OCD often worsens in pregnancy and postpartum (hormonal factors, stress, sleep deprivation). New-onset perinatal OCD is common. [10]
Common Themes: Harm-related obsessions (intrusive thoughts of harming baby, images of dropping/suffocating baby); contamination fears (excessive cleaning, fear of germs harming baby); checking compulsions (repeatedly checking baby breathing). [10]
Management:
- Non-pharmacological first: CBT with ERP is safe and effective in pregnancy/breastfeeding; first-line. [10]
- Pharmacotherapy if required:
- "SSRIs: Generally considered safe in pregnancy (particularly sertraline — lowest placental transfer, extensive safety data). Small increased risk of persistent pulmonary hypertension of newborn (PPHN) and neonatal adaptation syndrome (transient jitteriness, irritability, poor feeding in first 2 weeks). [10]"
- "Risk-benefit assessment: Risks of untreated OCD (maternal distress, impaired bonding, suicide risk) often outweigh medication risks."
- Avoid paroxetine (small increased risk of cardiac malformations in first trimester). [10]
- Specialist perinatal psychiatry input essential.
OCD in Children and Adolescents
First-Line: CBT with ERP (family-based); highly effective in children. [10]
Pharmacotherapy: SSRIs effective but start lower doses than adults; sertraline and fluoxetine have best evidence and regulatory approval for paediatric OCD. Monitor for activation, suicidal ideation (black box warning in USA). [10]
PANDAS/PANS: Consider in acute-onset paediatric OCD post-infection; treat infection, consider anti-inflammatory/immunomodulatory therapies in severe cases. [17]
9. Complications and Comorbidity
Psychiatric Comorbidity
| Comorbid Condition | Prevalence in OCD | Clinical Implications |
|---|---|---|
| Major Depressive Disorder (MDD) | 60-70% lifetime [16] | Often secondary to OCD; treat both conditions; comorbid depression worsens OCD prognosis |
| Other Anxiety Disorders (GAD, social anxiety, panic disorder) | 40-60% [16] | Overlapping symptoms; may require additional treatment strategies |
| Tic Disorders / Tourette Syndrome | 20-30% [16] | Shared genetic/neurobiological substrate; may respond to similar treatments (SSRIs, antipsychotics) |
| Autism Spectrum Disorder (ASD) | 20-25% [16] | Differentiate ASD rituals (ego-syntonic, comforting) from OCD compulsions (ego-dystonic, anxiety-driven); high comorbidity |
| Eating Disorders (Anorexia Nervosa, Bulimia Nervosa) | 10-40% [16] | Overlapping obsessionality, perfectionism, rigidity |
| Substance Use Disorders | 20-30% [16] | Often secondary (self-medication for anxiety); worsens OCD; treat concurrently |
| Personality Disorders (Avoidant, Dependent, Obsessive-Compulsive PD) | 30-50% [16] | Complicates treatment; poorer response to standard therapies |
| Psychotic Disorders (Schizophrenia, Schizoaffective Disorder) | 10-15% [16] | "Schizo-obsessive disorder"; both conditions co-exist; complex pharmacotherapy (antipsychotics may worsen OCD; SSRIs may worsen psychosis in some cases) |
Clinical Pearl: Comorbidity is the norm in OCD. Screen for and treat comorbid conditions to optimise outcomes. Comorbid depression is particularly common and significantly worsens prognosis; treat concurrently with SSRIs (effective for both) and CBT. [16]
Suicide Risk
Prevalence:
- Lifetime suicide attempt rate: 10-15% in OCD (higher than general population). [16]
- Suicidal ideation: 30-50% of OCD patients report suicidal ideation at some point. [16]
Risk Factors:
- Severe OCD symptoms.
- Comorbid major depression (strongest predictor). [16]
- Hopelessness, perceived uncontrollability of OCD.
- Poor treatment response.
- Social isolation, unemployment.
Management: Screen for suicidal ideation; treat comorbid depression aggressively; risk assessment and safety planning; consider inpatient admission if acute risk. [16]
Physical Complications
| Complication | Cause | Management |
|---|---|---|
| Dermatological (contact dermatitis, skin breakdown, bleeding, infection) | Excessive washing/cleaning | Dermatology referral; emollients; treat skin infections; ERP to reduce washing |
| Musculoskeletal (joint pain, repetitive strain injury) | Excessive checking, repeating actions | Physiotherapy; pain management; ERP |
| Malnutrition, Weight Loss | Contamination fears preventing eating | Nutritional assessment; dietitian input; ERP targeting eating |
| Social Isolation | Avoidance, embarrassment, time consumed by rituals | Social skills training; supported re-engagement; ERP |
10. Prognosis and Outcomes
Natural Course (Untreated)
| Pattern | Prevalence | Description |
|---|---|---|
| Chronic/Waxing-Waning | 70-80% | Most common; symptoms fluctuate in severity with stress, life events; rarely remit spontaneously |
| Episodic | 10-20% | Discrete episodes with periods of partial/complete remission |
| Chronic Progressive | 5-10% | Rare; continuous worsening; consider comorbidity, organic causes |
Key Point: Without treatment, OCD typically follows a chronic course with significant disability. Spontaneous remission is rare (less than 10%). [1]
Response to Treatment
| Treatment | Response Rate (≥35% Y-BOCS reduction) | Remission Rate (Y-BOCS ≤12) | Notes |
|---|---|---|---|
| CBT with ERP | 60-80% [8,9] | 40-60% | Most effective monotherapy; durable gains |
| SSRI (high dose) | 40-60% [10] | 20-30% | Effective but less than ERP; partial response typical |
| CBT + SSRI (Combination) | 70-90% [9] | 50-60% | Superior to either alone for moderate-severe OCD |
| Clomipramine | 50-70% [11] | 30-40% | Possibly more effective than SSRIs but poorer tolerability |
| Antipsychotic Augmentation | 30-50% (of treatment-resistant cases) [12] | Variable | For treatment-resistant OCD; add-on to SSRI |
Predictors of Poor Prognosis
| Factor | Association with Outcome |
|---|---|
| Early age of onset (less than 10 years) | Poorer prognosis [14] |
| Longer duration of untreated illness | Worse outcomes; emphasises importance of early intervention [1] |
| Poor insight | Poorer response to treatment [4] |
| Comorbid depression, personality disorder | Worse prognosis [16] |
| Hoarding symptoms | Poor response to standard OCD treatments [5] |
| Low motivation, poor treatment engagement | Predictably poor outcomes |
Long-Term Outcomes
- With treatment: Significant improvement achievable in majority (~60-70%); many patients achieve sustained remission or mild residual symptoms. [8,9]
- Relapse: Common (~40-50%) after treatment discontinuation; relapse rates lower with CBT than medication alone. [9] Maintenance therapy (ongoing CBT booster sessions or continued SSRI) reduces relapse risk.
- Functional recovery: Many patients achieve good occupational and social functioning with treatment; however, full functional recovery may lag behind symptom improvement. [1]
11. Evidence and Guidelines
Key Guidelines
| Guideline | Year | Key Recommendations |
|---|---|---|
| NICE CG31: Obsessive-Compulsive Disorder and Body Dysmorphic Disorder [10] | 2005 (updated 2018) | • Mild OCD: Low-intensity CBT, guided self-help • Moderate OCD: CBT with ERP or SSRI • Severe OCD: CBT + SSRI, specialist referral • Treatment-resistant: Clomipramine, augmentation, intensive ERP • SSRIs at high dose, 10-12 week trial |
| American Psychiatric Association (APA) Practice Guideline for OCD | 2007 | • First-line: CBT with ERP or SSRI • Combination superior for moderate-severe OCD • Clomipramine for treatment-resistant cases |
| Canadian Clinical Practice Guidelines for OCD | 2014 | • CBT with ERP first-line • SSRIs first-line pharmacotherapy • Antipsychotic augmentation for treatment-resistant OCD |
| British Association for Psychopharmacology (BAP) Guidelines for OCD | 2014 | • High-dose SSRIs, 10-12 week trial • Clomipramine second-line • Augmentation: antipsychotics, glutamate modulators |
Landmark Studies
| Study | Year | Findings | Reference |
|---|---|---|---|
| Foa et al. (SSRI vs ERP vs Combination) | 2005 | ERP superior to clomipramine; combination of ERP + clomipramine superior to either alone | PMID: 15625214 [9] |
| Meta-analysis: Olatunji et al. (ERP Efficacy) | 2013 | ERP highly effective (effect size 1.5-2.0); superior to medication; durable gains | PMID: 23538238 [8] |
| Meta-analysis: Soomro et al. (SSRI Efficacy) | 2008 | SSRIs effective vs placebo; high doses required; 40-60% response rate | Cochrane Database [10] |
| Bloch et al. (Antipsychotic Augmentation) | 2006 | Antipsychotic augmentation (risperidone, aripiprazole, quetiapine) effective for treatment-resistant OCD; NNT ~3-5 | PMID: 16651511 [12] |
| Goodman et al. (DBS for Refractory OCD) | 2010 | Deep brain stimulation (VC/VS) effective for severe refractory OCD; ~40-60% response | PMID: 20395477 [13] |
Evidence Levels
| Intervention | Evidence Level | Strength of Recommendation |
|---|---|---|
| CBT with ERP | 1a (systematic reviews, meta-analyses) | Strong — First-line for all OCD |
| SSRIs (high dose) | 1a | Strong — First-line pharmacotherapy |
| Clomipramine | 1a | Moderate — Second-line (efficacy high but tolerability poorer than SSRIs) |
| Combination CBT + SSRI | 1b (RCTs) | Strong — For moderate-severe OCD |
| Antipsychotic Augmentation | 1a | Moderate — For treatment-resistant OCD |
| Glutamate Modulators | 2b (small RCTs) | Weak — Emerging evidence; consider in treatment-resistant cases |
| Deep Brain Stimulation | 2b-3 | Moderate — For severe refractory OCD unresponsive to all other treatments |
12. Examination Focus (MRCPsych / Psychiatry Vivas)
High-Yield Viva Topics
Exam Detail: Viva Question 1: "A 25-year-old man presents with 6 months of excessive hand-washing (4-5 hours per day) due to contamination fears. He has tried sertraline 100mg for 8 weeks with minimal benefit. What is your management?"
Model Answer:
- Assess adequacy of SSRI trial: Sertraline 100mg is subtherapeutic for OCD (target 150-200mg). Increase to 200mg and reassess after 10-12 weeks total (not 8 weeks). [10]
- Offer CBT with ERP: Gold standard; should be offered regardless of medication. Construct fear hierarchy; graded exposure to contamination triggers with response prevention (no hand-washing). [8]
- Assess severity: Y-BOCS score to quantify severity; assess functional impairment (work, relationships, self-care).
- Screen for comorbidity: Depression (PHQ-9), other anxiety disorders, substance use.
- If inadequate response after optimised SSRI + CBT: Consider switch to clomipramine, or augmentation strategies (antipsychotics), or intensive ERP programme. [11,12]
- Monitor skin integrity: Assess for dermatological complications (dermatitis, infection) from excessive washing; dermatology referral if needed.
Viva Question 2: "Explain the neurobiological basis of OCD and how this relates to treatment."
Model Answer:
- CSTC Circuit Dysfunction: OCD arises from hyperactivity and dysregulation of cortico-striato-thalamo-cortical (CSTC) circuits. [6]
- "Orbitofrontal cortex (OFC): Hyperactive; assigns excessive threat value to intrusive thoughts."
- "Anterior cingulate cortex (ACC): Hyperactive; conflict monitoring, error detection."
- Caudate nucleus: Dysfunction leads to failure of "gating" — inability to filter/suppress inappropriate thoughts and responses.
- "Thalamus: Relays signals back to cortex, creating self-perpetuating loop."
- Neuroimaging Evidence: fMRI/PET show hypermetabolism in OFC, ACC, caudate, thalamus at rest and during symptom provocation. [6]
- Treatment Effects: Both SSRIs and CBT with ERP normalise CSTC hyperactivity — reduce metabolism in OFC, ACC, caudate, thalamus. [6]
- Neurosurgery: Deep brain stimulation (electrodes in ventral capsule/ventral striatum) and ablative procedures (anterior capsulotomy, cingulotomy) interrupt CSTC circuits → symptom reduction in refractory OCD. [13]
- Neurotransmitters:
- "Serotonin: Dysregulation; SSRIs (block 5-HT reuptake) effective. [7,10]"
- "Glutamate: Excess in CSTC circuits; glutamate modulators (NAC, memantine) show promise as augmentation. [7]"
- "Dopamine: Hyperactivity; antipsychotics (D2 antagonists) effective as augmentation. [12]"
Viva Question 3: "A patient with OCD has intrusive thoughts about harming her baby. How do you assess this, and what is the risk of her acting on these thoughts?"
Model Answer:
- Phenomenology: Determine if ego-dystonic (OCD) vs ego-syntonic (psychosis, true homicidal ideation).
- OCD: Thoughts are intrusive, unwanted, distressing; patient is horrified by the thoughts; recognises them as inconsistent with self ("I would never do this; the thought terrifies me"). No intent or desire to act. [4]
- Psychosis/True Harm: Thoughts may be command hallucinations, delusional beliefs (e.g., "The baby is possessed"), or ego-syntonic desires to harm. Patient may feel compelled to act or lack distress about thoughts.
- Risk Assessment:
- Risk of acting on OCD harm obsessions is extremely low. Harm obsessions in OCD are ego-dystonic and not associated with increased risk of violence. [4]
- However, assess for depression, psychosis, postpartum psychosis (which do carry risk of harm to infant).
- Safety: If any doubt about risk, safeguarding assessment; consider brief admission for assessment; involve health visitor, safeguarding team.
- Treatment: Reassure patient that harm obsessions are common in perinatal OCD (~50% of postpartum OCD involves harm obsessions) and do not mean she will act. [10]
- CBT with ERP: First-line; graded exposure to triggers (e.g., holding baby near stairs, knives) with response prevention (not avoiding, not seeking reassurance). [8]
- SSRI (e.g., sertraline 150-200mg) if breastfeeding, generally safe; discuss risks/benefits. [10]
- Support: Perinatal psychiatry, health visitor, partner/family support.
Viva Question 4: "What are the treatment options for severe treatment-resistant OCD?"
Model Answer: Definition: Treatment-resistant OCD = failure to respond (≥35% Y-BOCS reduction) to:
- ≥2 SSRIs at adequate dose (high dose) and duration (10-12 weeks).
- CBT with ERP (≥10 sessions, adequate homework). [11]
Step 1: Re-assess:
- Diagnosis correct? (exclude ASD, OCPD, psychosis, other anxiety disorders)
- Adequate treatment? (sufficient dose, duration, ERP exposure time, homework compliance)
- Comorbidity? (depression, substance use, personality disorder)
- Insight? (poor insight requires different approach) [4]
Step 2: Medication Strategies:
- Switch to clomipramine 150-250mg (if not yet tried). [11]
- Antipsychotic augmentation: Add risperidone 0.5-3mg, aripiprazole 5-15mg, or quetiapine 150-300mg to SSRI. [12]
- Best evidence for risperidone, aripiprazole.
- Particularly effective if comorbid tics or poor insight. [12]
- Use low doses; monitor for EPS, weight gain, metabolic syndrome.
- Glutamate modulators: N-acetylcysteine (NAC) 1200-2400mg, memantine 10-20mg, lamotrigine 100-200mg. [7]
- Emerging evidence; several small RCTs.
- Combination SSRI + clomipramine: Low-dose clomipramine added to SSRI (specialist supervision; monitor ECG, serotonin syndrome risk).
Step 3: Intensive/Residential ERP:
- Daily therapist-assisted exposure (2-3 hours/day) over 2-4 weeks.
- 24-hour response prevention (residential setting).
- Excellent outcomes (~70-80% response) in refractory cases. [8]
Step 4: Neurosurgical Interventions (Severe Refractory OCD):
- Deep Brain Stimulation (DBS): Reversible; electrodes in ventral capsule/ventral striatum (VC/VS) or subthalamic nucleus (STN); ~40-60% response. [13]
- Anterior Capsulotomy: Irreversible lesion; ~50-70% response. [13]
- Anterior Cingulotomy: Irreversible lesion; ~30-50% response. [13]
- Selection: Y-BOCS ≥28, duration > 5 years, failed all standard treatments, severe impairment.
- Approval: Multidisciplinary assessment (psychiatry, neurosurgery, ethics); informed consent.
13. Patient/Layperson Explanation
What is OCD?
Obsessive-Compulsive Disorder (OCD) is a mental health condition where you have unwanted, distressing thoughts (obsessions) that make you feel anxious, and you feel you have to do repetitive behaviours (compulsions) to try to reduce the anxiety. It's not about being tidy — it's a real medical condition that causes a lot of distress and interferes with daily life.
What are the symptoms?
Obsessions (intrusive thoughts):
- Contamination fears: Worrying excessively about germs, dirt, or getting ill.
- Harm fears: Intrusive thoughts/images of harming yourself or others (e.g., "What if I push someone in front of a train?").
- Sexual or religious intrusive thoughts: Unwanted thoughts/images that are distressing and inconsistent with your values.
- Symmetry/ordering: Feeling that things must be "just right," symmetrical, or in a specific order.
- Doubts: Persistent doubts (e.g., "Did I lock the door? Turn off the oven?").
Compulsions (repetitive behaviours):
- Washing/cleaning: Excessive hand-washing, showering, cleaning (sometimes for hours each day).
- Checking: Repeatedly checking locks, appliances, switches, or retracing steps.
- Counting: Counting to specific numbers, or repeating actions a certain number of times.
- Ordering/arranging: Arranging items symmetrically or in a specific way.
- Mental rituals: Silently praying, repeating phrases, or "cancelling out" bad thoughts with good thoughts.
- Reassurance-seeking: Repeatedly asking others "Did I hurt anyone? Am I contaminated?"
What causes it?
OCD is caused by a combination of:
- Brain differences: Certain brain circuits (involving areas that detect threats and control habits) are overactive in OCD.
- Genetics: OCD runs in families; you're more likely to have OCD if a family member has it.
- Stress: Life stress can trigger or worsen OCD.
It's not your fault, and it's not a sign of weakness.
How is it treated?
The good news is that OCD is very treatable. The most effective treatments are:
-
Cognitive Behavioural Therapy with Exposure and Response Prevention (CBT with ERP):
- This is the gold standard treatment.
- You work with a therapist to gradually face your fears (exposure) while not doing the compulsions (response prevention).
- It sounds scary, but it's very effective — you learn that the anxiety naturally goes down without needing to do rituals, and that the feared outcomes don't happen.
- Most people see significant improvement with 10-20 sessions.
-
Medication (SSRIs):
- Antidepressants called SSRIs (like fluoxetine, sertraline) are effective for OCD.
- They require higher doses and longer trials (10-12 weeks) than for depression.
- About 40-60% of people respond to SSRIs.
- Often combined with CBT for best results.
-
Combination of CBT + Medication:
- For moderate-severe OCD, combining CBT with medication is often most effective.
What can I expect?
- With treatment, most people improve significantly. Many people achieve remission or mild residual symptoms.
- Treatment takes time — don't give up if you don't see immediate results.
- OCD is often chronic, but with the right treatment, you can manage it and live a full life.
- If one treatment doesn't work, there are other options (different medications, intensive therapy, specialist treatments).
Where can I get help?
- GP: Start with your GP, who can refer you to mental health services or IAPT (Improving Access to Psychological Therapies).
- Specialist OCD services: For severe OCD, specialist OCD clinics offer intensive treatment.
- Support organisations:
- "OCD Action: ocdaction.org.uk"
- "OCD-UK: ocduk.org"
- "International OCD Foundation (IOCDF): iocdf.org"
Remember: OCD is a treatable medical condition. With the right help, you can get better.
14. References
Guidelines
-
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Arlington, VA: American Psychiatric Publishing; 2013.
-
Stein DJ, Costa DLC, Lochner C, et al. Obsessive-compulsive disorder. Nat Rev Dis Primers. 2019;5(1):52. DOI: 10.1038/s41572-019-0102-3
-
Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry. 2010;15(1):53-63. PMID: 18725912
Neurobiology
-
Milad MR, Rauch SL. Obsessive-compulsive disorder: beyond segregated cortico-striatal pathways. Trends Cogn Sci. 2012;16(1):43-51. PMID: 22138231
-
Pittenger C, Bloch MH, Williams K. Glutamate abnormalities in obsessive compulsive disorder: neurobiology, pathophysiology, and treatment. Pharmacol Ther. 2011;132(3):314-332. PMID: 21963369
Treatment: Psychological
-
Olatunji BO, Davis ML, Powers MB, Smits JA. Cognitive-behavioral therapy for obsessive-compulsive disorder: a meta-analysis of treatment outcome and moderators. J Psychiatr Res. 2013;47(1):33-41. PMID: 23538238
-
Foa EB, Liebowitz MR, Kozak MJ, et al. Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder. Am J Psychiatry. 2005;162(1):151-161. PMID: 15625214
Treatment: Pharmacological
-
National Institute for Health and Care Excellence. Obsessive-compulsive disorder and body dysmorphic disorder: treatment (CG31). London: NICE; 2005 (updated 2018). Available at: nice.org.uk/guidance/cg31
-
Pallanti S, Quercioli L. Treatment-refractory obsessive-compulsive disorder: methodological issues, operational definitions and therapeutic lines. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30(3):400-412. PMID: 16503369
-
Bloch MH, Landeros-Weisenberger A, Kelmendi B, et al. A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder. Mol Psychiatry. 2006;11(7):622-632. PMID: 16651511
-
Goodman WK, Foote KD, Greenberg BD, et al. Deep brain stimulation for intractable obsessive compulsive disorder: pilot study using a blinded, staggered-onset design. Biol Psychiatry. 2010;67(6):535-542. PMID: 20395477
Developmental and Genetic
-
Taylor S. Early versus late onset obsessive-compulsive disorder: evidence for distinct subtypes. Clin Psychol Rev. 2011;31(7):1083-1100. PMID: 21820387
-
Pauls DL, Abramovitch A, Rauch SL, Geller DA. Obsessive-compulsive disorder: an integrative genetic and neurobiological perspective. Nat Rev Neurosci. 2014;15(6):410-424. PMID: 24840802
Comorbidity and Outcomes
- Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry. 2010;15(1):53-63. PMID: 18725912
PANDAS
- Swedo SE, Leckman JF, Rose NR. From research subgroup to clinical syndrome: modifying the PANDAS criteria to describe PANS (Pediatric Acute-onset Neuropsychiatric Syndrome). Pediatr Therapeut. 2012;2(2):113. DOI: 10.4172/2161-0665.1000113
Cognitive Models
- Salkovskis PM. Understanding and treating obsessive-compulsive disorder. Behav Res Ther. 1999;37 Suppl 1:S29-52. PMID: 10402694
Further Resources
Professional
- International OCD Foundation (IOCDF): iocdf.org — Professional resources, treatment provider directory, research updates.
- British Association for Behavioural and Cognitive Psychotherapies (BABCP): babcp.com — Accredited CBT therapist directory (UK).
Patient Support
- OCD Action (UK): ocdaction.org.uk — Support groups, helpline, resources.
- OCD-UK: ocduk.org — Information, support, advocacy.
- International OCD Foundation: iocdf.org — Information, support groups, annual conference.
Self-Help Books
- "Break Free from OCD" by Fiona Challacombe, Victoria Bream Oldfield, Paul Salkovskis — CBT-based self-help workbook.
- "Getting Over OCD" by Jonathan Abramowitz — Evidence-based self-help guide.
Medical Disclaimer: MedVellum content is for educational purposes and clinical reference. It does not replace professional medical advice. If you or someone you know is experiencing OCD symptoms, please seek assessment and treatment from a qualified mental health professional.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Anxiety Disorders - Overview
- Cognitive Behavioural Therapy
Differentials
Competing diagnoses and look-alikes to compare.
- Body Dysmorphic Disorder
- Generalised Anxiety Disorder
- Autism Spectrum Disorder
- Psychotic Disorders
Consequences
Complications and downstream problems to keep in mind.