Osteoarthritis
It is a "Whole Joint Failure". The cardinal features are pain (mechanical), stiffness (short duration), and loss of function. It predominantly affects weight-bearing joints (Hips, Knees) and the hands (DIPs, CMC thumb).
What matters first
It is a "Whole Joint Failure". The cardinal features are pain (mechanical), stiffness (short duration), and loss of function. It predominantly affects weight-bearing joints (Hips, Knees) and the hands (DIPs, CMC thumb).
Night Pain (Rest pain = Severe or Malignancy)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Night Pain (Rest pain = Severe or Malignancy)
- Fever + Redness (Septic Arthritis)
- Locking (Meniscal Tear / Loose Body)
- Weight Loss (Metastases)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Osteoarthritis (OA)
1. Clinical Overview
Summary
Osteoarthritis (OA) is the most common form of arthritis worldwide. Historically considered a passive "wear and tear" disease, it is now understood as a metabolically active process involving the breakdown of cartilage, subchondral bone remodelling, and synovial inflammation.
It is a "Whole Joint Failure". The cardinal features are pain (mechanical), stiffness (short duration), and loss of function. It predominantly affects weight-bearing joints (Hips, Knees) and the hands (DIPs, CMC thumb).
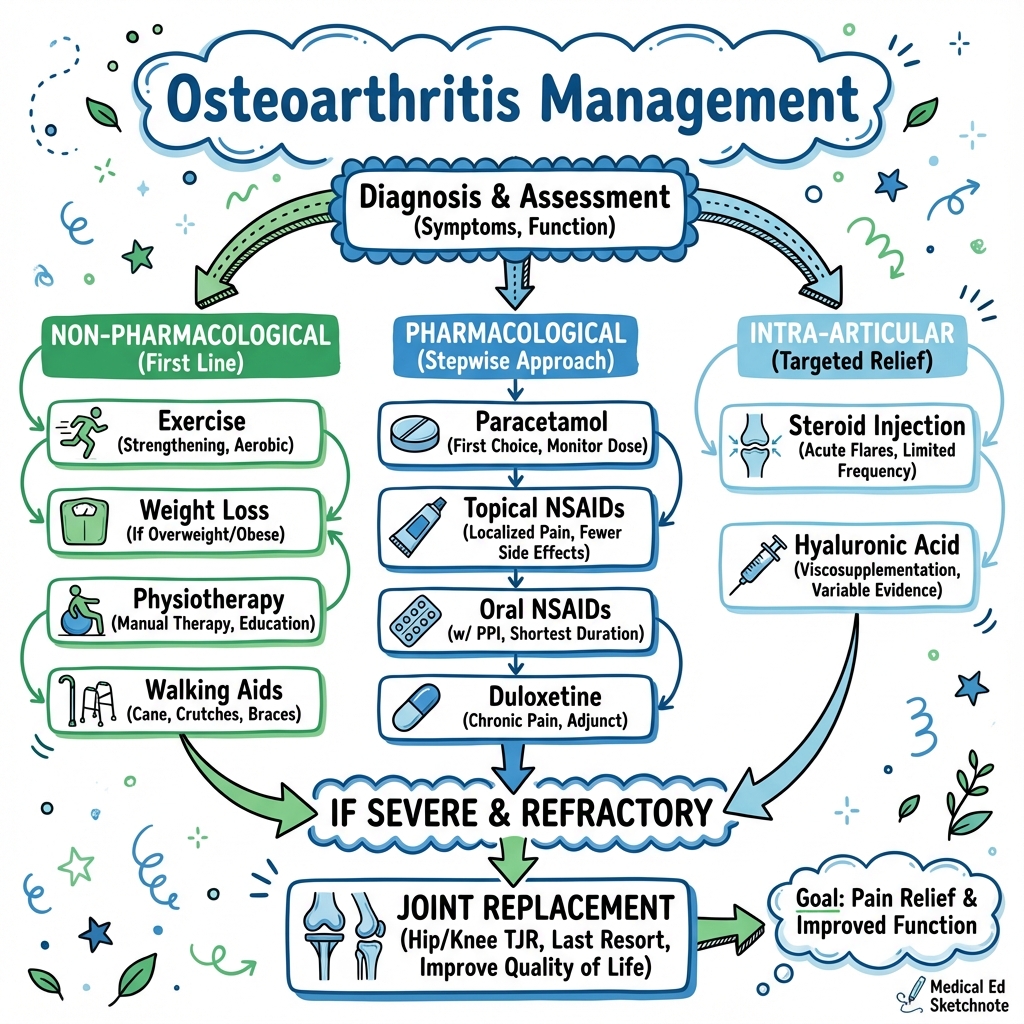
Management follows a strict step-ladder:
- Non-Pharmacological: Education, Weight Loss, Physiotherapy (The Core Treatments).
- Pharmacological: Paracetamol, Topical NSAIDs, Oral NSAIDs, Intra-articular Steroids.
- Surgical: Joint Replacement (Arthroplasty) is the definitive treatment for end-stage disease with resistant pain.
Key Facts
- Prevalence: Affects > 8.5 million people in the UK.
- Obesity: The single biggest modifiable risk factor for Knee OA. Losing 10% body weight reduces pain by 50%.
- X-Ray vs Symptoms: There is poor correlation. Patients with terrible X-rays may have no pain, and vice versa. Treat the patient, not the X-ray.
- Arthroplasty: Total Hip Replacement (THR) is "The Operation of the Century" (Lancet), providing immense quality of life improvement.
Clinical Pearls
The "Groin" Pearl: Hip pathology presents as Groin Pain, usually radiating to the anterior thigh/knee. "Hip Pain" pointed to on the lateral aspect of the hip (trochanter) is usually Trochanteric Bursitis or Gluteal Tendinopathy, NOT the hip joint.
The "Stiffness" Pearl: Morning stiffness in OA lasts less than 30 minutes (usually 5-10 mins). If it lasts > 1 hour, suspect Rheumatoid Arthritis.
The "Stick" Pearl: Walking sticks should be held in the Opposite hand to the affected leg. This reduces the lever arm force across the hip joint by up to 40%.
2. Epidemiology
Risk Factors
1. Systemic
- Age: Major risk factor.
- Obesity: Metabolic load (Adipokines) + Mechanical load.
- Genetics: High heritability for Hand and Hip OA (60%).
- Gender: Women > Men (after menopause).
2. Local Biomechanical
- Trauma: Previous fracture or cruciate ligament tear (Post-traumatic OA).
- Malalignment: Varus (Bow leg) causes Medial compartment OA. Valgus (Knock knee) causes Lateral compartment OA.
- Occupation: Heavy lifting, kneeling (Carpet fitters).
- Dysplasia: Developmental Dysplasia of Hip (DDH) causes early OA.
3. Pathophysiology
The Cycle of Destruction
- Cartilage Loss: Imbalance between breakdown (MMPs) and repair. Type II collagen network disrupted. Water content increases initially, then cartilage softens ("Chondromalacia") and wears away.
- Bone Response:
- Eburnation: Exposed subchondral bone becomes polished/hard (Sclerosis).
- Cysts: Synovial fluid is pressed through micro-cracks into bone, forming cysts.
- Osteophytes: New bone forms at the margins to increase surface area and stabilise the joint.
- Synovium: Mild secondary inflammation (synovitis) due to debris phagocytosis.
Pain Mechanisms
Cartilage has no nerve supply. Pain comes from:
- Subchondral bone micro-fractures.
- Stretching of periosteum (Osteophytes).
- Synovitis.
- Muscle spasm.
4. Clinical Presentation (By Joint)
1. Knee OA
- Symptoms: Pain on stairs (Patellofemoral), Locking/Giving way.
- Signs:
- Varus deformity (Bow legs).
- Baker's Cyst (Posterior herniation of synovium).
- Crepitus.
- Fixed Flexion Deformity (cannot straighten leg).
2. Hip OA
- Symptoms: Groin pain. Difficulty putting on socks/shoes (stiffness).
- Signs:
- Antalgic Gait (Limps to shorten stance time).
- Trendelenburg Gait (Abductor weakness).
- Fixed Flexion Deformity (Thomas Test positive).
- Loss of Internal Rotation (First sign).
3. Hand OA
- Heberden's Nodes: Bony swellings at DIP joints.
- Bouchard's Nodes: Bony swellings at PIP joints.
- CMC Thumb: Pain at base of thumb ("Squaring" of the hand). Good grip strength preserved but painful.
The "Young Adult" Hip (FAI)
The precursor to OA.
- Femoroacetabular Impingement (FAI): Abnormal contact between hip ball and socket.
- Cam Lesion: Bump on femoral neck (common in young male athletes).
- Pincer Lesion: Over-coverage of acetabulum (common in females).
- Symptoms: "C-Sign" (Hand cupped over hip). Pain on deep flexion.
- Management: Arthroscopic reshaping prevents OA.
Patellofemoral Pain Syndrome (PFPS)
The OA Mimic.
- Anterior Knee Pain in young women.
- Driven by maltracking of patella, weak VMO muscle, tight IT Band.
- Management: Physio taping, VMO strengthening. NOT surgery.
5. Radiological Classification
(Kellgren-Lawrence Grading)
| Grade | Severity | Findings |
|---|---|---|
| 0 | None | Normal |
| 1 | Doubtful | Minute osteophytes, doubtful narrowing. |
| 2 | Mild | Definite osteophytes, possible narrowing. |
| 3 | Moderate | Moderate narrowing, multiple osteophytes, some sclerosis/deformity. |
| 4 | Severe | Large osteophytes, Bone-on-Bone (No joint space), Severe sclerosis/deformity. |
The Cardinal X-Ray Signs (LOSS)
Mnemonic: LOSS
- L - Loss of Joint Space (Asymmetrical).
- O - Osteophytes.
- S - Subchondral Sclerosis (Whiter bone).
- S - Subchondral Cysts (Black circles).
6. Management: Conservative
**(The "Core Treatments"
- NICE)**
1. Education & Self Management
- "Wear and Repair" vs "Wear and Tear".
- Motion is Lotion: Activity feeds the cartilage.
2. Weight Loss
- Impact on knees is 4x body weight.
- 5kg weight loss = 20kg load reduction per step.
3. Physiotherapy / Exercise
- Quadriceps Strengthening: Critical for Knee OA. Stabilises the joint.
- Aerobic Exercise: Swimming/Cycling (Non-impact).
4. Aids
- Walking Stick (Contralateral side).
- Shock absorbing footwear.
7. Management: Pharmacological
Guidelines (NICE NG226)
- Topical NSAIDs: First line for Knee/Hand. (e.g. Ibuprofen gel). Safer than oral.
- Oral NSAIDs: Use lowest effective dose for shortest time. MUST co-prescribe PPI.
- Steroid Injections: Intra-articular Methylprednisolone. Provides short term relief (weeks/months). Useful for "Bridge" to surgery or special occasions (Holiday/Wedding).
- Opiates: NOT RECOMMENDED for chronic OA pain. (Addiction/Falls risk > Benefit).
- Glucosamine/Chondroitin: Not recommended by NICE (Placebo effect mainly).
Viscosupplementation (Hyaluronic Acid)
- Injection of lubricant.
- Controversial. Not recommended by NICE due to cost-effectiveness, but widely used privately. Small benefit over placebo.
8. Management: Surgical (Arthroplasty)
Indications
- End-stage disease (Grade 3-4).
- Refractory pain (Failed conservative).
- Night pain affecting sleep.
- Significant functional impairment.
1. Total Hip Replacement (THR)
- Procedure: Femoral head removed. Acetabulum reamed.
- Fixation:
- Cemented: Methylmethacrylate cement. Best for Osteoporotic/Elderly bone. Immediate full weight bearing.
- Uncemented: Press-fit. Bone grows into porous coating (Hydroxyapatite). Best for Young/Good bone.
- Bearing Surfaces:
- Metal on Polyethylene: Standard. Low wear.
- Ceramic on Ceramic: Lowest wear. Risk of squeaking / fracture (rare). Good for young patients.
- Metal on Metal: ABANDONED (ALVAL/Pseudotumours complications).
2. Total Knee Replacement (TKR)
- Resurfacing of Femur, Tibia, and Patella. (Cruciate ligaments usually sacrificed or PCL retained).
- Recovery: Harder than Hip. Requires intense physio to regain Range of Motion (ROM).
3. Unicompartmental Knee Replacement (UKR)
- "Half Knee". Usually Medial compartment.
- Pros: Smaller incision, faster recovery, feels more "natural" (ACL preserved).
- Cons: Higher revision rate (progression of OA in other compartments).
4. Osteotomy (HTO)
- High Tibial Osteotomy. Realigns the leg (corrects varus) to offload the damaged compartment.
- Used in Young (less than 50) active patients to delay replacement.
9. ERAS & Complications
(Enhanced Recovery After Surgery)
The ERAS Protocol
Optimising patients for rapid discharge (Day 0/1).
- Pre-Hab: Joint School education. Optimise Hb > 120. Smoking cessation.
- Peri-op:
- Spinal Anaesthesia (avoid GA nausea).
- Tranexamic Acid (reduce bleeding).
- Local Infiltration Analgesia (LIA) into joint.
- Carbohydrate Loading drinks pre-op.
- Post-op:
- Mobilise within 4 hours.
- Opioid sparing analgesia.
Complications
General
- DVT/PE: High risk. Chemical prophylaxis (LMWH/Aspirin) required for 14-28 days.
- Infection (1%): Catastrophic. Biofilm formation on metal. Requires "Two Stage Revision" (Remove implant -> Antibiotic Spacer for 6 weeks -> Re-implant).
Hip Specific
- Dislocation: Risk higher in first 6 weeks. Precautions (don't cross legs, don't flex > 90).
- Leg Length Discrepancy.
- Sciatic Nerve Injury (Foot drop).
Knee Specific
- Stiffness: Arthrofibrosis.
- Numbness: Lateral to incision (Saphenous nerve branch).
10. Evidence & Guidelines
Guidelines
- NICE NG226 (2022): Osteoarthritis in over 16
s: diagnosis and management.
- Major change: Do NOT offer Paracetamol as monotherapy (ineffective).
- Strong focus on Exercise and Weight Loss.
- Strong advice AGAINST opioids.
- OARSI Guidelines: Global guidelines mirroring NICE.
Key Trials
- Moseley et al (2002): Arthroscopic Lavage for OA.
- Sham surgery trial. Showed arthroscopy ("wash out") is NO better than placebo for OA. Now largely abandoned.
- KAT Trial: Knee Arthroplasty Trial. Compared Patella resurfacing vs not. Equivocal results.
12. Patient Explanation
Is it "Bone on Bone"?
On the X-ray, yes, the cartilage cushion has worn away. But that doesn't mean you are disabled. Many people with "bone on bone" walk for miles. It depends on how strong your muscles are.
Will exercise make it worse?
No. Your cartilage has no blood supply. It gets its food from the joint fluid. The only way to pump food into the cartilage is to move the joint. Exercise feeds your hip. Rest starves it.
When should I have surgery?
When you can't be you anymore. When the pain stops you sleeping, stops you walking to the shops, or stops you enjoying your hobbies. We operate on pain, not X-rays.
13. References
-
National Institute for Health and Care Excellence (NICE). Osteoarthritis in over 16 s: diagnosis and management. NICE Guideline [NG226]. Published: 19 October 2022.
-
Moseley JB et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002 Jul 11;347(2):81-8. PMID: 12110735
-
Learmonth ID et al. The operation of the century: total hip replacement. Lancet. 2007 Oct 27;370(9597):1508-19. PMID: 17965013
-
Bannuru RR et al (OARSI). OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019 Nov;27(11):1578-1589. PMID: 31278997
14. Examination Focus
Common Exam Questions
- "X-Ray features of OA?"
- Answer: LOSS (Loss of joint space, Osteophytes, Subchondral sclerosis, Subchondral cysts).
- "Contraindication to High Tibial Osteotomy?"
- Answer: Inflammatory arthritis (RA), Older age (> 60), Tricompartmental disease.
- "First line drug for Hand OA?"
- Answer: Topical NSAID.
Viva Points
- Uncemented vs Cemented Hip: Know the indications (Age/Bone quality).
- infection: Understand why antibiotics don't work on prosthesis (Biofilm).
Last Updated: 2026-01-04