Osteoporosis
Clinically, it is known as the "silent thief" because bone loss occurs without symptoms until a fragility fracture occurs. A fragility fracture is defined as a fracture resulting from a fall from standing height or...
What matters first
Clinically, it is known as the "silent thief" because bone loss occurs without symptoms until a fragility fracture occurs. A fragility fracture is defined as a fracture resulting from a fall from standing height or...
Vertebral Fracture with Neurological Signs (Cauda Equina/Cord Compression)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Vertebral Fracture with Neurological Signs (Cauda Equina/Cord Compression)
- Hip Fracture (Surgical Emergency - Mortality Risk)
- Multiple Fractures (Exclude Myeloma/Metastatic Disease)
- Young Patient (less than 50) with Osteoporosis (Secondary Cause Likely)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Osteoporosis
1. Clinical Overview
Summary
Osteoporosis is a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, leading to increased bone fragility and susceptibility to fracture. It is the most common metabolic bone disease worldwide. The World Health Organization (WHO) defines osteoporosis as a Bone Mineral Density (BMD) T-score of ≤ -2.5 at the femoral neck or lumbar spine.
Clinically, it is known as the "silent thief" because bone loss occurs without symptoms until a fragility fracture occurs. A fragility fracture is defined as a fracture resulting from a fall from standing height or less. The most common sites are the vertebrae, hip (proximal femur), and distal radius (Colles' fracture).
Current management has shifted from a "treat the T-score" approach to a "treat the risk" approach. Guidelines (NOGG 2024) now stratify patients into Low, High, and Very High Risk categories based on fracture probability. This stratification dictates whether to start with standard antiresorptive therapy (bisphosphonates) or "Anabolic First" therapy (Teriparatide/Romosozumab) for those at imminent risk of fracture.
Key Facts
- Prevalence: Affects 1 in 2 women and 1 in 5 men over the age of 50.
- Mortality: Hip fractures carry a 20-30% mortality rate within 12 months.
- Imminent Risk: The risk of a second fracture is highest in the first 2 years after an index fracture (the "imminent risk" window).
- Diagnosis: Gold standard is DXA (Dual-energy X-ray Absorptiometry), but clinical diagnosis can be made in the presence of a fragility fracture regardless of T-score.
- Treatment Gap: Only ~20% of patients presenting with a fragility fracture receive osteoporosis treatment.
Clinical Pearls
The "Sentinel Fracture" Pearl: A wrist (Colles') fracture is often the first sign of osteoporosis. It typically occurs 15 years before a hip fracture. Identifying and treating at this stage can prevent the devastating hip fracture later.
The "Height Loss" Pearl: Loss of > 4cm from peak height (or > 2cm in one year) is highly suggestive of vertebral compression fractures. Two-thirds of vertebral fractures are asymptomatic ("silent"). Measure height at every review.
The "Anabolic Window" Pearl: Anabolic agents (Teriparatide, Romosozumab) build new bone faster than antiresorptives preserve it. They are most effective in treatment-naïve bone. Therefore, for Very High Risk patients, use "Anabolic First", followed by bisphosphonates to "lock in" the gains.
The "Drug Holiday" Pearl: Bisphosphonates bind avidly to bone and recycle locally. After 5 years (oral) or 3 years (IV), a pause in treatment ("holiday") may be considered for lower-risk patients to reduce the risk of atypical femoral fractures, while residual drug continues to work.
The "Secondary Screen" Pearl: In men, premenopausal women, or Z-scores < -2.0, always screen aggressively for secondary causes. "Osteoporosis in a man is Myeloma until proven otherwise" is a safe maxim to prompt thorough investigation.
2. Epidemiology
Prevalence and Incidence
- Global: Affects > 200 million people worldwide.
- UK Impact: ~3.5 million people in the UK have osteoporosis.
- Fracture Burden: > 500,000 fragility fractures occur annually in the UK.
- Economic Cost: Costs the NHS >£4.5 billion annually, primarily due to hip fracture care.
Demographics
- Sex: Post-menopausal women are at highest risk due to rapid estrogen withdrawal. F:M ratio is 4:1.
- Age: Prevalence increases exponentially with age. By age 80, 70% of women have osteoporosis.
- Ethnicity: Highest risk in Caucasian and Asian populations. Lower risk in Afro-Caribbean populations (higher peak bone mass).
Risk Factors
| Risk Factor | Relative Risk | Mechanism | Notes |
|---|---|---|---|
| Age > 65 | High | Senescence of osteoblasts, reduced renal calcium conservation | Universal risk factor |
| Female Sex | 4.0 | Estrogen deficiency (loss of osteoclast inhibition) | Rapid bone loss phase lasts 5-10 yrs post-menopause |
| Prior Fracture | 2.0 - 5.0 | Structural failure, reduced biomechanical competence | Strongest predictor of future fracture |
| Glucocorticoids | High | Apoptosis of osteoblasts, increased RANKL, decreased gut Ca absorption | Dose-dependent; significant risk at > 7.5mg prednisolone > 3 months |
| Family History | 1.5 - 2.0 | Genetic peak bone mass determinants (e.g., LRP5, VDR genes) | Parental hip fracture is a key FRAX input |
| Low BMI (less than 19) | 2.0 | Reduced mechanical loading, reduced aromatization of androgens to estrogen | Anorexia Nervosa is a critical cause in young |
| Smoking | 1.5 | Direct toxic effect on osteoblasts, accelerated estrogen metabolism | Reversible risk |
| Alcohol | 1.5 | Nutritional deficiency, fall risk, direct osteoblast inhibition | > 3 units/day |
| Rheumatoid Arthritis | 2.0 | Systemic inflammation (TNF, IL-6) drives osteoclastogenesis via RANKL | Independent of steroid use |
Secondary Causes (The "BAD BONES" Mnemonic)
Must be excluded in all patients, especially men and young women.
- Blood: Multiple Myeloma, Mastocytosis, Thalassemia.
- Autoimmune: RA, SLE, Ankylosing Spondylitis.
- Drugs: Steroids, PPIs, SSRIs, Anticonvulsants, Aromatase Inhibitors, GnRH agonists.
- Bone/GI: Coeliac disease, IBD, Gastrectomy (Malabsorption).
- Osteomalacia: Vitamin D deficiency.
- Nephrology: CKD-MBD (Renal Osteodystrophy), Hypercalciuria.
- Endocrine: Hyperparathyroidism, Hyperthyroidism, Cushing's, Hypogonadism, Diabetes (T1 & T2).
- Senesence/Idiopathic.
3. Pathophysiology
Bone is a dynamic tissue undergoing constant remodelling. Osteoporosis represents a decoupling of this process where resorption exceeds formation.
The Bone Remodelling Cycle (Molecular Mechanism)
Step 1: Activation & Signalling
- Mechanical stress (or lack thereof) and systemic hormones affect osteocytes.
- Osteocytes (embedded bone cells) regulate the cycle via Sclerostin.
- High Sclerostin inhibits the Wnt/β-catenin pathway, suppressing bone formation.
- Clinical Relevance: Romosozumab inhibits Sclerostin, releasing the "brake" on bone formation.
Step 2: Resorption Phase
- Pre-osteoblasts express RANKL (Receptor Activator of Nuclear factor Kappa-B Ligand).
- RANKL binds to RANK receptors on osteoclast precursors.
- Osteoclasts mature, form a ruffled border, and seal to the bone surface.
- They secrete Cathepsin K (degrades collagen) and H+ ions (dissolves mineral).
- OPG (Osteoprotegerin) is a natural decoy receptor that binds RANKL, preventing resorption.
- Pathology: Estrogen deficiency leads to ↓OPG and ↑RANKL → unchecked resorption.
- Clinical Relevance: Denosumab mimics OPG, binding RANKL. Bisphosphonates poison osteoclasts.
Step 3: Reversal Phase
- Osteoclasts undergo apoptosis.
- Macrophage-like cells clear debris.
- Growth factors (TGF-β, IGF-1) released from the bone matrix attract osteoblasts.
Step 4: Formation Phase
- Osteoblasts (derived from mesenchymal stem cells) arrive.
- They synthesize Osteoid (Type I Collagen matrix).
- This process is driven by the Wnt/β-catenin pathway.
- Clinical Relevance: Teriparatide (PTH analogue) stimulates osteoblast number and activity and inhibits osteoblast apoptosis.
Step 5: Mineralisation
- Osteoid is mineralised with Hydroxyapatite crystals (Calcium + Phosphate).
- Requires adequate Vitamin D and Calcium availability.
- Pathology: In Osteomalacia, this step fails (lots of osteoid, no mineral). In Osteoporosis, the mineralisation is normal, but the amount of bone is reduced.
Step 6: Quiescence
- Osteoblasts either undergo apoptosis, become bone-lining cells, or become embedded Osteocytes.
- The new bone unit is complete.
Microarchitectural Changes
- Trabecular Bone (Vertebrae, ends of long bones):
- Loss of horizontal trabeculae (struts).
- Reduced connectivity ("perforation").
- Highly susceptible to compression fractures.
- Cortical Bone (Shafts of long bones):
- Endocortical thinning ("tunneling").
- Increased porosity.
- Loss of structural rigidity.
4. Clinical Presentation
Asymptomatic Phase
- Most patients are asymptomatic.
- Incidental finding on X-ray (osteopenia) or CT (vertebral wedging).
- Opportunistic screening via FRAX in primary care.
Symptomatic Phase (Fractures)
- Vertebral Compression Fracture:
- Acute: Sudden, severe midline back pain. Often precipitated by trivial movement (lifting a bag, coughing). Pain radiates to the flank/anterior abdomen.
- Chronic: Height loss, progressive thoracic kyphosis ("Dowager's Hump"), protuberant abdomen, chronic mechanical back pain, reflux symptoms.
- Hip Fracture (Neck of Femur):
- Pain in groin/thigh.
- Inability to weight bear.
- Leg shortened and externally rotated.
- Distal Radius (Colles'):
- "Dinner fork" deformity following a fall on outstretched hand (FOOSH).
Red Flags (Differential Diagnosis)
Symptoms that suggest pathology OTHER than simple osteoporosis:
- Night Pain: Suggests malignancy or osteoid osteoma.
- Unexplained Weight Loss: Metastatic disease, Myeloma.
- Fever/Sweats: Osteomyelitis, TB spine, Malignancy.
- History of Primary Cancer: Breast, Prostate, Lung, Kidney, Thyroid (Bone metastases).
- Severe Anaemia/Renal Failure: Multiple Myeloma.
5. Clinical Examination
Inspection
- Kyphosis: Thoracic curvature (Wall-Occiput test: inability to touch head to wall while standing straight).
- Rib-Pelvis Distance: less than 2 fingerbreadths indicates significant lumbar vertebral height loss.
- Skin folds: "Christmas tree" skin folds on the back (due to trunk shortening).
Measurements
- Height: Use stadiometer. Loss of > 4cm historical or > 2cm prospective.
- Weight: Low BMI (less than 19 kg/m²).
Spine
- Percussive tenderness over spinous process (acute fracture).
- Range of motion restriction.
Functional Assessment
- Get Up and Go Test: Ability to rise from chair without arms, walk 3m, turn, and sit. > 10 seconds indicates fall risk.
- Neurology: Brief screen (power/sensation) if vertebral fracture suspected (exclude cord compromise).
6. Investigations
Diagnosis: DXA Scan (Dual-energy X-ray Absorptiometry)
- Standard: L1-L4 Spine and Total Hip/Femoral Neck.
- T-Score: Standard deviations from young healthy adult mean.
- Normal: ≥ -1.0
- Osteopenia: -1.0 to -2.5
- Osteoporosis: ≤ -2.5
- Severe Osteoporosis: ≤ -2.5 + Fragility Fracture
- Z-Score: Comparison to age-matched peers. Z-score < -2.0 warrants search for secondary causes.
Risk Stratification: FRAX Tool
- Inputs: Age, Sex, BMI, Previous Fracture, Parent Hip Fracture, Smoking, Steroids, RA, Secondary Causes, Alcohol, Femoral Neck BMD.
- Output: 10-year probability of Major Osteoporotic Fracture (MOF) and Hip Fracture.
- Integration: NOGG charts map FRAX score to action (Reassure, DXA, Treat).
Imaging
- X-Ray (Thoracolumbar Spine): To identify prevalent vertebral fractures. 30-50% bone loss required to be visible on X-ray.
- VFA (Vertebral Fracture Assessment): Lateral spine view done by DXA machine. Lower radiation.
- Isotope Bone Scan: Differentiates acute (hot) vs old (cold) fracture; identifies metastasis.
- MRI Spine: Gold standard for cord compression, metastasis, or differentiating osteoporotic vs malignant fracture.
Laboratory Screen (Secondary Causes)
Mandatory for all new diagnoses.
- Bone Profile: Corrected Calcium, Phosphate, Albumin, ALP.
- High Ca: Hyperparathyroidism, Myeloma, Metastasis.
- Low Ca/Phos, High ALP: Osteomalacia.
- Renal Function: eGFR, Creatinine (CKD-MBD).
- FBC & ESR: Anaemia/ESR ↑ in Myeloma/Malignancy.
- Thyroid Function: TSH (Thyrotoxicosis).
- Vitamin D (25-OH): Deficiency common; must correct before potent antiresorptives (risk of hypocalcaemia).
- Coeliac Screen: Tissue Transglutaminase (tTG).
- Myeloma Screen: Serum Protein Electrophoresis (SPEP) + Serum Free Light Chains (if indicated).
- Men: Testosterone, SHBG, LH/FSH.
- Bone Turnover Markers (Specialist): P1NP (formation), CTX (resorption). Used to monitor adherence and efficacy.
7. Management
Management is guided by fracture risk, not just T-score. The NOGG 2024 guideline introduces the "Very High Risk" category.
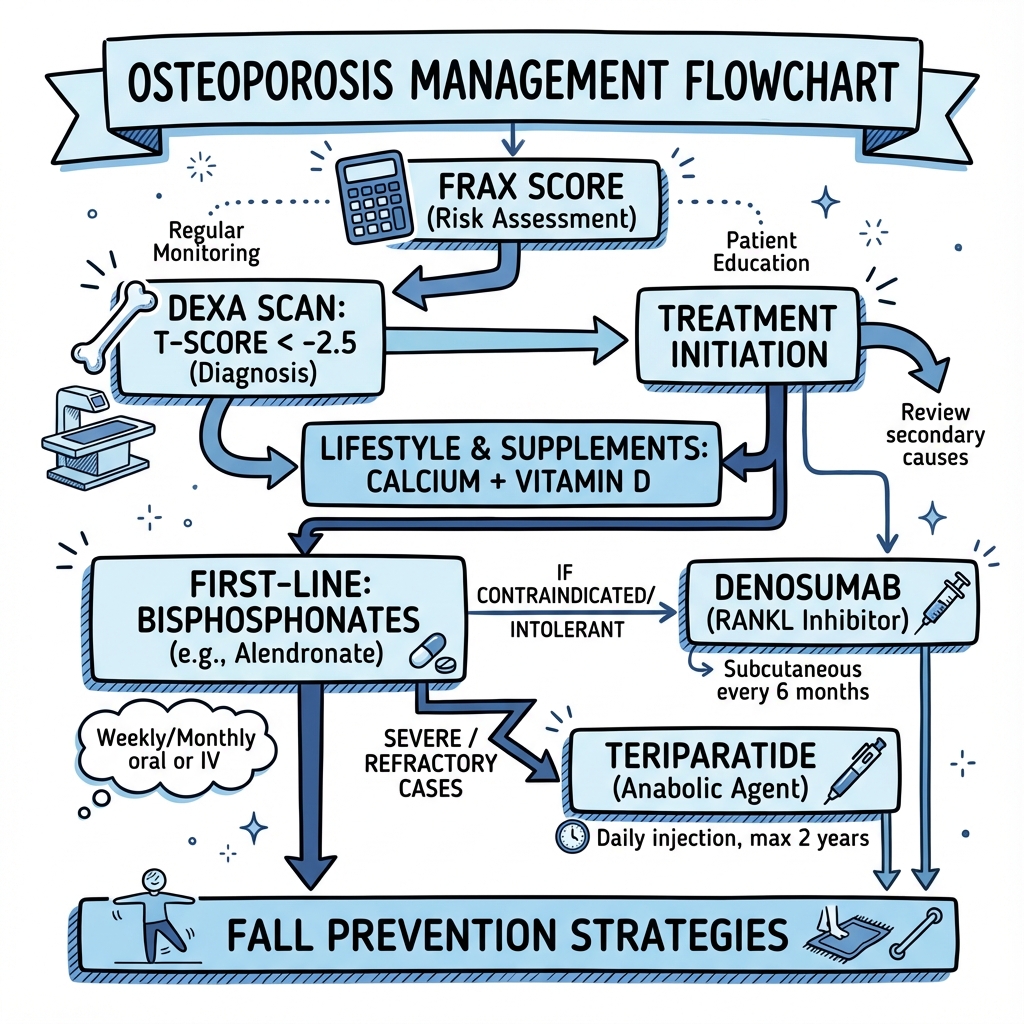
ASCII Management Algorithm
┌─────────────────────────────────────────┐
│ SUSPECTED OSTEOPOROSIS / FRACTURE │
└────────────────────┬────────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ RISK ASSESSMENT (FRAX) │
│ + DXA (if indicated by FRAX) │
└────────────────────┬────────────────────┘
│
┌──────────────────────────┼───────────────────────────┐
▼ ▼ ▼
┌─────────────────┐ ┌─────────────────┐ ┌──────────────────┐
│ LOW RISK │ │ HIGH RISK │ │ VERY HIGH RISK │
└────────┬────────┘ └────────┬────────┘ └─────────┬────────┘
│ │ │
│ │ │
┌────────▼────────┐ ┌────────▼────────┐ ┌─────────▼────────┐
│ LIFESTYLE ONLY │ │ ANTIRESORPTIVE │ │ ANABOLIC FIRST │
│ • Vit D / Calc │ │ • Alendronate │ │ • Romosozumab │
│ • Exercise │ │ • Risedronate │ │ • Teriparatide │
│ • Falls Prev. │ │ • Zoledronate │ │ (For 12-24 mths) │
└─────────────────┘ │ • Denosumab │ └─────────┬────────┘
└────────┬────────┘ │
│ │
│ ◄──────────────────────────┘
│ (Switch to lock in gains)
▼
┌─────────────────┐
│ REVIEW │
│ (3-5 Years) │
└─────────────────┘
1. Lifestyle & Non-Pharmacological
- Nutrition: Calcium 700-1000mg/day (diet preferred). Vitamin D 800IU/day (supplements usually needed in UK).
- Exercise: Combination of weight-bearing (impact) and muscle strengthening.
- Falls Prevention: Physiotherapy, home hazard assessment, sight correction, medication review (stop sedatives).
- Smoking/Alcohol: Cessation and reduction.
2. "Very High Risk" (Anabolic First)
Criteria: Recent fracture (less than 2 yrs), T-score < -3.5, or multiple fractures.
- Romosozumab (Anti-Sclerostin):
- Action: Dual effect (↑Formation, ↓Resorption).
- Dose: 210mg SC monthly x 12 months.
- Evidence: Superior to Alendronate (ARCH trial).
- Contraindication: History of MI or Stroke.
- Teriparatide (PTH Analogue):
- Action: Anabolic (↑Formation).
- Dose: 20mcg SC daily x 24 months.
- Evidence: Superior to Risedronate (VERO trial).
- Note: Must be followed immediately by antiresorptive.
3. "High Risk" (Antiresorptive First)
Criteria: Above intervention threshold but not meeting Very High Risk.
- Oral Bisphosphonates (First Line):
- Alendronate 70mg weekly or Risedronate 35mg weekly.
- Counselling: Take fasting with water, stay upright 30 mins (risk of oesophagitis).
- Duration: Review at 5 years.
- IV Bisphosphonates (Second Line/GI Intolerance):
- Zoledronic Acid 5mg IV annually.
- Side Effects: Acute phase reaction (flu-like) after first dose.
- Duration: Review at 3 years.
- Denosumab (Specialist):
- RANKL Inhibitor. 60mg SC every 6 months.
- Critical Warning: Rebound phenomenon. If missed/stopped, risk of multiple vertebral fractures spikes. Must not be stopped without transition to bisphosphonate.
- Use: Renal failure (safe in CKD), intolerance to bisphosphonates.
4. Glucocorticoid-Induced Osteoporosis (GIOP)
- Threshold for treatment is lower.
- Women > 70 taking > 7.5mg Prednisolone: Start Alendronate immediately (don't wait for DXA).
- Post-menopausal women / Men > 50: Assess with FRAX.
8. Complications
Disease Complications
- Hip Fracture: 20% mortality at 1 year. 50% permanent disability.
- Vertebral Fracture: Chronic pain, height loss, respiratory compromise (severe kyphosis), depression, gastric reflux.
- Social: Loss of independence, need for institutional care.
Treatment Complications
- Bisphosphonate-Related Osteonecrosis of the Jaw (MRONJ):
- Rare (1:10,000 to 1:100,000 patient-years in osteoporosis doses). Higher in oncology doses.
- Risk factors: Dental extractions, poor hygiene.
- Advice: Maintain good dental hygiene. Inform dentist.
- Atypical Femoral Fracture (AFF):
- Stress fractures of femoral shaft.
- Associated with long-term (> 5 yrs) suppression of bone turnover.
- Warning sign: Prodromal thigh/groin pain. X-ray shows cortical thickening ("beaking").
- Management: Stop bisphosphonate, orthopedic pinning.
- Oesophagitis/Gastritis: Common with oral bisphosphonates.
- Hypocalcaemia: Risk with Denosumab/Zoledronate if Vitamin D not replete.
9. Prognosis
- Fracture Risk: One vertebral fracture increases risk of further vertebral fracture 5-fold and hip fracture 3-fold.
- Treatment Efficacy:
- Bisphosphonates reduce vertebral fracture risk by 50-70% and hip fracture by 40-50%.
- Anabolics (Romosozumab) reduce vertebral fracture risk by ~73% vs placebo.
- Recurrence: "Imminent risk" is highest in the first 12-24 months post-fracture.
- Life Expectancy: Reduced following hip fracture, largely due to comorbidities and immobility complications (pneumonia, PE).
10. Evidence & Guidelines
Key Guidelines
- NOGG (2024): National Osteoporosis Guideline Group (UK). Endorses "Anabolic First" for very high risk. Uses hybrid FRAX/intervention thresholds.
- ESCEO/IOF (2020): European guidance supporting risk stratification.
- ASBMR (2020): American Society for Bone and Mineral Research. Recommendations on long-term bisphosphonate use and drug holidays.
Landmark Trials
| Trial | Intervention | Outcome (Hazard Ratio / Risk Reduction) | PMID |
|---|---|---|---|
| FIT (1996) | Alendronate vs Placebo | 47% reduction in vertebral #; 51% reduction in hip # | 8950879 |
| HORIZON-PFT (2007) | Zoledronate vs Placebo | 70% reduction in vertebral #; 41% reduction in hip # | 17476007 |
| FREEDOM (2009) | Denosumab vs Placebo | 68% reduction in vertebral #; 40% reduction in hip # | 19671655 |
| VERO (2017) | Teriparatide vs Risedronate | 56% reduction in new vertebral fractures (Superiority). First head-to-head anabolic vs antiresorptive. | 29129436 |
| ARCH (2017) | Romosozumab vs Alendronate | 48% reduction in new vertebral fractures; 38% reduction in hip fractures. | 28892457 |
| FRAME (2016) | Romosozumab vs Placebo | 73% reduction in vertebral fractures at 12 months. | 27641143 |
11. Patient Explanation
What is Osteoporosis?
"Osteoporosis means 'porous bone'. Think of your bone like a honeycomb. In osteoporosis, the holes in the honeycomb get bigger and the walls get thinner. This makes the bone weak and brittle, so it can break easily from a simple fall."
Why do I need treatment?
"Because you have had a fracture (or have a very low bone scan result), your risk of breaking another bone, particularly your hip, is very high. A hip fracture can be life-changing. The treatment strengthens the bone to prevent this."
How do I take the tablet (Alendronate)?
"Pick one day a week. When you wake up, take the tablet with a full glass of tap water. Do not crush or chew it. You must stay upright (sitting or standing) and not eat, drink (other than water), or take other pills for at least 30 minutes. This ensures the medicine is absorbed and doesn't irritate your food pipe."
How long for?
"We usually treat for 5 years. At that point, we will check your bone density again. We might be able to give you a 'drug holiday' where you stop the tablet for a few years, as the medicine stays in your bones and keeps working."
12. References
- Gregson CL et al. National Osteoporosis Guideline Group (NOGG) 2024: Clinical guideline for the prevention and treatment of osteoporosis. Wait for publication/online. Available at: www.nogg.org.uk.
- Black DM et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Lancet. 1996 Dec 7;348(9041):1535-41. PMID: 8950879.
- Black DM et al. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med. 2007 May 3;356(18):1809-22. PMID: 17476007.
- Cummings SR et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009 Aug 20;361(8):756-65. PMID: 19671655.
- Kendler DL et al. Effects of teriparatide and risedronate on new fractures in post-menopausal women with severe osteoporosis (VERO): a multicentre, double-blind, double-dummy, randomised controlled trial. Lancet. 2018 Jan 20;391(10117):230-240. PMID: 29129436.
- Saag KG et al. Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis (ARCH). N Engl J Med. 2017 Oct 12;377(15):1417-1427. PMID: 28892457.
- Cosman F et al. Romosozumab treatment in postmenopausal women with osteoporosis (FRAME). N Engl J Med. 2016 Oct 20;375(16):1532-1543. PMID: 27641143.
- Kanis JA et al. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2019 Jan;30(1):3-44. PMID: 30324412.
- Eastell R et al. Diagnosis and management of osteoporosis in postmenopausal women and men over 50 years of age in the UK: Clinical Guideline for Prevention and Treatment of Osteoporosis. Arch Osteoporos. 2022;17:15.
- Tsourdi E et al. Discontinuation of Denosumab therapy for osteoporosis: A systematic review and position statement by ECTS. Bone. 2017 Dec;105:11-17. PMID: 28789921.
- Shane E et al. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the ASBMR. J Bone Miner Res. 2014 Jan;29(1):1-23. PMID: 23712442.
- Compston JE et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos. 2017;12(1):43. PMID: 28425085.
- Harvey NC et al. Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures. Osteoporos Int. 2020;31:1-12.
- Baron R, Hesse E. Update on Bone Anabolics in Osteoporosis Treatment: Rationale, Current Status, and Perspectives. J Clin Endocrinol Metab. 2012 Feb;97(2):311–325.
- Khosla S et al. Osteoporosis in the aged: mechanisms and therapy. Nature. 2012;481:284-289.
13. Examination Focus
OSCE Station: Counselling a Patient on Alendronate
Scenario: "Mrs Jones, 68, has just been diagnosed with osteoporosis. Her GP has prescribed Alendronate. Please explain the diagnosis and how to take the medication." Checklist:
- Define: "Thinning of bones, higher risk of fracture."
- Rationale: "Prevents hip/spine fractures."
- Instructions:
- Once weekly (same day).
- First thing in morning.
- Empty stomach.
- Full glass of tap water.
- Stay upright 30 mins (prevent oesophagitis).
- Wait 30 mins before food/coffee/other meds (absorption).
- Side Effects: "Indigestion, heart burn. Rare jaw/thigh problems."
- Dental: "Tell your dentist you are on this medication."
- Duration: "Review in 5 years."
Viva Questions
- "What is the definition of severe osteoporosis?"
- T-score ≤ -2.5 AND presence of one or more fragility fractures.
- "What is the mechanism of action of Denosumab?"
- Monoclonal antibody against RANKL. Prevents RANKL binding to RANK on osteoclasts. Inhibits osteoclast formation and survival.
- "Why must you not stop Denosumab abruptly?"
- Causes a rebound increase in bone turnover (overshoot) and rapid loss of BMD, leading to high risk of multiple vertebral fractures.
- "Name three secondary causes of osteoporosis."
- Hyperparathyroidism, Hyperthyroidism, Cushing's, Multiple Myeloma, Coeliac Disease.
- "When would you consider an anabolic agent first?"
- In "Very High Risk" patients: T-score < -3.5, recent fracture (less than 12-24 months), or multiple vertebral fractures.
Last Updated: 2026-01-04