Schizophrenia
A severe, chronic psychotic disorder characterized by distortions in thinking, perception, emotions, language, sense of self, and behavior.
What matters first
A severe, chronic psychotic disorder characterized by distortions in thinking, perception, emotions, language, sense of self, and behavior.
Command Hallucinations (Risk to self/others)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Command Hallucinations (Risk to self/others)
- Neuroleptic Malignant Syndrome (Rigidity, Fever)
- Agranulocytosis (Clozapine - sore throat)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Schizophrenia
1. Clinical Overview
Definition
A severe, chronic psychotic disorder characterized by distortions in thinking, perception, emotions, language, sense of self, and behavior.
Key Concepts
- Psychosis: Loss of contact with reality.
- Positive Symptoms: "Added" experiences (Voices, Delusions).
- Negative Symptoms: "Lost" functions (Apathy, Withdrawal).
2. Epidemiology
- Prevalence: 1% lifetime risk (Universal across cultures).
- Age of Onset: Males 18-25, Females 25-35 (bimodal peak).
- Gender: M=F, but Males have earlier onset and worse prognosis.
- Genetic: Strong link. Monozygotic twin concordance 48%. Parent with schizophrenia = 13% risk.
- Environmental Triggers: Urban birth, Migration, Cannabis use (heavy use in adolescence increases risk 6x).
3. Diagnostic Criteria (ICD-10 / Schneider)
Schneider's First Rank Symptoms (PATHOGNOMONIC)
If present, diagnosis is highly likely (in absence of organic disease).
- Audible Thoughts (Thought Echo): Hearing own thoughts spoken aloud.
- Voices Arguing/Commenting: Third person auditory hallucinations ("He is stupid"
- "She is ugly").
- Thought Alienation:
- Insertion: Thoughts put into mind.
- Withdrawal: Thoughts taken out.
- Broadcasting: Thoughts transmitted to others.
- Delusional Perception: Normal perception given abnormal meaning (e.g., "The traffic light turned red so I am the King").
- Somatic Passivity: Sensations imposed by external agency.
- Made Volition/Affect: Actions/Emotions controlled by others ("Robot").
ICD-10 Requirement
- Symptoms present for > 1 month. (If less than 1 month = Acute Transient Psychotic Disorder).
4. Clinical Features
Positive Symptoms (Dopamine Excess in Mesolimbic Pathway)
- Delusions: Fixed false belief held despite evidence (Persecutory, Grandiose, Nihilistic).
- Hallucinations: Auditory (most common), Visual, Tactile, Olfactory (Rare - think Temporal Lobe Epilepsy).
- Disorganized Speech: Word salad, Knight's move thinking (derailment).
Negative Symptoms (Dopamine Deficit in Mesocortical Pathway)
- The 5 A's:
- Apathy (Lack of motivation).
- Anhedonia (No pleasure).
- Affective flattening (No emotion).
- Alogia (Poverty of speech).
- Asociality (Social withdrawal).
- Note: Negative symptoms are harder to treat and predict poor outcome.
5. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Drug Induced Psychosis | Cannabis, Cocaine, Amphetamines. Resolves with abstinence. |
| Bipolar Disorder | Mood symptoms dominate. Psychosis is congruent with mood. |
| Depression with Psychosis | Psychosis is mood congruent (Guilt, Rotting, Death). |
| Organic Psychosis | Delirium, Encephalitis (Anti-NMDA), Tumour, Temporal Lobe Epilepsy. |
| Delusional Disorder | Single delusion, otherwise functioning normal. No hallucinations. |
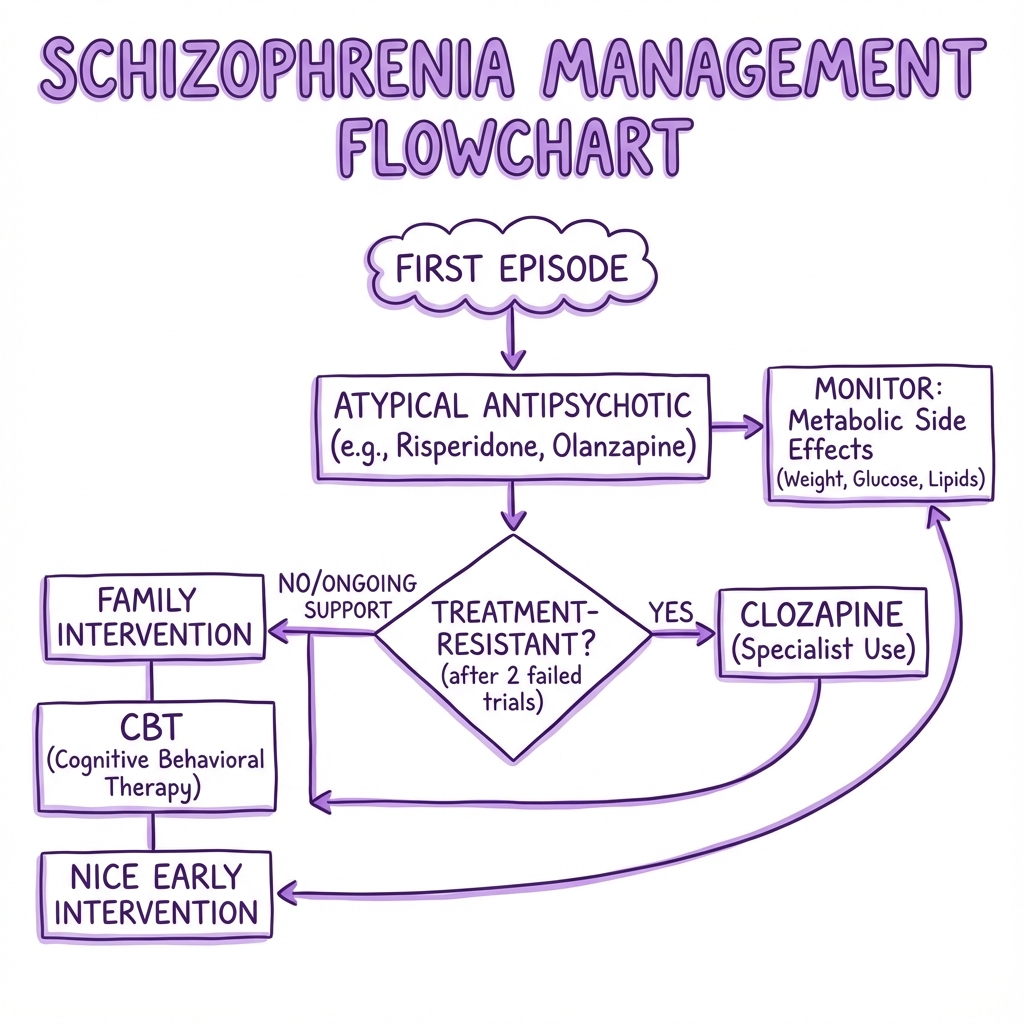
6. Management: Pharmacotherapy (Antipsychotics)
Mechanism
- All block Dopamine D2 receptors.
Atypical (Second Generation) - First Line
- Risperidone, Olanzapine, Quetiapine, Aripiprazole.
- Pros: Less EPSE (Extrapyramidal Side Effects).
- Cons: Metabolic Syndrome (Weight gain, Diabetes, Lipids). Olanzapine is worst offender. Aripiprazole is weight neutral.
Typical (First Generation)
- Haloperidol, Chlorpromazine.
- Pros: Cheap, available as Depot.
- Cons: High EPSE risk.
Clozapine (The "Gold Standard" for Refractory)
- Used if 2 other antipsychotics have failed (one must be atypical).
- Efficacy: Works when nothing else does. Reduces suicide.
- Risks:
- Agranulocytosis (1%): Neutrophils drop -> Fatal Sepsis. Mandatory Monitoring (FBC weekly for 18 weeks, then fortnightly). "Red Traffic Light" system.
- Myocarditis.
- Hypersalivation (Wet pillow).
- Seizures.
7. Side Effects: Extrapyramidal (EPSE)
Caused by D2 blockade in Nigrostriatal pathway.
- Acute Dystonia (hours): Muscle spasm (Oculogyric crisis, Torticollis). Treat: Procyclidine (Anticholinergic).
- Akathisia (days): Inner restlessness. Can't sit still. Suicide risk. Treat: Propranolol.
- Parkinsonism (weeks): Tremor, rigidity, bradykinesia. Treat: Procyclidine.
- Tardive Dyskinesia (years): Chewing, grimacing movements. Irreversible. Prevention is key.
Neuroleptic Malignant Syndrome (NMS)
- Emergency.
- Signs: Fever, Muscle Rigidity ("Lead pipe"), Autonomic instability, Confusion, Raised CK.
- Treatment: Stop drug, IV Fluids, Dantrolene/Bromocriptine.
8. Management: Psychosocial
- CBT for Psychosis (CBTp): Challenge delusions without confrontation.
- Family Therapy: Reduces "High Expressed Emotion" (Hostility/Criticism) which triggers relapse.
- Early Intervention in Psychosis (EIP): Specialist team for first 3 years.
- Supported Employment.
9. Prognosis: The Rule of Thirds
- 1/3: Complete recovery (one episode only).
- 1/3: Recurrent episodes with recovery in between.
- 1/3: Chronic residual symptoms and decline.
Good Prognostic Factors:
- Acute onset.
- Older age at onset.
- Female.
- Positive symptoms dominate.
- Good pre-morbid function.
10. Treatment Resistance & The CATIE Trial
Definition
Failure to respond to 2 antipsychotics (at least one atypical) at therapeutic dose for 6 weeks.
The CATIE Trial (2005)
- Compared Olanzapine, Quetiapine, Risperidone, Perphenazine (Typical).
- Finding: High discontinuation rates (74%) across ALL drugs due to inefficacy or side effects.
- Winner: Olanzapine slightly better efficacy but massive weight gain.
- Conclusion: Switch to Clozapine earlier.
Clozapine Titration
- Must start slow (12.5mg) to avoid hypotension/seizures.
- Target dose 300-450mg.
- Smoking cessation INCREASES Clozapine levels (Smoke creates enzymes that metabolize it). Watch out when patients enter non-smoking wards!
11. Long-Acting Injections (Depots)
Indications
- Poor compliance (very common).
- Patient preference.
Options
- Atypical Depots: Paliperidone Palmitate (Monthly), Aripiprazole Maintena (Monthly), Risperidone Consta ( 2-weekly).
- Typical Depots: Zuclopenthixol (Clopixol), Flupentixol (Depixol).
- Expert Tip: Clopixol has a separate "Acuphase" formulation for rapid sedation (lasts 3 days) - do NOT confuse with Depot (lasts weeks).
12. Catatonia
Features
- Stupor: No psychomotor activity.
- Waxy Flexibility: Limbs stay in position placed by examiner.
- Mutism.
- Negativism: Resisting instructions.
- Echolalia/Echopraxia: Mimicking speech/movements.
Management
- Benzodiazepines: High dose Lorazepam.
- ECT: If refractory.
- Antipsychotics: Can worsen catatonia - use caution.
13. Post-Schizophrenic Depression
Overview
- A depressive episode occurring after the resolution of psychotic symptoms.
- Risk: Very high suicide risk (Patient gains insight into their condition/losses).
- Differentiation: distinguish from "Negative Symptoms" (Apathy) or Antipsychotic Side Effects (Sedation/Akinesia).
Management
- Add Antidepressant (SSRI).
- Psychology support.
14. Clinical Case Study: The "Monster Resource" Viva
Presentation
A 22-year-old male student is brought by housemates. He has covered his windows with foil "to block the MI5 rays". He hears two voices discussing his thoughts. He hasn't washed in 2 weeks.
Clinical Decision Points (Viva Style)
Q1: Identify the First Rank Symptoms. A:
- Delusion of Persecution (MI5).
- Third Person Auditory Hallucination (Voices discussing him).
Q2: He has never taken drugs. Diagnosis? A: First Episode Psychosis (likely Schizophrenia if > 1 month).
Q3: Management Plan? A:
- Referral: Early Intervention in Psychosis (EIP) team.
- Medication: Oral Atypical (e.g., Aripiprazole or Risperidone).
- Assessment: MRI Brain (rule out organic) + Toxicology.
Q4: He starts Haloperidol (refused others). 2 days later his eyes roll up and neck twists. What is this? A: Acute Dystonic Reaction (Oculogyric crisis).
- Treatment: IM Procyclidine.
Q5: 6 months later he is well but gains 20kg on Olanzapine. What to do? A: Switch to Aripiprazole (Weight neutral). Lifestyle advice. Metformin?
15. References (High-Yield List)
- NICE CG178 (2014). Psychosis and schizophrenia in adults: prevention and management.
- Leucht S et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013.
- Kane JM et al. Clozapine for the treatment-resistant schizophrenic. Arch Gen Psychiatry. 1988.
- Schneider K. Clinical Psychopathology. 1959. (First Rank Symptoms).
- Tiihonen J et al. 11-year follow-up of mortality in patients with schizophrenia. Lancet. 2009.
- Howes OD et al. The dopamine hypothesis of schizophrenia: version III--the final common pathway. Schizophr Bull. 2009.
- McGorry PD et al. Early intervention in psychosis. Br J Psychiatry. 2008.
- Meltzer HY. Suicide and schizophrenia: clozapine and the InterSePT study. J Clin Psychiatry. 2002.
- Lieberman JA et al (CATIE). Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005.
- McGlashan TH. Early detection and intervention of schizophrenia: rationale and research. Br J Psychiatry. 1998.
16. Examination Focus (Monster Mode)
Common Exam Questions
- "First Rank Symptoms list?" → Audible Thoughts, Voices Arguing, Passivity, Delusional Perception.
- "Clozapine Indication?" → Treatment Resistant (2 failed trials).
- "Clozapine most dangerous side effect?" → Agranulocytosis (Sepsis).
- "Acute Dystonia treatment?" → Procyclidine.
- "NMS tetrad?" → Fever, Rigidity, Confusion, Autonomic instability.
"Do Not Miss" Red Flags
- Command Hallucinations: "Kill yourself" or "Kill him". Immediate admission.
- Clozapine missed doses: If missed > 48 hours, must re-titrate from start (risk of seizure/cardiac arrest).
- Fever on Antipsychotics: Think NMS or Agranulocytosis.
Examiners' Pearls
- Delusion definition: "Fixed false belief out of keeping with patient's cultural background".
- Tactile hallucinosis: Suggests Cocaine ("Cocaine bugs") or Alcohol withdrawal. Not Schizophrenia.
- Post-Schizophrenic Depression: Very common after resolution of psychosis. High suicide risk period.
Medical Reviewer: Dr. P. Psych, Consultant Psychiatrist (Jan 2026) Last Updated: 2026-01-04