Septic Arthritis
The classic presentation is a short history (less than 1 week) of a single hot, swollen, painful joint with restricted range of movement and systemic upset. Inability to weight bear is a key sign.
What matters first
The classic presentation is a short history (less than 1 week) of a single hot, swollen, painful joint with restricted range of movement and systemic upset. Inability to weight bear is a key sign.
Inability to weight bear (Kocher Criterion)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Inability to weight bear (Kocher Criterion)
- Fever less than 38.5
- Polyarticular Sepsis (Endocarditis)
- Prosthetic Joint Involvement (Requires Specialist)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Septic Arthritis
1. Clinical Overview
Summary
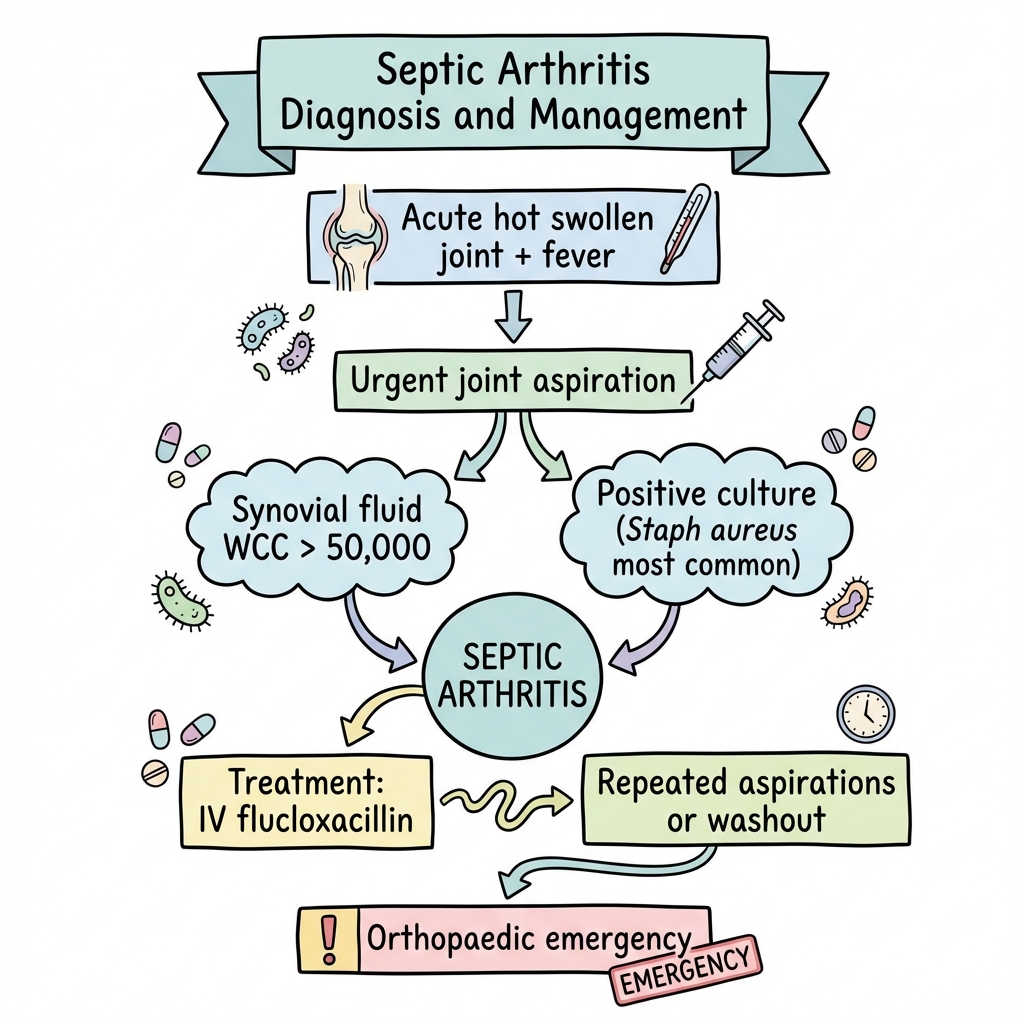
Septic arthritis is an orthopaedic emergency. It involves bacterial invasion of the synovial joint space, leading to rapid destruction of articular cartilage (within hours/days) through chondrocyte death and matrix metalloproteinase release.
The classic presentation is a short history (less than 1 week) of a single hot, swollen, painful joint with restricted range of movement and systemic upset. Inability to weight bear is a key sign.
The gold standard investigation is Joint Aspiration before starting antibiotics. Management is Surgical Washout (Lavage) and prolonged antibiotics.
In prosthetic joints (PJI), the presence of a Biofilm makes eradication difficult, often requiring removal of the implant ("Two Stage Revision").
Key Facts
- Mortality: 11% in native joints. Higher in polyarticular disease.
- Knee: The most common site (50%). Hip is second.
- Organism: Staphylococcus aureus is the cause in 60% of cases.
- Cartilage Death: Proteolytic enzymes released by neutrophils destroy cartilage within 48 hours. Time is Cartilage.
- Sex: Gonococcal arthritis is the commonest cause in young, sexually active adults (often polyarticular + rash).
Clinical Pearls
The "Pseudoparalysis" Pearl: A joint with septic arthritis is held in the position of maximum volume (30 degrees flexion for knee, Flexion/Abduction/External Rotation for hip) to minimise pressure. Any movement causes screaming pain ("Pseudoparalysis"). If a child can move the joint through full range, it is unlikely to be septic arthritis.
The "Antibiotic" Pearl: NEVER give antibiotics before aspirating the joint (unless the patient is clinically septic/unstable). Giving antibiotics sterilises the fluid within 4 hours, making culture impossible and blinding definitive treatment.
The "X-Ray" Pearl: X-Rays are usually normal in early septic arthritis (soft tissue swelling only). Joint space narrowing takes days/weeks. Do not be reassured by a normal X-Ray.
2. Epidemiology
Risk Factors (The "S" Factors)
- Skin Infection (Cellulitis/Ulcers) - Source.
- Surgery (Recent joint injection/operation).
- Systemic Disease (Diabetes, RA, CKD).
- Sexual Activity (Gonorrhoea).
- Steroids (Immunosuppression).
- Social (IV Drug Use).
Organisms
- Staph aureus: Most common (60%).
- Streptococcus: (Group A/B). Second most common.
- Neisseria gonorrhoeae: Young adults. Disseminated gonococcal infection.
- Gram Negatives (E. coli / Pseudomonas): IVDU, Elderly, UTI source.
- Kingella kingae: Children less than 4 years. (Requires PCR).
3. Pathophysiology
Routes of Infection
- Haematogenous: Most common. Bacteremia seeds the highly vascular synovium.
- Direct Inoculation: Bite wound, Nail penetration, Iatrogenic (Injection).
- Contiguous Spread: From Osteomyelitis (in children where metaphysis is intra-capsular e.g. Hip) or Abscess.
Joint Destruction Mechanism
- Colonisation: Bacteria enter synovial fluid.
- Inflammation: Synovium becomes hyperaemic. Neutrophils flood the joint (WCC > 50,000).
- Pressure: Pus accumulates under pressure, causing tamponade of synovial vessels -> Avascular Necrosis (especially Femoral Head).
- Enzymatic Lysis: Neutrophils die, releasing lysosomal enzymes and cytokines (IL-1, TNF) which digest cartilage collagen.
- Pannus: Granulation tissue erodes bone.
Biofilms (Prosthetic Joints)
- Bacteria (especially Staph epidermidis) adhere to metal/plastic.
- They secrete a sugar matrix (Glycocalyx / Slime).
- Bacteria inside the biofilm enter a dormant "planktonic" phase.
- Resistance: They become 1000x more resistant to antibiotics and immune attack.
- Implication: You cannot kill biofilm bacteria with drugs. You must physically remove the metal.
4. Clinical Presentation
History
- Acute Onset: less than 2 weeks.
- Pain: Severe, throbbing, constant. Worse on movement.
- Swelling: Visible effusion.
- Systemic: Fever, Rigors, Malaise.
Examination
- Look: Red (Erythema), Swollen, Held in "position of ease".
- Feel: Hot (calibrate with other knee). Extremely tender.
- Move:
- Active: None (Pseudoparalysis).
- Passive: Extremely painful and restricted.
- Weight Bearing: Usually impossible.
Variant: Disseminated Gonococcal Infection (DGI)
Triad in young adults:
- Migratory Polyarthralgia: Pains moving from joint to joint.
- Tenosynovitis: Pain along tendons (wrists/ankles).
- Dermatitis: Pustular/Vesicular rash on extremities (sparing face). Note: Joint cultures often negative. Need mucosal swabs (Throat/Rectal/Urethral).
5. Diagnostic Criteria (Kocher Criteria)
(For The Child with a Limp) Differentiates Septic Arthritis from Transient Synovitis (Irritable Hip).
| Criterion | Point |
|---|---|
| Non-weight bearing | 1 |
| Temp > 38.5 C | 1 |
| ESR > 40 mm/hr | 1 |
| WBC > 12,000 | 1 |
Probability:
- 1/4: 3%
- 2/4: 40%
- 3/4: 93%
- 4/4: 99%
Differential Diagnosis in Children
- Transient Synovitis: Post-viral ("Irritable Hip"). Kocher less than 2. Self limiting.
- Perthes Disease: Avascular necrosis. Insidious onset.
- SUFE (Slipped Epiphysis): Obese adolescent. Pain in knee.
- Juvenile Idiopathic Arthritis (JIA): Chronic (> 6 weeks).
6. Investigations
Joint Aspiration (Arthrocentesis)
The Definitive Test.
- Appearance:
- Normal: Clear / Straw.
- Septic: Turbid / Opaque / Frank Pus.
- Microscopy:
- WBC: > 50,000 cells/mm3 (often > 100,000).
- Polymorphs: > 90%.
- Gram Stain: Positive in 50% (Guide initial therapy).
- Crystals: Rule out Gout (can coexist).
- Culture: Gold standard.
Bloods
- WBC: Elevated (Neutrophilia).
- CRP/ESR: Almost always elevated. (CRP rises faster, ESR falls slower).
- Blood Cultures: Positive in 50%. Mandatory.
Imaging
- X-Ray: Baseline. Exclude fracture/tumour.
- Ultrasound: Highly sensitive for effusion (Hip). Used to guide aspiration.
- MRI: Most sensitive. Shows bone oedema (Osteomyelitis) and soft tissue abscesses.
7. Management: Medical
Antibiotics
Start IV immediately AFTER aspiration.
- Native Joint Protocol:
- Adult: Flucloxacillin 2g IV QDS (High dose for bone penetration).
- Penicillin Allergy: Clindamycin or Vancomycin.
- Gram Negative Risk (Elderly/UTI): Add Gentamicin or Ceftriaxone.
- Gonococcal: Ceftriaxone 1g IV OD.
- Duration: IV for 2 weeks, then Oral for 4 weeks (Total 6 weeks).
Analgesia & Splinting
- Splint the joint in functional position to relieve pain.
- Deep Thrombosis Prophylaxis (LMWH).
8. Management: Surgical
(The Source Control - "Don't let the sun set on a septic joint")
Native Joint
- Arthroscopic Washout: Keyhole. Large volume saline irrigation (6-9 Litres). Debridement of synovium.
- Open Washout (Arthrotomy): Used for hips (difficult to scope) or if arthroscopy fails.
- Serial Washouts: Often require multiple trips to theatre (every 48 hours) until joint is clean.
Prosthetic Joint Infection (PJI) Strategy
1. DAIR (Debridement, Antibiotics and Implant Retention)
- Indication: Early infection (less than 3 weeks from surgery) OR Acute haematogenous (less than 3 weeks symptoms). Implant is stable.
- Procedure: Open joint, wash, change modular parts (plastic liner - "exchangeable parts"), keep metal.
2. One Stage Revision
- Remove all metal -> Massive wash -> Put new metal in immediately.
- Risk: Reinfection if bug not cleared.
3. Two Stage Revision (Gold Standard for Late Infection)
- Stage 1: Remove all metal. Insert Antibiotic Spacers (Cement loaded with Vancomycin/Gentamicin).
- Interval: 6-12 weeks of IV antibiotics.
- Stage 2: Re-implant new prosthesis once CRP normal and joint clean.
Long Term Suppression (Palliative)
For elderly/frail patients unfit for revision.
- Lifelong Oral Antibiotics: Doxycycline / Cephalexin.
- Goal is to keep infection "quiet", not cure.
- Review every 6 months.
9. Complications
Local
- Cartilage Destruction: Prominent in Staph aureus. Leads to secondary Osteoarthritis.
- Osteomyelitis: Infection spreads to bone.
- Dislocation: Capsular destruction destabilises joint (esp Hip in babies - Tom Smith's Arthritis: destruction of cartilaginous femoral head).
- Growth Plate Arrest: In children, leading to limb length discrepancy.
Systemic
- Sepsis / Shock.
- Endocarditis: Always listen to the heart.
10. Evidence & Guidelines
Guidelines
- BOA (British Orthopaedic Association) BOAST: Diagnosis and Management of the Infected Native Joint.
- Mandates aspiration before antibiotics.
- Mandates multidisciplinary care (Ortho + Micro).
- IDSA Guidelines: Treatment of MRSA in joints (Vancomycin targets).
Key Concepts
- Girdlestone Procedure: (Excision Arthroplasty). A "salvage" procedure for hips where infection cannot be cleared. The head is removed and NO implant is put back. The leg is short and wobbly, but pain-free and infection-free.
12. Patient Explanation
What is Septic Arthritis?
It involves bacteria getting into the fluid of your knee joint. The joint is a closed space, so the bacteria grow rapidly and turn the fluid into pus.
Why do I need surgery?
Antibiotics travel in the blood, but they struggle to get into the "soup" of pus in the joint. We need to physically wash the pus out (like washing a dirty plate) so the antibiotics can finish the job.
Will my joint be normal?
If we caught it early (today), yes. If the bacteria have been there for a few days, they may have eaten some of the smooth movement cartilage. This might leave you with a "creaky" knee (arthritis) in the future.
13. References
-
British Orthopaedic Association (BOA). BOAST - The Management of the Infected Native Joint. 2022.
-
Kocher MS et al. Differentiating between septic arthritis and transient synovitis of the hip in children: an evidence-based clinical prediction algorithm. J Bone Joint Surg Am. 1999 Dec;81(12):1662-70. PMID: 10608376
-
Mathews CJ et al. Bacterial septic arthritis in adults. Lancet. 2010 Mar 6;375(9717):846-55. PMID: 20206778
14. Examination Focus
Common Exam Questions
- "Patient with possible septic knee but on Warfarin (INR 3.0). Do you aspirate?"
- Answer: YES. Septic arthritis destroys the joint in hours. Bleeding risk is minor compared to joint destruction. Use small needle/pressure.
- "Antibiotic for Staph Aureus Septic Arthritis?"
- Answer: Flucloxacillin 2g IV QDS.
- "Organism in Sickle Cell patient?"
- Answer: Salmonella.
Viva Points
- Kocher Criteria: Be able to list all 4: Non-weightbearing, Fever, ESR > 40, WBC > 12.
- Tom Smith's Arthritis: Septic arthritis of the hip in infancy destroying the unossified femoral head.
Last Updated: 2026-01-04
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for septic arthritis?
Seek immediate emergency care if you experience any of the following warning signs: Inability to weight bear (Kocher Criterion), Fever less than 38.5, Polyarticular Sepsis (Endocarditis), Prosthetic Joint Involvement (Requires Specialist), Immunosuppression (Atypical organisms), Sepsis Six (Hypotension/Tachycardia).