Ulcerative Colitis (Adult)
Ulcerative colitis (UC) is a chronic, idiopathic inflammatory bowel disease (IBD) characterized by continuous mucosal inflammation of the colon, always involving the rectum and extending proximally to varying degrees....
What matters first
Ulcerative colitis (UC) is a chronic, idiopathic inflammatory bowel disease (IBD) characterized by continuous mucosal inflammation of the colon, always involving the rectum and extending proximally to varying degrees....
Severe abdominal pain and distension (suggests toxic megacolon)
3 Jan 2026
Generated educational material; verify before clinical use.
22 cited sources
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Severe abdominal pain and distension (suggests toxic megacolon)
- High fever and tachycardia in an acute flare
- Profuse bloody diarrhea (less than 6-10 times per day)
- Signs of peritonitis (suggests perforation)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Ulcerative Colitis (Adult)
1. Clinical Overview
Summary
Ulcerative colitis (UC) is a chronic, idiopathic inflammatory bowel disease (IBD) characterized by continuous mucosal inflammation of the colon, always involving the rectum and extending proximally to varying degrees. Unlike Crohn's disease, which can affect any part of the gastrointestinal tract and is transmural, UC is limited to the colon and involves only the mucosa and submucosa. The clinical course is typically one of relapses and remissions, with symptoms including bloody diarrhea, urgency, tenesmus, and abdominal pain. The diagnosis is established through a combination of clinical suspicion, biochemical markers (e.g., fecal calprotectin), and definitive endoscopic and histological findings. Management is stratified by disease severity and extent, ranging from topical 5-aminosalicylates (5-ASAs) for mild proctitis to systemic corticosteroids, biologics (e.g., TNF-alpha inhibitors), and small molecules (e.g., JAK inhibitors) for moderate-to-severe disease. Surgery (total proctocolectomy) is curative but reserved for medically refractory cases or complications such as dysplasia or toxic megacolon.
Key Facts
- Definition: Chronic inflammatory disease of the colonic mucosa, starting in the rectum and extending proximally.
- Distribution: Continuous and circumferential; limited to the colon.
- Core Symptoms: Bloody diarrhea, rectal urgency, tenesmus, and mucus discharge.
- Pathology: Mucosal inflammation, crypt abscesses, and goblet cell depletion; no granulomas.
- Diagnosis: Colonoscopy with biopsy is the gold standard.
- First-line Treatment: 5-aminosalicylates (Mesalazine) for induction and maintenance of remission.
- Extraintestinal Manifestations: Primary Sclerosing Cholangitis (PSC), erythema nodosum, uveitis, and ankylosing spondylitis.
- Cancer Risk: Increased risk of colorectal cancer (CRC) after 8-10 years of disease, requiring surveillance.
Clinical Pearls
"UC always starts in the rectum" — If the rectum is spared (in an untreated patient), think Crohn's disease or another form of colitis. UC is a "bottom-up" disease.
"Continuous, not patchy" — UC inflammation is continuous and circumferential. "Skip lesions" are a hallmark of Crohn's, not UC.
"Fecal calprotectin is your best friend" — A very sensitive marker for intestinal inflammation. Use it to distinguish IBD from Irritable Bowel Syndrome (IBS) and to monitor for subclinical flares.
"Smoking is 'protective' in UC" — Paradoxically, UC is more common in non-smokers and ex-smokers. However, smoking cessation is still advised for overall health, though it may trigger a flare.
Why This Matters Clinically
Ulcerative colitis is a lifelong condition that significantly impacts quality of life and carries risks of life-threatening complications. Acute severe ulcerative colitis (ASUC) is a medical emergency with a 10-20% risk of requiring emergency colectomy. Furthermore, the association with Primary Sclerosing Cholangitis (PSC) significantly increases the risk of both colorectal and cholangiocarcinoma. Clinicians must be adept at risk-stratifying patients, monitoring for treatment response, and implementing long-term cancer surveillance.
2. Epidemiology
Incidence & Prevalence
- Prevalence: Approximately 200-300 per 100,000 people in Western populations.
- Incidence: 10-20 per 100,000 person-years.
- Geography: Highest in North America, Northern Europe, and Australia; incidence is rapidly rising in newly industrialized countries (Asia, South America).
- Age of Onset: Bimodal distribution; primary peak between 15-30 years, secondary smaller peak between 50-70 years.
Demographics
| Factor | Details |
|---|---|
| Age | Most commonly diagnosed in young adulthood (20s and 30s). |
| Sex | Slight male predominance in older age groups; roughly equal in younger groups. |
| Ethnicity | Higher incidence in Jewish populations (especially Ashkenazi) and Caucasians. |
| Socioeconomic | More common in urban areas and higher socioeconomic groups. |
Risk Factors
Genetic Factors:
- ~10-15% of patients have a first-degree relative with IBD.
- Multiple susceptibility loci identified (e.g., HLA-DRB1*0103).
Environmental & Lifestyle Factors:
| Factor | Association | Mechanism |
|---|---|---|
| Smoking | Protective (Non-smokers > Smokers) | May increase mucus production or alter blood flow. |
| Appendectomy | Protective (if done early for appendicitis) | May alter the immune response in the gut. |
| NSAID Use | Increased risk of flares | Impairs mucosal barrier function. |
| Diet | High fat/sugar may increase risk | Alters gut microbiome (dysbiosis). |
| Antibiotics | Early life exposure increases risk | Disrupts normal gut flora development. |
| Infection | Enteric infections may trigger onset | "Hit and run" immune activation. |
3. Pathophysiology
The Inflammatory Cascade
Step 1: Epithelial Barrier Dysfunction
- Increased intestinal permeability ("leaky gut") allows luminal antigens (bacteria, food) to penetrate the mucosal layer.
- Defects in the mucus layer (produced by goblet cells) reduce the physical barrier between bacteria and the epithelium.
Step 2: Dysbiosis & Antigen Presentation
- An imbalance in the gut microbiome (reduced diversity, increased Proteobacteria) triggers an abnormal immune response.
- Dendritic cells and macrophages in the lamina propria sample these antigens and present them to T-cells.
Step 3: Th2-Mediated Immune Response
- UC is primarily characterized by an atypical Th2 response (unlike the Th1/Th17 response in Crohn's).
- Natural Killer T (NKT) cells produce large amounts of Interleukin-13 (IL-13), which is directly cytotoxic to epithelial cells.
Step 4: Cytokine Storm & Neutrophil Recruitment
- Pro-inflammatory cytokines (TNF-alpha, IL-1-beta, IL-6) are released.
- Chemokines (e.g., IL-8) recruit neutrophils from the bloodstream into the mucosa.
- Neutrophils migrate through the epithelium, forming "crypt abscesses."
Step 5: Mucosal Damage & Ulceration
- Release of reactive oxygen species (ROS) and proteases by activated immune cells leads to tissue destruction.
- This results in the characteristic continuous ulceration, loss of vascular pattern, and friability seen on endoscopy.
Anatomical Extent (Montreal Classification)
| Category | Extent | Description |
|---|---|---|
| E1: Proctitis | Rectum only | Limited to the distal 10-12 cm. |
| E2: Left-sided | Up to Splenic Flexure | Involves rectum, sigmoid, and descending colon. |
| E3: Extensive | Beyond Splenic Flexure | Includes "Pancolitis" (involving the whole colon). |
4. Clinical Presentation
Gastrointestinal Symptoms
1. Diarrhea
- Usually chronic (> 4 weeks).
- Often nocturnal (a key sign of organic rather than functional disease).
- Classically contains blood and mucus.
2. Rectal Symptoms
- Urgency: The "must go now" feeling (due to rectal inflammation and reduced compliance).
- Tenesmus: The painful, ineffective urge to defecate.
- Proctalgia: Rectal pain.
3. Abdominal Pain
- Often crampy, lower abdominal pain.
- Frequently relieved by defecation.
4. Systemic Features (in Moderate-to-Severe Flares)
- Fever, malaise, and fatigue.
- Weight loss and anorexia.
- Anemia (due to chronic blood loss and inflammation).
Extraintestinal Manifestations (EIMs)
| System | Manifestation | Relation to Bowel Activity |
|---|---|---|
| Hepatobiliary | Primary Sclerosing Cholangitis (PSC) | Independent (does not follow flares). |
| Skin | Erythema Nodosum | Parallel (occurs during flares). |
| Skin | Pyoderma Gangrenosum | Independent (can occur in remission). |
| Joints | Type 1 Peripheral Arthritis (large joints) | Parallel (follows bowel activity). |
| Joints | Ankylosing Spondylitis / Sacroiliitis | Independent. |
| Eyes | Episcleritis / Uveitis | Episcleritis (Parallel); Uveitis (Independent). |
Red Flags
[!CAUTION] Red Flags — Acute Severe Ulcerative Colitis (ASUC):
- Stool frequency ≥6 per day — Plus any systemic toxicity.
- Tachycardia (> 90 bpm) — Sign of systemic inflammation or hypovolemia.
- Fever (> 37.8°C) — Suggests severe inflammation or secondary infection.
- Anemia (Hb less than 10.5 g/dL) — Significant blood loss.
- Elevated ESR/CRP — Objective markers of severe inflammation.
- Abdominal distension/tenderness — Risk of toxic megacolon.
5. Clinical Examination
General Assessment
- Vital Signs: Check for tachycardia, fever, and hypotension (signs of ASUC).
- Nutritional Status: Look for muscle wasting, pallor (anemia), or peripheral edema (hypoalbuminemia).
Abdominal Examination
- Inspection: Distension (toxic megacolon?).
- Palpation: Tenderness (usually lower left quadrant). Guarding or rebound tenderness suggests perforation.
- Percussion: Loss of liver dullness (suggests free air from perforation).
Rectal Examination (PR)
- Essential in the initial workup.
- Findings: Tenderness, blood, mucus, and assessment of anal sphincter tone.
- Note: Rule out perianal disease (more common in Crohn's).
Extraintestinal Signs
- Skin: Tender red nodules on shins (Erythema Nodosum); deep ulcers (Pyoderma Gangrenosum).
- Eyes: Redness, pain, or photophobia.
- Joints: Swelling or reduced range of motion.
- Liver: Jaundice or hepatomegaly (PSC).
6. Investigations
Laboratory Tests
1. Fecal Calprotectin (FC)
- The most useful non-invasive test.
- Interpretation: less than 50 μg/g (Normal); > 250 μg/g (Highly suggestive of IBD).
- Use: Screening for IBD and monitoring for relapse.
2. Blood Tests
- FBC: Anemia (iron deficiency or chronic disease), leukocytosis (flare or infection).
- CRP/ESR: Markers of systemic inflammation (CRP is more dynamic).
- Albumin: Low levels indicate severe disease and poor prognosis.
- LFTs: Check for cholestatic pattern (elevated ALP/GGT) suggesting PSC.
- Iron Studies: Assess for deficiency.
3. Stool Microbiology
- Mandatory in every flare to rule out infection.
- Tests: C. difficile toxin, culture for Salmonella, Shigella, Campylobacter, and E. coli O157.
Endoscopy (The Gold Standard)
1. Flexible Sigmoidoscopy
- Often sufficient in an acute flare to confirm diagnosis and assess severity.
- Findings: Loss of vascular pattern, erythema, friability (bleeding on contact), and ulceration.
2. Colonoscopy
- Required to determine the full extent of disease (Montreal classification).
- Biopsy: Essential to confirm UC and rule out Crohn's or CMV colitis.
- Histology: Crypt distortion, crypt abscesses, and basal plasmacytosis.
Imaging
- Abdominal X-ray (AXR): Essential in ASUC to rule out toxic megacolon (transverse colon diameter > 6 cm).
- CT/MRI Abdomen: Useful to rule out complications (abscess, perforation) or to assess for Crohn's (small bowel involvement).
- MRCP: If PSC is suspected.
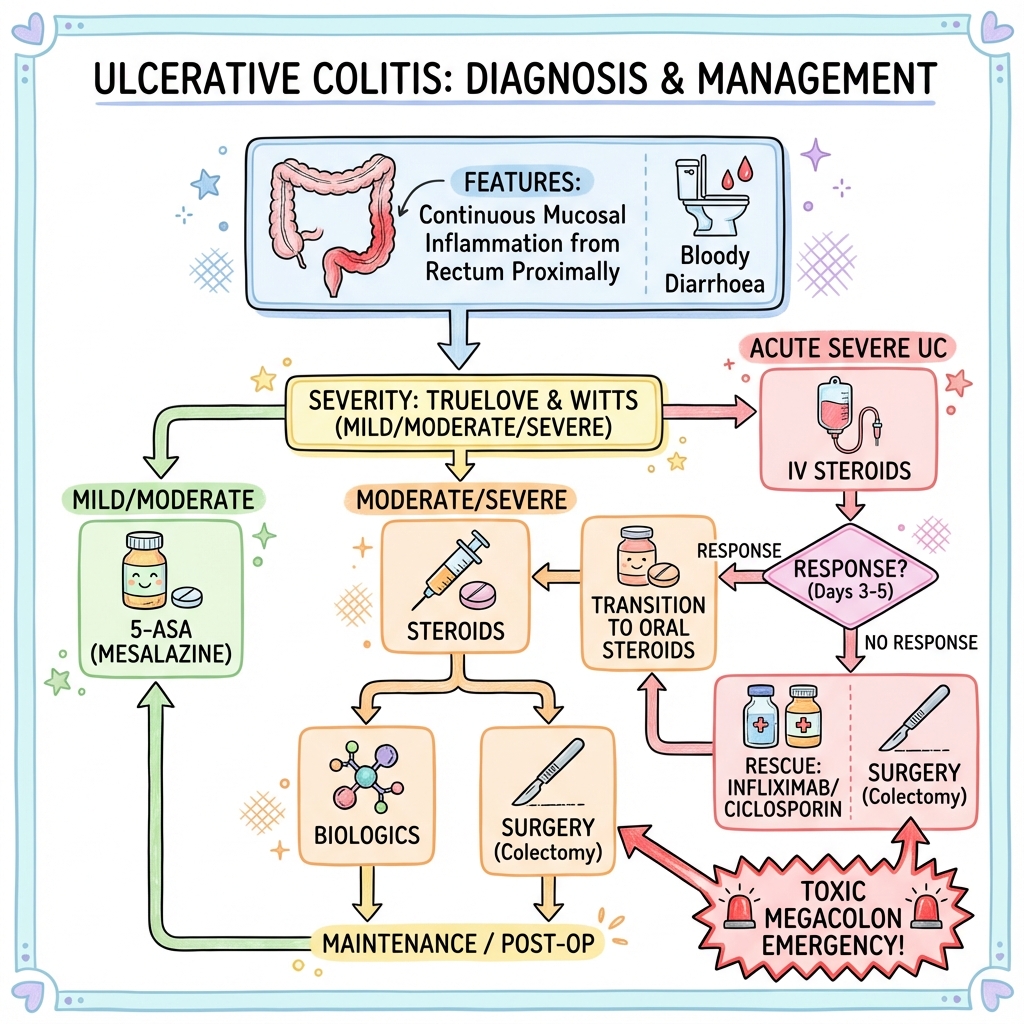
7. Management
Management Algorithm
DIAGNOSIS OF ULCERATIVE COLITIS
(Clinical + Endoscopic + Histological)
↓
┌─────────────────────────────────────────────────┐
│ ASSESS SEVERITY (Truelove & Witts) │
└─────────────────────────────────────────────────┘
/ | \
┌─────────────────┐ ┌─────────────────┐ ┌─────────────────┐
│ MILD │ │ MODERATE │ │ SEVERE │
│ (less than 4 stools/day) │ │ (4-6 stools/day)│ │ (> 6 stools/day) │
├─────────────────┤ ├─────────────────┤ ├─────────────────┤
│ • Topical 5-ASA │ │ • Oral 5-ASA │ │ • ADMIT TO HOSP │
│ (if proctitis) │ (High dose) │ │ • IV STEROIDS │
│ • Oral 5-ASA │ • Oral Steroids │ │ • VTE Prophylax │
│ (if extensive) │ (Prednisolone) │ │ • Surgical Rev. │
└─────────────────┘ └─────────────────┘ └─────────────────┘
↓
┌─────────────────────────────────────────────────┐
│ MAINTENANCE OF REMISSION │
├─────────────────────────────────────────────────┤
│ FIRST-LINE: 5-ASA (Oral +/- Topical) │
│ │
│ IF 5-ASA FAILS: │
│ • Thiopurines (Azathioprine) │
│ • Biologics (Infliximab, Adalimumab, Vedolizumab)│
│ • Small Molecules (Tofacitinib, Ozanimod) │
└─────────────────────────────────────────────────┘
↓
┌─────────────────────────────────────────────────┐
│ SURGICAL INTERVENTION │
│ (If medically refractory or complications) │
├─────────────────────────────────────────────────┤
│ • Total Proctocolectomy │
│ • Ileal Pouch-Anal Anastomosis (IPAA) │
│ • Permanent Ileostomy │
└─────────────────────────────────────────────────┘
Pharmacotherapy
1. 5-Aminosalicylates (5-ASAs)
- Drugs: Mesalazine, Sulfasalazine.
- Use: Induction and maintenance in mild-to-moderate disease.
- Note: Topical (suppositories/enemas) are more effective than oral for distal disease.
2. Corticosteroids
- Drugs: Prednisolone (oral), Hydrocortisone (IV), Budesonide (topical/MMX).
- Use: Induction of remission only. Never for maintenance.
3. Immunomodulators
- Drugs: Azathioprine, Mercaptopurine.
- Use: Maintenance of remission in steroid-dependent or refractory patients.
- Monitoring: Check TPMT activity before starting; monitor FBC and LFTs.
4. Biologics & Small Molecules
- Anti-TNF: Infliximab, Adalimumab.
- Anti-Integrin: Vedolizumab (gut-selective).
- JAK Inhibitors: Tofacitinib (oral).
- IL-12/23 Inhibitor: Ustekinumab.
Management of Acute Severe UC (ASUC)
- IV Hydrocortisone (100mg QDS) or Methylprednisolone.
- Day 3 Assessment: If CRP > 45 or stool frequency > 8, 85% will need surgery.
- Rescue Therapy: IV Infliximab or Ciclosporin.
8. Complications
Acute Complications
- Toxic Megacolon: Non-obstructive colonic dilatation > 6 cm with systemic toxicity. High risk of perforation.
- Perforation: Usually a complication of toxic megacolon; requires emergency surgery.
- Massive Hemorrhage: Rare but life-threatening.
Chronic Complications
- Colorectal Cancer (CRC): Risk increases with duration (> 8-10 years) and extent (pancolitis).
- Strictures: Rare in UC (unlike Crohn's); any stricture in UC is malignant until proven otherwise.
- Cholangiocarcinoma: In patients with concomitant PSC.
- Osteoporosis: Due to chronic inflammation and steroid use.
9. Prognosis
- Course: 90% of patients have a relapsing-remitting course.
- Surgery: ~15-20% of patients will eventually require a colectomy.
- Mortality: Overall mortality is not significantly increased, but ASUC remains a high-risk event.
- Cancer Risk:
- 2% at 10 years.
- 8% at 20 years.
- 18% at 30 years.
- Surveillance: Colonoscopy every 1-5 years depending on risk factors (PSC, family history, severity of inflammation).
10. Evidence
Landmark Trials
- ACT 1 & 2 Trials (2005): Established Infliximab as effective for induction and maintenance in moderate-to-severe UC. PMID: 16339094.
- GEMINI 1 Trial (2013): Demonstrated the efficacy of Vedolizumab (gut-selective) in UC. PMID: 23964932.
- OCTAVE Trials (2017): Established Tofacitinib (JAK inhibitor) as an effective oral option for UC. PMID: 28467869.
- VARSITY Trial (2019): First head-to-head biologic trial; showed Vedolizumab was superior to Adalimumab for clinical remission. PMID: 31553869.
Guidelines
- NICE Guideline [NG130]: Ulcerative colitis: management.
- ECCO Guidelines: European evidence-based consensus on the diagnosis and management of ulcerative colitis.
- ACG Guidelines: American College of Gastroenterology guidelines for ulcerative colitis in adults.
11. Patient Education
Key Counseling Points
- Adherence: Emphasize that maintenance therapy is required even when feeling well to prevent flares and reduce cancer risk.
- Cancer Surveillance: Explain the need for regular colonoscopies after 8-10 years.
- Diet: No specific "IBD diet" is proven, but a low-residue diet may help during a flare.
- Smoking: Advise against starting smoking, but warn that stopping may trigger a flare (manage with IBD team).
- Pregnancy: Most IBD medications (except Methotrexate and some small molecules) are safe in pregnancy. Remission at conception is key.
Support Resources
- Crohn's & Colitis UK / Crohn's & Colitis Foundation (US).
- IBD Nurse Specialists: Essential for long-term management and rapid access during flares.
12. References
- Ungaro R, et al. Ulcerative colitis. Lancet. 2017;389(10080):1756-1770. PMID: 28007310.
- Magro F, et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileopouch Disorders. J Crohns Colitis. 2017;11(6):649-670. PMID: 28158501.
- Rutgeerts P, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353(23):2462-2476. PMID: 16339094.
- Feagan BG, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369(8):699-710. PMID: 23964932.
- Sandborn WJ, et al. Tofacitinib as Induction and Maintenance Therapy for Ulcerative Colitis. N Engl J Med. 2017;376(18):1723-1736. PMID: 28467869.
- Sands BE, et al. Vedolizumab versus Adalimumab for Moderate-to-Severe Ulcerative Colitis. N Engl J Med. 2019;381(13):1215-1226. PMID: 31553869.
- Truelove SC, Witts LJ. Cortisone in ulcerative colitis; final report on a therapeutic trial. Br Med J. 1955;2(4947):1041-1048. PMID: 13260656.
- Turner D, et al. Management of Acute Severe Ulcerative Colitis: A Clinical Update. Gastroenterology. 2012;142(3):454-461. PMID: 22245665.
- Eaden JA, et al. The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut. 2001;48(4):526-535. PMID: 11247898.
- Kobayashi T, et al. Ulcerative colitis. Nat Rev Dis Primers. 2020;6(1):74. PMID: 32913180.
- NICE. Ulcerative colitis: management. [NG130]. 2019.
- Rubin DT, et al. ACG Clinical Guideline: Ulcerative Colitis in Adults. Am J Gastroenterol. 2019;114(3):384-413. PMID: 30840605.
- Beaugerie L, Itzkowitz SH. Cancers complicating inflammatory bowel disease. N Engl J Med. 2015;372(15):1441-1452. PMID: 25853987.
- Ordás I, et al. Ulcerative colitis. Lancet. 2012;380(9853):1606-1619. PMID: 22914406.
- Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med. 2011;365(18):1713-1725. PMID: 22040678.
13. Examination Focus
The "Opening Statement" for a UC Case
"This patient presents with a chronic history of bloody diarrhea, rectal urgency, and tenesmus, associated with raised fecal calprotectin and systemic markers of inflammation. The clinical picture is highly suggestive of ulcerative colitis, likely involving at least the left side of the colon."
Common Viva Questions
- How do you distinguish UC from Crohn's disease? (Continuous vs skip lesions, mucosal vs transmural, rectum always involved vs often spared, no granulomas vs granulomas).
- What are the Truelove and Witts criteria? (Used to define ASUC: > 6 stools/day + fever, tachycardia, anemia, or high ESR).
- What is the management of Acute Severe UC? (IV steroids, VTE prophylaxis, daily AXR, surgical review, rescue therapy with Infliximab/Ciclosporin if no response by day 3).
- What is the risk of colorectal cancer in UC? (Increases after 8-10 years; requires surveillance colonoscopy).
- What is the significance of PSC in a UC patient? (Significantly higher risk of CRC and cholangiocarcinoma; requires annual surveillance).
Common Mistakes to Avoid
- Forgetting the stool cultures: Never start steroids without ruling out C. diff and other infections.
- Using steroids for maintenance: Steroids are for induction only; always have a plan for steroid-sparing maintenance.
- Missing toxic megacolon: Always perform an AXR in a severe flare.
- Ignoring the rectum: Remember that UC always involves the rectum; if it's spared, reconsider the diagnosis.