Paeds · acute-care-resuscitation-and-toxicology
Cardiogenic and obstructive shock
Also known as Paediatric cardiogenic shock · Obstructive shock in children · Cardiac tamponade · Tension pneumothorax · Low cardiac output syndrome · Pump failure shock
Fellowship guide to paediatric cardiogenic and obstructive shock: recognising the low cardiac output state from pump failure versus mechanical obstruction, the distinguishing bedside signs of cardiac tamponade (Beck triad, pulsus paradoxus) and tension pneumothorax, the cautious fluid and inotrope strategy for cardiogenic shock, the emergency needle decompression and pericardiocentesis that reverse obstructive shock, and the ANZ, AHA and European guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Shock is the failure of the cardiovascular system to deliver enough oxygen to the tissues to meet metabolic demand. It is not defined by a blood pressure reading — a child can be in shock with a normal blood pressure, because compensatory tachycardia and vasoconstriction keep the pressure up until late. Shock becomes decompensated when the blood pressure falls below the fifth percentile for age, and this is the threshold at which mortality rises steeply.[1][2]
Paediatric shock is classified by its mechanism into four types: hypovolaemic (loss of volume), distributive (vasodilation, as in sepsis or anaphylaxis), cardiogenic (pump failure), and obstructive (mechanical obstruction to forward flow). This page owns the last two types. Cardiogenic shock is the failure of the heart to generate an adequate cardiac output because of impaired contractility, a structural lesion, or a pathological rhythm. Obstructive shock is the failure of forward flow because something mechanical is blocking the heart or the great vessels: cardiac tamponade, tension pneumothorax, or massive pulmonary embolism.[1][3]
The reason cardiogenic and obstructive shock are grouped together is that they share a cold, low-output phenotype and, crucially, they are the two shock types where aggressive fluid resuscitation can harm. Both demand early vasoactive support or physical decompression rather than the large-volume crystalloid boluses that rescue hypovolaemic and septic shock. Recognising the type within the first minutes of assessment is the skill that separates the safe from the dangerous resuscitation.[1]
Classification
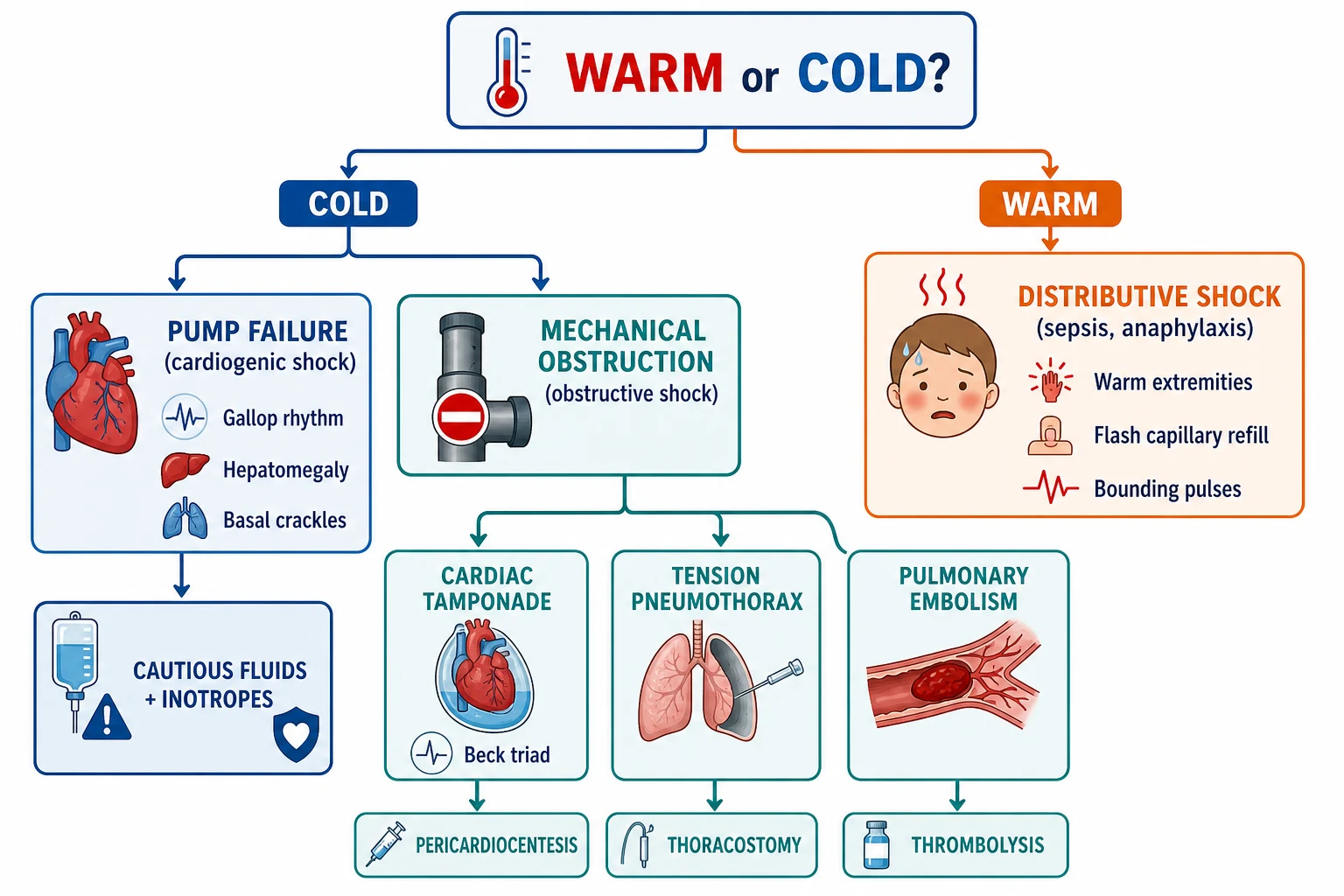
The first classification decision at the bedside is whether the shock is warm or cold, because this sorts distributive shock (warm, vasodilated, flash capillary refill) from cardiogenic, obstructive and late hypovolaemic shock (cold, vasoconstricted, prolonged capillary refill). Within the cold group, the next decision is whether the problem is the pump (cardiogenic) or the plumbing (obstructive), and that decision turns on the lungs, the heart sounds, and the neck veins.[1][2]
Cardiogenic shock
- Cause is pump failure: myocarditis, cardiomyopathy, congenital heart disease, arrhythmia, post-cardiac surgery low cardiac output syndrome, sepsis-induced myocardial dysfunction, drug toxicity
- Cold peripheries, weak or bounding-but-thready pulses, prolonged capillary refill over 2 seconds, mottled skin, oliguria, altered consciousness
- Examination clues: gallop rhythm, hepatomegaly, basal crackles, cool extremities despite warm core; blood pressure preserved then falls late
- Management: cautious 5 to 10 mL per kg fluid boluses with reassessment, early inotropes (adrenaline, dobutamine, milrinone), mechanical support (ECMO) for refractory cases
Obstructive shock
- Cause is mechanical obstruction: cardiac tamponade, tension pneumothorax, massive pulmonary embolism, duct-dependent congenital heart disease with obstruction
- Cold peripheries with distended neck veins (unlike flat neck veins of hypovolaemia), narrow pulse pressure, muffled or absent heart sounds (tamponade) or unilateral absent breath sounds (tension pneumothorax)
- Recognised by the obstructive triad and confirmed by point-of-care ultrasound: pericardial effusion with right ventricular collapse in diastole, lung point or absent lung sliding, or right heart strain
- Management: immediate physical reversal of the obstruction — needle or finger thoracostomy, pericardiocentesis, thrombolysis — then vasoactive support
Cold versus warm at the bedside
- Warm shock (distributive): wide pulse pressure, warm dry skin, flash capillary refill under 1 second, bounding pulses — typical of early sepsis and anaphylaxis
- Cold shock (cardiogenic, obstructive, hypovolaemic): narrow pulse pressure, cold mottled skin, capillary refill over 2 seconds, weak thready pulses
- Most paediatric septic shock is cold shock, unlike the warm vasodilatory shock typical of adults — this is why early fluid and adrenaline dominate the paediatric sepsis algorithm
- A child who remains cold after fluid boluses has cardiogenic or obstructive shock until proven otherwise — stop the fluids and look for the pump or the obstruction
Severity
Shock severity
Epidemiology & Risk Factors
Cardiogenic and obstructive shock are far less common than septic or hypovolaemic shock in children, which is exactly why they are missed. Together they account for a minority of paediatric shock presentations, but they carry a disproportionate mortality because they are not reversed by the fluids that rescue the common types. The recognition skill is to spot the exception among the rule.[1][2]
The dominant causes of cardiogenic shock in children shift with age. In infants, the leading causes are duct-dependent congenital heart disease that presents as acidotic shock when the ductus arteriosus closes in the first days of life, myocarditis, and supraventricular tachycardia. In older children and adolescents, myocarditis, cardiomyopathy, arrhythmia, drug toxicity, and post-cardiac surgical low cardiac output syndrome dominate. Sepsis itself can produce a sepsis-induced myocardial dysfunction that behaves as a mixed cardiogenic and distributive shock.[1][4]
Obstructive shock causes are age-dependent too. Cardiac tamponade in children most often follows post-pericardiotomy syndrome after cardiac surgery, urarena or bacterial pericarditis, malignant effusion in oncology patients, and trauma. Tension pneumothorax follows blunt or penetrating chest trauma, asthma, positive-pressure ventilation (especially in the ventilated neonate or child with lung disease), and central line insertion. Massive pulmonary embolism is rare but rising in adolescents with central venous catheters, oral contraceptives, obesity, immobility, prothrombotic conditions, and COVID-19 or MIS-C.[3][9][11]
The children at highest risk are those with complex congenital heart disease and cardiac surgical substrates, oncology patients with central lines, ventilated neonates and children at risk of air leak, and adolescents on oral contraceptives or with prothrombotic conditions. Technology-dependent children with home ventilation and complex chronic conditions are a high-risk subgroup for both pump failure and obstructive events.[3][11]
Pathophysiology
Cardiac output is the product of stroke volume and heart rate. Stroke volume depends on preload (the filling volume), contractility (the inotropic state of the myocardium), and afterload (the resistance against which the heart pumps). Cardiogenic shock is the failure of contractility or rhythm; obstructive shock is the failure of preload (tamponade, tension pneumothorax) or the overwhelming of afterload (massive pulmonary embolism raising pulmonary vascular resistance against a failing right ventricle). Understanding these three levers is the key to choosing the right drug or procedure.[1][3]
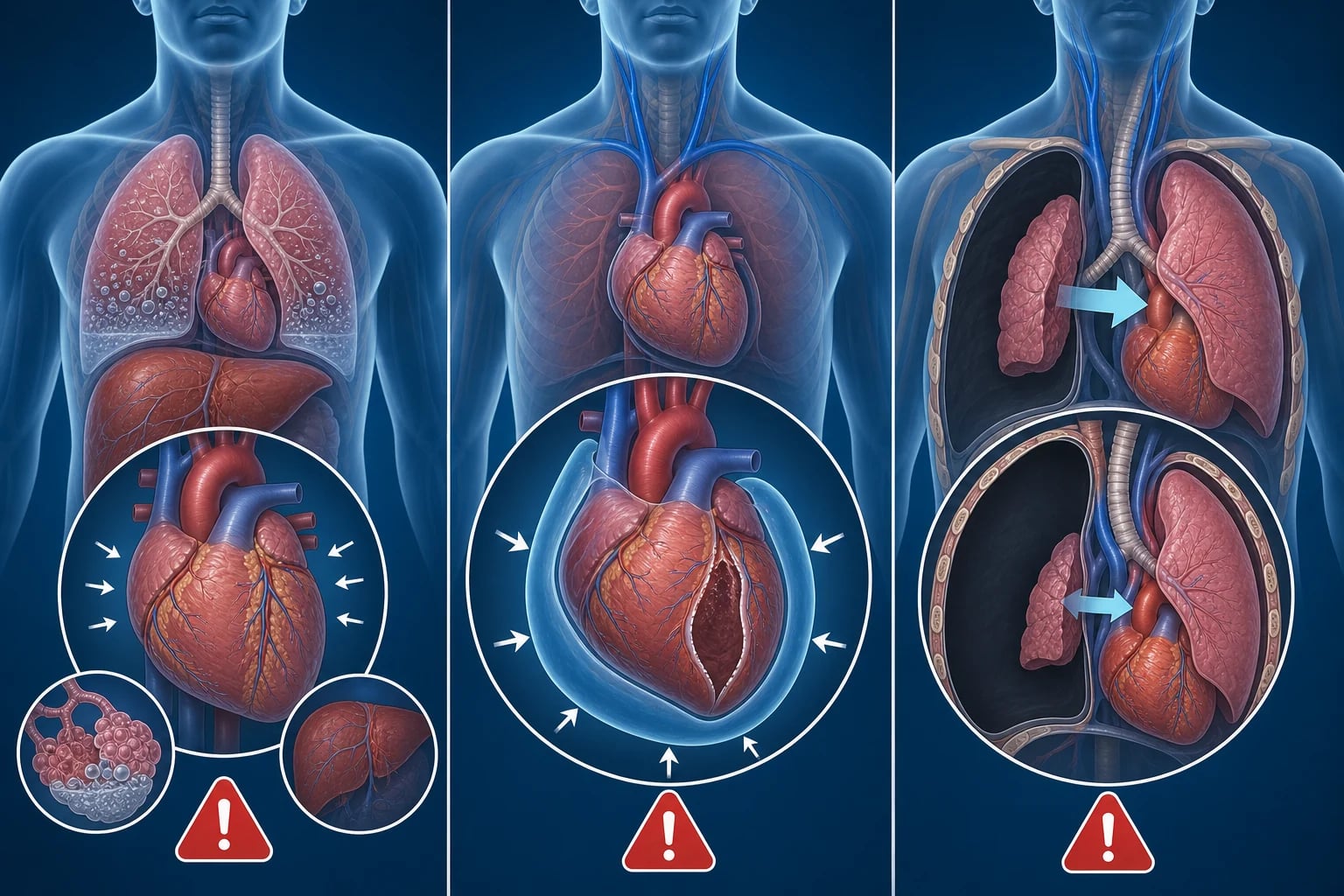
In cardiogenic shock, the myocardium fails. Contractility falls, the stroke volume drops, and the heart compensates with tachycardia. The falling cardiac output triggers sympathetic vasoconstriction, which produces the cold, mottled peripheries and the prolonged capillary refill. The failing ventricle backs up: the right side produces hepatomegaly and raised jugular venous pressure, the left side produces pulmonary oedema and basal crackles. Giving a large fluid bolus to a failing ventricle that cannot pump the extra volume forwards worsens the congestion and can tip the child into pulmonary oedema and collapse — this is the central danger.[1][2]
In cardiac tamponade, fluid or blood in the pericardial space at a pressure exceeding the intracardiac pressure compresses the chambers. The ventricles cannot fill, the stroke volume falls, and the heart rate rises to compensate. The three components of Beck's triad — hypotension, muffled heart sounds, and distended neck veins — describe the consequences: low output, the sound-dampening effect of the fluid, and the backed-up venous return that cannot enter the heart. Pulsus paradoxus (a fall in systolic blood pressure of more than 10 mmHg on inspiration) reflects the exaggerated interventricular dependence, and electrical alternans (alternating QRS amplitude) reflects the heart swinging in the effusion. The treatment is to remove the fluid.[3][9][10]
In tension pneumothorax, air enters the pleural space but cannot escape. The rising intrathoracic pressure collapses the ipsilateral lung, pushes the mediastinum and trachea to the opposite side, compresses the great vessels, and blocks venous return to the heart. The result is the obstructive picture: hypotension from reduced preload, distended neck veins from backed-up venous return, unilateral absent breath sounds, and tracheal deviation away from the affected side. The treatment is to release the air. Positive-pressure ventilation converts a simple pneumothorax to a tension pneumothorax rapidly, which is why ventilated children are at particular risk.[3][6][7]
Clinical Presentation
The child with cardiogenic or obstructive shock looks cold, grey and unwell. The peripheries are mottled and cold to touch, the capillary refill is prolonged beyond 2 seconds, and the pulses are weak and thready. The child is tachycardic (unless the rhythm is the problem), tachypnoeic, and increasingly lethargic. The blood pressure may be normal in compensated shock and falls late. This cold, low-output picture is the shared presentation that the clinician must then dissect to find the mechanism.[1][2]
For cardiogenic shock, the discriminating signs are the gallop rhythm (a third heart sound from a stiff, failing ventricle), hepatomegaly (from right heart back-up), and basal crackles on auscultation (from pulmonary oedema). A child with cardiogenic shock often has a history of a recent viral illness (myocarditis), a known cardiomyopathy, congenital heart disease, recent cardiac surgery, or a drug overdose. The infant with duct-dependent obstructive congenital heart disease presents at days to weeks of life with sudden, profound shock and differential cyanosis or pulses as the duct closes.[1][4]
For cardiac tamponade, the discriminating signs are Beck's triad: hypotension with a narrow pulse pressure, muffled heart sounds, and distended neck veins. Pulsus paradoxus of more than 10 mmHg is a sensitive sign. The child may report breathlessness, orthopnoea, and a dragging chest sensation. There is often a relevant history: recent cardiac surgery, a pericardial effusion on a known oncology patient, trauma, or a febrile illness with chest pain (pericarditis). The chest X-ray shows an enlarged globular cardiac silhouette, but you should not delay decompression to obtain one.[3][9][10]
For tension pneumothorax, the discriminating signs are unilateral absent or reduced breath sounds, tracheal deviation away from the affected side, hyper-resonance to percussion on the affected side, hypotension, and distended neck veins. The child may be ventilated and deteriorating rapidly, or may have a history of chest trauma, asthma, or a recent central line or procedure. The classic signs of tracheal deviation and distended neck veins are late and often absent; unilateral reduced air entry with shock in a ventilated child is enough to decompress.[6][7]
Differential Diagnosis
The differential has two layers. The first layer distinguishes cardiogenic and obstructive shock from the other shock types, because this determines whether fluids help or harm. The second layer distinguishes the specific cause within cardiogenic and obstructive shock, because this determines the definitive treatment.[1][2]
Cardiogenic causes
- Myocarditis: viral illness, chest pain, arrhythmia, raised troponin and BNP, global hypokinesis on echo
- Cardiomyopathy: dilated (most common), hypertrophic, restrictive; family history of sudden death; echocardiography confirms
- Congenital heart disease: duct-dependent lesions (coarctation, hypoplastic left heart, critical aortic stenosis) presenting as shock at days to weeks; differential pulses and SpO2
- Arrhythmia: supraventricular tachycardia above 220 in infants or 180 in children; ventricular tachycardia; complete heart block
- Post-cardiac surgery: low cardiac output syndrome in the first 24 to 48 hours; tamponade and effusion must be excluded
Obstructive causes
- Cardiac tamponade: post-pericardiotomy syndrome, uraemic or bacterial pericarditis, malignant effusion, trauma, post-procedural (catheter); Beck triad, pulsus paradoxus, echo shows effusion with right ventricular diastolic collapse
- Tension pneumothorax: chest trauma, asthma, positive-pressure ventilation, central line insertion; unilateral absent breath sounds, tracheal deviation, shock
- Massive pulmonary embolism: central line, oral contraceptive pill, obesity, immobility, prothrombotic condition, COVID-19; right heart strain on echo, hypoxia, deep vein thrombosis signs
- Duct-dependent obstruction: critical coarctation or aortic stenosis with closed ductus; differential pulses, acidotic shock in neonate
Mimics and mixed pictures
- Sepsis with myocardial dysfunction: a mixed distributive and cardiogenic shock that needs both fluids and inotropes; look for the septic source and the failing echo
- Anaphylaxis: warm shock usually, but can be cold if severe; urticaria, wheeze, hypotension, known allergen
- Severe metabolic acidosis: compensatory tachypnoea and tachycardia mimic shock; the blood gas and lactate reveal the primary process
- Large-volume aspiration or tension from a blocked endotracheal tube: high intrathoracic pressure mimics tension pneumothorax; check the tube first
Clinical & Bedside Assessment
Assessment follows the structured ABCDE approach, but the clinician is asking two specific questions throughout: is this shock, and what type? The answer to the second question determines whether the child gets fluids or inotropes or a needle, and it is answerable at the bedside within minutes if the examination is systematic.[1][2]
The hands and peripheries tell the first story. Cold, mottled skin with capillary refill over 2 seconds and weak, thready pulses indicates a cold, low-output state. Compare central and peripheral pulses: a bounding radial with a weak femoral suggests coarctation. The neck reveals distended jugular veins in tamponade and tension pneumothorax, and flat veins in hypovolaemia. The chest examination is the hinge: bilateral crackles and a gallop point to cardiogenic shock; muffled heart sounds point to tamponade; unilateral absent breath sounds with hyper-resonance point to tension pneumothorax.[2][10]
Point-of-care ultrasound has transformed the bedside assessment of cardiogenic and obstructive shock. A focused cardiac ultrasound identifies a pericardial effusion with right ventricular diastolic collapse (tamponade), a dilated hypocontractile left ventricle (cardiogenic shock), or a dilated right ventricle with septal bowing (massive pulmonary embolism). A lung ultrasound identifies the absent lung sliding and lung point of a pneumothorax. In the hands of a trained operator, bedside ultrasound confirms the diagnosis within minutes and should be available in any emergency department or PICU managing a shocked child.[10]
Investigations
Investigations in the shocked child are parallel and point-of-care first. Do not delay treatment to complete a panel. The minimum dataset in the first minutes is a venous or capillary blood gas (for pH, lactate, glucose and electrolytes), a blood glucose (hypoglycaemia is common and harmful in the shocked neonate and infant), a full blood count, urea and electrolytes, CRP, and blood cultures if sepsis is possible. A 12-lead ECG is essential to exclude arrhythmia and to look for the low-voltage QRS of a large effusion or the electrical alternans of tamponade.[1][2]
For cardiogenic shock, the key investigations are a cardiac troponin and BNP or NT-proBNP (elevated in myocarditis and heart failure), an echocardiogram (the definitive test: assesses contractility, structure, valve function, effusion and tamponade physiology), and a chest X-ray (cardiomegaly, pulmonary oedema, or the globular heart of tamponade). Myocarditis may need cardiac MRI for tissue characterisation, and coronary angiography if Kawasaki disease or anomalous coronary origin is suspected.[4]
For cardiac tamponade, the echocardiogram is definitive and should be performed urgently. It confirms the pericardial effusion and shows the tamponade physiology: right atrial collapse in late diastole, right ventricular free wall collapse in early diastole, a plethoric inferior vena cava, and exaggerated respiratory variation in mitral and tricuspid inflow. The echo also guides pericardiocentesis. A chest X-ray showing an enlarged globular heart supports the diagnosis but is not required before decompression in the crashing child.[9][10]
For tension pneumothorax, the diagnosis is clinical in the unstable child — imaging must not delay decompression. A chest X-ray, once the child is stabilised, confirms the pneumothorax and the mediastinal shift. Point-of-care lung ultrasound showing absent lung sliding and a lung point can confirm the diagnosis at the bedside in the stable or borderline child. The Ahmad 2025 meta-analysis confirms that the traditional second intercostal space mid-clavicular line decompression site often fails in adults because standard cannulae are too short, and the fourth or fifth intercostal space in the anterior axillary line is increasingly recommended as the primary site; finger thoracostomy is the definitive emergency decompression in the ventilated child.[6][7]
For massive pulmonary embolism, a D-dimer is useful only if negative in a low-risk child. The definitive imaging is a CT pulmonary angiogram in the stable adolescent, or a bedside echocardiogram showing right ventricular dilatation and septal bowing in the unstable child who cannot travel to CT. The electrocardiogram may show the S1Q3T3 pattern or right bundle branch block. Deep vein thrombosis should be sought with compression ultrasound of the lower limbs.[11][12]
CARDIOGENIC
Management — Resuscitation
The first principle of managing cardiogenic and obstructive shock is not to treat them like septic or hypovolaemic shock. Large, repeated 20 mL per kg fluid boluses that rescue the septic child can kill the child with a failing or obstructed heart. The second principle is that the definitive treatment differs by mechanism: cardiogenic shock needs inotropes and sometimes mechanical support; tamponade needs pericardiocentesis; tension pneumothorax needs thoracostomy; pulmonary embolism needs thrombolysis. The resuscitation is the bridge to the definitive treatment.[1][2]
Airway and breathing come first. Give high-flow oxygen to every shocked child. The child with cardiogenic pulmonary oedema may need non-invasive ventilation (CPAP or BiPAP) to reduce the work of breathing and improve oxygenation, or intubation and positive-pressure ventilation if tiring. Positive-pressure ventilation reduces afterload on the failing left ventricle, which can dramatically improve cardiac output — but the transition to positive pressure can also drop venous return and blood pressure, so be ready with volume and vasoactives. Avoid excessive positive pressure in suspected tension pneumothorax until the chest is decompressed.[1][2]
Fluid resuscitation in cardiogenic and obstructive shock must be cautious. Give 5 to 10 mL per kg boluses of isotonic crystalloid over 5 to 10 minutes, with reassessment after each bolus for signs of improvement (heart rate, capillary refill, blood pressure, liver size, work of breathing, oxygenation). Stop the fluids if the child develops crackles, rising hepatomegaly, a falling oxygen saturation, or no improvement — these are signs that the heart cannot handle the volume. In tamponade and tension pneumothorax, fluids are only a temporary bridge to decompression; the definitive treatment is the physical release.[1][2]
Vasoactive support should be started early in cardiogenic shock, after the first cautious fluid bolus, and not delayed until the child is in extremis. The choice of inotrope follows the physiology. Adrenaline at 0.05 to 0.5 micrograms per kg per minute is the first-line inotrope for the cold, low-output child because it increases contractility and peripheral vascular tone. Noradrenaline at 0.05 to 1 microgram per kg per minute is added for vasodilatory shock with low systemic vascular resistance. Dobutamine at 5 to 20 micrograms per kg per minute is an alternative inotrope for milder cardiogenic shock, but it can cause tachycardia and vasodilation. Milrinone at 0.25 to 0.75 micrograms per kg per minute (after a loading dose of 50 micrograms per kg) is a lusitrope that improves diastolic relaxation and reduces afterload, useful in post-cardiac surgical low cardiac output syndrome.[1][2]
Adrenaline (epinephrine) infusion
Dose
0.05 to 0.5 micrograms per kg per minute (titrate upward; may need up to 2 micrograms per kg per minute in refractory shock)
Arrhythmia causing cardiogenic shock needs rhythm control. For supraventricular tachycardia with shock, perform synchronized cardioversion at 0.5 to 1 J per kg, escalating to 2 J per kg if needed, after sedation if time permits; try vagal manoeuvres or intravenous adenosine 100 to 200 micrograms per kg (maximum 500 micrograms first dose, then 300 micrograms per kg if needed) if the child is stable. For ventricular tachycardia with shock, perform synchronized cardioversion at 0.5 to 1 J per kg; if pulseless, defibrillate at 2 to 4 J per kg. Correct potassium, magnesium and calcium. For the neonate or infant with suspected duct-dependent congenital heart disease, start an intravenous prostaglandin E1 (alprostadil) infusion at 0.01 to 0.05 micrograms per kg per minute to reopen or maintain the ductus arteriosus while definitive repair is arranged.[2][4]
Tension pneumothorax is decompressed immediately — it is a clinical diagnosis and imaging must not delay treatment. Needle thoracostomy with a large-bore cannula is the traditional first step: insert at the second intercostal space in the mid-clavicular line on the affected side, just above the third rib to avoid the neurovascular bundle. However, the Ahmad 2025 meta-analysis found that standard adult cannulae are often too short for the second intercostal space mid-clavicular line site, and recommends the fourth or fifth intercostal space in the anterior axillary line as a more reliable site. In the ventilated child, a finger thoracostomy at the fourth or fifth intercostal space in the anterior axillary line is the definitive emergency decompression and is preferred over needle thoracostomy in many trauma systems, because it provides immediate, reliable drainage and allows a formal chest drain to be inserted. The definitive management is an intercostal chest drain connected to an underwater seal.[6][7]
Cardiac tamponade is treated with emergency pericardiocentesis. In the crashing child, this is performed emergently at the bedside, ideally with echocardiographic guidance to identify the largest pocket of fluid and to avoid the myocardium. Insert the needle at the subxiphoid approach, directing the needle toward the left shoulder at a 30-degree angle to the skin, aspirating continuously. Once pericardial fluid is aspirated and the blood pressure improves, advance a guidewire, remove the needle, and place a drain. A surgical pericardial window is the definitive treatment for recurrent or loculated effusions, particularly post-pericardiotomy syndrome, where surgical drainage has better outcomes than percutaneous pericardiocentesis in some series.[8][9][10]
Management — Definitive & Stepwise
Once the immediate resuscitation has stabilised the child, the definitive treatment targets the specific cause. This is the phase where the diagnosis is confirmed, the precipitant is treated, and the child is transferred to definitive care in a PICU or cardiac centre. The goal is to restore a sustained, adequate cardiac output and to prevent re-collapse.[1][2]
Cardiogenic shock definitive
- Myocarditis: intravenous immunoglobulin is sometimes used; avoid digoxin; treat heart failure with diuretics, ACE inhibitors and beta-blockers once stable; ECMO or ventricular assist device for refractory cases
- Cardiomyopathy: heart failure therapy; evaluation for transplant if end-stage; mechanical support as a bridge
- Duct-dependent congenital heart disease: prostaglandin E1 infusion to maintain the ductus; transfer to a cardiac centre for definitive surgical or catheter repair
- Arrhythmia: definitively terminate with cardioversion, adenosine, or antiarrhythmics; identify the substrate and arrange electrophysiology
- Post-cardiac surgery: low cardiac output syndrome managed with tailored inotropes, milrinone, delayed sternal closure and ECMO if refractory
Obstructive shock definitive
- Cardiac tamponade: pericardiocentesis or surgical pericardial window; treat the underlying cause (antibiotics for bacterial pericarditis, steroids and colchicine for post-pericardiotomy syndrome, chemotherapy for malignant effusion)
- Tension pneumothorax: intercostal chest drain after emergency decompression; address the cause (trauma repair, asthma optimisation, ventilator adjustment, line removal)
- Massive pulmonary embolism: systemic thrombolysis with tissue plasminogen activator, or catheter-directed thrombolysis or surgical embolectomy; anticoagulation and IVC filter if recurrent
Mechanical circulatory support
- Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) for refractory cardiogenic shock: provides both cardiac and respiratory support; the SAVE score predicts survival and guides candidacy
- Ventricular assist device as a bridge to transplant in selected children with end-stage cardiomyopathy
- Indications: refractory cardiogenic shock despite maximal inotrope support, potentially reversible cause, no contraindication to anticoagulation
- Outcomes depend on the underlying diagnosis, duration of arrest or shock before cannulation, and the centre's expertise
Duct-dependent congenital heart disease — the neonatal trap
The neonate who presents with shock in the first days to weeks of life must be assumed to have duct-dependent congenital heart disease until proven otherwise. Lesions such as hypoplastic left heart syndrome, critical coarctation of the aorta, critical aortic stenosis, and interrupted aortic arch rely on the ductus arteriosus to supply the systemic circulation; when it closes, the child collapses with profound acidotic shock, differential pulses, and differential cyanosis. The treatment is immediate intravenous prostaglandin E1 (alprostadil) at 0.01 to 0.05 micrograms per kg per minute to reopen the ductus, with transfer to a cardiac centre for definitive surgical or catheter-based repair. The classic clues are absent or weak femoral pulses, a differential in pre- and post-ductal oxygen saturation, a chest X-ray with a boot-shaped or cardiomegalic heart, and profound metabolic acidosis. Starting prostaglandins is the single most important act — it is safe and the downside of not starting them in a duct-dependent child is death.[1][4]
Mechanical circulatory support and the SAVE score
For refractory cardiogenic shock that does not respond to inotropes, veno-arterial extracorporeal membrane oxygenation (VA-ECMO) provides temporary cardiopulmonary support while the heart recovers or a bridge to transplant is arranged. The SAVE score (Schmidt 2015), developed in adults but applied to older children, predicts survival after VA-ECMO for refractory cardiogenic shock using pre-cannulation variables including the underlying diagnosis, pre-ECMO cardiac arrest, age, weight, renal function, and the mode of ECMO. It is a tool to guide the decision and the conversation with the family, not an absolute rule. The key principle is that ECMO is most effective when the cause is potentially reversible and cannulated before irreversible end-organ damage sets in.[5]
Fields 2023 — pericardial window versus pericardiocentesis in post-pericardiotomy syndrome
Retrospective comparison of surgical pericardial window and catheter pericardiocentesis in children with post-pericardiotomy syndrome
Population: Children who developed post-pericardiotomy syndrome after cardiac surgery
Key finding
The study compared outcomes including reaccumulation, need for repeat intervention and length of stay, informing the choice between surgical and percutaneous drainage
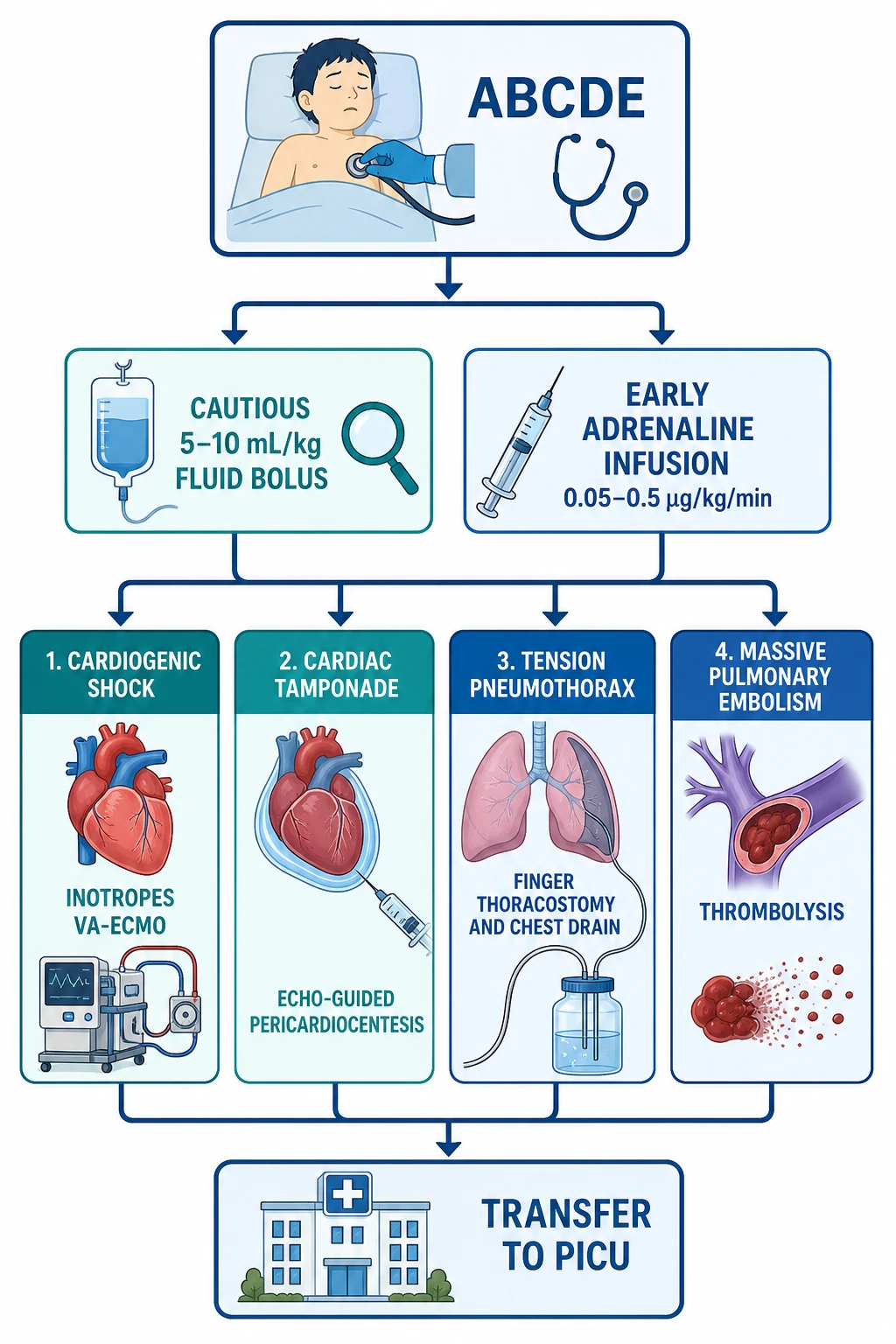
Recognise the cold, low-output state: weak pulses, capillary refill over 2 seconds, mottled skin, altered consciousness.
Give high-flow oxygen; assess airway and breathing; consider non-invasive or invasive ventilation for pulmonary oedema or exhaustion.
Give a cautious 5 to 10 mL per kg isotonic crystalloid bolus with reassessment; stop if no improvement or if congestion worsens.
Start an adrenaline infusion at 0.05 to 0.5 micrograms per kg per minute for cold cardiogenic shock; add noradrenaline for vasodilatory shock.
Exclude arrhythmia on the 12-lead ECG; cardiovert SVT or VT with shock at 0.5 to 1 J per kg.
For suspected tamponade, call for urgent echo and prepare echo-guided pericardiocentesis; decompress if Beck triad or shock.
For suspected tension pneumothorax, decompress immediately with needle or finger thoracostomy; insert a chest drain.
For massive pulmonary embolism, start systemic thrombolysis or arrange catheter-directed thrombolysis.
Transfer to PICU or a cardiac centre; arrange VA-ECMO for refractory cardiogenic shock.
Specific Subtypes & Scenarios
The neonate with duct-dependent shock. An infant presenting at days to weeks of life with profound shock, metabolic acidosis, and weak or absent femoral pulses has duct-dependent obstructive congenital heart disease until proven otherwise. Start prostaglandin E1 at 0.01 to 0.05 micrograms per kg per minute immediately, before the echo confirms the lesion, because the downside of withholding it is death. Monitor for apnoea, hypotension and fever, which are common prostaglandin side effects, and have intubation equipment ready.[1][4]
Post-cardiac surgical low cardiac output syndrome. Children in the first 24 to 48 hours after cardiac surgery for complex congenital heart disease are at high risk of a low cardiac output state from myocardial stunning, residual lesions, arrhythmia, and tamponade. Management is tailored inotrope support with milrinone for lusitropy and afterload reduction, adrenaline or noradrenaline for blood pressure, and delayed sternal closure. Tamponade must be excluded urgently in any post-surgical child with unexplained tachycardia, hypotension and rising lactate, and may present atypically because the pericardium is open or surgically modified.[4][8]
Myocarditis presenting as cardiogenic shock. A child with a recent viral illness, chest pain, arrhythmia and progressive shock has myocarditis until proven otherwise. The echocardiogram shows global or regional hypokinesis, often with a normal or dilated left ventricle. Troponin and BNP are elevated. Management is supportive: treat heart failure, control arrhythmia, avoid digoxin, and escalate to VA-ECMO for refractory shock. The American Heart Association scientific statement on myocarditis in children guides the diagnostic and therapeutic pathway.[4]
The ventilated child with sudden deterioration. A ventilated child who suddenly desaturates, becomes hypotensive and develops unequal breath sounds has a tension pneumothorax until proven otherwise. The positive-pressure ventilation converts a simple pneumothorax to a tension pneumothorax within minutes. Do not wait for imaging; decompress immediately. Check the endotracheal tube is not blocked or displaced first, then perform a finger thoracostomy at the fourth or fifth intercostal space in the anterior axillary line, followed by a chest drain. The anterior axillary site is preferred in the ventilated patient because it is more reliable than the second intercostal space mid-clavicular line.[6][7]
The oncology patient with tamponade. A child with cancer and a pericardial effusion can develop tamponade from malignant involvement, from bleeding after a procedure, or as a complication of treatment. These children are often thrombocytopenic, which increases the risk of pericardiocentesis. Echo-guided pericardiocentesis is the emergency treatment, and a surgical window may be needed for recurrent or loculated effusions. The underlying malignancy drives the long-term prognosis.[9][10]
The adolescent with massive pulmonary embolism. An adolescent with risk factors (oral contraceptive pill, obesity, immobility, central line, prothrombotic condition, recent COVID-19) presenting with sudden dyspnoea, pleuritic chest pain, hypoxia and shock has a massive pulmonary embolism until proven otherwise. The bedside echo shows right ventricular dilatation and septal bowing. Treatment is systemic thrombolysis with tissue plasminogen activator, or catheter-directed thrombolysis if a interventional radiology service is available. Anticoagulation is started once the bleeding risk allows. A systematic review of paediatric pulmonary embolism confirms that massive PE is rare but increasingly recognised in adolescents.[11][12]
Complications & Pitfalls
The dominant complication of both cardiogenic and obstructive shock is end-organ damage from sustained low perfusion: acute kidney injury, hepatic dysfunction, ischaemic gut injury, and neurological injury from hypoxic-ischaemic encephalopathy. Cardiogenic shock can progress to cardiopulmonary arrest if untreated, and obstructive shock can progress to pulseless electrical activity arrest within minutes. The treatments themselves carry risks: inotropes cause tachyarrhythmia and hypertension; pericardiocentesis risks myocardial puncture, coronary laceration and pneumothorax; needle thoracostomy risks vascular injury and failure to decompress; thrombolysis risks catastrophic bleeding.[1][2]
Pitfalls are the recurring, preventable errors. Treating cardiogenic or obstructive shock like septic shock with large 20 mL per kg fluid boluses is the commonest and most dangerous error, worsening congestion and compression. Waiting for imaging to diagnose tension pneumothorax or tamponade in the unstable child costs minutes that the circulation does not have. Using a too-short cannula for needle thoracostomy, particularly at the second intercostal space mid-clavicular line, fails to decompress and gives false reassurance — the Ahmad 2025 meta-analysis confirms this is a common failure in adults and applies to larger children and adolescents. Failing to start an inotrope early in cardiogenic shock, waiting instead for the child to collapse, is a preventable error. Missing duct-dependent congenital heart disease in the neonate with shock, by attributing the picture to sepsis alone and omitting prostaglandins, is a lethal trap.[1][6]
After stabilisation, the pitfalls are failing to seek and treat the underlying cause, delaying transfer to definitive care, and underestimating the risk of re-collapse before the definitive intervention is completed.[2]
Prognosis & Disposition
Outcomes depend on the underlying cause, the speed of recognition, and the timeliness of definitive treatment. Children with reversible causes recognised early — a tension pneumothorax decompressed within minutes, a tamponade drained promptly, a supraventricular tachycardia cardioverted — generally do well. Children with myocarditis have a variable prognosis: fulminant myocarditis can recover completely with supportive care, while chronic myocarditis can progress to dilated cardiomyopathy and need transplant. Post-cardiac surgical shock carries a mortality proportional to the complexity of the surgery and the presence of residual lesions. Refractory cardiogenic shock requiring VA-ECMO carries a substantial mortality; the SAVE score helps stratify the risk.[1][4][5]
Disposition is to a PICU or a paediatric cardiac centre, with continuous arterial and central venous pressure monitoring, serial echocardiography, and early involvement of paediatric cardiology, intensive care and, where relevant, cardiothoracic surgery. Retrieval services should be involved early for children in rural and remote settings, because the definitive treatment for cardiogenic and obstructive shock is often available only at a tertiary centre.[1][2]
Special Populations
The neonate and young infant with cardiogenic or obstructive shock most often has duct-dependent congenital heart disease, myocarditis, or a complication of a central line or congenital diaphragmatic hernia. Prostaglandins must be started empirically when a duct-dependent lesion is suspected. The neonatal myocardium is less compliant than the older child's, making it more sensitive to volume overload; fluids must be given in small aliquots.[1][4]
Children with complex congenital heart disease and post-surgical patients are the highest-risk subgroup for both cardiogenic shock (low cardiac output syndrome, arrhythmia, residual lesions) and tamponade. They need rapid access to echocardiography, cardiology and ECMO. Technology-dependent children with tracheostomies, home ventilation and complex chronic conditions can obstruct or fail from airway, ventilator or line problems and need caregivers trained to recognise deterioration.[3][8]
Immunocompromised and oncology children may develop tamponade from malignant or infectious pericardial effusions, are thrombocytopenic at presentation, and carry worse outcomes. Adolescents are the group at risk of massive pulmonary embolism (from oral contraceptives, obesity, prothrombotic conditions), drug-induced cardiomyopathy, and post-viral myocarditis.[9][11]
Indigenous, rural and remote, and socioeconomically disadvantaged children present later, have less access to echocardiography, cardiology and ECMO, and carry worse outcomes from the same insult. Retrieval systems, early recognition, and equitable access to tertiary cardiac care are the corrective priorities.[1]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric cardiogenic and obstructive shock combines guideline consensus, observational registry data, and a growing body of paediatric-specific studies. The American Heart Association 2021 scientific statement on myocarditis in children guides the diagnostic and management pathway for the commonest cause of paediatric cardiogenic shock. The SAVE score (Schmidt 2015), though developed in adults, is widely used to stratify survival after VA-ECMO in older children with refractory cardiogenic shock. The Ahmad 2025 meta-analysis reshaped the approach to tension pneumothorax decompression by confirming that the traditional second intercostal space mid-clavicular line site often fails because standard cannulae are too short, and recommends the fourth or fifth intercostal space in the anterior axillary line. Observational studies of paediatric pulmonary embolism (Alsabri 2025) and catheter-directed thrombolysis (Ji 2020) inform the management of massive PE.[4][5][6][11]
Australian and New Zealand practice follows the ANZCOR guidelines for paediatric advanced life support, the Royal Children's Hospital Melbourne clinical practice guideline on shock, and the Advanced Trauma Life Support approach to tension pneumothorax in trauma. Adrenaline infusion for cardiogenic shock is 0.05 to 0.5 micrograms per kg per minute; fluid boluses in cardiogenic shock are 5 to 10 mL per kg with reassessment. For tension pneumothorax, finger thoracostomy at the fourth or fifth intercostal space in the anterior axillary line is increasingly the preferred emergency decompression in ventilated children and in trauma, with a chest drain following. Echo-guided pericardiocentesis is performed by the intensivist or cardiologist. Retrieval to a tertiary paediatric cardiac centre is organised early for rural and remote children.[1][6]
In low- and middle-income settings, cardiogenic and obstructive shock carry a higher mortality because of later presentation, limited access to echocardiography, cardiology, intensive care and ECMO. The highest-leverage interventions are early recognition of the cold, low-output state, cautious fluid boluses, early adrenaline, and the prompt physical reversal of tamponade and tension pneumothorax. Prostaglandins for suspected duct-dependent lesions, needle decompression for tension pneumothorax, and pericardiocentesis for tamponade are achievable in resource-limited settings and save lives. Prevention of rheumatic heart disease and timely treatment of sepsis reduce the burden of paediatric cardiogenic shock.[1]
Controversies include the optimal inotrope strategy and the role of milrinone versus adrenaline in post-surgical low cardiac output syndrome, the threshold and timing for VA-ECMO in refractory cardiogenic shock, the role of catheter-directed versus systemic thrombolysis in paediatric PE, and the ideal site and technique for tension pneumothorax decompression in children of different ages and sizes. The convergence of trauma guidelines toward the anterior axillary line and finger thoracostomy is the clearest recent shift.[6][7]
Exam Pearls
OBSTRUCTIVE
- Cardiogenic and obstructive shock present as cold, low-output states — weak pulses, capillary refill over 2 seconds, mottled skin — distinct from the warm shock of early sepsis.[1]
- Fluids must be cautious: 5 to 10 mL per kg with reassessment, never the large 20 mL per kg boluses of septic shock, because the failing or obstructed heart cannot handle the volume.[1][2]
- Adrenaline 0.05 to 0.5 micrograms per kg per minute is the first-line inotrope for cold cardiogenic shock; start early after the first cautious bolus.[1]
- Tension pneumothorax is a clinical diagnosis — do not wait for imaging; decompress with needle or finger thoracostomy, and the anterior axillary line at the fourth or fifth intercostal space is preferred.[6][7]
- Cardiac tamponade presents with Beck triad — hypotension, muffled heart sounds, distended neck veins — and is treated with echo-guided pericardiocentesis.[3][10]
- The neonate with shock at days to weeks of life has duct-dependent congenital heart disease until proven otherwise — start prostaglandin E1 at 0.01 to 0.05 micrograms per kg per minute immediately.[1][4]
- SVT above 220 in infants or 180 in children with shock needs synchronized cardioversion at 0.5 to 1 J per kg.[2]
Quick check: a 3-year-old presents with fever, tachycardia at 190 per minute, cold peripheries, capillary refill of 4 seconds, weak pulses, hepatomegaly and bilateral basal crackles. Blood pressure is 78 over 45 mmHg. What type of shock is this and what is your first fluid and drug step?
This is cardiogenic shock: the cold peripheries, weak pulses, prolonged capillary refill, hepatomegaly and bilateral basal crackles point to pump failure, not hypovolaemia. Give a cautious 5 mL per kg bolus of isotonic crystalloid over 10 minutes with reassessment — do not give 20 mL per kg blindly. Start an adrenaline infusion at 0.05 to 0.5 micrograms per kg per minute after the first bolus, give high-flow oxygen, arrange an urgent echocardiogram and 12-lead ECG, and call the PICU and cardiology early. Consider non-invasive ventilation for the pulmonary oedema. The differential includes myocarditis (send troponin and BNP) and sepsis-induced myocardial dysfunction (a mixed picture).[1][2]
References
- [1]Bjorklund A, Resch J, Slusher T Pediatric Shock Review. Pediatr Rev, 2023.PMID 37777656
- [2]Mendelson J Emergency Department Management of Pediatric Shock. Emerg Med Clin North Am, 2018.PMID 29622332
- [3]Morgan WM 3rd, O'Neill JA Jr Hemorrhagic and obstructive shock in pediatric patients. New Horiz, 1998.PMID 9654322
- [4]Law YM, Lal AK, Chen S, et al. Diagnosis and Management of Myocarditis in Children: A Scientific Statement From the American Heart Association. Circulation, 2021.PMID 34229446
- [5]Schmidt M, Burrell A, Roberts L, et al. Predicting survival after ECMO for refractory cardiogenic shock: the survival after veno-arterial-ECMO (SAVE)-score. Eur Heart J, 2015.PMID 26033984
- [6]Ahmad SJS, Degiannis JR, Head M, et al. Meta-analysis of the optimal needle length and decompression site for tension pneumothorax and consensus recommendations on current ATLS and ETC guidelines. World J Emerg Surg, 2025.PMID 40383767
- [7]Harris M, Rocker J Pneumothorax In Pediatric Patients: Management Strategies To Improve Patient Outcomes. Pediatr Emerg Med Pract, 2017.PMID 28252382
- [8]Fields JT, O'Halloran CP, Tannous P, et al. Differences in outcomes between surgical pericardial window and pericardiocentesis in children with postpericardiotomy syndrome. Ann Pediatr Cardiol, 2023.PMID 38817257
- [9]Donovan M, Smith N, Holton R, et al. Pediatric Bacterial Pericarditis. Am J Emerg Med, 2020.PMID 31859192
- [10]Alerhand S, Choi A, Varga P Cardiac Ultrasound for Pediatric Emergencies. Pediatr Ann, 2021.PMID 34617847
- [11]Alsabri M, Abo-Elnour DE, Ayyad M, et al. Epidemiology and management of massive, sub-massive, and non-massive pediatric pulmonary embolism: a systematic review. BMC Pediatr, 2025.PMID 40287637
- [12]Ji D, Gill AE, Durrence WW, et al. Catheter-Directed Pharmacologic Thrombolysis for Acute Submassive and Massive Pulmonary Emboli in Children and Adolescents-An Exploratory Report. Pediatr Crit Care Med, 2020.PMID 31688811