Paeds · acute-care-resuscitation-and-toxicology
Cardiorespiratory arrest and post-arrest care
Also known as Paediatric cardiac arrest · Cardiopulmonary arrest · Return of spontaneous circulation · Post-arrest syndrome · Post-cardiac arrest syndrome · Targeted temperature management in children
Fellowship guide to paediatric cardiorespiratory arrest and post-arrest care: recognising the deteriorating child and the arrest, the high-quality CPR and defibrillation pathway to return of spontaneous circulation, and the post-arrest bundle of targeted temperature management, normoxia and normocarbia, haemodynamic and glucose control, seizure detection and delayed multimodal prognostication, with the ANZ, AHA and European guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Cardiorespiratory arrest in a child is the sudden loss of a palpable pulse and effective breathing, and it is the end-point of a failing respiratory or circulatory system far more often than a primary cardiac event. Most paediatric arrests are asphyxial or hypoxic, driven by respiratory failure or shock, in contrast to the arrhythmic, ventricular-fibrillation-dominated arrests of adults.[2][4]
The goal of resuscitation is return of spontaneous circulation (ROSC), defined as the restoration of a palpable pulse and a perfusing rhythm without ongoing chest compressions. ROSC is not the finish line. It launches the post-cardiac arrest syndrome, a predictable, multi-system combination of post-arrest brain injury, myocardial dysfunction, systemic ischaemia-reperfusion injury, and the persistence of the precipitating pathology.[1]
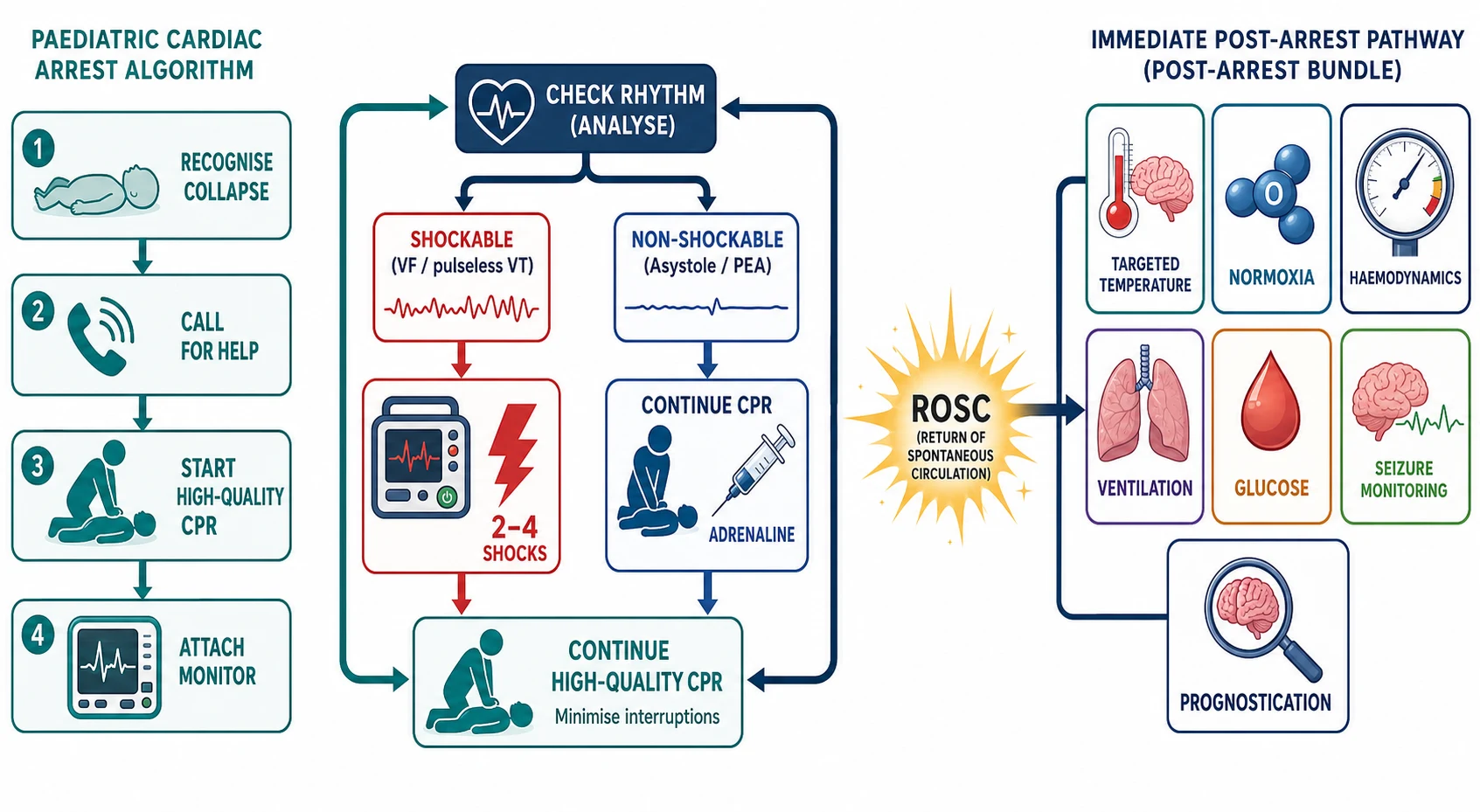
The clinician's task therefore has two halves that this page addresses in sequence. The first half is achieving ROSC: recognising the arrest within seconds, delivering high-quality cardiopulmonary resuscitation, ventilating with oxygen, giving adrenaline, and defibrillating shockable rhythms. The second half, and the half that most determines who survives neurologically intact, is the post-arrest care bundle: targeted temperature management, oxygenation and ventilation targets, haemodynamic support, glucose control, seizure detection, and honest, delayed prognostication.[1][3]
Classification
Paediatric arrest is best classified along two axes that govern the entire resuscitation and that examiners probe in parallel: the initial rhythm, which dictates whether you defibrillate, and the arrest location and mechanism, which sets prognosis and the differential. The rhythm check after each two-minute cycle of compressions sorts the child into a shockable or non-shockable group, and this single decision is the hinge of advanced life support.[2][3]
Shockable rhythms
- Ventricular fibrillation (VF) and pulseless ventricular tachycardia (pVT)
- Far less common in children than adults, but more common in adolescent sudden cardiac arrest, cardiomyopathy, channelopathies and drug toxicity
- Immediate defibrillation: first shock 2 to 4 J per kg, subsequent shocks at least 4 J per kg up to a maximum of 10 J per kg
- Adrenaline 10 micrograms per kg IV or IO every 3 to 5 minutes after the second shock, with amiodarone 5 mg per kg for refractory VF or pVT
Non-shockable rhythms
- Asystole and pulseless electrical activity (PEA): the majority of paediatric arrests, usually the end-stage of respiratory failure or shock
- Continue high-quality CPR and treat reversible causes (the 4 Hs and 4 Hs)
- Adrenaline 10 micrograms per kg IV or IO as soon as IV or IO access is achieved, every 3 to 5 minutes
- Identify and reverse the precipitant — airway obstruction, hypoxia, hypovolaemia, tension pneumothorax, tamponade, toxins, thrombosis, hypoglycaemia, hypothermia
Location and mechanism
- Out-of-hospital cardiac arrest (OHCA): lower survival to discharge (around 8 to 12 percent), predominantly asphyxial or sudden cardiac death
- In-hospital cardiac arrest (IHCA): higher survival to discharge (around 35 to 45 percent), often witnessed and monitored, frequently respiratory or perioperative
- Asphyxial arrest from respiratory failure or shock versus arrhythmic sudden cardiac arrest: the former dominates in infants and young children, the latter rises in adolescents
Severity
Arrest phase
Epidemiology & Risk Factors
Cardiac arrest is rare in children compared with adults, which is exactly why recognition often comes late. In-hospital cardiac arrest occurs in roughly 8 to 12 per 1000 paediatric hospital admissions in large registries, while out-of-hospital arrest affects about 8 to 20 per 100,000 children per year. Survival has improved over two decades of focus on high-quality CPR, but outcomes remain starkly divided by location and rhythm.[1][2]
The single most important prognostic fact is that most paediatric arrests are respiratory or asphyxial in origin. Infants arrest from sudden infant death, bronchiolitis, sepsis and congenital heart disease; older children arrest from respiratory failure, sepsis, drowning, trauma and, increasingly in adolescents, sudden cardiac death. Only about 5 to 15 percent of paediatric arrests present in a shockable rhythm, which is why airway, breathing and adrenaline dominate the early algorithm.[2][4]
The children at highest risk are those with reduced physiologic reserve or an identifiable precipitant. Premature infants, children with chronic lung disease or complex congenital heart disease, neuromuscular disorders that impair breathing, immunocompromised children, and technology-dependent children with tracheostomies or home ventilation all carry elevated risk. Socioeconomic disadvantage, rural and remote location, and indigenous heritage are associated with later presentation and worse outcomes from the same insult, which is why retrieval systems and early recognition matter most where reserve is least.[1]
Pathophysiology
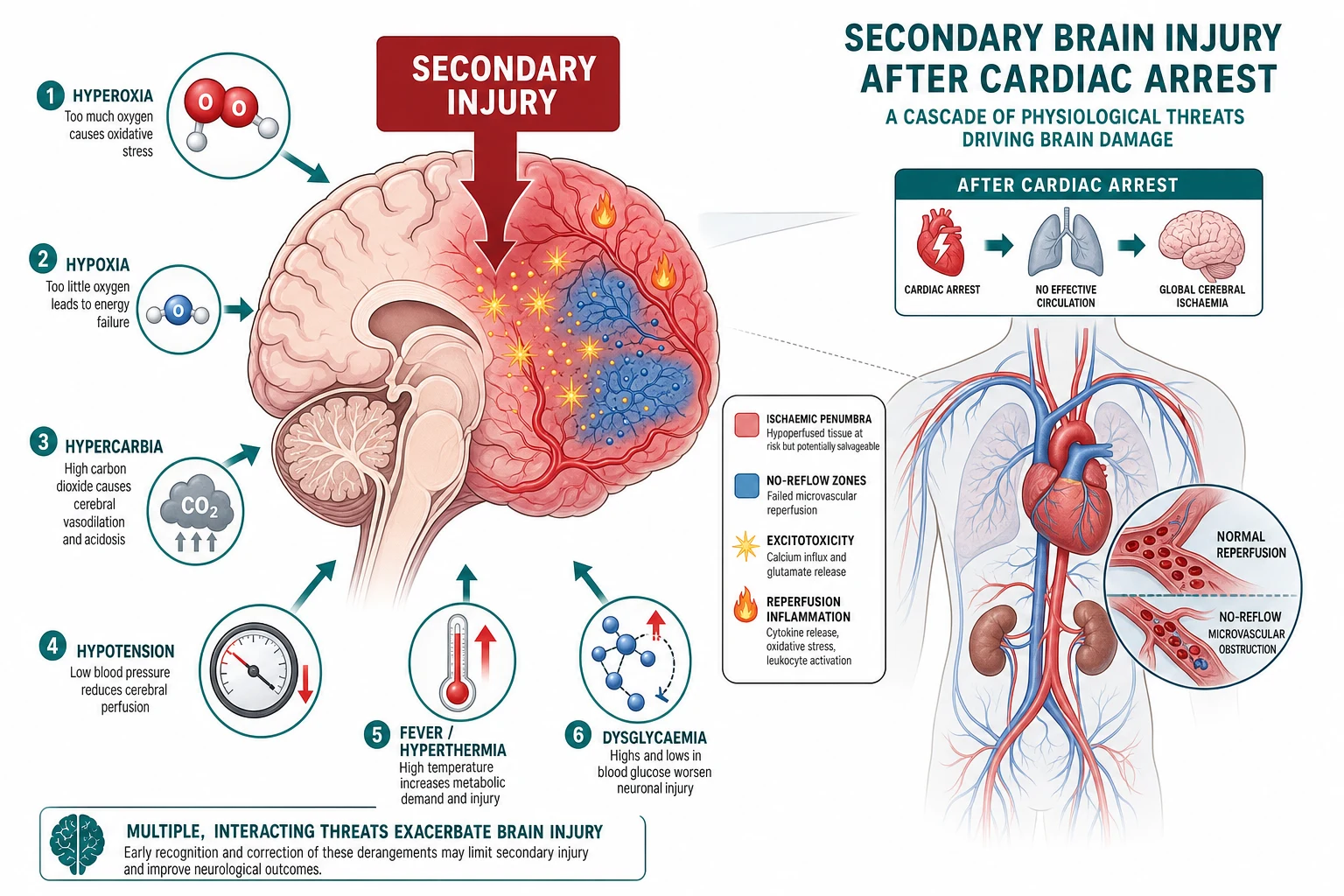
Because most paediatric arrests are asphyxial, the tissue dies in a characteristic three-phase sequence: progressive hypoxaemia and hypercarbia drive bradycardia and a fall in cardiac output; the bradycardia deepens into agonal rhythms and then asystole or PEA; and the loss of perfusion produces global ischaemia. The arrest is the visible end of a respiratory or circulatory failure that has often been unfolding for many minutes, which is why effective ventilation with oxygen is the single most important intervention in the first minutes.[2][4]
When ROSC returns perfusion, the damage is not over. Reperfusion reignites injury through a cascade of mitochondrial dysfunction, calcium overload, glutamate-mediated excitotoxicity, free-radical generation, neuroinflammation and microvascular "no-reflow". This secondary brain injury is the dominant determinant of who wakes up intact, and it is exquisitely sensitive to the very insults the post-arrest child is prone to: hypoxia and hyperoxia, hypocarbia and hypercarbia, hypotension, fever, hyperglycaemia and seizures.[1][7]
The heart is stunned too. Post-arrest myocardial dysfunction — a reversible, global reduction in contractility peaking at 6 to 24 hours after ROSC — produces hypotension and a low cardiac output state that can drop cerebral perfusion below the injured brain's already-impaired autoregulatory threshold. This is why haemodynamic support, not just oxygen, is central to post-arrest care.[1]
Clinical Presentation
The arrested child is found unresponsive, with absent or abnormal (gasping or agonal) breathing and no central pulse. In an infant, a heart rate below 60 per minute with signs of poor perfusion despite effective ventilation is the threshold to begin compressions, because a bradycardic, poorly perfusing infant is functionally arrested. Recognition must take less than 10 seconds — hesitation is the commonest and most lethal error.[2][3]
The presentation immediately before arrest — the peri-arrest state — is where prevention lives. The child who is tachypnoeic with recessions and increasing work of breathing, then becomes slow, dusky and bradycardic, is describing the classic descent into asphyxial arrest. A falling level of consciousness, a rising respiratory rate that then falls as the child tires, grunting that goes silent, and a heart rate that drifts downward are pre-arrest signs demanding escalation before the pulse is lost.[2]
After ROSC, the presentation is the post-arrest syndrome. The child is typically comatose, intubated and ventilated, hypotensive from myocardial stunning and vasoplegia, and at risk of seizures, fever and re-arrest. The clinician shifts from the scripted compression-ventilation rhythm of arrest to the sustained, multimodal optimisation of perfusion, oxygenation, ventilation, temperature, glucose and the brain.[1]
Differential Diagnosis
The differential serves two purposes during and after an arrest. During compressions it forces the team to hunt for reversible causes; after ROSC it prompts investigation of the precipitant that will otherwise cause re-arrest. The structured 4 Hs and 4 Ts frame the search and should be voiced aloud by the team leader every two minutes.[2]
The 4 Hs (and the rest)
- Hypoxia: the commonest paediatric cause — verify airway, oxygen and ventilation first
- Hypovolaemia: give a 10 to 20 mL per kg bolus of isotonic crystalloid for shock; reassess for cardiogenic causes before repeating
- Hypo- or hyperkalaemia, hypocalcaemia, metabolic crisis: check a point-of-care blood gas, glucose, potassium and calcium
- Hypothermia: rewarm, but avoid hyperthermia; respect the drowning and exposure context
The 4 Ts
- Tension pneumothorax: asymmetric breath sounds, tracheal deviation, haemodynamic collapse — needle or finger thoracostomy
- Tamponade (cardiac): muffled sounds, distended neck veins, electrical alternans — echo-guided pericardiocentesis
- Toxins: tricyclic antidepressant, beta-blocker, calcium-channel blocker, local anaesthetic, opioid — give specific antidotes (sodium bicarbonate, glucagon, lipid emulsion, naloxone)
- Thrombosis (massive pulmonary embolism or myocardial infarction): rare in children, consider in adolescents, prothrombotic states and central lines
For the precipitant, the question after ROSC is why did this child arrest? Sepsis, pneumonia, bronchiolitis, asthma, anaphylaxis, drowning, trauma, metabolic or electrolyte derangement, arrhythmia from cardiomyopathy or channelopathy, drug toxicity, and surgical emergencies such as appendicitis with septic shock all belong on the list, and each carries its own definitive treatment that must run in parallel with the post-arrest bundle.[1]
Clinical & Bedside Assessment
Assessment collapses into two questions that the team leader asks continuously: is there a pulse, and is the CPR good enough? The pulse check is central (brachial in infants, carotid or femoral in children), lasts no more than 10 seconds, and triggers compressions if the pulse is absent or the infant's heart rate is below 60 with poor perfusion. During compressions, the quality of CPR is monitored by end-tidal CO2, arterial line waveform, and depth and rate.[2][8]
High-quality CPR is defined by five measurable targets: compression depth of at least one third of the anteroposterior chest diameter (about 4 cm in infants and 5 cm in children), a rate of 100 to 120 per minute, full chest recoil between compressions, minimised interruptions (under 10 seconds for rhythm checks and shocks), and avoidance of excessive ventilation. Two-thumb encircling hands technique is preferred for infants with two rescuers; the lower half of the sternum is the landmark for all ages.[2][3]
End-tidal CO2 is the most useful real-time monitor. A sudden rise in end-tidal CO2 is a sensitive indicator of ROSC, because restoring cardiac output delivers CO2 from the periphery to the lungs. An end-tidal CO2 persistently below 10 to 15 mmHg during CPR signals poor-quality compressions or a poor prognosis, and should prompt a check of technique and the reversible causes. Physiologic, feedback-guided CPR — titrating depth, rate and vasopressors to arterial pressure and end-tidal CO2 targets — improved survival with favourable neurologic outcome in the multicentre ICU-RESUS trial.[8]
Investigations
Investigations during cardiac arrest are point-of-care and reversible-cause-directed only. Do not interrupt compressions for imaging. A blood gas, glucose, potassium, calcium, lactate and haemoglobin guide correction of the 4 Hs; an echocardiographic (sub-xiphoid) view during the pulse check can distinguish fine VF from asystole and reveal tamponade or poor contractility. After ROSC, a 12-lead ECG screens for ischaemia and arrhythmia, a chest X-ray confirms tube position and excludes pneumothorax, and targeted bloods seek the precipitant.[1][2]
After ROSC, continuous monitoring drives the post-arrest bundle. Arterial line blood pressure, continuous or near-continuous EEG for seizure detection, temperature monitoring, point-of-care glucose and blood gas for oxygenation, ventilation and electrolytes form the minimum dataset. Echocardiography assesses post-arrest myocardial dysfunction and guides vasoactive choice. Neuroprognostication uses a multimodal panel — examination, continuous EEG, somatosensory evoked potentials, neuroimaging and biomarkers — applied late and never on the basis of a single modality.[1][7]
ROSCARREST
Management — Resuscitation
The first minutes determine survival. The scripted sequence is: recognise the arrest in under 10 seconds, call for help, start high-quality CPR, open the airway and ventilate with 100 percent oxygen, attach a monitor, and establish IO or IV access. Because most paediatric arrests are asphyxial, effective ventilation is both the diagnosis-confirming and the first therapeutic act; a single rescuer performs 30 compressions to 2 ventilations, while two rescuers use 15 to 2.[2][4]
Adrenaline is the vasoconstrictor that raises aortic diastolic and coronary perfusion pressure during compressions. Give 10 micrograms per kilogram (0.01 mg per kg, that is 0.1 mL per kg of 1 in 10,000) by the IV or IO route every 3 to 5 minutes. Intraosseous access is preferred and should be placed early when IV access is not immediately available; the endotracheal route is no longer recommended because absorption is unreliable. Adrenaline is given to non-shockable rhythms as soon as access is established, and to shockable rhythms after the second defibrillation.[2][12]
Defibrillation is reserved for VF and pulseless VT. Deliver the first shock at 2 to 4 J per kg using a biphasic defibrillator with appropriately sized pads; subsequent shocks use at least 4 J per kg, escalating to a maximum of 10 J per kg. Resume compressions immediately after each shock and check the rhythm only after a full two-minute cycle, because shocks interrupt coronary perfusion and most shocks fail without high-quality CPR running underneath. An observational study found that a first-shock dose of 2 J per kg was associated with improved survival to discharge for in-hospital arrest in VF or pVT.[2][11]
For refractory VF or pVT, give amiodarone 5 mg per kg IV or IO (maximum 300 mg) after the third shock, repeated up to a total of 15 mg per kg per day, with lidocaine 1 mg per kg as the alternative if amiodarone is unavailable. Magnesium 25 to 50 mg per kg (maximum 2 g) is reserved for torsades de pointes or known hypomagnesaemia.[2]
Adrenaline (epinephrine) 1 in 10,000
Dose
10 micrograms per kg (0.1 mL per kg of 1 in 10,000)
Management — Definitive & Stepwise
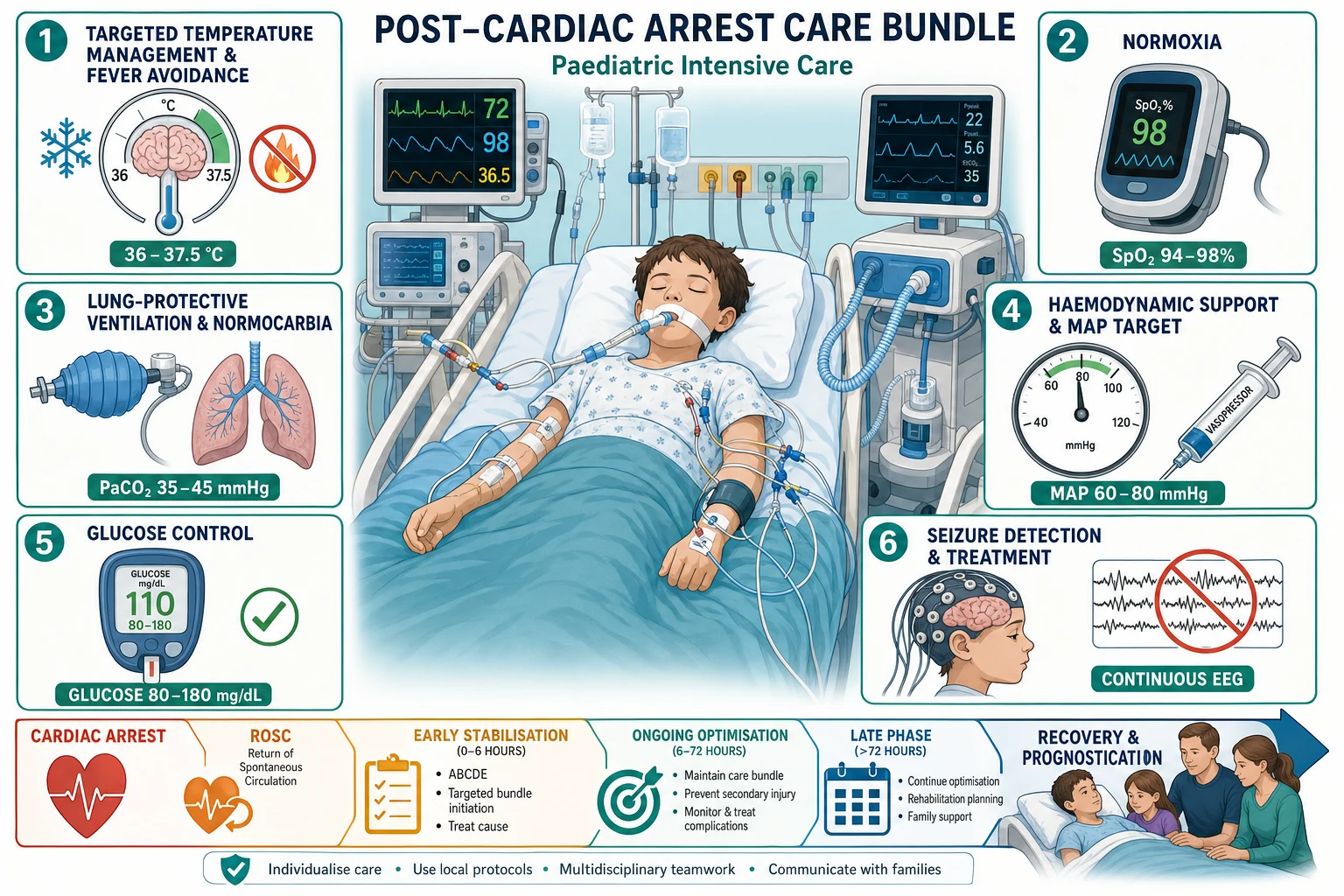
When ROSC is achieved — a palpable pulse returns, the end-tidal CO2 jumps, and the monitor shows an organised rhythm — the team pivots to the post-arrest care bundle. This is the phase that decides neurologic outcome, and it is delivered as a single, simultaneous, protocol-driven package rather than a sequence of afterthoughts.[1][3]
Airway and breathing
- Intubate early for the comatose child; confirm tube position with waveform capnography and chest X-ray
- Target normoxia: titrate FiO2 to the lowest value keeping SpO2 at 94 to 99 percent to avoid hyperoxia, which is associated with worse outcome
- Target normocarbia: ventilate to PaCO2 35 to 45 mmHg (4.7 to 6.0 kPa); avoid hyperventilation and prophylactic hypocarbia, which cause cerebral vasoconstriction
Circulation
- Treat post-arrest myocardial dysfunction and vasoplegia: start an adrenaline or noradrenaline infusion for hypotension, add milrinone for low cardiac output with high filling pressures
- Maintain an age-appropriate mean arterial pressure and a systolic blood pressure at or above the 50th percentile; never accept hypotension, which is linked to death and poor neurologic outcome
- Assess volume status with echocardiography; give cautious 5 to 10 mL per kg boluses only if hypovolaemic, avoiding overload in cardiogenic arrest
Brain-directed care
- Targeted temperature management: maintain 36 to 37.5 degrees C with active normothermia; treat any temperature at or above 37.5 to 38 degrees C aggressively with antipyretics and cooling
- Therapeutic hypothermia at 32 to 34 degrees C is no longer superior to normothermia after the THAPCA trials showed no outcome difference
- Detect and treat seizures with continuous EEG; avoid hypoglycaemia and marked hyperglycaemia; keep the head midline and elevated 30 degrees
THAPCA-OH and THAPCA-IH (Moler 2015, 2017, NEJM)
Two parallel multicentre randomised controlled trials of comatose children after out-of-hospital and in-hospital cardiac arrest
Population: Children aged 2 days to 18 years, comatose after cardiac arrest, across North American PICUs
Key finding
No significant difference in 12-month survival with a favourable neurologic outcome in either trial; outcomes were poor in both arms overall, and survivors carried a substantial burden of neurologic disability
Targeted temperature management in detail
Targeted temperature management means keeping the brain at a deliberate, controlled temperature rather than letting it drift. The THAPCA trials randomised comatose children to two days of hypothermia at 32 to 34 degrees C versus five days of normothermia at 36 to 37.5 degrees C, and found no difference in survival with favourable neurologic outcome. The 2020 American Heart Association guideline therefore allowed either strategy after out-of-hospital arrest, while the 2025 American Heart Association and Academy of Pediatrics and the 2025 European Resuscitation Council guidelines now recommend targeted temperature management with normothermia at 36 to 37.5 degrees C and the active prevention and treatment of fever.[2][3][4]
The harm to avoid is hyperthermia, which worsens secondary brain injury. Treat any temperature at or above 37.5 degrees C with paracetamol and surface or intravascular cooling; treat shivering with sedation and, where needed, a low-dose neuromuscular blocker. Conversely, avoid inadvertent overcooling below 32 degrees C unless a specific hypothermia protocol is being followed, because uncontrolled hypothermia brings bleeding and infection. The target is a steady, monitored 36 to 37.5 degrees C for at least five days in the comatose child.[1][3]
Blood pressure, oxygen and ventilation targets
Hypotension after ROSC is associated with increased mortality and worse neurologic outcome. The ICU-Resuscitation study identified age-specific mean arterial pressure thresholds below which outcomes deteriorate, and a 2025 systematic review confirmed that maintaining a higher post-arrest blood pressure target is associated with better survival. The practical rule is to maintain a mean arterial pressure at or above age-appropriate norms and a systolic blood pressure at or above the 50th percentile, escalating vasoactives early rather than accepting borderline perfusion.[9]
For oxygen, avoid both hypoxia and hyperoxia. Wean the FiO2 to the lowest value that keeps SpO2 at 94 to 99 percent; observational data show an association between hyperoxia and worse survival and neurologic outcome. For ventilation, target normocarbia with a PaCO2 of 35 to 45 mmHg (4.7 to 6.0 kPa); avoid the older practice of prophylactic hyperventilation, which causes cerebral vasoconstriction and worsens ischaemia, reserving hyperventilation only for the acute management of impending herniation.[10][1]
Recognise the arrest within 10 seconds; call for help; start high-quality CPR and ventilate with 100 percent oxygen.
Attach the monitor; check the rhythm every 2 minutes; defibrillate VF or pVT at 2 to 4 J per kg, then at least 4 J per kg.
Establish IO or IV access; give adrenaline 10 micrograms per kg every 3 to 5 minutes; amiodarone 5 mg per kg after the third shock for refractory VF or pVT.
Voice the 4 Hs and 4 Ts every cycle; correct hypoxia, hypovolaemia, potassium, glucose, pneumothorax, tamponade, toxins and thrombosis.
Achieve ROSC — confirm pulse, organise airway and monitoring; move to the post-arrest bundle.
Bundle: targeted temperature management 36 to 37.5 degrees C, normoxia SpO2 94 to 99 percent, normocarbia PaCO2 35 to 45 mmHg, age-appropriate blood pressure, glucose control, continuous EEG.
Identify and treat the precipitant (sepsis, arrhythmia, toxins, metabolic); plan delayed multimodal prognostication at 72 hours or later.
Support the family throughout; debrief the team; arrange rehabilitation for survivors.
Specific Subtypes & Scenarios
The witnessed, monitored in-hospital arrest carries the best prognosis and is where high-quality CPR saves the most lives. Rapid response systems, physiologic feedback-guided compressions and early adrenaline compress the no-flow and low-flow intervals that determine outcome. The ICU-RESUS trial showed that training PICU teams to titrate CPR to arterial-pressure and end-tidal CO2 targets improved survival with favourable neurologic outcome.[8]
Out-of-hospital arrest, especially unwitnessed or asphyxial, has a far poorer outlook. Bystander CPR and early dispatch of emergency services are the modifiable levers; the receiving hospital should continue high-quality CPR and proceed to the post-arrest bundle if ROSC is achieved. Drowning and sudden infant death are the classic OHCA scenarios in children.[2]
Refractory arrest and ECPR. For in-hospital arrest that is refractory to conventional CPR but potentially reversible — typically a witnessed, monitored arrest in a child with a cardiac or post-surgical substrate — extracorporeal cardiopulmonary resuscitation (ECPR) using veno-arterial extracorporeal membrane oxygenation can restore perfusion while the heart and lungs recover. Registry data show survival to discharge in a meaningful proportion of well-selected children, and ECPR is incorporated into contemporary algorithms for refractory in-hospital arrest in centres with the capability.[3]
Pulmonary hypertensive crisis is a specific, lethal scenario in children with repaired or unrepaired congenital heart disease: a surge in pulmonary vascular resistance produces acute right-heart failure and a pulseless low-output state. Treatment is high-dose oxygen, alkalosis, inhaled nitric oxide or prostacyclin, and inotropes, with ECMO as rescue.[1]
The perioperative or procedural arrest — sedation-related, anaesthetic, or catheter-lab — demands identification of the trigger (hypoxia, hypotension, local-anaesthetic toxicity, vagal response) and reversal (naloxone, flumazenil, lipid emulsion, atropine, fluid).[2]
Complications & Pitfalls
The dominant complication is post-arrest brain injury: the leading cause of death in PICU arrest survivors, it shows itself as seizures, impaired consciousness, and long-term cognitive and behavioural disability in a substantial proportion of survivors, even with excellent care. Layered on top are the harms of intensive-care therapies themselves and the ever-present risk of re-arrest if the precipitant is not controlled.[1][7]
Pitfalls are the recurring, preventable failures that kill. Poor-quality CPR — compressions too shallow or too slow, leaning on the chest, long pauses for rhythm checks or intubation — is the commonest remediable problem and the reason feedback devices and end-tidal CO2 monitoring exist. Delayed adrenaline, particularly in non-shockable rhythms, is associated with worse outcome; establish IO access early. Over-ventilation during CPR raises intrathoracic pressure and drops coronary perfusion; ventilate at 20 to 30 breaths per minute during arrest, not faster. Failing to look for reversible causes — especially tension pneumothorax and tamponade in the deteriorating child — converts a survivable arrest into a death.[2][8]
After ROSC, the dominant pitfalls are accepting hypotension, allowing fever, inducing hyperoxia, hyperventilating to hypocarbia, and missing non-convulsive seizures on a comatose child without continuous EEG. Premature prognostication — declaring futility on a single early examination or one EEG — is a grave and well-described error; modern guidelines mandate a delayed, multimodal assessment.[1][7]
Prognosis & Disposition
Outcomes divide sharply by location and rhythm. In-hospital arrest survival to discharge is approximately 35 to 45 percent, with a majority of survivors neurologically intact or only mildly impaired; out-of-hospital arrest survival to discharge is approximately 8 to 12 percent and is heavily dependent on witness status, bystander CPR and the presenting rhythm. Children who arrest in VF or pVT, who receive rapid high-quality CPR and early adrenaline, and who avoid sustained post-arrest hypotension and hyperoxia do best.[1][2]
Neuroprognostication must be delayed, multimodal and humble. Wait at least 72 hours after ROSC (and longer where sedation or targeted temperature management confound the examination), then combine the neurologic examination, continuous EEG background and reactivity, somatosensory evoked potentials, neuroimaging and neuron-specific biomarkers into a consensus judgement. No single predictor — including an early absent motor response or a single suppressed EEG — reliably predicts poor outcome after paediatric arrest, and decisions to limit life-sustaining treatment should rest on concordant, serial, multimodal evidence.[1][7]
Disposition is to a PICU with neurocritical-care capability, with continuous EEG, temperature and arterial-pressure monitoring, early rehabilitation input, and structured family communication and support. Survivors need longitudinal neurodevelopmental follow-up because cognitive, behavioural and quality-of-life impairments emerge over months and are common even in children who appear to recover well.[1]
Special Populations
The neonate and young infant arrests almost exclusively from asphyxia, sepsis or congenital heart disease; the threshold to compress is a heart rate below 60 despite effective ventilation, and the team must consider duct-dependent congenital heart disease and start a prostaglandin infusion when a cyanotic lesion is suspected. Neonatal resuscitation follows its own guideline (the ILCOR neonatal algorithm) and is addressed in the neonatal domain.[2]
Children with congenital heart disease and cardiac surgical patients form a high-risk subgroup with specific failure modes — pulmonary hypertensive crisis, tamponade, low cardiac output syndrome, arrhythmia — and benefit from rapid access to ECMO and cardiology. Technology-dependent children with tracheostomies, home ventilation and complex chronic conditions arrest from airway or ventilator failure and need caregivers trained in resuscitation.[1]
Immunocompromised children may arrest from sepsis with atypical organisms or from treatment-related cardiotoxicity, and carry a worse prognosis. Adolescents increasingly arrest from sudden cardiac death (cardiomyopathy, channelopathy, commotio cordis), drug overdose and suicide, demanding an arrhythmia work-up, toxicology and mental-health follow-up for survivors.[1][4]
Indigenous, rural and remote, and socioeconomically disadvantaged children present later, arrest more often from preventable respiratory and infectious causes, and have worse outcomes; retrieval systems, early recognition and equitable access to PICU and rehabilitation are the corrective priorities.[1]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric post-arrest care has been reshaped by three landmark bodies of work. The THAPCA trials (Moler 2015, 2017) randomised comatose children to hypothermia or normothermia and found no difference in survival with favourable neurologic outcome, retiring routine therapeutic hypothermia and establishing targeted temperature management with normothermia as the standard. The ICU-RESUS trial (Sutton 2022) showed that physiologic, feedback-guided CPR improved survival with favourable neurologic outcome in PICU arrest. Observational studies of post-arrest oxygenation, blood pressure and seizures established hyperoxia, hypotension and untreated seizures as modifiable harms.[1][5][6][8]
Australian and New Zealand practice follows the ANZCOR guidelines, the Royal Children's Hospital Melbourne clinical practice guideline, and the Australian Resuscitation Council. Adrenaline is 10 micrograms per kg IV or IO every 3 to 5 minutes; the first shock is 2 to 4 J per kg escalating to a maximum of 10 J per kg. Post-arrest care uses targeted temperature management with normothermia 36 to 37.5 degrees C, normoxia, normocarbia, and avoidance of hypotension, with early retrieval to a PICU and structured support for rural and remote and Aboriginal and Torres Strait Islander children and whanau.[4]
In low- and middle-income settings, paediatric arrest is dominated by asphyxia, sepsis and preventable respiratory failure, and outcomes are worse for lack of rapid access, oxygen and intensive care. The World Health Organization and basic life-support teaching emphasise bystander CPR, early oxygen, and a functional emergency and referral system; where PICU and targeted temperature management are unavailable, prevention, recognition and high-quality basic resuscitation carry the greatest benefit.[1]
Controversies include the optimal post-arrest blood-pressure target, whether any subgroup benefits from hypothermia, the role of ECPR in out-of-hospital arrest, the timing and dose of adrenaline in OHCA (the subject of ongoing trials of early intramuscular adrenaline), and the best multimodal prognostication algorithm. The convergence of the 2025 American and European guidelines around normothermia rather than hypothermia is the clearest recent shift.[3][4]
Exam Pearls
POSTROSC
- Adrenaline is 10 micrograms per kg IV or IO every 3 to 5 minutes, first dose immediately for non-shockable rhythms and after the second shock for shockable rhythms.[2][12]
- Defibrillate VF and pVT at 2 to 4 J per kg first, then at least 4 J per kg up to 10 J per kg, with amiodarone 5 mg per kg after the third shock.[2][11]
- THAPCA retired routine hypothermia — current care is targeted temperature management with normothermia 36 to 37.5 degrees C and aggressive fever avoidance.[5][6]
- Hypotension, hyperoxia, hypocarbia, fever and untreated seizures are the modifiable harms of post-arrest brain injury; each is independently linked to worse outcome.[9][10]
- Physiologic, feedback-guided CPR improved survival in the ICU-RESUS trial; monitor end-tidal CO2 and arterial pressure and titrate compressions.[8]
- Never prognosticate on a single early examination or one EEG — wait at least 72 hours and combine examination, EEG, evoked potentials, imaging and biomarkers.[1][7]
Quick check: a comatose child four hours after ROSC has a temperature of 38.2 degrees C, SpO2 of 100 percent on FiO2 1.0, and a mean arterial pressure at the 10th percentile for age. Which three post-arrest harms are active and what do you do?
All three classic harms are present: fever, hyperoxia and hypotension. Cool the child actively with paracetamol and surface cooling to 36 to 37.5 degrees C and treat shivering; wean the FiO2 to the lowest value keeping SpO2 at 94 to 99 percent; and start a vasoactive infusion (adrenaline or noradrenaline, with milrinone for low cardiac output) to lift the mean arterial pressure to age-appropriate norms. Each of these insults worsens secondary brain injury and is independently associated with poor outcome.[1][9][10]
References
- [1]Topjian AA, de Caen A, Wainwright MS, Abella BS, Abend NS, Atkins DL, et al. Pediatric Post-Cardiac Arrest Care: A Scientific Statement From the American Heart Association. Circulation, 2019.PMID 31242751
- [2]Topjian AA, Raymond TT, Atkins D, Chan M, Duff JP, Joyner BL Jr, et al. Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2020.PMID 33081526
- [3]Lasa JJ, Dhillon GS, Duff JP, Ganti L, Hsieh TC, Kessler SK, et al. Part 8: Pediatric Advanced Life Support: 2025 American Heart Association and American Academy of Pediatrics Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2025.PMID 41122885
- [4]Djakow J, Turner NM, Skellett S, Stone K, Buss PW, Baldi E, et al. European Resuscitation Council Guidelines 2025 Paediatric Life Support. Resuscitation, 2025.PMID 41117571
- [5]Moler FW, Silverstein FS, Holubkov R, Slomine BS, Christensen JR, Nadkarni VM, et al. Therapeutic hypothermia after out-of-hospital cardiac arrest in children. N Engl J Med, 2015.PMID 25913022
- [6]Moler FW, Silverstein FS, Holubkov R, Slomine BS, Christensen JR, Nadkarni VM, et al. Therapeutic Hypothermia after In-Hospital Cardiac Arrest in Children. N Engl J Med, 2017.PMID 28118559
- [7]Ichord R, Silverstein FS, Slomine BS, Telford R, Christensen J, Holubkov R, et al. Neurologic outcomes in pediatric cardiac arrest survivors enrolled in the THAPCA trials. Neurology, 2018.PMID 29884735
- [8]ICU-RESUS and Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network Investigator Groups, Sutton RM. Effect of Physiologic Point-of-Care Cardiopulmonary Resuscitation Training on Survival With Favorable Neurologic Outcome in Cardiac Arrest in Pediatric ICUs: A Randomized Clinical Trial. JAMA, 2022.PMID 35258533
- [9]Gardner MM, Hehir DA, Reeder RW, Yates AR, Ahmed T, Asaro LA, et al. Identification of post-cardiac arrest blood pressure thresholds associated with outcomes in children: an ICU-Resuscitation study. Crit Care, 2023.PMID 37805481
- [10]Barreto JA, Weiss NS, Nielsen KR, Morgan RW, Robertsen TK, Stovel EV, et al. Hyperoxia after pediatric cardiac arrest: Association with survival and neurological outcomes. Resuscitation, 2022.PMID 34906621
- [11]Hoyme DB, Zhou Y, Girotra S, Tan HKS, Mahant T, Kaye W, et al. Improved survival to hospital discharge in pediatric in-hospital cardiac arrest using 2 Joules/kilogram as first defibrillation dose for initial pulseless ventricular arrhythmia. Resuscitation, 2020.PMID 32522702
- [12]Ohshimo S, Wang CH, Couto TB, Matsuura Y, Watanabe E, Kirschen MP, et al. Pediatric timing of epinephrine doses: A systematic review. Resuscitation, 2021.PMID 33529645