Paeds · acute-care-resuscitation-and-toxicology
Care after death, unexpected child death and family support
Also known as Care after death · Sudden unexpected death in infancy (SUDI) · Sudden infant death syndrome (SIDS) · Sudden unexpected death in childhood (SUDIC) · Bereavement support in paediatrics · Coronial referral and child death review · Breaking bad news after a child death
Fellowship guide to care after a child's death and the unexpected child death: distinguishing expected from unexpected death, confirming death and the certification and coronial referral rules, breaking bad news with SPIKES, family time and memory-making, the SUDI and SUDIC definitions and the triple risk model of SIDS, the AAP 2022 safe-sleep recommendations, the multi-agency SUDI response with a joint paediatrician-and-police home visit, bereavement follow-up and sibling support, team welfare and child death review, with the ANZ, UK and North American differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A child's death is the single hardest event in paediatric practice, and the way you behave in the hours around it is remembered by the family for the rest of their lives. This page covers two overlapping jobs: the immediate and longitudinal care after death delivered to every bereaved family, and the structured response to the unexpected child death, which carries safeguarding, coronial and public-health duties that an expected death does not.[7][8]
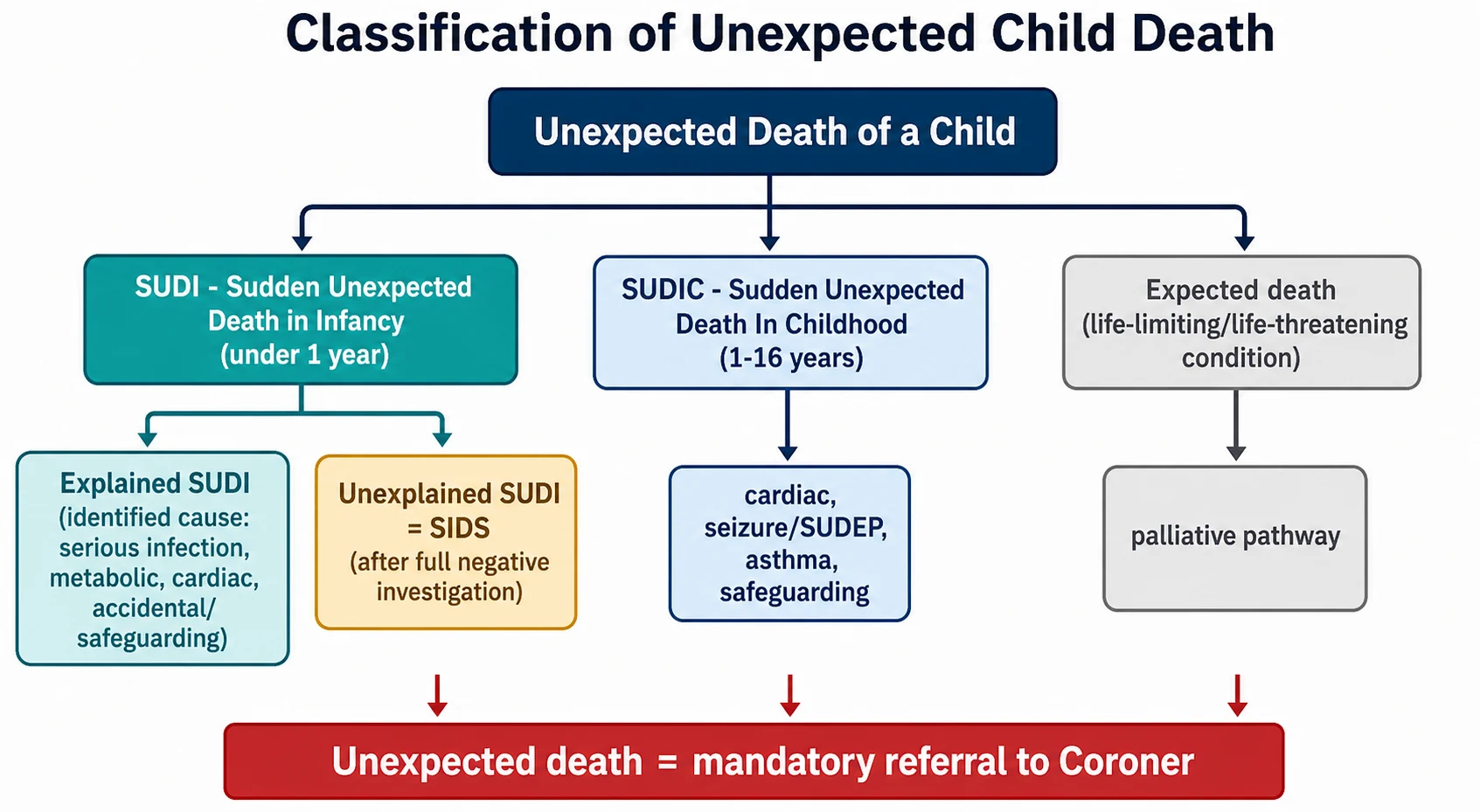
The first decision, made within minutes, sorts the death into one of two streams that determine everything which follows. An expected death is the death of a child with a known life-limiting or life-threatening condition, anticipated on an advance care plan, and it can be certified by the attending doctor. An unexpected death is a death that was not reasonably anticipated within the preceding 24 hours, or that is sudden, violent, of unknown cause, or occurs in custody, and it must be reported to the coroner and must not be certified.[2][3]
Within the unexpected stream sits the most studied entity in paediatric mortality: sudden unexpected death in infancy (SUDI), defined as the sudden and unexpected death of an infant under one year in whom the cause is not immediately obvious. After a complete investigation — history, scene review and post-mortem — a SUDI is reclassified as either explained (an identified cause such as infection, metabolic disease, cardiac disorder, accidental or inflicted injury) or unexplained.[3][4]
Only the unexplained subgroup, after that complete negative work-up, may be labelled sudden infant death syndrome (SIDS). SIDS is therefore a diagnosis of exclusion, never a scene diagnosis. For older children the parallel term is sudden unexpected death in childhood (SUDIC), covering the sudden death of a child beyond infancy.[11]
The clinician's task across both streams is to confirm the death, disclose it with compassion, offer time and memory-making, meet the legal and investigative duties without compromising them, and then sustain the family through bereavement. This page walks that pathway in the order it happens at the bedside.
[3] [7]Classification
The death is best classified along three axes that together decide the legal pathway, the investigation and the bereavement message. The first is expected versus unexpected, which sets whether you certify or refer to the coroner. The second, within the unexpected stream, is age: SUDI for under one year and SUDIC for beyond infancy. The third, within SUDI, is explained versus unexplained, reached only after the full investigation is complete.[3][4]
Expected death
- Known life-limiting or life-threatening condition, anticipated on an advance care plan
- Attending doctor MAY certify the cause of death and complete a Medical Certificate of Cause of Death
- Coroner referral only if a specific criterion is met (sudden, of unknown cause, related to a procedure, or any safeguarding concern)
- Family-centred care and bereavement support as for any death, with palliative services involved
Unexpected death (SUDI, under 1 yr)
- Sudden death of an infant under one year where the cause is not immediately obvious
- MUST be reported to the coroner; do NOT certify
- Triggers the multi-agency SUDI response: joint home visit by a designated paediatrician and police, scene review, post-mortem
- After complete investigation: explained (infection, metabolic, cardiac, accidental, inflicted) or unexplained = SIDS
Unexpected death (SUDIC, over 1 yr)
- Sudden unexpected death of a child beyond infancy, e.g. cardiac arrhythmia, epilepsy/SUDEP, asthma, anaphylaxis, infection, trauma
- Same coronial referral and multi-agency rules as SUDI
- Cardiac and genetic screening of first-degree relatives is often indicated (channelopathies, cardiomyopathy)
- Adolescent sudden death prompts suicide, overdose and sudden cardiac death consideration
Epidemiology & Risk Factors
SIDS remains the leading category of post-neonatal infant death in high-income countries, even after the dramatic fall that followed the back-to-sleep campaigns of the early 1990s. The incidence peaks at 2 to 4 months of age, and over 90 percent of SIDS deaths occur before 6 months, which is why the safe-sleep message concentrates on the first six months and the developmental window used by the triple risk model.[1][6]
The risk factors separate cleanly into the ones a family can change and the ones they cannot. Modifiable risk factors are the foundation of prevention: the prone or side sleeping position, a soft or inclined sleep surface, loose bedding and soft objects, bed-sharing, overheating, and smoke exposure in pregnancy and after birth. The protective factors are the mirror image: supine sleep on a firm flat surface, the infant's own sleep space, room-sharing without bed-sharing, breastfeeding, a pacifier, and a smoke-free environment.[1][6]
The non-modifiable risks matter for counselling rather than prevention. They include male sex, prematurity and low birth weight, younger maternal age, socioeconomic disadvantage and a winter peak. None of these can be changed, but they explain why some families carry higher baseline risk and why prevention messages must reach them most.[1]
The single most powerful modifiable risk after sleep position is smoke exposure. Maternal smoking in pregnancy and postnatal smoke exposure multiply SIDS risk several-fold, both by impairing autonomic and arousal development in utero and by continuing exposure after birth. This is why the safe-sleep conversation is incomplete unless it opens the smoke-free conversation.[1]
Socioeconomic disadvantage, overcrowding, rural and remote location, and indigenous heritage are associated with higher SUDI rates and later presentation, not because of biology but because of housing, heating, bedding, access to care and the legacy of colonisation. The implication for practice is that safe-sleep messaging must be culturally safe, practical and free of shame, delivered with the family rather than to them.[2][6]
Pathophysiology
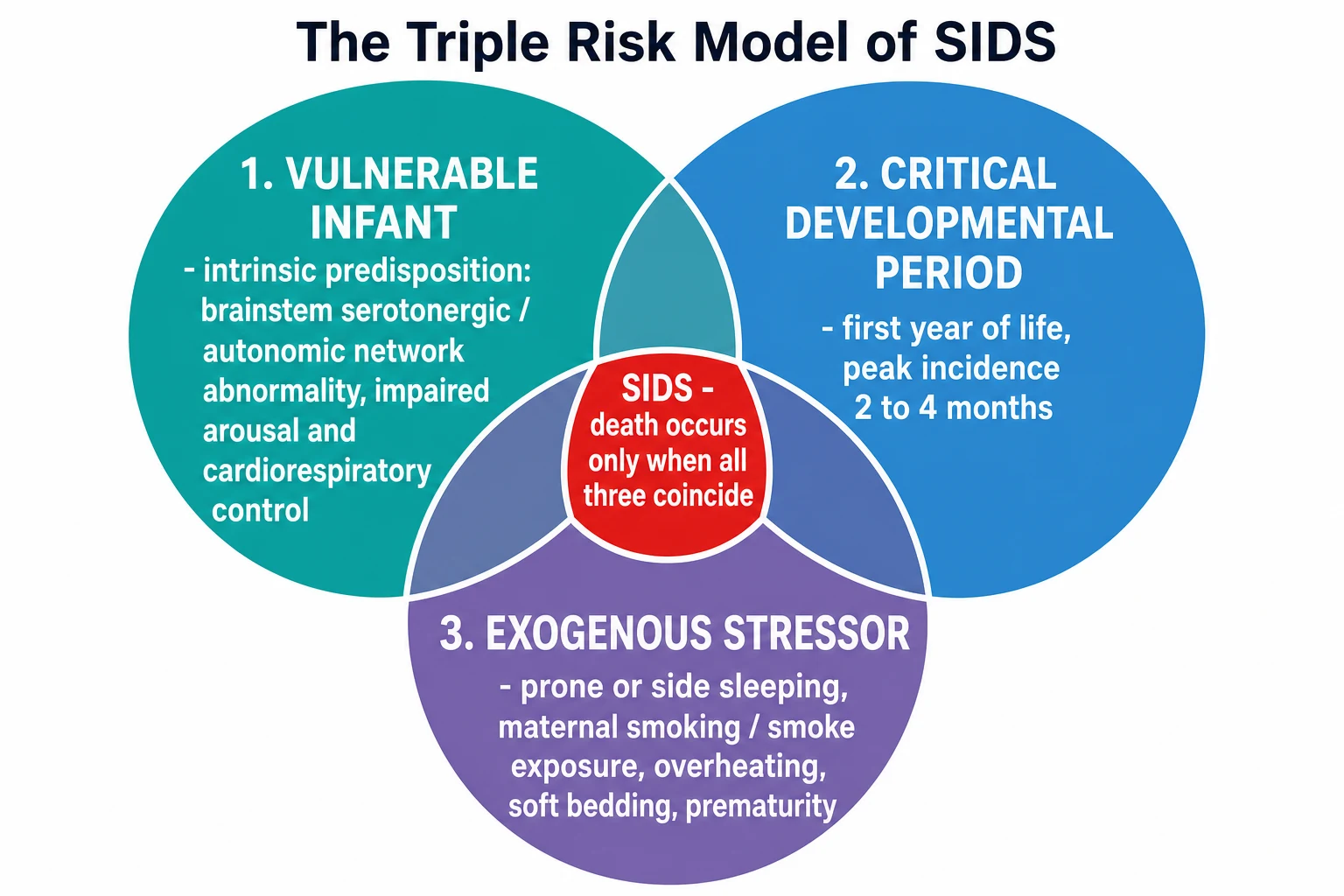
SIDS does not have a single cause, and that is the central teaching point. The framework that explains why an infant dies at a particular age and in a particular setting is the triple risk model: death occurs only when three things coincide — a vulnerable infant, a critical developmental period, and an exogenous stressor. Remove any one of the three and the infant survives the night.[5]
The vulnerable infant carries an intrinsic, usually invisible, predisposition. The most consistent finding across decades of neuropathology is an abnormality of the serotonergic (5-HT) network in the medullary brainstem, the region that governs arousal, autoresuscitation (gasping), heart-rate variability and respiratory drive. Infants who die of SIDS are less able to arouse from sleep and less able to autoresuscitate when they become hypoxic or hypercarbic.[5]
The critical developmental period is the first year, with the risk concentrated between 2 and 4 months when sleep architecture, autonomic control and respiratory drive are all maturing rapidly and unevenly. This is why SIDS is vanishingly rare in the first week and after a year — the developmental window has either not opened or has largely closed.[5]
The exogenous stressor is the one leg of the tripod the family and clinician can actually remove. Prone and side sleeping impair arousal, cause rebreathing of expired gases, increase upper-airway obstruction and reduce heat loss. Soft surfaces, loose bedding and bed-sharing do the same. Overheating and smoke exposure further blunt the already-impaired arousal response. When this stressor lands on a vulnerable infant in the critical window, arousal fails, autoresuscitation fails, and the infant dies silently.[1][5]
Clinical Presentation
The unexpected infant death presents in one of two ways that shape the team's first moves. Most commonly the family calls emergency services after finding the infant limp, pale or mottled, cold, apnoeic and pulseless in a sleep environment, and resuscitation is attempted and then ceased either at home or on arrival. Less often, the infant arrives in the emergency department during an ongoing, ultimately unsuccessful resuscitation after a collapse witnessed at home.[3]
At the moment of disclosure the parents are usually in shock: numb, disbelieving, sometimes angry, often desperate to have done something differently. How they appear at this moment is not a guide to how they will grieve later, and it must not be recorded as such. Your job is to deliver the news clearly, to allow the reaction, and to offer time.[7][12]
Certain features in the history and scene must be noted and, if present, escalate the safeguarding and forensic response. These include an inconsistent or changing account, a delay in calling for help, a history of previous infant deaths in the family, marks or injuries on examination, a sleep arrangement that is unsafe for the infant's age, and parental intoxication or impairment. None of these proves harm, but each demands that the death be treated as unexpected and referred, with the multi-agency process allowed to do its work.[3][4]
An expected death at home, in hospice or on the ward presents differently. The family have usually been preparing, an advance care plan is in place, the child is in a familiar setting, and the immediate tasks are confirmation, certification, family time and bereavement support rather than coronial referral.[7]
Siblings are part of the presentation even when they are not in the room. Anticipate and ask about regression (bed-wetting, clinging), guilt ("was it my fault?"), school difficulty, sleep disturbance and somatic complaints, because these are common, often missed, and amenable to honest explanation and routine.[8]
Differential Diagnosis
The differential after an unexpected infant death is the list the post-mortem and investigation are designed to resolve, and naming it helps the team understand why a thorough work-up is non-negotiable. The categories are serious infection (sepsis, pneumonia, meningitis), metabolic disease (fatty-acid oxidation defects such as medium-chain acyl-CoA dehydrogenase deficiency, MCADD), cardiac disorders (channelopathies such as long-QT syndrome, cardiomyopathy, anomalous coronary artery), accidental or inflicted asphyxia, and, after everything else is excluded, the unexplained group labelled SIDS.[3][4]
The category that must never be missed is non-accidental injury and inflicted asphyxia. The same presentation — an infant found lifeless in a cot — can conceal inflicted head injury, airway obstruction or smothering. The scene and history features listed above are the triggers, and the safeguarding threshold is deliberately low: when the concern exists, the death is managed as unexpected and the multi-agency response runs in full.[3][4]
Several inherited causes carry implications for surviving relatives and demand family testing. A long-QT or other channelopathy found at molecular autopsy means first-degree relatives should have an ECG and genetic testing; MCADD and other metabolic disorders mean siblings may need biochemical screening. Missing these condemns the next death to happen in the same family.[3]
For the older child (SUDIC) the differential shifts toward cardiac arrhythmia and cardiomyopathy, epilepsy and SUDEP (sudden unexpected death in epilepsy), asthma, anaphylaxis and infection, with trauma, suicide and overdose rising in adolescence. Each carries its own cascade of family screening and prevention.[11]
The apparent life-threatening event (ALTE, now termed BRUE, brief resolved unexplained event) sits on the same pathway: an infant who is found cyanotic, limp or not breathing but who recovers. A BRUE that meets low-risk criteria needs only focused assessment, but a high-risk BRUE is investigated much like a SUDI that was narrowly survived.[3]
Clinical & Bedside Assessment
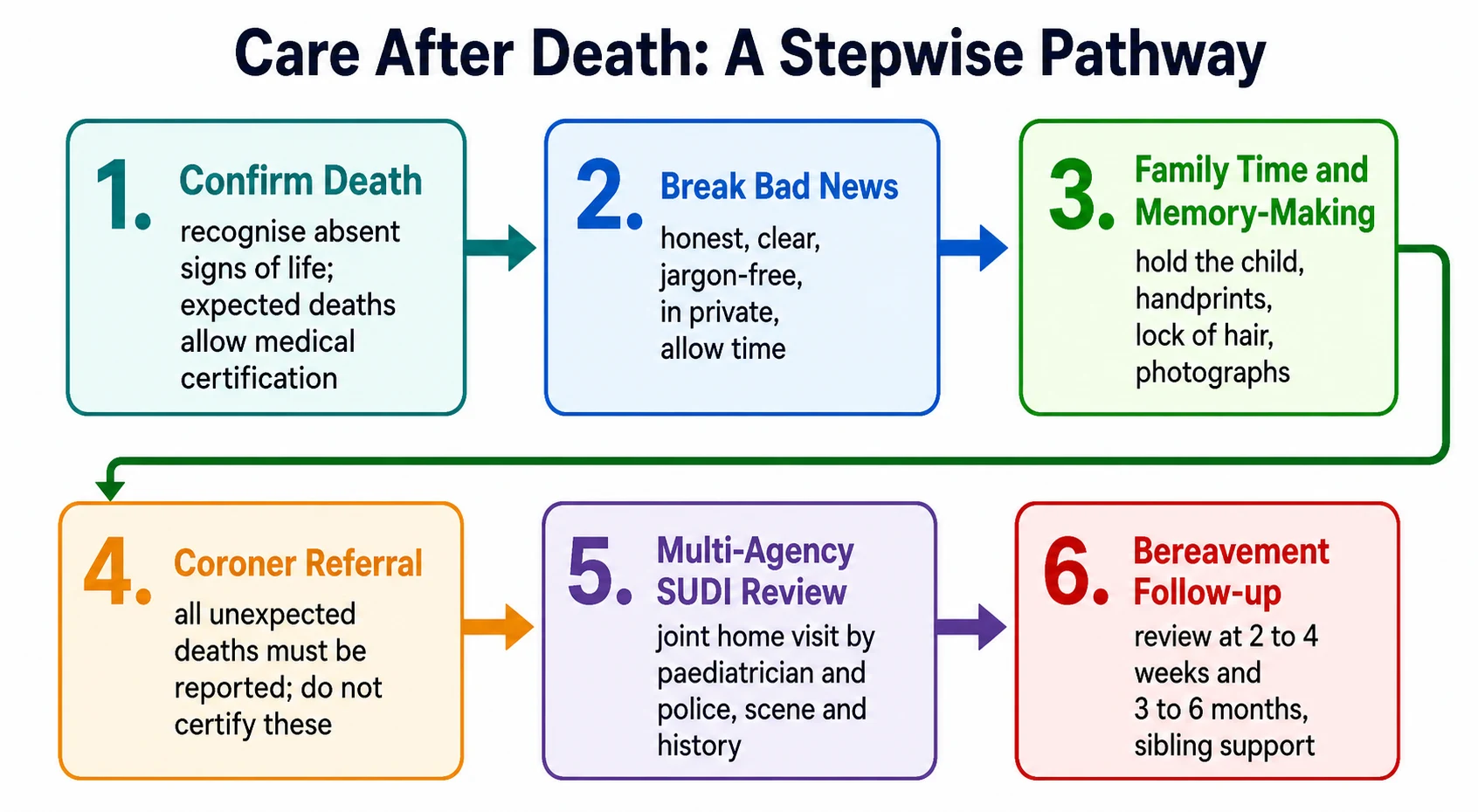
Confirming death is a clinical act and must be done with care. The signs are fixed and dilated pupils, absent heart sounds and central pulse on auscultation for at least a full minute, absent respiratory effort, and absent brainstem reflexes. Brain-stem death testing, with its formal apnoea component, applies only to a ventilated child in whom withdrawal of life support is being considered, not to the child who has already died in the community.[3]
For the unexpected death, the bedside assessment doubles as evidence-gathering. Once death is confirmed, do not remove lines, tubes or clothing, do not wash the child, and preserve any bedding or items that were with the infant, because these are part of the scene investigation. Document the sleep environment, position found, bedding, clothing, heating and the room, ideally photographically when a joint agency visit is conducted.[2][4]
The structured joint history is taken at the home visit, not in the chaos of the emergency department. It covers the last sleep period in detail (where, in what, in what position, with what bedding and clothing), the feeding history, intercurrent illness, maternal and household smoke exposure, the pregnancy, birth and postnatal course, and the family history of sudden death, cardiac disease, epilepsy, metabolic disease or consanguinity. This history is often where the explanation is found.[2][4]
In Australia and Aotearoa New Zealand the designated paediatrician conducts the joint home visit with police, usually within 24 to 48 hours, under the framework described by Jeffery and colleagues and the state SUDI guidelines. The RCH Melbourne and state-based SUDI services coordinate the scene review, the family meeting and the post-mortem referral.[2]
There are deliberate things to avoid. Do not certify an unexpected death. Do not propose a cause at the scene. Do not suggest SIDS before the investigation is complete. Do not remove or alter evidence. And do not, in the desire to be kind, block the family from time with their child.[3]
Investigations
The investigation bundle is the mechanism by which an unexplained SUDI becomes explained, unexplained, or SIDS, and it must be applied completely every time. It has four parts: the joint home visit and scene review, the structured history and clinical examination, the standardised post-mortem with histology, microbiology, virology, metabolic and toxicology, and, increasingly, molecular autopsy with cardiac and metabolic gene panels.[2][3]
Some samples are time-critical and are lost if they are not taken early. Blood, urine and vitreous samples for metabolic and toxicology, and a skin biopsy for fibroblast culture (for metabolic and chromosome studies), must be collected at or soon after death, because tissue viability falls quickly. This is why the protocol is written into the first response, not added later.[3][4]
Imaging supports the post-mortem. A plain skeletal survey looks for occult injury, and post-mortem imaging (whole-body CT or MRI, where available) can guide the autopsy and is increasingly used, as the French nationwide survey of SUDI imaging documented. Imaging never replaces the autopsy; it complements it.[3]
Targeted genetic testing is indicated when the autopsy is negative or equivocal and the history or family data suggest an inherited cause. A molecular autopsy with a cardiac channelopathy gene panel is now standard after an unexplained SUDI or SUDIC, because it identifies inherited arrhythmia syndromes in a meaningful proportion of otherwise unexplained cases and enables cascade testing of relatives.[3][11]
Results are communicated back in stages: preliminary findings to the family at the 2- to 4-week review, and final post-mortem and coronial findings at the 3- to 6-month meeting. The designated paediatrician usually owns this communication, supported by the coroner's officer and bereavement services.[2][9]
The child death review process is separate from the acute coronial investigation. In the UK it runs through the CDOP; in ANZ through equivalent state child death review committees. Its purpose is system learning and prevention — turning an individual death into changes that protect the next child — and it operates on de-identified aggregated data.[9]
Management — Resuscitation
The term "resuscitation" in a care-after-death context means the first, scripted actions of the response, not chest compressions. When an unexpected child death is reported or a child arrives dead, five things happen in parallel, and the team leader should voice each.[2][3]
First, confirm identity and confirm death by the clinical signs above, and document the time. Second, preserve the scene and any clothing and bedding — nothing that was with the infant should be discarded or cleaned. Third, do not certify the death; notify the coroner (or in ANZ, the police who notify the coroner), because an unexpected death is reportable by law.[2][3]
Fourth, involve the SUDI or bereavement team and the designated paediatrician early, so that the joint home visit, family support and post-mortem can be arranged as a single coordinated response rather than a series of ad-hoc calls. Fifth, support the staff: child deaths are traumatic for the team, and a hot debrief immediately afterwards and a formal cold debrief within days are part of safe practice.[7][8]
Breaking bad news is a clinical skill with a structure, and the structure protects both the family and the clinician. The SPIKES protocol — Setting (private, seated, time), Perception (what do they already know), Invitation (how much do they want to hear), Knowledge (a clear warning shot, then the news in plain words), Emotions (allow and acknowledge the reaction), and Strategy/Summary (the next steps) — was built for cancer disclosure and adapts cleanly to the death of a child.[12]
Two phrases make the disclosure land. Give a warning shot ("I am afraid I have very serious news"), then deliver the news in short, unambiguous words ("Your child has died"), and then stop and allow silence. Do not pad the sentence with technical detail, do not soften the word "died" into "passed away" or "lost", and do not flee the room when the reaction comes. Parents repeatedly say that honest, clear words delivered with presence are what they remember and value.[7][12]
If the death followed an attempted resuscitation, the resuscitation documentation — drugs, doses, timings, rhythm checks, who was present, and the decision to cease — must be complete and legible, because it forms part of the coronial record and the child death review.[3]
Management — Definitive & Stepwise
Once the immediate response is running, the definitive pathway is the package that carries the family through the months ahead. It has six linked elements, each with an owner and a timeframe.[2][7]
Family time and memory-making come before almost anything else, because the window is short and cannot be reopened. Offer the family unhurried time to hold, bathe, dress and be with their child, and offer memory-making: handprints and footprints, a lock of hair, photographs, named clothing and a keepsake box. The scoping review by Thornton and colleagues found that parents who made and kept these mementoes had better bereavement outcomes and a lasting sense of parenthood.[10]
Do not let fear of the investigation steal this from the family. After the brief evidence-preservation steps, time with the child is almost always possible, and the SUDI team will support it. The one injunction is not to remove medical lines or alter the body before the forensic requirements are met.[3][10]
The multi-agency SUDI response is the investigative core. A designated paediatrician and a police officer conduct a joint home visit, usually within 24 to 48 hours, to review the scene, take the structured history, examine the family's account of the sleep environment, and refer for post-mortem. This joint model exists precisely so that safeguarding and clinical care run together rather than in suspicion of each other.[2][4]
Safe sleep ABC plus three
The safe-sleep counselling message for the next baby, and for every family you see in clinic, is the AAP 2022 bundle reduced to its operational core. Babies sleep Alone, on the Back, in a clear Cot; they room-share without bed-sharing for at least six months; the household is smoke-free; overheating is avoided; and a pacifier is offered. Bed-sharing is particularly dangerous when the parent smokes, is impaired by alcohol or drugs, on a soft surface, or with a normal infant under four months or any premature or low-birth-weight infant.[1][6]
Lower-risk bed-sharing
- Breastfeeding mother, non-smoker, sober
- Firm mattress on the floor, no gaps
- No pillows, doonas or soft bedding near the infant
- Still not recommended by AAP 2022; discuss harm reduction if bed-sharing is inevitable
High-risk bed-sharing (AVOID)
- Mother or partner is a smoker
- Impaired by alcohol, sedatives, marijuana or opioids
- Sofa, armchair, waterbed or soft surface
- Pillows, doonas or bumpers around the infant
- Term, normal-weight infant under 4 months
- Any premature or low-birth-weight infant
Bereavement follow-up is scheduled, not left to chance. An early contact within days checks practical needs; a face-to-face review at 2 to 4 weeks shares preliminary findings and opens the bereavement conversation; and a meeting at 3 to 6 months delivers the final post-mortem and coronial results and reviews ongoing support needs. October and colleagues, and Gijzen and colleagues, found that what parents value most is continuity — the same trusted clinician across these contacts — and honest communication that acknowledges their child's life and death.[7][8]
When you share the cause, be honest and never blame. If the death was SIDS, explain that it is unexplained despite complete investigation, and that the safe-sleep measures reduce but do not abolish risk. If a cause was found, name it and explain the implications for siblings and future pregnancies. If safeguarding was involved, the communication is led by the safeguarding and police partners within the agreed plan.[7][9]
Sibling support rests on three things: an honest, age-appropriate explanation of the death, explicit reassurance that they are not responsible (children often feel their thoughts or behaviour caused it), and the maintenance of routine. Specialist child bereavement services — in ANZ, services such as those linked through children's hospitals and SIDS organisations; in the UK, child bereavement charities — should be signposted at the first follow-up, not reserved for crisis.[8]
A key worker, often the designated paediatrician or a bereavement nurse specialist, coordinates the handoffs between hospital, coroner, primary care, bereavement services and the family. The single most common failure of bereavement care is the family being passed between agencies with no one owning them; the key worker exists to prevent that.[7][9]
Specific Subtypes & Scenarios
The expected death on a palliative pathway is the cleanest variant and the one most often mishandled by being over-medicalised. An advance care plan should already state the family's wishes for place of death, symptom management and what happens afterwards. The doctor may certify the cause, the family have time and memory-making as for any death, and the coroner is involved only if a specific criterion is met.[7]
The death of a child with a complex chronic or technology-dependent condition blurs the line. The family may expect the death, but if it was sudden, occurred during a procedure, or had any safeguarding element, it is treated as unexpected and referred. When in doubt, refer and let the coroner decide.[3]
A death during a resuscitation attempt in the emergency department or PICU adds the question of family presence. Current practice supports offering parents the choice to be present during resuscitation with a trained support person, because it aids bereavement; it is an offer, never an expectation. The resuscitation record feeds the coronial file, and a hot debrief supports the team.[7]
A neonatal or perinatal death overlaps with maternity bereavement care. Memory-making is central here too — the Thornton scoping review was conducted in this population — and the same honest communication and follow-up principles apply, with attention to postmortem consent and the option of investigation for inherited and placental causes.[10]
When safeguarding or non-accidental injury is suspected, the response becomes police-led within the multi-agency framework. A strategy meeting is convened, evidence is preserved, and communication with the family is carefully planned and legally constrained. The clinical team supports the child's siblings and other children in the household under the safeguarding plan.[3][4]
After an adolescent sudden death, the differential broadens to sudden cardiac death, SUDEP, suicide, overdose and asthma, and the response must include cardiac and genetic screening of first-degree relatives when the death is unexplained. The bereavement needs of adolescent peers and siblings are substantial and often overlooked.[11]
Complications & Pitfalls
Most failures in care after death are failures of process or communication, not of knowledge, and they cluster into recognisable patterns. The certification errors are the most legally serious: certifying an unexpected death, writing an unacceptable or vague cause, or failing to refer to the coroner. The rule is simple — if the death is unexpected, refer and do not certify.[2][3]
The diagnostic pitfall is the premature assumption of SIDS. Labelling a death SIDS at the scene masks non-accidental injury, hides inherited cardiac and metabolic disease, and denies the family an accurate answer and cascade testing. SIDS is a diagnosis of exclusion reached only after the complete investigation.[3][4]
The communication pitfalls are the ones families remember: medical jargon, false reassurance, a tone that blames the parents (especially mothers) for the sleep setting, and withholding or rushing time with the child. None of these is kind, and all of them worsen bereavement outcomes.[7][8]
Some parents develop prolonged grief disorder (also called complicated grief), defined by grief that remains intense and disabling, with persistent preoccupation with the deceased, avoidance, or a sense of meaninglessness, beyond about 6 to 12 months and causing functional impairment. These families need specialist mental-health referral; they are not "grieving normally", and the signal to act on is functional impairment, not the passage of time alone.[8]
The risks to siblings — guilt, anxiety, regression, and academic decline — are mitigated by honest explanation, reassurance, maintained routine, and early access to child bereavement services. Ask about siblings at every follow-up; they are the silent bereaved.[8]
Staff burnout and secondary traumatic stress are real after a child death, particularly after an unexpected or safeguarding death. The protections are a hot debrief, a formal cold debrief, peer support, access to employee assistance, and a culture that treats the team's welfare as part of the care, not an afterthought.[7]
Prognosis & Disposition
The death of a child changes the family permanently, and the long-term outcomes explain why follow-up is a clinical duty rather than a courtesy. Bereaved parents carry raised all-cause mortality, increased rates of depression, anxiety and post-traumatic stress, higher relationship breakdown, and reduced quality of life, effects that can persist for years and that structured bereavement support can moderate.[7][8]
The risk of recurrence in a subsequent pregnancy is a specific clinical question. For most SUDI, the recurrence risk is low and is reduced further by safe sleep and a smoke-free household. For the inherited causes — a channelopathy, a cardiomyopathy, or a metabolic disorder — the recurrence risk is genetic and cascade testing of the parents and siblings must happen before the next pregnancy, so the next infant can be managed proactively.[3][11]
The investigation timeline is something families should be warned about, because waiting is itself a source of suffering. Preliminary findings are usually available within weeks, but the final post-mortem, histology, metabolic, genetic and coronial findings can take several months. The 2- to 4-week and 3- to 6-month reviews are built around this timeline.[2][9]
When an inherited cause is identified, the communication has a preventive purpose: it allows cascade family testing (ECG and genetic testing for channelopathies; biochemical screening for metabolic disorders) before the next pregnancy, so that the next child can be diagnosed and managed early.[3][11]
The child death review is the disposition of last resort in the best sense. By aggregating de-identified data across deaths, the CDOP in the UK and equivalent committees in ANZ identify modifiable factors, service gaps and safeguarding themes, and turn individual tragedies into system change. Sanders and colleagues' review of CDOP working found that the process surfaces preventable deaths and drives local improvement, though it depends on complete data from every death.[9]
Ongoing care is handed over to primary care with a clear summary: the cause (or that it is unexplained), the follow-up plan, the bereavement services involved, and any outstanding results to be fed back. The key worker ensures the handover is real, not a letter that no one reads.[7][9]
Special Populations
Care after death is not culturally neutral, and treating it as if it were causes real harm. For Aboriginal and Torres Strait Islander, Maori and other indigenous families, the bereavement conversation, the role of extended family and community, the wishes around the body, and the memory-making practices may differ profoundly from a biomedical default. Culturally safe care — which may mean engaging an Aboriginal health worker or cultural support service, allowing time for family gathering, and respecting protocols around the deceased — is the standard, not an add-on.[2][6]
For migrant, refugee and asylum-seeking families, language barriers, religious requirements, an unfamiliar coronial system, and the absence of extended family all compound the bereavement. Professional interpreters (never family members), culturally and faith-appropriate space, and practical help with the things that follow a death are essential.[8]
The death of a child with a disability or neurodiversity affects a family who may have spent years as a complex-care team and who grieve both the child and the caring role. Communication must accommodate the child's and family's communication style, and sibling support must account for the often intense sibling relationships in these families.[7]
A death in out-of-home care, or where there are safeguarding or youth-justice concerns, carries the highest scrutiny. The multi-agency response runs in full, the child's legal guardians and birth family are engaged according to the care plan, and the coroner and child protection services are involved from the outset. The risk is that the system's focus on investigation crowds out the family's bereavement, which must still be supported.[3][9]
Socioeconomically disadvantaged families experience bereavement support differently: they may lack transport, stable housing, leave from work, or the funds for a funeral. Practical help — funeral assistance, transport to follow-up, flexibility about appointments — is often more valued than any words, and is part of equitable care.[8]
For an adolescent or young-adult death, memory-making and follow-up must be age-appropriate, the peer group becomes central to bereavement, and the screening of siblings and relatives for inherited causes (especially cardiac) is often the most important preventive action.[11]
Evidence, Guidelines & Regional Differences
The evidence base is a blend of consensus guidelines, observational epidemiology and qualitative parent research, and using each for what it can support keeps the content honest. The AAP 2022 safe-sleep recommendations (Moon and colleagues) are the operational standard for prevention, strengthened since 2016 on the firm flat non-inclined surface, the explicit advice against bed-sharing, room-sharing for at least six months, the avoidance of weighted bedding and of alcohol and illicit drugs, and supervised awake tummy time.[1]
The ANZ SUDI investigation framework (Jeffery and colleagues, and the state SUDI services) and the UK Kennedy and RCPCH multi-agency protocols align closely: both mandate a joint paediatrician-and-police home visit, a full scene review and history, a specialist post-mortem, and staged family feedback. The differences are administrative — who coordinates, the name of the review committee — rather than conceptual.[2][4]
The child death review evidence (Sanders and colleagues on the UK CDOP) shows that a systematic, anonymised review of every child death surfaces modifiable factors and drives prevention, but is only as good as the data fed into it. The UK operates a statutory CDOP for every child death; ANZ operates state-based child death review committees with a similar function.[9]
What bereaved parents value comes from qualitative research rather than trials, because a trial of bereavement support is ethically fraught. October and colleagues and Gijzen and colleagues converge on the same themes: honest, clear communication; the chance for continuing bonds through time with the child and memory-making; continuity with a trusted clinician; and practical support. Thornton and colleagues' scoping review confirms that memory-making after perinatal and newborn death is associated with better bereavement outcomes.[7][8][10]
Quinn and colleagues' five-year review of SUDIC in Greater Manchester quantifies the older-child problem and the proportion with cardiac, epilepsy and safeguarding causes, and Das and colleagues document, from a low-resource setting, how end-of-life communication and breaking bad news are experienced by both parents and providers — a reminder that the principles travel, even when resources do not.[11][12]
The controversies are real and must be communicated without shaming. Bed-sharing, swaddling and pacifier use all have cultural and practical weight, and a blanket prohibition that parents cannot follow is worse than honest harm-reduction. The AAP 2022 position is to avoid bed-sharing; the clinician's task in ANZ and the UK is to make that recommendation clearly, identify the high-risk bed-sharing situations that carry the steepest risk, and offer a non-judgmental plan that families can actually follow.[1][6]
Exam Pearls
References
- [1]Moon RY, Carlin RF, Hand I, et al. Sleep-Related Infant Deaths: Updated 2022 Recommendations for Reducing Infant Deaths in the Sleep Environment. Pediatrics, 2022.PMID 35726558
- [2]Jeffery HE, Carberry AE, Gordon A, et al. The investigation of sudden unexpected deaths in infancy in Australia. Med J Aust, 2023.PMID 36653164
- [3]Fitzgerald DA, Jeffery H, Arbuckle S, et al. Sudden Unexpected Death in Infancy [SUDI]: What the clinician, pathologist, coroner and researchers want to know. Paediatr Respir Rev, 2022.PMID 34998675
- [4]Garstang J, Ellis C, Sidebotham P. An evidence-based guide to the investigation of sudden unexpected death in infancy. Forensic Sci Med Pathol, 2015.PMID 25999133
- [5]Spinelli J, Collins-Praino L, Van Den Heuvel C, et al. Evolution and significance of the triple risk model in sudden infant death syndrome. J Paediatr Child Health, 2017.PMID 28028890
- [6]Jullien S. Sudden infant death syndrome prevention. BMC Pediatr, 2021.PMID 34496779
- [7]October T, Dryden-Palmer K, Copnell B, et al. Caring for Parents After the Death of a Child. Pediatr Crit Care Med, 2018.PMID 30080812
- [8]Gijzen S, L'Hoir MP, Boere-Boonekamp MM, et al. How do parents experience support after the death of their child? BMC Pediatr, 2016.PMID 27927172
- [9]Sanders C, Fisher-Smith D, Neill S, et al. Lessons for the future: Reflections on a review of child death overview panels through a local lens in the United Kingdom. J Child Health Care, 2020.PMID 31067977
- [10]Thornton R, Nicholson P, Harms L. Scoping Review of Memory Making in Bereavement Care for Parents After the Death of a Newborn. J Obstet Gynecol Neonatal Nurs, 2019.PMID 30946804
- [11]Quinn S, Dierckx E, Long T, et al. Sudden Unexpected Death in Childhood in Greater Manchester (United Kingdom): A Five-Year Review (2015-2020). Compr Child Adolesc Nurs, 2022.PMID 36440870
- [12]Das MK, Arora NK, Chellani HK, et al. Perceptions of the parents of deceased children and of healthcare providers about end-of-life communication and breaking bad news at a tertiary care public hospital in India: a qualitative exploratory study. PLoS One, 2021.PMID 33735296