Paeds · fetal-neonatal-and-perinatal
Antenatally detected kidney and urinary-tract anomalies: newborn management
Also known as Antenatal hydronephrosis · Congenital anomalies of the kidney and urinary tract (CAKUT) · Fetal renal pelvic dilatation · Prenatally detected urinary tract dilation · Posterior urethral valves newborn management · Multicystic dysplastic kidney · Vesicoureteric reflux presenting in the newborn · Congenital solitary kidney
Fellowship guide to the newborn with an antenatally detected kidney or urinary-tract anomaly. Covers the CAKUT spectrum, antenatal hydronephrosis risk-stratification by anteroposterior pelvic diameter, the timing and interpretation of postnatal ultrasound, posterior urethral valves, vesicoureteric reflux, ureteropelvic junction obstruction, multicystic dysplastic kidney, duplex systems and ureteroceles, the role of prophylactic antibiotics, when to image with VCUG or renography, and long-term renal surveillance with regional guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Most renal and urinary-tract anomalies are now detected before birth, and the finding lands on the paediatrician as a prenatal ultrasound report rather than a sick newborn. The umbrella term is congenital anomalies of the kidney and urinary tract, or CAKUT, a family of structural disorders that share a common thread: they threaten nephron mass, either by obstructing urine flow, allowing urine to reflux back into the kidney, or replacing functioning tissue with cysts and dysplasia. [1] [2]
The most common presentation is antenatal hydronephrosis — dilatation of the renal pelvis and collecting system seen on the mid-trimester or third-trimester scan. The question the paediatrician must answer is not "is there a problem" but "how big is the risk, and what do I do about it in the first weeks of life." Most antenatal hydronephrosis resolves or is physiologic, but a minority signals obstruction, reflux or dysplasia that will damage the kidney if left alone. [3] [4]
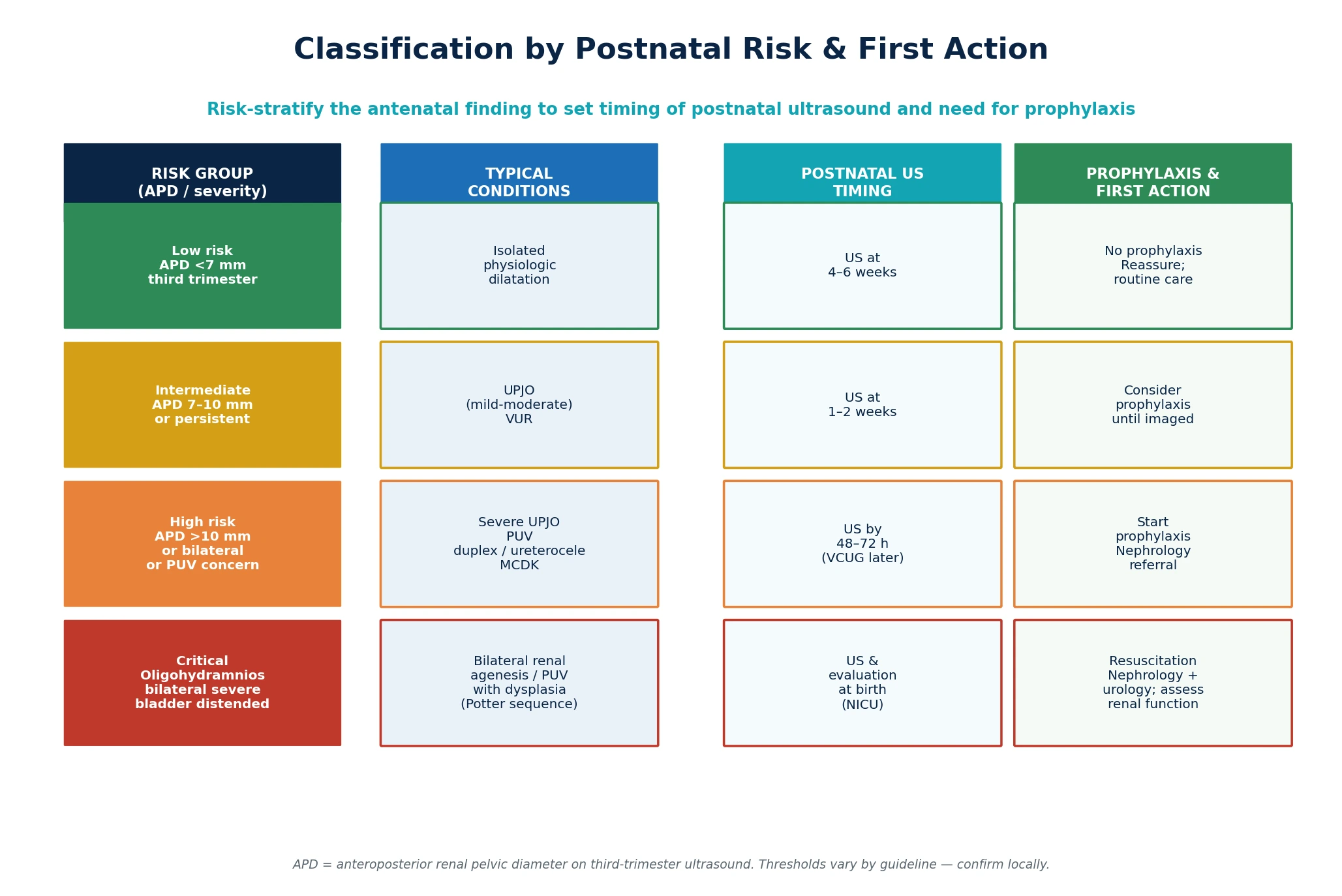
The organising principle is therefore risk stratification. You use the severity of the antenatal dilatation (measured as the anteroposterior pelvic diameter, or APD), whether it is unilateral or bilateral, the appearance of the bladder, and the amniotic fluid volume to sort each infant into a low, intermediate, high or critical risk band. That band then dictates when you scan after birth, whether you start a prophylactic antibiotic, and how quickly you involve paediatric nephrology and urology. [3]
Classification
CAKUT is best understood through two lenses: the anatomical lesion and the postnatal risk band. The anatomical lens names the structural defect — obstruction at the pelviureteric or ureterovesical junction, a posterior urethral valve, reflux up the ureter, a cystic dysplastic kidney, or a duplex system with an ectopic ureter. The risk-band lens, which is the one that drives your newborn actions, sorts infants by the likelihood that the finding will harm the kidney. [1] [3]
[1] [3] [4]The postnatal risk band is set largely by the third-trimester APD, the standardised measurement of the renal pelvis in the anteroposterior plane. An APD below 7 mm in the third trimester is low risk, 7 to 10 mm is intermediate, and above 10 mm, or any bilateral dilatation with bladder abnormality, places the infant in the high-risk band. Bilateral severe disease with oligohydramnios is the critical band, because the lack of fetal urine threatens lung growth as well as renal function. These thresholds vary slightly between guidelines — confirm the cut-offs used by your local network. [3] [11]
By the numbers
Epidemiology & Risk Factors
Antenatal hydronephrosis is the most common fetal anomaly detected on routine ultrasound, found in roughly 1 to 2 percent of pregnancies. The apparent rise in incidence over recent decades reflects better transducers and earlier, more systematic scanning rather than a true increase in disease. About half of these findings are transient dilatation that resolves without consequence, while roughly 10 to 15 percent conceal obstruction, reflux or dysplasia that requires postnatal investigation or intervention. [3] [4]
The lesions that matter most for long-term renal prognosis cluster in boys with obstruction and in infants with bilateral disease. Posterior urethral valves occur only in males, with an incidence of roughly 1 in 4000 to 8000 live births, and they remain the most common cause of end-stage renal disease of urological origin in children. Vesicoureteric reflux is more common in girls after infancy but frequently presents in the newborn period when associated with an antenatal finding. [7] [14]
Several factors raise the risk that an antenatal finding is significant rather than physiologic. A family history of CAKUT, parental consanguinity, a known syndromic or chromosomal diagnosis, and concurrent anomalies on the anomaly scan all increase the likelihood of true structural disease. Severe early-onset dilatation, bilateral involvement, a thick-walled or enlarged bladder, echogenic kidneys, and oligohydramnios are the prenatal markers that push an infant from low to high risk. [2] [13]
Access to antenatal care and to postnatal imaging shapes outcomes as much as biology. An infant born in a centre without timely ultrasound, prophylactic antibiotics or paediatric nephrology may lose the window in which obstruction is relieved before permanent damage accrues. Rural and remote families, and those with barriers to transport and follow-up, carry a disproportionate risk of late presentation with infection or renal impairment, which makes the discharge safety-net and a clear surveillance pathway part of the treatment. [4] [10]
Pathophysiology
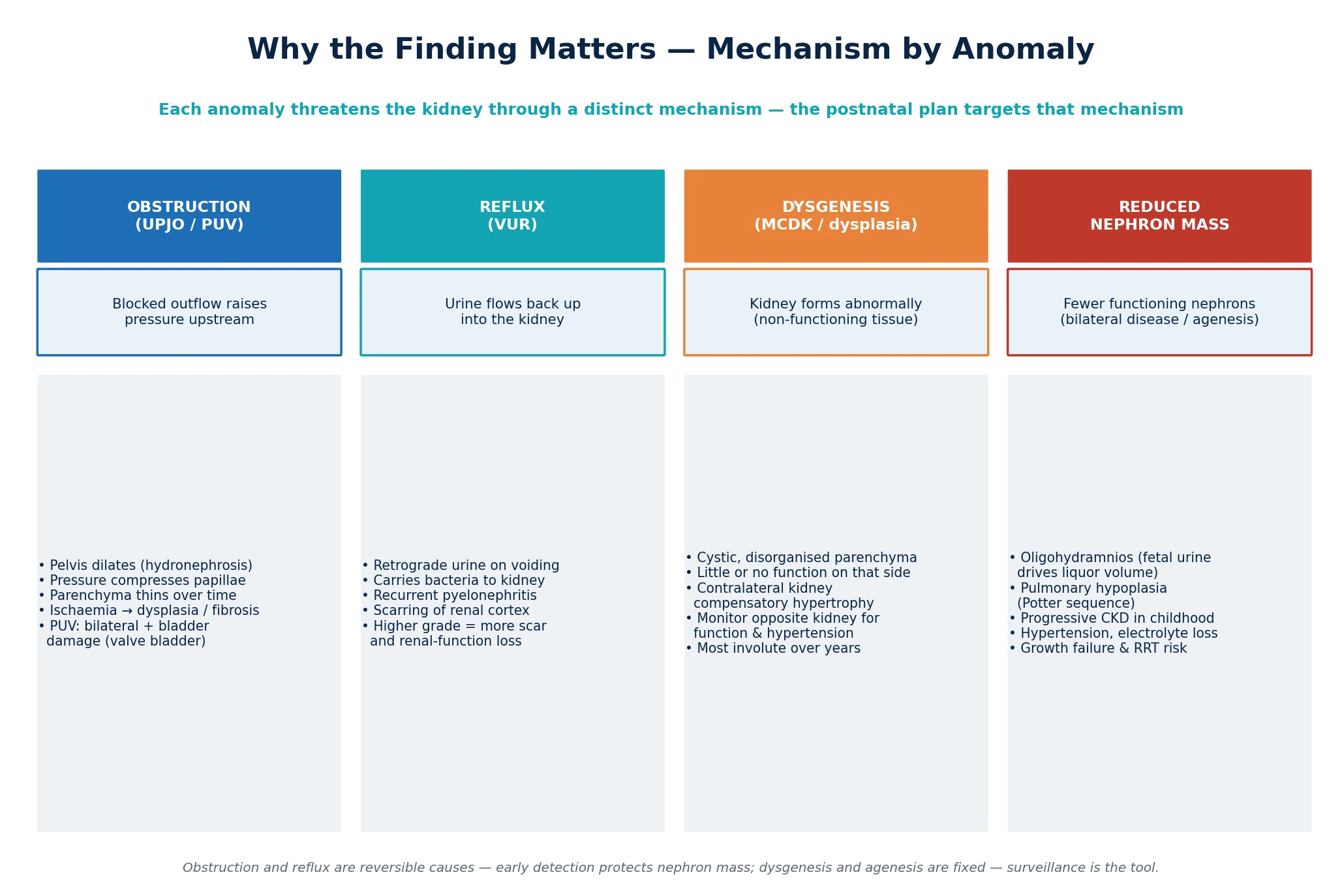
Each CAKUT lesion threatens the kidney through a distinct mechanism, and the postnatal plan targets that mechanism directly. Understanding the mechanism explains why a mild dilatation can be watched while a bilateral one cannot, and why reflux scars the kidney even when the ureter looks unremarkable. [1] [2]
Obstruction is a pressure problem. When urine cannot leave the kidney freely — whether at a stenotic pelviureteric junction in UPJO, or at a posterior urethral valve — the collecting system dilates and the rising pressure is transmitted back into the renal parenchyma. Over weeks and months that pressure compresses the renal papillae, thins the cortex, and produces ischaemia that ends in dysplasia and fibrosis. In posterior urethral valves the obstruction sits below the bladder, so the bladder wall thickens and dilates both upper tracts, damaging two kidneys and the bladder itself (the "valve bladder"). [7] [14]
Reflux is an infection-and-pressure problem. In vesicoureteric reflux the ureterovesical junction fails as a one-way valve, so urine travels back up into the kidney during voiding. That retrograde urine can carry bacteria from the bladder to the renal parenchyma, converting a simple cystitis into pyelonephritis, and recurrent pyelonephritis scars the cortex irreversibly. Higher reflux grades (the reflux reaches the kidney with ureteric and collecting-system dilatation) carry the greatest scarring and renal-function risk. [5] [6]
Dysgenesis is a fixed developmental problem. A multicystic dysplastic kidney never formed properly: its tissue is a collection of non-communicating cysts with little or no functioning parenchyma, and it contributes negligibly to total renal function. The danger is not the affected kidney but the contralateral one, which must hypertrophy to compensate and which itself may carry reflux or obstruction that places the child's entire renal reserve at risk. [9] [10]
When disease is bilateral and severe, the fetus loses the very thing that drives amniotic fluid volume — urine. Oligohydramnios removes the fluid cushion that splints the lungs and shapes the face, producing the Potter sequence: pulmonary hypoplasia, limb deformities and the characteristic facies. It is the lung hypoplasia, as much as the renal failure, that threatens life in the delivery room. [13]
Clinical Presentation
An antenatally detected renal anomaly almost never presents as a symptom in the newborn — it presents as a handover. The obstetric or fetal-medicine team flags the finding, and the paediatrician receives a referral, a multidisciplinary note, or an entry in the maternal record. The newborn is usually well, pink and feeding, which is precisely why the finding can be forgotten if it is not written into a postnatal plan. [3] [4]
A minority of infants present with signs rather than a scan result. A palpable abdominal mass in a newborn may be a hydronephrotic kidney, a distended bladder from posterior urethral valves, or a multicystic dysplastic kidney. A male infant with a weak urinary stream, a palpable bladder, or respiratory distress from pulmonary hypoplasia should raise PUV immediately. Poor weight gain, vomiting, or electrolyte disturbance in the first weeks can be the first clue to renal dysplasia or obstruction. [7] [14]
The first febrile illness is a sentinel event. A urinary tract infection in an infant with known antenatal hydronephrosis is not simple cystitis — it is evidence that the tract may be obstructed or refluxing, and it should trigger a review of the postnatal imaging plan rather than antibiotic treatment alone. Missing this link is one of the commonest ways an antenatal finding translates into late renal scarring. [5] [6]
Differential Diagnosis
For an antenatal renal-tract finding, the differential is really a question of which CAKUT lesion it represents, and whether it is isolated or part of a syndrome. The first branch is between physiologic dilatation, which needs no treatment, and pathologic dilatation, which does. The APD, the presence of ureteric dilation, the bladder, and the parenchymal echogenicity separate them. [3] [11]
For a unilateral pelviectasis with a normal-calibre ureter, the differential is ureteropelvic junction obstruction versus physiologic dilatation; a normal ureter excludes vesicoureteric reflux and megaureter as primary causes, though reflux can coexist. If the ureter itself is dilated, the differential widens to include vesicoureteric reflux, megaureter (obstructed or non-obstructed), and an ectopic ureter from a duplex system. [3] [12]
For a cystic-appearing kidney, the differential is multicystic dysplastic kidney versus hydronephrosis, and the distinction matters. MCDK shows cysts of varying sizes that do not communicate, with no identifiable renal sinus, whereas hydronephrosis shows a central dilated pelvis communicating with the dilated calyces. An echogenic, enlarged kidney raises dysplasia, polycystic disease, or storage disorder. A duplex system may show a dilated upper moiety (often from an ectopic ureter or ureterocele) and is easily missed if the upper pole is not deliberately examined. [9] [12]
When the anomaly is bilateral or associated with other structural findings, ask whether it is part of a syndrome or chromosomal condition. CAKUT is a feature of many syndromes (for example, syndromes with chromosomal anomalies, ciliopathies, and Townes-Brocks or branchio-oto-renal spectrum), and the renal finding may be the entry point to a wider genetic work-up. A normal karyotype does not exclude a single-gene cause, and referral to clinical genetics is warranted when the lesion is bilateral, syndromic, or familial. [1] [2]
Clinical & Bedside Assessment
The bedside assessment begins before the baby is born. Review the antenatal records for the APD measurement, the gestation at which dilatation was first seen, its progression on serial scans, the laterality, the bladder appearance, the amniotic fluid volume, and any associated anomalies. Note the family history of renal disease, consanguinity, and any genetic results. This review sets the risk band and decides what happens in the first days of life. [3] [4]
Examine the newborn with the finding in mind. Palpate the abdomen for a renal mass (hydronephrosis, MCDK) or a distended bladder (PUV), observe the urinary stream in a male infant, and assess perfusion and hydration. Inspect for dysmorphic features, limb or ear anomalies, and anorectal malformations that suggest a syndromic association. Measure blood pressure, though hypertension in the newborn period is uncommon except with severe dysplasia or renal vein thrombosis. [9] [10]
The examination alone never confirms or excludes the diagnosis — that needs postnatal ultrasound — but it identifies the infant who needs urgent imaging rather than a delayed scan. A well, feeding newborn with isolated mild unilateral dilatation and a normal examination can follow the routine pathway. A male infant with a distended bladder or palpable kidneys needs same-day ultrasound, prophylaxis and urgent urology input. [7] [14]
Counsel the family at the bedside using plain language and teach-back. Explain that the antenatal finding is common, that most are harmless, but that a small number need watching and a smaller number need treatment. Name the follow-up plan, the timing of the scan, the reason for prophylactic antibiotics if prescribed, and the safety-net for fever. A family that understands why the scan is delayed (to avoid a falsely reassuring early result) is far more likely to return for it. [3] [4]
The newborn assessment at a glance
Investigations
Postnatal renal ultrasound is the cornerstone investigation, and timing it correctly is the single most important decision the paediatrician makes. An ultrasound done in the first 48 hours can underestimate dilatation because the neonate is relatively dehydrated and the glomerular filtration rate is low, so a normal early scan does not reliably exclude obstruction. For low-risk infants, defer the scan to four to six weeks; for intermediate risk, scan at one to two weeks; for high-risk infants, scan by 48 to 72 hours. [3] [4]
The postnatal ultrasound reports the same APD measurement used antenatally, plus the calyceal and parenchymal pattern, ureteric dilation, bladder wall thickness, and post-void residual. Severity is often graded on the Society for Fetal Urology scale, which combines pelvic dilatation with peripheral calyceal dilation and parenchymal thickness to grade hydronephrosis from 0 to 4. A high grade or worsening dilatation on serial scans is the trigger for further functional imaging. [11]
A voiding cystourethrogram (VCUG) is not needed for every infant with antenatal hydronephrosis. Reserve it for those with high-grade or worsening dilatation, a dilated ureter, a thick-walled or abnormal bladder (to look for PUV in a male), recurrent urinary tract infection, or a duplex system. In a male with suspected PUV, the VCUG shows the dilated posterior urethra and the obstructing valve, and it is diagnostic. Because the VCUG involves catheterisation and radiation, the decision should sit with the nephrology or urology team. [3] [12]
Functional renography (mercaptoacetyltriglycine, MAG3, or dimercaptosuccinic acid, DMSA) measures how well each kidney works and whether obstruction is present. MAG3 with diuretic challenge is the test of choice for suspected UPJO, showing differential renal function and the washout curve that separates obstructive from non-obstructive dilatation. DMSA maps cortical scarring and is used after a febrile UTI or to confirm a non-functioning MCDK. These tests guide the decision to operate. [3] [9]
Baseline blood and urine tests complete the work-up for significant disease. A serum creatinine and electrolytes (later converted to an estimated GFR as the child grows), a blood pressure, and a urinalysis or urine culture establish the renal functional baseline. In bilateral disease or suspected dysplasia, these baselines are essential because they track the trajectory toward chronic kidney disease over the years that follow. [1] [10]
What the postnatal imaging chooses between
Management — Resuscitation
Most antenatally detected renal anomalies need no resuscitation at all — the newborn transitions normally, and the resuscitation is really a planning action. The exception is the critical band: the infant with bilateral severe disease and oligohydramnios who may be born with pulmonary hypoplasia and respiratory failure from the Potter sequence. These infants need a delivery-room team prepared for neonatal respiratory support, and the plan must be made antenatally with neonatology present. [13]
For the high-risk infant who is stable at birth, the "resuscitation" is the protective bundle you start while awaiting the formal ultrasound and specialist review. Start a prophylactic antibiotic (trimethoprim is the usual first choice for neonatal urinary-tract prophylaxis; confirm the exact agent and dose against your local guideline) to cover the period before obstruction or reflux is excluded. [3] [6]
Maintain hydration and perfusion, because a dehydrated infant produces less urine and the collecting system under-fills, both worsening the clinical picture and degrading the ultrasound. In posterior urethral valves, insert a urethral catheter to decompress the bladder if the infant is in retention, and arrange urgent urology review for cystoscopic valve ablation. Send baseline creatinine and electrolytes. [7] [14]
Do not over-treat. Most infants with antenatal hydronephrosis are well, and the temptation to start broad investigations, intravenous fluids or repeated imaging in a stable baby creates harm through false-positive results, line infections and family anxiety. The discipline of the resuscitation phase is to do the protective minimum — prophylaxis, hydration, baseline bloods, a timed ultrasound — and to escalate only the infants whose risk band or examination demands it. [3] [4]
Trimethoprim (prophylactic)
Dose
2 mg/kg once daily (neonatal prophylactic dosing — confirm exact agent, dose and route against your local protocol and formulary)
Management — Definitive & Stepwise
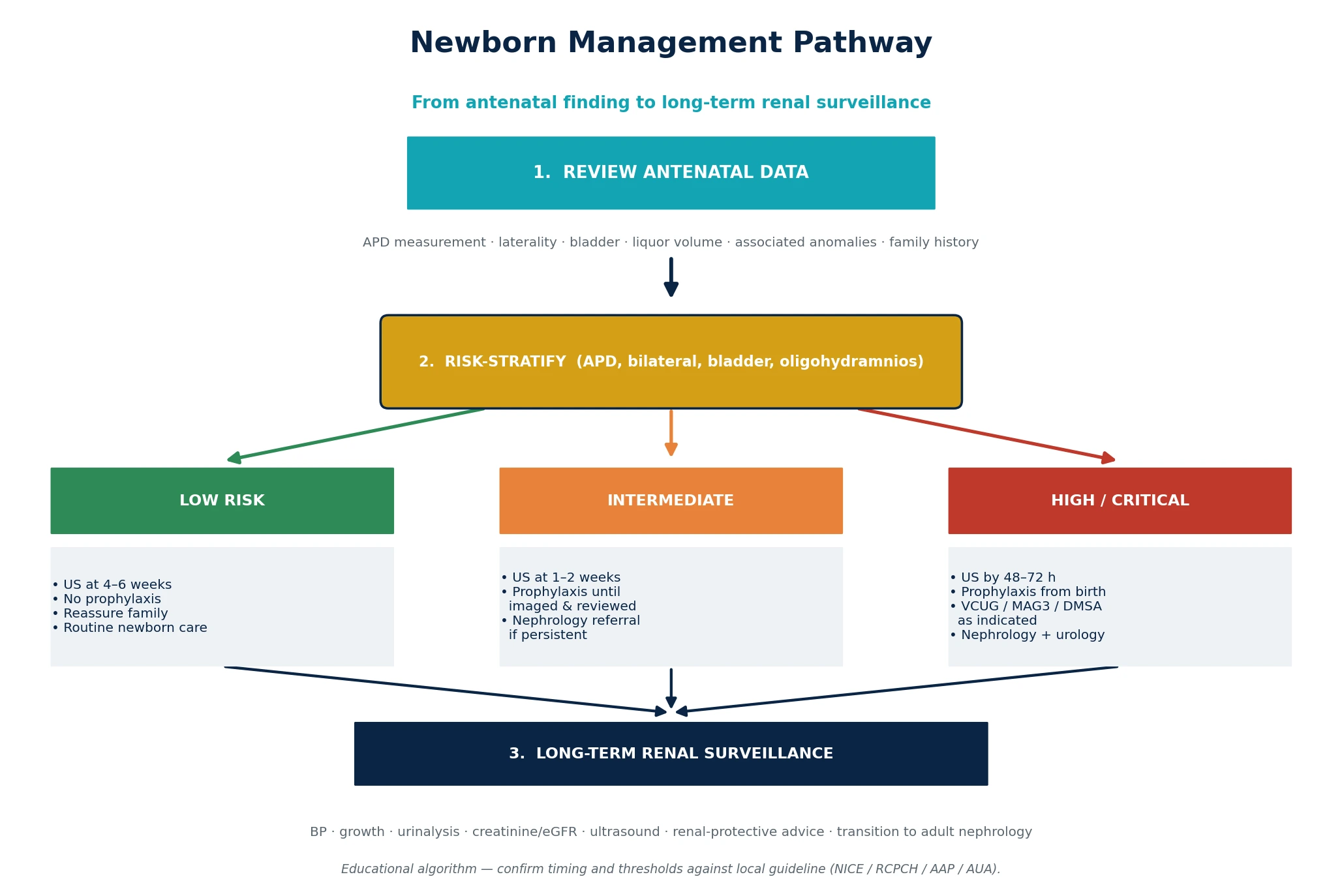
The definitive pathway runs from the risk band, through the timed ultrasound, to a decision about functional imaging, specialist referral and long-term surveillance. Each step is driven by the severity of the finding and its behaviour on serial imaging, not by a fixed protocol applied to every infant. [3] [4]
For low-risk infants (isolated, mild, unilateral dilatation with a normal bladder and liquor), the pathway is expectant. Book a postnatal ultrasound at four to six weeks, give no prophylaxis, reassure the family, and arrange routine follow-up. If the scan is normal or shows resolved dilatation, no further action is needed. If it shows persistent or worsening dilatation, the infant moves into the intermediate pathway. [3] [11]
For intermediate-risk infants, scan at one to two weeks and consider prophylactic antibiotics until the scan result is reviewed. Persistent moderate dilatation triggers referral to paediatric nephrology or urology, functional imaging with MAG3 if UPJO is suspected, and a VCUG if ureteric dilation or reflux is a concern. The decision to operate on a UPJO rests on worsening dilatation, falling differential function, or a poor washout curve on MAG3 — not on a single dilatation measurement. [3] [9]
For high-risk infants, the pathway accelerates. Ultrasound by 48 to 72 hours, prophylactic antibiotics from birth, and early nephrology and urology referral are the default. A male with bilateral hydronephrosis and a thick-walled bladder needs a VCUG to confirm or exclude PUV; if valves are confirmed, cystoscopic ablation is performed, and the child enters long-term follow-up for bladder and renal function. A duplex system with an upper-moiety ureterocele needs surgical planning tailored to the anatomy and the function of the affected moiety. [7] [12]
For the critical infant with bilateral severe disease and oligohydramnios, management is neonatal intensive care: respiratory support for pulmonary hypoplasia, renal-function support, electrolyte management, and early discussion with nephrology about the trajectory toward chronic kidney disease and renal replacement therapy. These infants represent the severe end of the spectrum where the antenatal plan — delivery at a tertiary centre with neonatology and nephrology — determines survival. [13]
The stepwise newborn plan
1 · Review antenatal data
APD, laterality, bladder, liquor, associated anomalies, family history. Set the risk band.
2 · Examine the newborn
Palpate for mass or bladder, observe the stream, assess for syndromic features, measure blood pressure.
3 · Time the ultrasound
Low risk at 4–6 weeks, intermediate at 1–2 weeks, high risk by 48–72 hours. Avoid scanning in the first 48 hours unless critical.
4 · Protect with prophylaxis
Start a prophylactic antibiotic for high-risk infants pending imaging and specialist review.
5 · Functional imaging & referral
MAG3 for suspected obstruction, VCUG for reflux or PUV, DMSA for scarring. Refer to nephrology or urology as indicated.
6 · Long-term surveillance
Blood pressure, growth, urinalysis, creatinine and eGFR, serial ultrasound. Give every family a fever safety-net.
Specific Subtypes & Scenarios
[7] [14]Vesicoureteric reflux is graded I to V by the degree of ureteric and collecting-system dilatation on VCUG. Low-grade reflux often resolves spontaneously, but higher grades carry a significant risk of recurrent pyelonephritis and renal scarring. The RIVUR trial established that antimicrobial prophylaxis reduces recurrent UTI in children with reflux, with the greatest benefit in those who have already had a febrile infection, and it remains the evidence base for using prophylaxis in infants with high-grade reflux or an antenatal finding pending imaging. [5] [6]
A multicystic dysplastic kidney is non-functioning and is managed conservatively in most cases — the lesion involutes over months to years and the affected kidney contributes little to total function. The clinical focus is the contralateral kidney, which must be assessed for reflux or obstruction and surveilled for compensatory hypertrophy, hypertension and function. Nephrectomy is reserved for the minority that grow, cause mass effects, or are associated with hypertension. The principles of managing a congenital solitary kidney — blood pressure monitoring, renal-function surveillance, renal-protective advice, and sports-participation counselling — apply to the child with an involuted MCDK as much as to one born with a single kidney. [9] [10]
Duplex systems and ureteroceles demand careful anatomical characterisation because each moiety behaves independently. An ectopic ureter draining an upper moiety may cause obstruction or continuous dribbling incontinence in girls; a ureterocele prolapsing into the bladder outlet may cause obstruction. Management ranges from endoscopic incision of an obstructing ureterocele to partial nephroureterectomy of a non-functioning moiety, individualised to the anatomy and the function shown on DMSA and MRI urography. [12]
In fetal lower urinary tract obstruction, the PLUTO trial examined whether antenatal vesicoamniotic shunting improved survival compared with conservative management. The trial found a trend toward improved survival that did not reach statistical significance, and it highlighted the uncertainty around selecting fetuses most likely to benefit. The paediatrician's role is to be aware that some of these infants will have had an antenatal intervention and to plan the postnatal urological management accordingly. [8]
Complications & Pitfalls
The complications fall into two time frames. In the newborn period, the risks are infection (a UTI in an obstructed or refluxing system), dehydration worsening the ultrasound picture, and — in the critical infant — respiratory failure from pulmonary hypoplasia. Over the longer term, the risks are progressive renal scarring, hypertension, growth failure, and progression to chronic kidney disease or end-stage renal disease, particularly in PUV and bilateral dysplasia. [5] [7]
Several pitfalls recur in practice. The first is the falsely reassuring early ultrasound — a scan done in the first 48 hours can look deceptively normal because the dehydrated neonate under-fills the collecting system, and the family is discharged with false reassurance and no follow-up. The second is the lost safety-net — the family returns to a local hospital with a fever, the UTI is treated as simple cystitis, and the underlying obstruction or reflux is not reconsidered until scarring has occurred. [3] [6]
The third pitfall is treating a single-kidney problem as isolated. A multicystic dysplastic kidney or a unilateral severe UPJO is only half the story if the contralateral kidney carries reflux or obstruction, and failing to image both kidneys and the bladder function leaves the child's entire renal reserve unprotected. The fourth is the opposite error — over-investigating a low-risk infant with a VCUG, repeated ultrasounds and unnecessary prophylaxis, generating false positives, radiation exposure, line infections and family anxiety without changing the outcome. [3] [10]
Prognosis & Disposition
Prognosis tracks the risk band and the underlying lesion. Low-risk, isolated, unilateral dilatation carries an excellent prognosis — most resolve, renal function is normal, and the child needs only routine care. Intermediate-risk infants with mild UPJO or low-grade reflux also do well, though a minority progress and need intervention. The prognosis darkens sharply with bilateral disease, PUV, and severe dysplasia, where a meaningful proportion of children progress to chronic kidney disease over childhood and adolescence. [1] [7]
Disposition depends on the risk band. Low-risk infants go home with a routine follow-up and a scan booked at four to six weeks. Intermediate-risk infants go home with prophylaxis, a scan at one to two weeks, and a clear review pathway. High-risk infants may need admission for urgent ultrasound, prophylaxis, catheterisation (in PUV) and specialist referral before discharge. The critical infant needs tertiary neonatal intensive care. [3] [4]
Long-term surveillance is the disposition for every infant with a confirmed CAKUT lesion, even after the acute management is complete. Blood pressure, growth, urinalysis, serum creatinine (tracked as eGFR), and serial ultrasound are the tools, and the interval is set by the lesion and its severity. The child with PUV or bilateral dysplasia enters lifelong nephrology follow-up with a plan for transition to adult renal care; the child with an involuted MCDK needs surveillance of the contralateral kidney into adolescence. [7] [10]
The disposition is not complete without a named owner and a written plan. An antenatal finding that lives only in one clinician's memory is an antenatal finding at risk of being lost between shifts, sites and clinicians. Write the ultrasound date, the prophylaxis, the safety-net, and the follow-up owner into the discharge record and the family's handheld record before the family leaves. [4]
Special Populations
Rural and remote families carry a disproportionate burden because the surveillance contract depends on access to ultrasound, prophylaxis and specialist review that may sit hours away. For these families, build the plan around what is locally available: a clear safety-net for fever, a telehealth link to nephrology or urology, a confirmed ultrasound date at the nearest capable service, and a retrieval plan if the infant becomes unwell. The plan is only useful if the family can execute it from where they live. [4] [10]
Indigenous children in Australia, New Zealand and other settler-colonial contexts face higher rates of post-infectious renal disease and poorer access to consistent surveillance, which compounds the risk of a CAKUT lesion. A culturally safe, family-centred surveillance pathway that names a local health worker or Aboriginal medical service as part of the team improves retention in follow-up and earlier detection of complications. [10]
Children with complex chronic conditions, syndromic CAKUT, or a single functioning kidney need integrated surveillance that spans nephrology, urology, genetics and developmental paediatrics. The single kidney (whether congenital or after MCDK involution) demands blood-pressure monitoring, renal-protective advice (hydration, avoidance of nephrotoxins, sports-participation counselling), and vigilance for hypertension and proteinuria across childhood. [9] [10]
Socioeconomic disadvantage changes the surveillance contract. Families with limited leave from work, transport barriers, or insecure housing may struggle to attend serial ultrasounds and clinic visits, and a plan that does not account for these realities will fail regardless of its clinical correctness. Practical support — scheduling scans with other appointments, confirming transport, using telehealth — is part of the treatment. [4]
Evidence, Guidelines & Regional Differences
The evidence base for managing antenatal hydronephrosis draws on observational cohorts for the natural history and risk thresholds, the RIVUR randomised trial for prophylaxis in reflux, the PLUTO trial for antenatal shunting in lower-tract obstruction, and large systematic reviews for long-term outcomes in PUV. A clinical predictive model of renal injury in isolated antenatal hydronephrosis has refined which infants are most likely to need intervention, supporting the move toward risk-stratified rather than blanket imaging. [5] [8] [11]
Guideline thresholds for the APD cut-offs, the timing of postnatal ultrasound, and the indications for VCUG differ modestly between regions. The American Academy of Pediatrics, the American Urological Association, NICE and RCPCH guidance, and the CPS and Perinatal Society recommendations each offer slightly different cut-offs and pathways, and the local perinatal network often sets the operative thresholds. The paediatrician's responsibility is to know the local pathway and to apply it consistently rather than to recall a single universal threshold. [3] [6]
A live controversy is the role of routine antimicrobial prophylaxis in infants with antenatal hydronephrosis pending the exclusion of reflux. The RIVUR trial supports prophylaxis in confirmed reflux, but its application to all infants with dilatation — many of whom have neither reflux nor obstruction — is debated, balancing the reduction in febrile UTI against the risk of antimicrobial resistance. Most pathways reserve prophylaxis for high-risk infants and discontinue it once normal imaging excludes reflux and obstruction. [5] [6]
The move toward conservative management of MCDK, the refinement of endoscopic and laparoscopic surgical options for UPJO and duplex systems, and the growing recognition of long-term renal risk even after successful valve ablation are the contemporary trends. The paediatrician's place in these debates is to hold the long view: the lesion is managed at one point in childhood, but the kidney is watched for a lifetime. [7] [9]
Exam Pearls
The exam rewards the candidate who can move fluently between the antenatal APD measurement and the postnatal risk band, name the lesion from the ultrasound pattern, and defend the timing of the postnatal scan. The single most common error is scanning too early and being falsely reassured — examiners will probe whether you know why the first 48 hours can mislead. The second is failing to protect the contralateral kidney in a unilateral lesion. [3] [11]
For the long case, structure your answer around the surveillance contract: review the antenatal data, state the risk band, justify the imaging timing, explain the role of prophylaxis, and describe the long-term renal surveillance and transition plan. For the short case, be ready to interpret a renal ultrasound and a VCUG, distinguish MCDK from hydronephrosis, and recognise PUV from the cystourethrogram. [7] [9]
References
- [1]Murugapoopathy V, Gupta IR. A Primer on Congenital Anomalies of the Kidneys and Urinary Tracts (CAKUT). Clinical journal of the American Society of Nephrology, 2020.PMID 32188635
- [2]Brockwell M, Hergenrother S, Satariano M, et al. Pathophysiology of Congenital Anomalies of the Kidney and Urinary Tract: A Comprehensive Review. Cells, 2024.PMID 39594614
- [3]Yalçınkaya F, Özçakar ZB. Management of antenatal hydronephrosis. Pediatric nephrology, 2020.PMID 31811536
- [4]Wong J, Rickard M, Dos Santos J, et al. Antenatal hydronephrosis: an updated review on postnatal care and management. Current opinion in pediatrics, 2025.PMID 40842394
- [5]RIVUR Trial Investigators, Hoberman A, Greenfield SP, et al. Antimicrobial prophylaxis for children with vesicoureteral reflux. The New England journal of medicine, 2014.PMID 24795142
- [6]Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management, Roberts KB. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics, 2011.PMID 21873693
- [7]Hafizar, Wahyudi I, Situmorang GR, et al. Long-term renal outcomes in children with posterior urethral valves: a systematic review and meta-analysis. Pediatric surgery international, 2026.PMID 42323785
- [8]Morris RK, Malin GL, Quinlan-Jones E, et al. Percutaneous vesicoamniotic shunting versus conservative management for fetal lower urinary tract obstruction (PLUTO): a randomised trial. Lancet, 2013.PMID 23953766
- [9]Cambio AJ, Evans CP, Kurzrock EA. Non-surgical management of multicystic dysplastic kidney. BJU international, 2008.PMID 18190645
- [10]La Scola C, Ammenti A, Bertulli C, et al. Management of the congenital solitary kidney: consensus recommendations of the Italian Society of Pediatric Nephrology. Pediatric nephrology, 2022.PMID 35713730
- [11]Costa FP, Simões E Silva AC, Mak RH, et al. A clinical predictive model of renal injury in children with isolated antenatal hydronephrosis. Clinical kidney journal, 2020.PMID 33123360
- [12]Pohl HG. Embryology, Treatment, and Outcomes of Ureteroceles in Children. Urologic clinics of North America, 2023.PMID 37385701
- [13]Baudin M, Herbez C, Guellec I, et al. Predictive factors for survival in patients with oligohydramnios secondary to antenatal kidney disease. Pediatric nephrology, 2023.PMID 36409365
- [14]Gatti JM, Kirsch AJ. Posterior urethral valves: pre- and postnatal management. Current urology reports, 2001.PMID 12084283