Paeds · fetal-neonatal-and-perinatal
Fetal assessment, prenatal screening and counselling
Also known as Antenatal fetal assessment · Prenatal screening · Cell-free DNA screening · Non-invasive prenatal testing · NIPT · Aneuploidy screening · Mid-trimester anomaly scan · Fetal growth surveillance · Antenatal counselling
Fellowship guide to antenatal fetal assessment and prenatal screening: first-trimester combined screening, mid-trimester anatomy ultrasound, cell-free DNA screening, fetal growth and Doppler surveillance, antepartum fetal-wellbeing testing, screen-versus-diagnosis counselling, soft markers, no-call results, CVS and amniocentesis risk, multidisciplinary planning and regional programme differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Most pregnancies are low risk, and most antenatal screening results come back reassuring. The difficulty is that the small number of abnormal or inconclusive results land in the middle of a working antenatal service and demand counselling, decisions and follow-through that families remember for the rest of their lives. Fetal assessment is the set of tests that estimates fetal risk, surveys fetal structure, monitors growth and placental function, and checks fetal wellbeing near term. [4] [8]
The single most important distinction in the whole topic is screening versus diagnosis. Screening estimates a probability. Diagnostic testing confirms or excludes a condition. First-trimester combined screening, cell-free DNA screening and the mid-trimester scan are screens — they tell you whether the chance of a problem is raised. Chorionic villus sampling and amniocentesis are diagnostic — they tell you what the chromosomes actually are. Blurring that line is the most common and most dangerous counselling error. [1] [16]
Antenatal screening fits classic screening principles when the condition is important, an accepted intervention exists, a suitable test is available, and the system can deliver confirmation and care rather than just a result. A positive screen that goes nowhere is not a programme. [6]
What you actually do across pregnancy
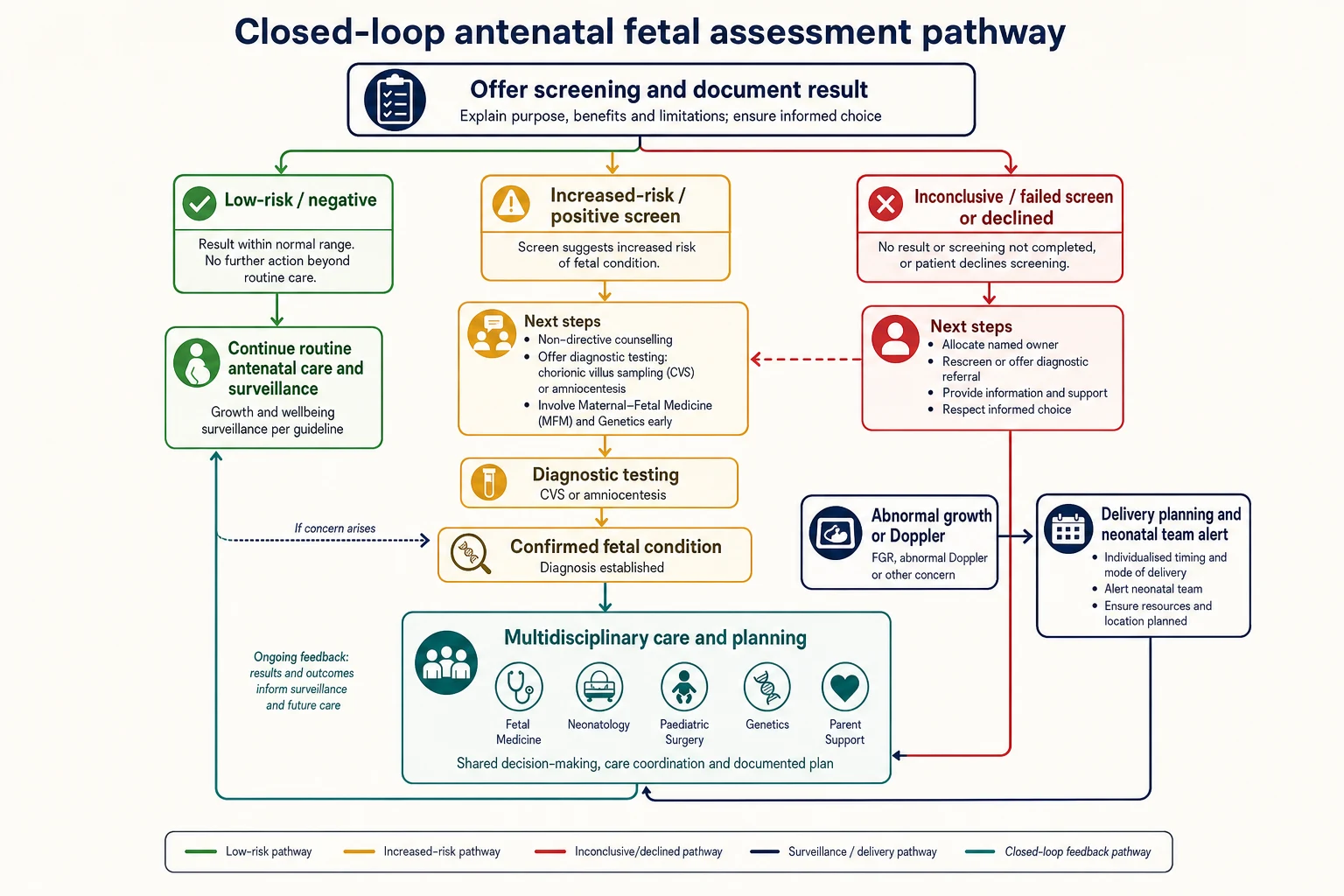
Offer and document
Offer aneuploidy and structural screening, and document the result explicitly. Never leave a blank that looks normal.
Name the result state
Record low-risk, increased-risk, inconclusive or declined. Each demands a different action.
Counsel non-directively
Screen is not diagnosis. Offer information, options and time. A no-call is not a low-risk result.
Confirm or surveil
Offer diagnostic testing for true increased-risk results. Plan surveillance for growth or Doppler concerns.
Close the loop
Multidisciplinary planning for confirmed conditions, neonatal alert, named owner, safety-net advice.
Classification
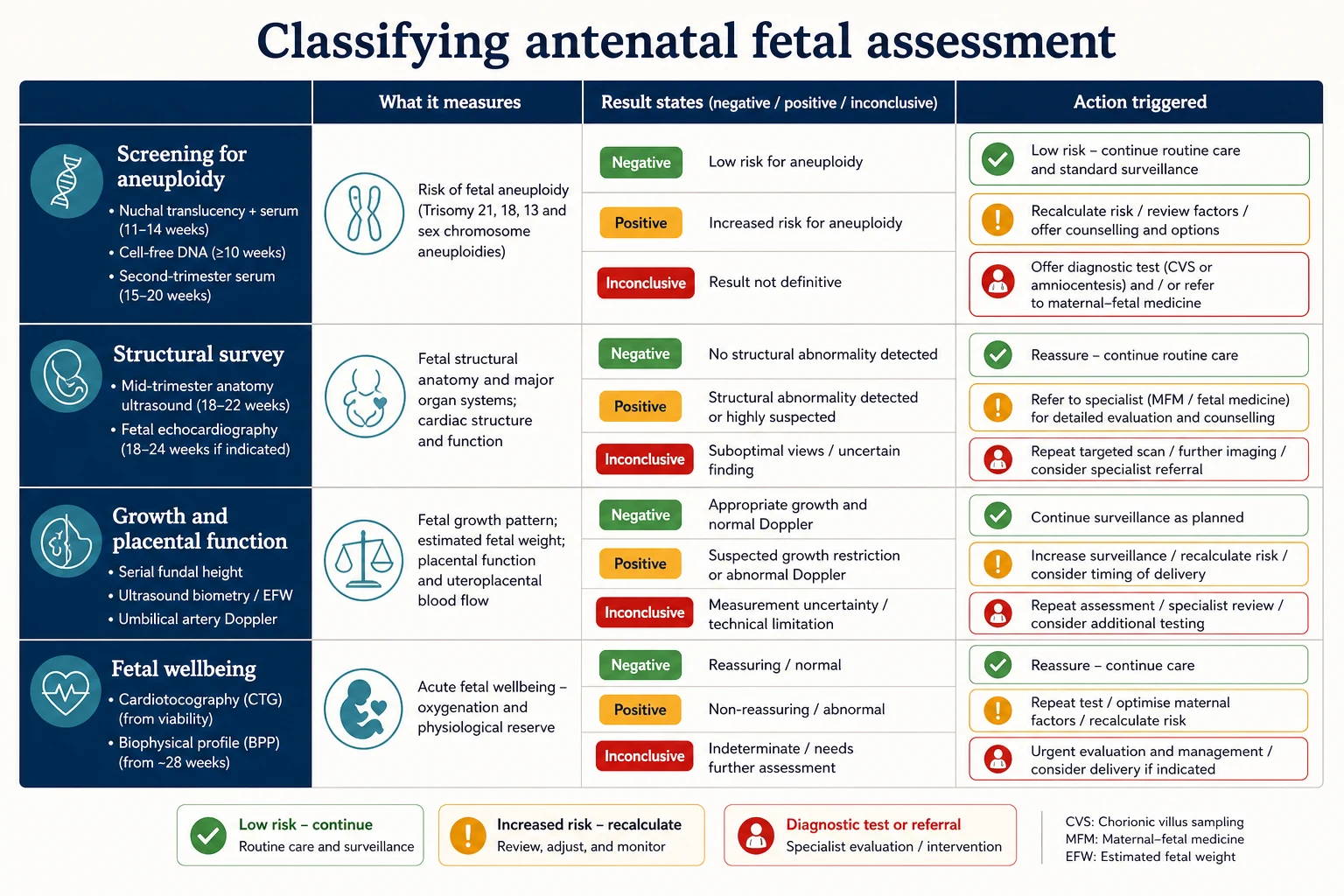
Think first in four assessment domains, each answering a different question about the fetus. [4] [9]
Aneuploidy screening estimates the chance of a chromosomal condition — trisomy 21, 18, 13 and sex-chromosome aneuploidies. Structural survey looks for physical malformations on the mid-trimester anatomy scan. Growth and placental-function assessment tracks whether the fetus is growing normally and whether the placenta is delivering. Fetal-wellbeing testing checks acute oxygenation and physiological reserve near term or when a fetus is known to be at risk. Mixing these up is how clinicians reassure themselves with the wrong test. [4] [9]
Then classify the result. Low-risk means continue routine care, but residual risk still exists. Increased-risk means counsel and offer diagnostic testing or specialist referral — it is not a diagnosis. Inconclusive (a no-call cell-free DNA result, a technically limited scan, or a result that could not be interpreted) is its own state with its own risk, not a pass. Declined means the family chose not to proceed, and it needs documentation and an open door, not coercion. [1] [16]
Two screening strategies exist for aneuploidy. Universal screening offers the test to everyone; contingent (risk-factor-targeted) screening reserves cell-free DNA for those at increased risk after first-trimester combined screening. Know which programme you work under rather than inventing a private algorithm. [1] [7]
A soft marker is a sonographic finding that is not a structural anomaly but that was once statistically associated with aneuploidy — an echogenic intracardiac focus, a choroid plexus cyst, mild renal pelviectasis, echogenic bowel or a short femur. The key teaching is that a soft marker's meaning depends almost entirely on the prior screening result. In a reassuringly screened pregnancy it usually changes nothing. In an unscreened pregnancy it recalculates risk. [6]
The common exam trap is treating a screen and a diagnostic test as interchangeable, or treating an inconclusive result as a low-risk result. Both are failures. [1] [16]
Screen
Estimates probability
- First-trimester combined, cfDNA, quad serum, anatomy scan
- Output is a risk, not a diagnosis
- A positive result triggers counselling and an offer of diagnosis
- A no-call is its own state, not low risk
Diagnostic
Confirms or excludes
- Chorionic villus sampling, amniocentesis
- Provides a definitive chromosomal or molecular result
- Carries a small procedure-related risk
- Residual structural and genetic risk may persist
Increased-risk
Not a diagnosis
- Counselling and an offer of diagnostic testing
- Cannot be cancelled by reassurance
- Pre-test probability matters
- Specialist referral for confirmed findings
Inconclusive
Not low-risk
- No-call cfDNA carries its own risk
- Repeat, diagnose or surveil by risk
- Name an owner before discharge
- Do not relabel as a pass
Epidemiology & Risk Factors
Major chromosomal aneuploidies and major structural anomalies are uncommon enough at the individual level but common enough at population level to justify universal screening rather than selective risk-factor testing. Trisomy 21 is the single most common survivable autosomal trisomy, and its probability rises steeply with maternal age. That is why advanced maternal age increases pre-test probability but does not, on its own, define a high-risk pregnancy. [7] [1]
Risk factors change counselling in two ways. They raise pre-test probability, which changes the meaning of any result, and they raise the chance of a no-call or inconclusive result. Maternal age, prior affected pregnancy, a parental balanced translocation, consanguinity, high body mass index and assisted reproduction all shift the baseline. A family history of a Mendelian condition moves the conversation toward targeted diagnostic testing rather than population screening. [1] [16]
Cell-free DNA has a specific failure mode worth knowing. A no-call result — when the laboratory cannot report because fetal fraction is too low — is more likely with high maternal weight, early gestational age at sampling, aneuploidy itself and fetal growth restriction. A no-call is therefore not a neutral outcome. It is a signal that carries its own risk and demands an action, not a re-labelling as low-risk. [1] [16]
Fetal growth restriction is driven by uteroplacental insufficiency, which is itself driven by maternal vascular disease, pre-eclampsia, smoking, chronic hypertension, antiphospholipid syndrome and multiple pregnancy. Recognising these factors early is what turns a late, unanticipated small baby into a planned, surveilled pregnancy. [2] [8]
Access barriers are part of the epidemiology, not an afterthought. Rural families, language-discordant families, those without reliable transport or leave from work, and those in out-of-home care all complete fewer screens and fewer diagnostic pathways. Incomplete pathways are where antenatal diagnosis silently fails. [18]
Pathophysiology
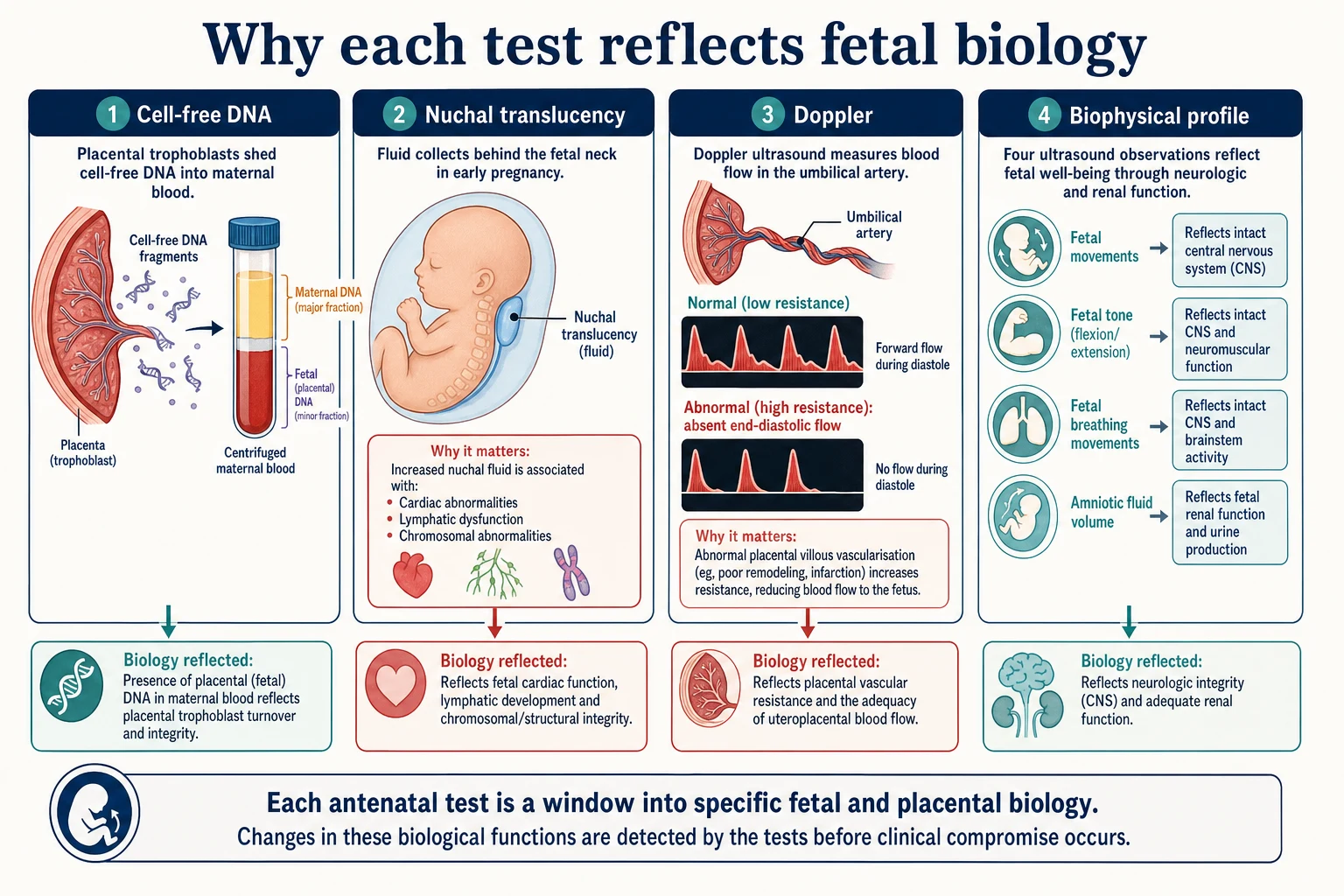
Each test reflects a different layer of fetal and placental biology, which is exactly why screens can disagree. [1] [4]
Cell-free DNA works because the placenta sheds DNA fragments into maternal blood. The test sequences that mixture and looks for the small fetal fraction. When the fetal fraction is adequate and the fetus carries a common trisomy, the relative excess of that chromosome is detectable. That placental origin matters: a confined placental mosaicism can produce a discordant result between cell-free DNA and the true fetal karyotype, which is why cell-free DNA remains a screen. It is also why a no-call is informative — a low fetal fraction is often a biological signal, not just a technical one. [1] [16]
Nuchal translucency is a measurement of fluid behind the fetal neck at 11 to 14 weeks. An increased measurement is not a single disease. It reflects delayed lymphatic drainage, cardiac failure from a structural lesion, a chromosomal cause, a structural anomaly or a genetic syndrome. That breadth is why an increased nuchal translucency with a normal karyotype still warrants detailed cardiac and structural review, and why a normal karyotype does not close the loop. [19]
The Doppler principle is the same one used elsewhere in medicine, applied to the umbilical artery. A normally developed placenta has low-resistance villous vessels, so blood flows forward throughout the cycle including diastole. When uteroplacental insufficiency remodels those vessels, resistance rises, diastolic flow falls, and in severe cases end-diastolic flow is absent or reversed. That waveform is a direct read-out of placental function, which is why it guides surveillance and delivery timing in growth restriction better than biometry alone. [8] [9]
The biophysical profile rests on the idea that an intact, well-oxygenated fetus moves, breathes and flexes, and that the kidneys produce urine to maintain amniotic fluid. Each component probes a different fetal system — central nervous system integrity, acute oxygenation and renal function — so a depressed profile reflects acute compromise rather than chronic growth failure. [3]
Clinical Presentation
The usual presentation of an abnormal fetal-assessment result is not a sick patient. It is a number on a report, a phone call, or a recall to clinic. The family was expecting reassurance. Your first task is to manage that expectation without minimising or over-calling. [6] [18]
Parents very often hear a positive screen as a confirmed diagnosis. The phrase "your screen came back positive" can be heard as "your baby has Down syndrome." Reframing is a clinical skill: a positive screen means the chance is raised and we need a more accurate test. State what the test does and does not say, then offer the next step. [1] [16]
An isolated soft marker usually presents as a line in a routine scan report. The temptation is to react to the finding alone. The correct reading is always against the prior screen. In a pregnancy that already had reassuring first-trimester or cell-free DNA screening, most isolated soft markers change nothing. In an unscreened pregnancy, the same finding recalculates risk and may prompt cell-free DNA or diagnostic testing. [6]
A no-call cell-free DNA result presents as a result that simply was not reported. Families may hear "they couldn't do the test" as "the test was normal." It is neither. It is a distinct result with its own risk and its own action. [1] [16]
An abnormal growth scan presents as an estimated fetal weight or centile that has fallen, often with an abnormal Doppler. The urgency comes from the combination — a small fetus with normal Doppler is managed very differently from a small fetus with absent end-diastolic flow. [8] [9]
A confirmed fetal condition presents to the family at counselling. From that moment the paediatrician's role begins: translate the diagnosis into a postnatal plan, involve neonatology and paediatric surgery where relevant, and hold the medical-home role through birth and beyond. [17] [18]
Differential Diagnosis
For a positive aneuploidy screen, four possibilities sit in the differential. A true positive (the fetus does carry the trisomy). A false positive (the screen is positive but the fetus is unaffected — common with biochemical screens). A screen elevated by a technical or biological confounder such as confined placental mosaicism. And a no-call artefact mistaken for a positive. The discriminating step is diagnostic testing, not a repeat screen when probability is high. [1] [16]
For an increased nuchal translucency with a normal karyotype, the differential is broad: cardiac malformation, a genetic syndrome (including RASopathies), structural anomaly, congenital infection and a transient or normal variant. The work-up is detailed fetal echocardiography, detailed anatomy review and, where indicated, microarray or gene-panel testing. A normal karyotype does not end the question. [19]
For a small-for-gestational-age fetus, the central discrimination is fetal growth restriction from a constitutionally small but healthy fetus. Doppler is the key discriminator: normal umbilical artery Doppler with normal growth velocity points toward constitutional smallness, while abnormal Doppler confirms placental insufficiency. The two are managed very differently. [2] [8]
For a soft marker, the prior screening result is the discriminator. In an already-screened pregnancy, isolated soft markers usually have negligible additional value. In an unscreened pregnancy, the same finding raises risk and prompts further testing. [6]
For a non-reassuring cardiotocograph, reversible causes (maternal position, hypoxia from supine compression, transient contractions, recent opioids) sit alongside pathological causes (cord compression, placental insufficiency, abruption). Act on the trace after addressing reversible factors, never on a single uninterpreted squiggle. [10]
For a family that declines screening, the differential of reasons is the real differential: values, fear, misunderstanding, access barriers, prior trauma and, rarely, safeguarding concern. Most declines are information or values problems, not safeguarding emergencies. Explore without coercing. [18]
Clinical & Bedside Assessment
Start with the focused history that changes risk: maternal age, parity, prior affected pregnancy, family history, consanguinity, parental translocation carrier status, medications and exposures, body mass index, smoking, ethnicity and assisted reproduction. These facts move pre-test probability and should be documented before any result is interpreted. [1] [7]
Fundal height is the bedside growth screen. Measure it consistently, with the mother supine and bladder empty, from the symphysis to the top of the fundus using a non-elastic tape. A discrepancy of around three centimetres from the expected gestation triggers ultrasound. Fundal height is operator-dependent, which is why it is a trigger rather than a diagnosis. [9]
Assess the family's real capacity to complete follow-up. Who has transport? Who has leave from work? Whose phone reliably works? Who holds decision-making authority? Does an interpreter need to be at the next visit, not just a translated letter days later? A perfect diagnostic booking that no one can attend is not a plan. [18]
At the bedside, read a cardiotocograph systematically: baseline rate, variability, accelerations and decelerations, and presence of contractions. Be explicit about reversible contributors before declaring the trace abnormal. The biophysical profile is read by its components — movement, tone, breathing, amniotic fluid volume, and the non-stress test — each scored to give a composite. A depressed profile is a reason to act, a single borderline component is not. [3] [10]
State an umbilical artery Doppler finding in plain terms: normal, increased resistance, absent end-diastolic flow or reversed end-diastolic flow. Avoid inventing a fixed systolic-to-diastolic ratio threshold in an exam if you cannot source the local cut-off; state that you will use the validated laboratory interpretation. [8] [9]
Investigations
The first-trimester combined screen, done between about 11 and 14 weeks, combines nuchal translucency measurement with maternal serum analytes — pregnancy-associated plasma protein A and free beta-human chorionic gonadotropin — alongside maternal age, to estimate risk for the common trisomies. It is the foundational aneuploidy screen and remains the comparator against which newer tests are judged. [7]
Cell-free DNA screening, offered from around 10 weeks, analyses placental cell-free DNA in maternal blood. It is highly sensitive for trisomy 21 in both high-risk and general-risk populations, but its performance for sex-chromosome aneuploidies and microdeletions is lower, and a no-call result is informative rather than neutral. It is a screen, not a diagnostic test. [1] [16]
The mid-trimester anatomy scan, performed between about 18 and 22 weeks, systematically surveys fetal structures, the placental site and amniotic fluid. It is the structural screen and detects a large proportion of major anomalies, with detection varying by system, operator and maternal body habitus. A focused fetal echocardiogram is added for defined high-risk groups. [4] [17]
Growth surveillance uses serial ultrasound biometry — biparietal diameter, head circumference, abdominal circumference and femur length — combined into an estimated fetal weight plotted against international standards. The INTERGROWTH-21st standards provide international references for fetal growth and estimated fetal weight. Umbilical artery Doppler, and in selected cases middle cerebral artery and ductus venosus Doppler, then interrogate placental function. [5] [14] [15]
Diagnostic testing is offered when pre-test probability is genuinely raised. Chorionic villus sampling, done from about 11 weeks, samples placental tissue and gives an earlier result but carries a small procedure-related risk and can encounter confined placental mosaicism. Amniocentesis, done from about 15 weeks, samples fetal cells in amniotic fluid. Contemporary estimates of procedure-related miscarriage risk are low and should be quoted in modern, not legacy, terms. [11] [12]
When prenatal testing is performed, chromosomal microarray detects submicroscopic copy-number variants that a conventional karyotype misses, and is preferred in the setting of structural anomalies. Be prepared to discuss variants of uncertain significance, which are real findings whose clinical meaning is not yet known. [4] [17]
Management — Resuscitation
Antenatal fetal assessment is rarely the first priority in a haemodynamically unstable mother. Resuscitate the mother first. Once she is stable, an abnormal surveillance result becomes the focus. [10]
For an acutely non-reassuring cardiotocograph, the immediate bundle is maternal repositioning (typically left lateral), intravenous fluids if hypotensive, stopping any oxytocin, treating a tachysystole, and considering acute tocolysis if needed. Oxygen is not routinely beneficial for fetal resuscitation when maternal saturation is normal; correct reversible contributors before declaring the trace pathological. [10]
For a growth-restricted fetus with abnormal Doppler — particularly absent or reversed end-diastolic flow — the time-critical question is delivery timing versus expectant surveillance, gated by gestational age. When delivery is brought forward, antenatal corticosteroids for fetal lung maturation and, at very preterm gestations, magnesium sulfate for neuroprotection enter the bundle. Plan these by gestation rather than improvising. [9] [13]
The other "resuscitation" moment in this topic is family crisis. A positive screen or a confirmed anomaly can trigger acute distress. Sit down, use plain language, separate screen from diagnosis, offer written information, involve senior staff and a genetic counsellor, and never force a decision in the same breath as the result. [6] [18]
When screening identifies a condition with a time-critical postnatal intervention — a ductal-dependent cardiac lesion, gastroschisis, congenital diaphragmatic hernia or a neural tube defect — the immediate bundle is multidisciplinary planning and deciding the place and time of delivery so that the right neonatal and surgical capability is present. [17] [18]
In rural settings where specialist fetal-medicine or neonatal capability is not on-site, a significant abnormality needs destination planning, not optimism. Give a named service, a timeframe and a backup contact before the family leaves. [18]
Management — Definitive & Stepwise
1. Interpret the result against pre-test probability
A result only means something against the prior chance of disease. The same positive screen in a 41-year-old and a 19-year-old carries a different positive predictive value. State the pre-test probability before you interpret. [1] [16]
2. Low-risk result
Continue routine antenatal care. Counsel residual risk: screening does not exclude every condition, and late-onset growth or wellbeing issues can still arise. Keep an open door for new concerns. [4] [8]
3. Increased-risk result
Offer non-directive counselling and a diagnostic test — chorionic villus sampling or amniocentesis, chosen by gestation and the question being asked. Involve maternal-fetal medicine and genetics. Do not substitute a repeat screen for diagnosis when probability is genuinely high. [1] [11]
4. Inconclusive or no-call result
Treat as its own state. Options are repeat cell-free DNA, diagnostic testing, or detailed ultrasound with surveillance — chosen by risk. A no-call is not a low-risk result and must not be relabelled as one. Name an owner before discharge. [1] [16]
5. Soft marker
Read against the prior screen. In an already-screened pregnancy, most isolated soft markers change nothing. In an unscreened pregnancy, offer screening or diagnostic testing as appropriate. The SMFM framework guides which isolated markers are clinically significant. [6]
6. Growth or Doppler concern
Confirm with repeat biometry against international standards, stratify as early-onset (often placental, Doppler-guided) or late-onset (often centile-guided), and set a surveillance and delivery-timing plan. Abnormal Doppler drives both surveillance intensity and the decision to deliver. [8] [9]
7. Confirmed fetal condition
Open the multidisciplinary pathway: maternal-fetal medicine, neonatology, paediatric surgery, genetics and parent support. Decide place and time of delivery, prepare the neonatal team, and assign the paediatrician the medical-home role for surveillance after birth. [17] [18]
Specific Subtypes & Scenarios
Increased nuchal translucency with normal karyotype. A normal chromosome result does not close the question. Detailed fetal echocardiography, a full anomaly review and consideration of microarray or a gene panel follow, because cardiac, structural and genetic causes may still be present. [19]
Isolated soft marker on the mid-trimester scan. Read against the prior screen. An echogenic intracardiac focus, choroid plexus cyst or mild renal pelviectasis in a reassuringly screened pregnancy usually changes nothing; the same finding in an unscreened pregnancy recalculates risk. [6]
Early-onset fetal growth restriction. Typically placental and detected before 32 weeks, often with abnormal Doppler. Management is Doppler-guided surveillance and delivery-timing, balancing prematurity against intrauterine compromise. [8] [9]
No-call cell-free DNA in a high-risk pregnancy. Do not simply repeat the screen. The no-call itself carries increased risk; diagnostic testing is often the right next step. [1] [16]
Sex-chromosome aneuploidy on cell-free DNA. Positive predictive value is lower than for common trisomies. Counsel carefully and confirm diagnostically before any management decision. [1] [16]
Ductal-dependent cardiac lesion. Plan delivery at a centre with neonatal cardiac capability, with the cardiology and neonatal teams prepared. The goal is to avoid an unanticipated duct-dependent collapse after birth. [17]
Confirmed structural anomaly requiring postnatal surgery. Gastroschisis, congenital diaphragmatic hernia and neural tube defects each demand antenatal paediatric-surgical consultation, place-of-delivery planning and a defined postnatal pathway. [18]
Twin pregnancy with discordant growth. Chorionicity drives everything. Monochorionic complications such as selective growth restriction require specialist surveillance and, in some cases, in-utero therapy. [8]
Variant of uncertain significance on prenatal microarray. Counsel honestly: this is a real finding whose clinical meaning is not yet known. Involve clinical genetics, parental testing where appropriate, and avoid over-interpreting. [4] [17]
Family declines further testing after a positive screen. Explore the reasons without coercion, document residual risk, offer ongoing antenatal care, and keep the door open. Respecting autonomy does not mean abandoning surveillance of growth and wellbeing. [18]
Complications & Pitfalls
False-positive screens cause anxiety, extra visits and, in the worst case, an unnecessary invasive procedure with its own risk. Accurate non-directive counselling and rapid access to diagnostic testing minimise this harm. [1] [11]
False-negative and missed diagnoses create the opposite harm: an unanticipated finding at birth, lost preparation time, and a neonatal team caught unready. Late booking and declined screening are where this harm concentrates. [4] [18]
Classic pitfalls recur across exams and practice: treating a screen as a diagnosis, relabelling a no-call as low-risk, dismissing a soft marker in an unscreened pregnancy, over-calling a single non-reassuring cardiotocograph, discharging an inconclusive result with no owner, forgetting residual risk after a normal diagnostic result, and substituting a repeat screen for diagnosis when probability is high. [1] [6]
Lost-to-follow-up is the quiet complication that destroys programme benefit. An increased-risk result with no booked diagnostic appointment is a systems failure and should be chased like any abnormal critical result. [18]
Poor documentation and handover across sites and clinicians is a preventable cause of missed planning. A result that lives only in one clinician's memory is a result at risk of being lost. [4] [9]
Prognosis & Disposition
Prognosis after an abnormal result is governed by three things: the pre-test probability, the positive predictive value of the result in that individual, and whether diagnostic testing confirms a real condition. A screen raises concern; only confirmation defines prognosis. [1] [16]
A constitutionally small but healthy fetus with normal growth velocity and normal Doppler has an excellent prognosis. A truly growth-restricted fetus with abnormal Doppler has a prognosis shaped by gestation at delivery, the degree of placental insufficiency and the presence of comorbidity. Doppler-guided delivery timing is what shifts that prognosis. [8] [9]
For major structural anomalies, earlier detection and planned multidisciplinary delivery measurably improve neonatal outcomes — the right team is present, resuscitation is anticipated, and the family is prepared. [17] [18]
Disposition is "result owned, loop closed." A low-risk result goes home with routine care and an open door. An increased-risk result goes home only with a booked diagnostic pathway and a named owner. An inconclusive result needs the same ownership standard. A confirmed condition needs a documented multidisciplinary plan and a neonatal alert. [4] [18]
Residual risk after a normal diagnostic result is real. A normal karyotype does not exclude structural or single-gene disease, so surveillance of growth, structure and postnatal development continues. [19]
Special Populations
Adolescent pregnancies, advanced-maternal-age pregnancies and those conceived through assisted reproduction each carry different counselling weights. Pre-test probability differs, and so does the family's readiness to make decisions under pressure. [1] [7]
Cultural safety changes uptake. Indigenous, Māori, Pacific, migrant, refugee and asylum-seeking families need interpreter-supported counselling at the moment of the result, not a translated letter days later, and care that respects family decision structures. [18]
Consanguinity and known familial genetic conditions move the conversation toward targeted diagnostic testing rather than population aneuploidy screening, and toward genetic counselling before pregnancy where possible. [4]
High body mass index lowers cell-free DNA performance through lower fetal fraction and raises the chance of a no-call. Multiple pregnancy changes every screen — cell-free DNA algorithms are more complex, and growth surveillance is more intensive. These are not edge cases; they are routine. [1] [16]
Rural and remote families need discharge plans matched to real travel times and capability. Socioeconomic disadvantage and out-of-home care reduce screening completion. Identify these barriers early and design the pathway around them. [18]
Families connected to Deaf or disability communities may frame outcomes differently from clinicians. Good care is accurate information, timely diagnosis, and respect for family values — never ableism dressed up as counselling. [18]
Evidence, Guidelines & Regional Differences
The FaSTER trial established first-trimester combined screening as a robust method for estimating trisomy risk and remains the comparator against which newer screens are judged. [7]
The CARE trial showed that cell-free DNA screening had high sensitivity and specificity for trisomy 21 in a general-risk population, which is the evidence base for offering it beyond high-risk cohorts. Its limitations — lower performance for sex-chromosome aneuploidies and microdeletions, the meaning of a no-call — are equally well described. [1]
The Gordijn Delphi consensus gave fetal growth restriction a definition that separates the truly growth-restricted fetus from the constitutionally small one, and that definition now underpins surveillance and delivery-timing guidance. [2] INTERGROWTH-21st supplied the international growth and estimated-fetal-weight standards against which size and growth are now judged. [14] [15]
ISUOG guidelines define the structural survey and the biometry and growth assessment. ACOG Practice Bulletins on fetal growth restriction and antepartum fetal surveillance, and the SMFM Consult Series on soft markers, shape management in North America. [4] [5] [6] [9] [10]
Contemporary systematic reviews place the procedure-related miscarriage risk of chorionic villus sampling and amniocentesis at low levels and argue against quoting legacy, higher estimates that deter families from diagnostic testing they need. [11] [12]
Australia and Aotearoa New Zealand offer universal aneuploidy and anomaly screening under national pregnancy-care guidance, with jurisdictional variation in cell-free DNA funding and rural diagnostic access. Quote the local programme panels and windows. [4]
United Kingdom runs national antenatal screening programmes (NHS Fetal Anomaly Screening Programme) with defined offer, referral and diagnostic pathways. [4]
United States follows ACOG and SMFM guidance; cell-free DNA is offered to all pregnant patients regardless of risk, with the option of diagnostic testing. Operational detail varies by institution and insurer. [1] [16]
Canada uses provincial programmes; geography and access often dominate diagnostic and surveillance planning. [4]
State only differences you have verified against current official programme pages. Do not invent a fixed Doppler index or a universal screening window. [8]
Exam Pearls
- Screening estimates risk; diagnostic testing confirms. Never blur the two. [1]
- A positive screen is a ticket to counselling and an offer of diagnosis, not a diagnosis. [1] [16]
- A no-call cell-free DNA result is not low-risk; it carries its own risk and action. [1]
- A soft marker is read against the prior screen, not in isolation. [6]
- Increased nuchal translucency with a normal karyotype still warrants cardiac and structural review. [19]
- Early-onset growth restriction is placental and Doppler-guided; late-onset is often centile-guided. [8] [9]
- Quote modern, not legacy, procedure-related risks for CVS and amniocentesis. [11] [12]
- A normal karyotype does not exclude structural or single-gene disease. [4] [17]
- Name an owner for every inconclusive, declined or incomplete result before discharge. [18]
- The paediatrician's antenatal role is to translate the diagnosis into a postnatal plan. [18]
CLOSURE package
References
- [1]Norton ME, Jacobsson B, Swamy GK, et al. Cell-free DNA analysis for noninvasive examination of trisomy. The New England journal of medicine, 2015.PMID 25830321
- [2]Gordijn SJ, Beune IM, Thilaganathan B, et al. Consensus definition of fetal growth restriction: a Delphi procedure. Ultrasound in obstetrics & gynecology, 2016.PMID 26909664
- [3]Manning FA, Platt LD, Sipos L. Antepartum fetal evaluation: development of a fetal biophysical profile. American journal of obstetrics and gynecology, 1980.PMID 7355965
- [4]Salomon LJ, Alfirevic Z, Berghella V, et al. ISUOG Practice Guidelines (updated): performance of the routine mid-trimester fetal ultrasound scan. Ultrasound in obstetrics & gynecology, 2022.PMID 35592929
- [5]Salomon LJ, Alfirevic Z, Da Silva Costa F, et al. ISUOG Practice Guidelines: ultrasound assessment of fetal biometry and growth. Ultrasound in obstetrics & gynecology, 2019.PMID 31169958
- [6]Society for Maternal-Fetal Medicine, Prabhu M, Kuller JA, et al. SMFM Consult Series #57: Evaluation and management of isolated soft ultrasound markers for aneuploidy in the second trimester. American journal of obstetrics and gynecology, 2021.PMID 34171388
- [7]Malone FD, Canick JA, Ball RH, et al. First-trimester or second-trimester screening, or both, for Down's syndrome. The New England journal of medicine, 2005.PMID 16282175
- [8]Lees CC, Romero R, Stampalija T, et al. Clinical Opinion: The diagnosis and management of suspected fetal growth restriction: an evidence-based approach. American journal of obstetrics and gynecology, 2022.PMID 35026129
- [9]American College of Obstetricians and Gynecologists. Fetal Growth Restriction: ACOG Practice Bulletin, Number 227. Obstetrics and gynecology, 2021.PMID 33481528
- [10]American College of Obstetricians and Gynecologists. Antepartum Fetal Surveillance: ACOG Practice Bulletin, Number 229. Obstetrics and gynecology, 2021.PMID 34011889
- [11]Salomon LJ, Sotiriadis A, Wulff CB, et al. Risk of miscarriage following amniocentesis or chorionic villus sampling: systematic review of literature and updated meta-analysis. Ultrasound in obstetrics & gynecology, 2019.PMID 31124209
- [12]Beta J, Zhang W, Geris S, et al. Procedure-related risk of miscarriage following chorionic villus sampling and amniocentesis. Ultrasound in obstetrics & gynecology, 2019.PMID 30977213
- [13]McGoldrick E, Stewart F, Parker R, et al. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. The Cochrane database of systematic reviews, 2020.PMID 33368142
- [14]Papageorghiou AT, Ohuma EO, Altman DG, et al. International standards for fetal growth based on serial ultrasound measurements: the Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project. The Lancet, 2014.PMID 25209488
- [15]Stirnemann J, Villar J, Salomon LJ, et al. International estimated fetal weight standards of the INTERGROWTH-21st Project. Ultrasound in obstetrics & gynecology, 2017.PMID 27804212
- [16]Society for Maternal-Fetal Medicine Publications Committee. SMFM Statement: clarification of recommendations regarding cell-free DNA aneuploidy screening. American journal of obstetrics and gynecology, 2015.PMID 26458766
- [17]Donofrio MT, Moon-Grady AJ, Hornberger LK, et al. Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American Heart Association. Circulation, 2014.PMID 24763516
- [18]Benachi A, Sarnacki S. Prenatal counselling and the role of the paediatric surgeon. Seminars in pediatric surgery, 2014.PMID 25459006
- [19]Bakker M, Pajkrt E, Bilardo CM. Increased nuchal translucency with normal karyotype and anomaly scan: what next? Best practice & research. Clinical obstetrics & gynaecology, 2014.PMID 24332983