Paeds · fetal-neonatal-and-perinatal
Antenatally diagnosed fetal conditions: paediatric planning
Also known as Antenatally diagnosed fetal anomaly · Prenatally diagnosed congenital condition · Fetal diagnosis and neonatal planning · Multidisciplinary antenatal planning · Delivery-room planning for fetal anomaly · Place, time and capability of delivery · EXIT procedure planning · Neonatal alert for prenatal diagnosis
Fellowship guide to paediatric planning for the antenatally diagnosed fetus: translating a prenatal diagnosis into a postnatal plan, running the multidisciplinary team, deciding place, time and capability of delivery, anticipating delivery-room resuscitation for ductal-dependent cardiac lesions, congenital diaphragmatic hernia, gastroschisis, omphalocele, congenital pulmonary airway malformation and neural tube defects, planning the EXIT airway strategy, counselling families, and long-term developmental follow-up with regional perinatal-network differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Most antenatal diagnoses arrive on the paediatrician's desk as a referral, a multidisciplinary note, or a phone call from fetal medicine. The family was expecting reassurance and has instead received news that changes the shape of the pregnancy. The obstetric team has made the diagnosis; the paediatrician's distinct role is to convert that diagnosis into a safe, executable postnatal plan. [2]
The single most useful organising idea is place, time and capability of delivery. Place means the centre with the right team present — neonatology, surgery, cardiology, retrieval — not merely the nearest hospital. Time means the gestational age at which delivery gives the best balance between the condition's natural history and the risks of prematurity. Capability means the specific skills and equipment the diagnosis demands, from prostaglandin for a ductal-dependent heart to an EXIT-capable airway team. These three decisions, made together with the family and the obstetric team, are the deliverable of antenatal paediatric planning. [1] [2]
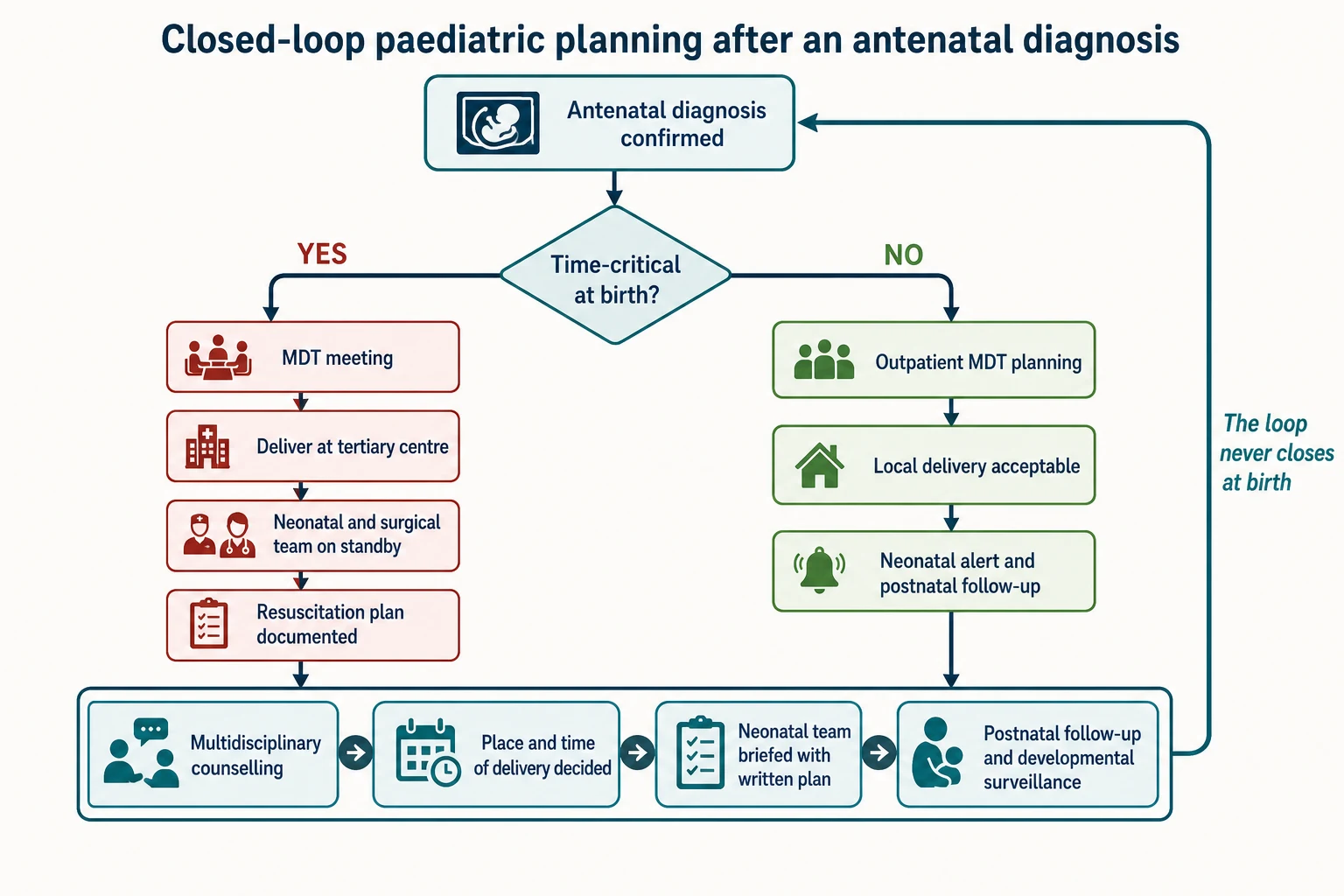
Antenatal planning rests on a simple biological truth: knowing what is coming lets you assemble the right people in the right place at the right time, and for several serious conditions that single advantage changes survival. The catch is that a plan only earns that benefit when it is written, shared, and executed by whoever is on shift when the baby arrives — a plan that lives in one person's head is a plan at risk of being lost. [7] [9]
What you actually do after a diagnosis
Confirm the diagnosis
Review the fetal medicine report, the imaging and the karyotype. Separate a confirmed structural finding from an uncertain or isolated variant.
Judge time-criticality
Is this condition dangerous at birth — ductal-dependent, airway-compromising, bowel-exposing — or surveillance-only? The answer sets place and capability.
Convene the team
Maternal-fetal medicine, neonatology, paediatric surgery, cardiology, genetics and allied health. Decide place, time and capability together.
Write it down
A written neonatal alert and resuscitation plan that survives shift and site changes. Name an owner.
Counsel and close the loop
Non-directive family-centred counselling, teach-back, booked follow-up, safety-net. The loop continues after birth with developmental surveillance.
Classification
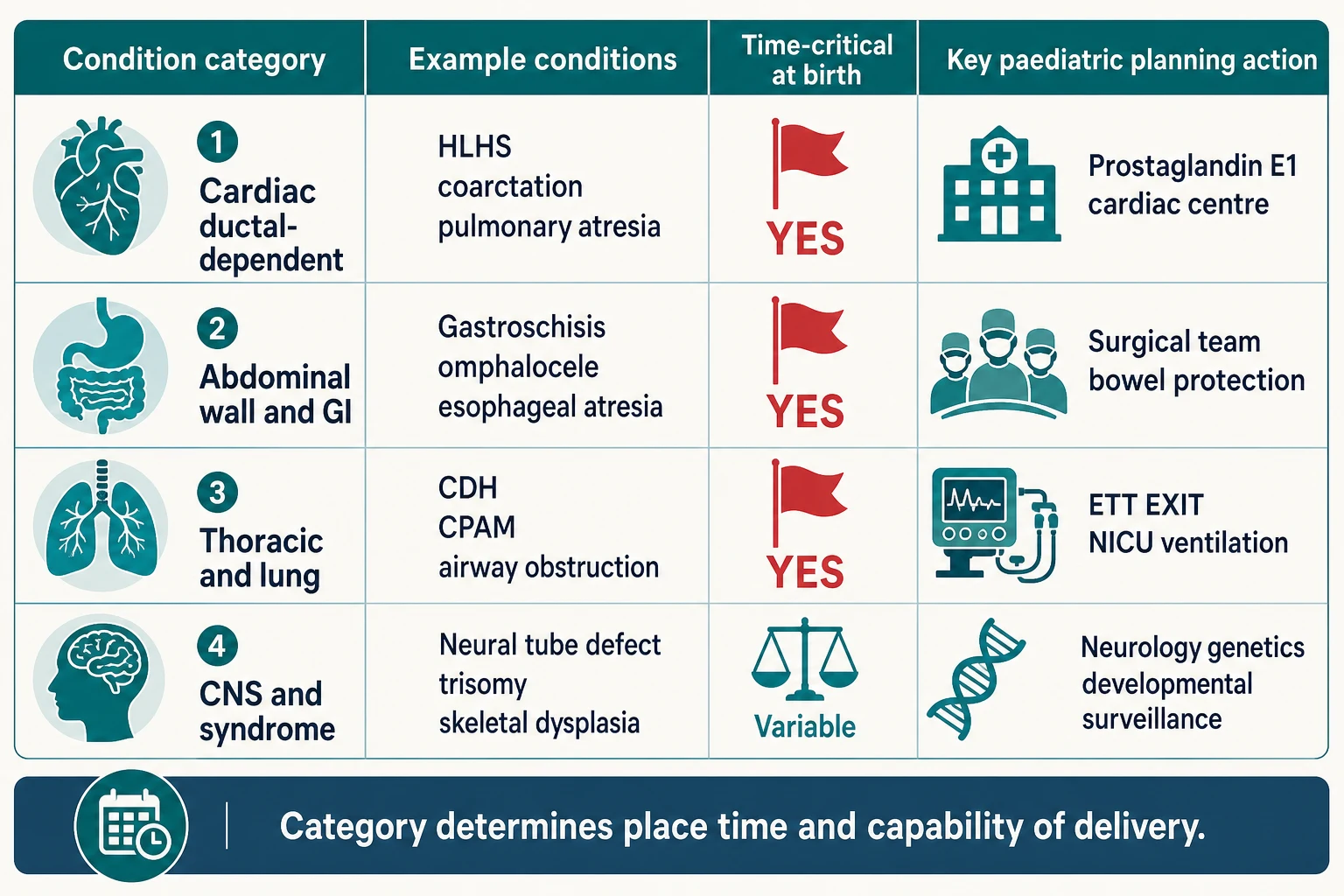
The fastest way to plan is to sort the diagnosis by what it demands at birth. Some conditions will kill or harm the baby within minutes of delivery unless the right team and treatment are already running; others need planned surgery or surveillance but tolerate a calm, routine transition. [1] [2]
A ductal-dependent cardiac lesion — hypoplastic left heart syndrome, critical aortic stenosis, interrupted aortic arch, pulmonary atresia with an intact septum — depends on the ductus arteriosus to carry blood to the body or the lungs. When the duct closes in the first hours of life, the circulation collapses. Antenatal diagnosis exists precisely so prostaglandin E1 can be started before that closure, and so the baby is delivered where cardiac capability is present. [1] [19]
Airway-compromising lesions — a large cervical lymphatic malformation, a cervical teratoma, severe micrognathia with obstruction — threaten the airway the moment the cord is cut. These are the diagnoses for which an EXIT procedure is considered: the airway is secured on placental support before the cord is divided. Bowel-exposing lesions — gastroschisis, and to a different degree ruptured omphalocele — lose heat and fluid quickly and need surgical cover from birth. [2] [9]
Thoracic and lung lesions — congenital diaphragmatic hernia, a large congenital pulmonary airway malformation, or a bronchogenic cyst — risk respiratory failure at birth from pulmonary hypoplasia, mediastinal shift or compression. CNS and syndromic diagnoses — neural tube defects, chromosomal conditions, skeletal dysplasias — are usually surveillance-oriented rather than minute-critical, but they carry their own depth of neurosurgical, genetic and developmental planning. [7] [10]
A useful second cut distinguishes isolated from syndromic. An isolated lesion — a straightforward gastroschisis with normal chromosomes — has a narrower plan. A syndrome or chromosomal diagnosis widens the plan to include genetics, recurrence counselling, and developmental follow-up, because the structural finding is only one part of a broader problem. A normal karyotype never closes that question, because single-gene disease and unrecognised syndromes remain. [10] [18]
Delivery-critical
Place and team dictated
- Ductal-dependent cardiac lesion
- Congenital diaphragmatic hernia
- Gastroschisis, large omphalocele
- Predicted airway obstruction (EXIT)
Transition-critical
Resuscitation plan dictated
- Severe fetal growth restriction with abnormal Doppler
- Large CPAM with mediastinal shift
- Hydrops of any cause
- Preterm planned delivery for a diagnosed condition
Surveillance-only
Local delivery often safe
- Small isolated CPAM
- Mild hydronephrosis
- Resolved soft marker
- Isolated borderline finding with normal karyotype
Syndromic
Breadth of plan dictated
- Chromosomal aneuploidy
- Recognisable syndrome
- Multiple anomalies
- Variant of uncertain significance with phenotype
Epidemiology & Risk Factors
Major congenital anomalies are uncommon in any single pregnancy but common enough across the population to justify structured antenatal detection. Only a proportion are picked up before birth, and that proportion varies sharply by condition and by the quality of the local ultrasound service. Congenital heart disease is the most common major malformation, but it remains one of the most frequently missed antenatally — which is exactly why a fetus with a confirmed cardiac lesion is precious planning territory. [1] [20]
The conditions that most often demand planned delivery at a tertiary centre cluster in the time-critical categories above. Congenital diaphragmatic hernia, gastroschisis, ductal-dependent cardiac lesions and large thoracic masses each carry a real risk of an unanticipated neonatal crisis if they are first met in an unprepared delivery room. Gastroschisis in particular has risen in prevalence over recent decades and disproportionately affects younger mothers, though the reason remains debated. [7] [9]
Maternal factors shift both the chance of a complex diagnosis and the depth of planning required. Advanced maternal age, assisted reproduction, pre-gestational diabetes, consanguinity, anticonvulsant or other teratogenic exposure, and a prior affected pregnancy all raise pre-test probability and the likelihood of a syndromic rather than isolated finding. A family history of a Mendelian condition moves the conversation toward targeted genetic testing and recurrence counselling rather than population screening. [10] [18]
Access is part of the epidemiology, not an afterthought. Rural and remote families, language-discordant families, and those without reliable transport or leave from work complete fewer antenatal pathways and reach fewer planned deliveries. An antenatal diagnosis that is made but never converted into a written, executable plan is where paediatric planning silently fails — the diagnosis is detected, the benefit is not realised. [2]
Preterm birth frequently compounds a structural diagnosis, and the two interact: a growth-restricted fetus with a cardiac lesion at 30 weeks carries a very different plan from the same lesion at term. Recognising these interactions early is what turns a late, unanticipated crisis into a prepared transition. [3] [4]
Pathophysiology
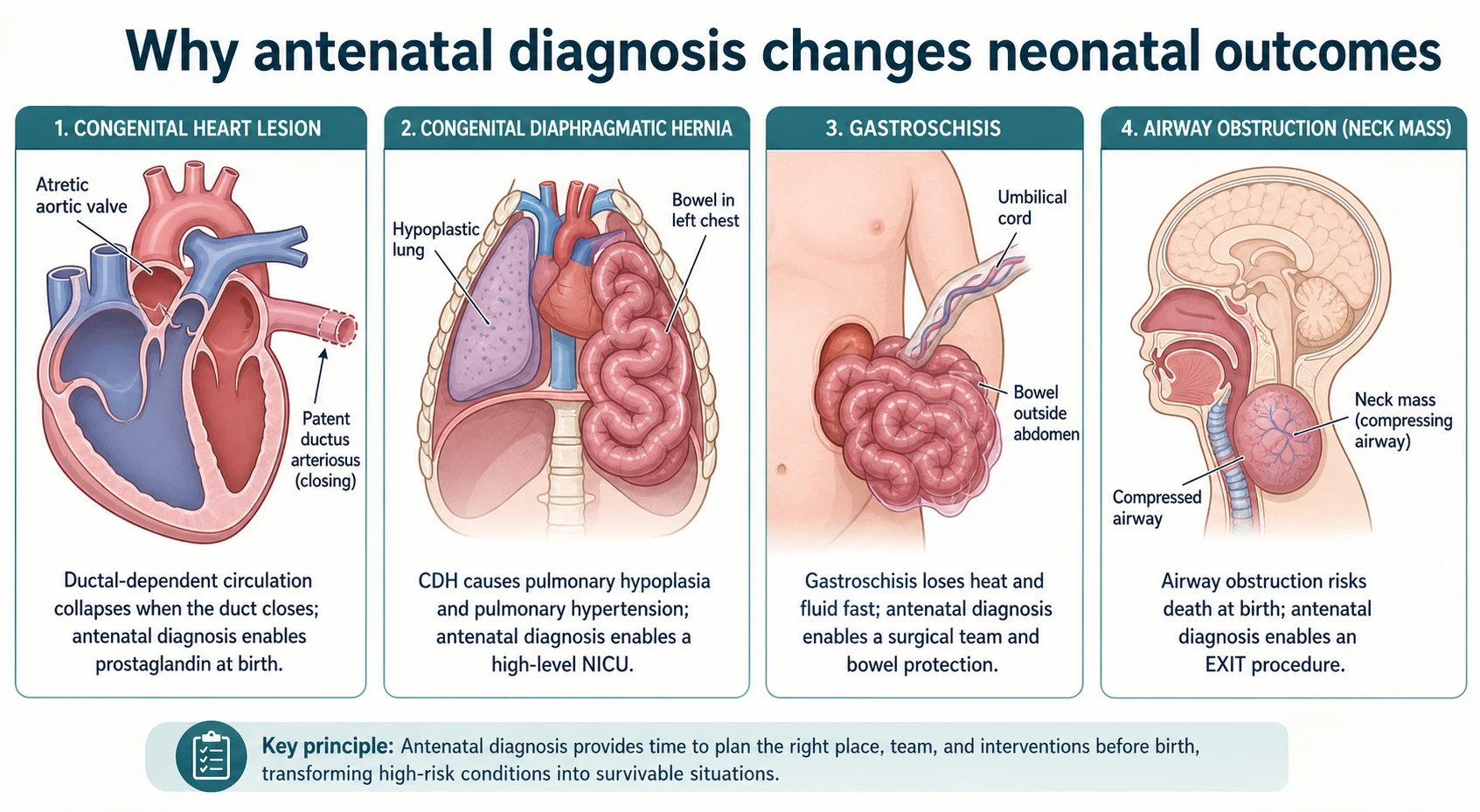
Each time-critical diagnosis has a mechanism that explains why knowing about it before birth changes the outcome. Understanding those mechanisms is what lets you defend a place-of-delivery decision in a viva, rather than memorising a list. [1] [7]
In a ductal-dependent circulation, the ductus arteriosus carries blood that the malformed side of the heart cannot. Hypoplastic left heart syndrome depends on the duct to supply the systemic circulation through the pulmonary artery; pulmonary atresia with an intact septum depends on it to supply the lungs. Prostaglandin E1 keeps the duct open, but the duct begins to close within hours of birth in response to the rise in oxygen. Without antenatal diagnosis, the first sign is often cardiovascular collapse after the duct has already narrowed — shock, acidosis, and an organ injury that staged surgery cannot fully undo. Antenatal diagnosis exists so prostaglandin is running before that point. [1] [19]
Congenital diaphragmatic hernia works through two mechanisms that operate together. The herniated bowel compresses the developing lung on the ipsilateral and contralateral sides, producing pulmonary hypoplasia — too few and too small airways and vessels. The same vascular abnormality then drives persistent pulmonary hypertension of the newborn, in which the pulmonary vessels fail to dilate at birth and right-to-left shunting perpetuates hypoxaemia. The lesson for the resuscitation team is concrete: mask ventilation inflates the stomach-bowel in the chest and worsens compression, so early intubation with gentle ventilation and gastric decompression is the planned approach, in a centre that can manage pulmonary hypertension. [7] [8]
Gastroschisis is a full-thickness para-umbilical abdominal wall defect through which the bowel herniates uncovered. At birth the exposed bowel loses heat and fluid rapidly, can become oedematous and compromised, and is at risk of volvulus or atresia. The mechanism dictates the plan: protect and cover the bowel, maintain warmth and hydration, keep the baby nil by mouth, and have the surgical team ready. Omphalocele is mechanistically different — the bowel is covered by a peritoneal sac, the defect is midline, and the condition is strongly associated with chromosomal and cardiac anomalies — which is why the two must never be planned identically. [9] [18]
An airway-compromising cervical mass threatens the single most time-critical task at birth: establishing an airway. A large lymphatic malformation or teratoma can distort or compress the upper airway so severely that intubation at birth is impossible. The EXIT procedure keeps the baby on placental support while the airway is secured by intubation, bronchoscopy, or tracheostomy, buying the minutes that would otherwise be unavailable after cord division. [2]
A neural tube defect works more slowly but no less seriously. The open spinal cord produces motor and sensory loss below the lesion, neurogenic bladder and bowel, and — through the associated Chiari II malformation — hindbrain herniation and hydrocephalus. The MOMS trial showed that prenatal repair improves hindbrain herniation and reduces the need for a ventricular shunt, at the cost of prematurity and maternal morbidity, which is why the decision is made at a specialist fetal-surgery centre rather than by the general paediatrician alone. [6] [10]
Clinical Presentation
An antenatal diagnosis rarely presents to the paediatrician as a sick patient. It presents as information — a referral, a copy of a fetal medicine report, a slot in a multidisciplinary meeting, or occasionally an unanticipated finding at birth when the antenatal pathway broke down. Managing that information, and the family's reaction to it, is the clinical work. [2]
The first task at an antenatal counselling visit is to understand what the family has already been told and how they have heard it. Families very commonly retain a diagnosis as a single catastrophic word — "heart problem", "hole in the diaphragm", "brain problem" — and may not have separated the structural finding from its severity, its associations, or its prognosis. Reframing is a clinical skill: state plainly what is and is not known, what the plan will be, and what the next decision is, without minimising or over-calling. [1] [2]
A ductal-dependent cardiac lesion presents in the planning phase as a fetal echocardiogram report; if the plan fails, it presents after birth as a baby who becomes grey, mottled and pulseless as the duct closes in the first hours of life. A congenital diaphragmatic hernia presents after birth as respiratory distress with a scaphoid abdomen and shifted heart sounds. Gastroschisis presents visibly — bowel beside the cord — at the moment of delivery. Each of these presentations is predictable, and predictability is the whole point of planning. [7] [9]
A missed or incomplete plan presents as the failures the planning exists to prevent: an unanticipated resuscitation, a baby delivered in a centre without the capability the diagnosis demands, a delayed retrieval, or a surgical emergency that meets an unbriefed team. The common thread is that the information existed but was not converted into an executable, shared plan. [2]
A diagnosis that is confirmed structurally but whose functional severity is uncertain until after birth is its own presentation. A borderline diaphragmatic hernia, a cardiac lesion of uncertain progression, or a growth-restricted fetus with an anomaly all demand honest counselling that the plan may need to adapt after delivery. The paediatrician holds open the possibility that the outcome may be better or worse than predicted, and builds surveillance to respond. [3] [19]
Differential Diagnosis
For an antenatal cardiac lesion, the discriminating question is whether the circulation is ductal-dependent. A ductal-dependent lesion — hypoplastic left heart, critical coarctation, interrupted aortic arch, critical aortic stenosis, pulmonary atresia — needs prostaglandin and a cardiac centre. A non-ductal-dependent lesion, such as a small ventricular septal defect, tolerates routine transition with postnatal evaluation. The fetal echocardiogram, not the postnatal exam alone, makes this call antenatally. [1]
For a thoracic mass, the differential sits between congenital diaphragmatic hernia, congenital pulmonary airway malformation, bronchogenic cyst, and bronchopulmonary sequestration. A diaphragmatic hernia puts bowel in the chest and drives pulmonary hypoplasia; a CPAM is a disordered pulmonary tissue mass that can cause mediastinal shift and hydrops when large. The distinction changes the resuscitation plan: hernia demands early intubation and gastric decompression, while a small asymptomatic CPAM may need only postnatal imaging and elective resection. [7] [11] [12]
For an abdominal wall defect, gastroschisis and omphalocele must never be conflated. Gastroschisis is typically right-sided, has no covering sac and a normally inserted cord, and is usually isolated with a favourable prognosis. Omphalocele is midline, covered by a peritoneal sac, and carries a high rate of chromosomal and cardiac associations that widen the work-up and change recurrence counselling. The surgical and genetic plans differ accordingly. [9] [18]
For a neck mass, lymphatic malformation, teratoma and thyromegaly each carry different airway risk and different associations. The discriminating question is whether the airway is predicted to be obstructed — and if so, EXIT moves from a possibility to the plan. For fetal hydrops, the differential is broad — immune, cardiac, anaemic (including parvovirus), infectious, metabolic and genetic — and each cause changes both the antenatal treatment and the postnatal plan. [2] [17]
For a suspected bowel obstruction, a double-bubble points to duodenal atresia (strongly associated with trisomy 21), polyhydramnios with an absent stomach bubble raises esophageal atresia, and dilated lower loops raise a lower obstruction. When an anomaly is found, the real differential is isolated versus syndromic, because a syndrome widens the plan to genetics, recurrence counselling and developmental follow-up. [10] [16]
Clinical & Bedside Assessment
Begin with the records, not the family. Before an antenatal counselling visit, read the fetal medicine report for the diagnosis, its severity markers, any associated findings, the karyotype or microarray result, the growth and liquor assessment, and any prior intervention. The planning-relevant facts are in that report, and a counselling visit built on an unread report wastes the family's time. [2]
The structured counselling encounter follows a reliable shape. State what is known and what is uncertain. Describe the plan in plain terms — where, when, and who will be present. Offer the options where options genuinely exist, and be honest where they do not. Use teach-back: ask the family to say back, in their own words, what they understand and what will happen next. A family that cannot teach the plan back has not been given a plan. [2]
Assess the family's real capacity to complete the plan. Who has transport to a tertiary centre that may be hours away? Who has leave from work? Whose phone reliably works? Does an interpreter need to be at the next visit, not merely a translated letter days later? Who holds decision-making authority in the family? A perfect plan that no one can execute is not a plan. [2]
Plan the immediate newborn assessment for the diagnosis. For a ductal-dependent lesion, that means pre-ductal and post-ductal oxygen saturation monitoring, assessment of perfusion, and prostaglandin readiness from the moment of birth. For a diaphragmatic hernia, it means anticipating respiratory distress, an asymmetric chest, a scaphoid abdomen, and the need for early intubation and gentle ventilation. For gastroschisis, it means protecting the exposed bowel with a clean covering and a bowel bag, maintaining temperature, keeping the baby nil by mouth, and alerting surgery. [1] [7] [9]
Document a neonatal alert and a written handover that can survive a change of shift or site. The written plan names the diagnosis, the place and time of delivery, the resuscitation steps, the team to be present, the postnatal investigations, and a named owner with contact details. A plan that lives only in one clinician's memory is a plan at risk of being lost. [2]
Investigations
The antenatal investigations that most refine the paediatric plan are the fetal echocardiogram, the detailed anomaly and growth ultrasound, fetal MRI where the anatomy is complex, and chromosomal microarray or gene-panel testing when a genetic cause is plausible. Each answers a different planning question. [1] [2]
A fetal echocardiogram defines the cardiac lesion, its ductal dependence, and the planned surgical strategy. It is also indicated for many non-cardiac anomalies, because associated cardiac lesions change both prognosis and place-of-delivery planning. A fetus with a diaphragmatic hernia, an omphalocele, or a recognised syndrome should have a fetal echo as part of the work-up. [1] [18]
Fetal MRI is preferred over ultrasound when the anatomy is complex or airway risk must be mapped — for a cervical mass being considered for EXIT, or a diaphragmatic hernia where lung-volume estimation refines prognosis. It does not replace ultrasound; it extends it where the question demands. [2]
Chromosomal microarray detects submicroscopic copy-number variants a conventional karyotype misses and is preferred when a structural anomaly is present. Gene-panel or exome testing is added when a syndrome is suspected. Be prepared to discuss variants of uncertain significance, which are real findings whose clinical meaning is not yet known; involve clinical genetics and, where appropriate, offer parental testing rather than over-interpreting. A normal result does not exclude single-gene disease. [10] [18]
Postnatal investigations should be pre-booked, not improvised. For a cardiac lesion, a postnatal echocardiogram and the prostaglandin-weaning strategy. For a diaphragmatic hernia, chest imaging, an echocardiogram for pulmonary hypertension, and baseline blood gases. For an omphalocele, a karyotype and a cardiac echo alongside the surgical plan. For a CNS diagnosis, a baseline neurology and developmental assessment. Pre-booking is what turns a plan into an executed plan. [7] [20]
Fetal anaemia, detected by raised middle cerebral artery peak systolic velocity, demands its own pathway: identifying the cause (alloimmune, parvovirus, genetic), and where indicated arranging intrauterine transfusion and planning the timing and place of delivery. [17]
Management — Resuscitation
The resuscitation phase is where planning most visibly pays off. For a time-critical diagnosis, the first minutes are not the time to discover the plan — they are the time to execute one already written. [1]
For a ductal-dependent cardiac lesion, the immediate bundle is warmth, commencement of a prostaglandin E1 infusion, avoidance of both hypoxia and hyperoxia by titrating oxygen to the saturation target, and delivery at a centre with cardiac capability where an echocardiogram can confirm the lesion and guide the staged strategy. The single most common preventable catastrophe is ductal closure before prostaglandin is running, which is precisely what antenatal diagnosis exists to prevent. [1] [19]
For a congenital diaphragmatic hernia, the immediate bundle is avoidance of mask ventilation that inflates the intrathoracic stomach-bowel, early endotracheal intubation, gastric decompression, and gentle ventilation to limit barotrauma and pulmonary hypertension. The baby is delivered where a high-level NICU can manage pulmonary hypertension, because the right lower- or upper-lobe pulmonary arteries and the vascular reactivity determine survival. [7] [8]
For gastroschisis, the immediate bundle is to protect and cover the exposed bowel with a clean sterile covering and a bowel bag, maintain temperature and hydration, keep the baby nil by mouth, and alert the surgical team. Analgesia and a nasogastric tube for decompression are part of the early care. The bowel is fragile, and rough handling or delay converts a manageable problem into a surgical emergency. [9]
For a predicted airway obstruction, the EXIT procedure secures the airway on placental support — uterine relaxation preserves placental gas exchange while the team intubates, bronchoscopes, or performs a tracheostomy before dividing the cord. This demands a coordinated obstetric, anaesthetic, airway and neonatal team briefed in advance; it cannot be improvised. [2]
For a preterm or growth-restricted planned delivery, antenatal corticosteroids for fetal lung maturation and, at very preterm gestations, magnesium sulfate for fetal neuroprotection enter the bundle, both gated by gestational age. Deferred cord clamping is favoured at preterm gestations where it can be achieved without compromising thermoregulation or the need for immediate resuscitation. [3] [5] [14] [15]
When the planned centre lacks the capability the diagnosis demands, the resuscitation question becomes retrieval: stabilise, then move to the right place, with a named service, a timeframe, and a backup contact. Optimism about local capability is not a plan. [2]
Management — Definitive & Stepwise
1. Confirm the diagnosis and judge time-criticality
Review the report, the imaging and the karyotype. Separate a confirmed structural finding from an uncertain variant. Then ask the single question that orders everything else: is this condition dangerous at birth? [1] [2]
2. Convene the multidisciplinary team
A planning meeting brings together maternal-fetal medicine, neonatology, paediatric surgery, cardiology, genetics and allied health. The output is a shared decision on place, time and capability of delivery, recorded where every clinician who will touch the case can see it. [2]
3. Ductal-dependent cardiac lesion
Deliver at a cardiac-capable centre with prostaglandin E1 ready. Plan the staged surgical strategy — the Norwood or hybrid for hypoplastic left heart, the appropriate repair for coarctation or pulmonary atresia — and the neurodevelopmental follow-up that survivors of congenital heart disease need. [1] [19] [20]
4. Congenital diaphragmatic hernia
Deliver at a tertiary NICU. Use early intubation, gastric decompression and gentle ventilation; manage pulmonary hypertension; and time surgical repair after stabilisation rather than as an emergency. Standardised postnatal CDH protocols improve survival. [7] [8]
5. Gastroschisis and omphalocele
For gastroschisis, plan surgical-team readiness, bowel protection, and either primary closure or a silo with staged reduction. For omphalocele, add chromosomal and cardiac work-up and, for giant lesions, staged closure. The two are not interchangeable. [9] [18]
6. Neural tube defect
Decide site of delivery, plan neurosurgical timing, and coordinate bladder, bowel and mobility services. Discuss the MOMS-trial context for prenatal repair when the family is seen at a fetal-surgery centre, including the benefits (improved hindbrain herniation, reduced shunt need) and the costs (prematurity, maternal morbidity). [6] [10] [13]
7. Congenital pulmonary airway malformation
A small asymptomatic lesion may be observed with postnatal imaging and elective resection. A large lesion with mediastinal shift or hydrops demands a centre ready for respiratory support and early surgical input. [11] [12]
8. Close the loop
After the planned delivery, coordinate developmental surveillance and a medical home. Pre-book the follow-up, name an owner, and give the family a safety-net for concerns. The loop does not close at discharge. [20]
Specific Subtypes & Scenarios
Hypoplastic left heart syndrome. The archetype of ductal dependence. Deliver at a cardiac centre with prostaglandin from birth, plan the staged surgical pathway (Norwood, Glenn, Fontan) or a hybrid in selected centres, and involve the family in the fetal-intervention discussion when a critical aortic stenosis is evolving toward HLHS. Neurodevelopmental follow-up is mandatory. [1] [19]
Congenital diaphragmatic hernia with predicted severe pulmonary hypoplasia. Plan a tertiary NICU, gentle ventilation from the first breath, pulmonary-hypertension management, and delayed surgical repair after stabilisation. Fetal endoscopic tracheal occlusion is considered in selected severe cases at specialist centres. [7] [8]
Gastroschisis versus omphalocele. Gastroschisis: bowel protection, surgical team, silo or primary closure, and a feeding and length-of-stay expectation set early. Omphalocele: chromosomal and cardiac work-up, distinction of giant from small lesions, and staged closure for the former. Never plan them identically. [9] [18]
Cervical mass with predicted airway obstruction. The EXIT scenario. Secure the airway on placental support with an obstetric, anaesthetic, airway and neonatal team briefed in advance, then divide the cord. Planning is everything; the airway cannot wait for improvisation. [2]
Myelomeningocele. Plan neurosurgical timing, coordinate bladder, bowel and mobility services, and discuss prenatal versus postnatal repair with reference to the MOMS trial. The general paediatrician coordinates the medical home and developmental surveillance. [6] [10] [13]
Large congenital pulmonary airway malformation. A lesion with mediastinal shift or hydrops needs a centre ready for respiratory support and early surgical input; a small asymptomatic lesion can be observed and electively resected. [11] [12]
Fetal growth restriction with absent end-diastolic flow at very preterm gestation. The Doppler guides surveillance and delivery timing; antenatal corticosteroids and magnesium for neuroprotection are gated by gestation; plan a NICU and deferred cord clamping where feasible. [3] [4] [5] [14]
Fetal hydrops of unknown cause. Work through immune, cardiac, anaemic, infectious, metabolic and genetic causes; the postnatal plan depends entirely on the cause, so involve fetal medicine, genetics and neonatology together. [17]
Twin pregnancy with an anomaly in one fetus. Chorionicity drives everything. A monochorionic complication or a discordant anomaly raises specific ethical and management questions that demand specialist fetal-medicine input. [2]
Diagnosis confirmed but severity uncertain. Counsel honestly that the functional outcome may be better or worse than predicted, build surveillance to respond, and avoid over-promising. Residual uncertainty is the rule, not the exception. [10] [19]
Complications & Pitfalls
The most feared complications are the very events planning exists to prevent. Ductal closure before prostaglandin in an unanticipated ductal-dependent lesion produces cardiovascular collapse and organ injury. Mask ventilation of a diaphragmatic hernia inflates the intrathoracic bowel and worsens respiratory failure. Delayed bowel protection in gastroschisis causes hypothermia, fluid loss and bowel ischaemia. Each is a failure to convert a known diagnosis into an executable resuscitation plan. [1] [7] [9]
A subtler pitfall is treating omphalocele like gastroschisis and missing its chromosomal and cardiac associations, which then surface unanticipated after birth. The same logic applies to any lesion — a normal karyotype does not exclude single-gene disease, and a structurally isolated finding may still be syndromic. [10] [18]
Team and documentation failures are quietly catastrophic. A planned delivery where the surgical or cardiac team was not actually briefed, or where an on-call team faces an EXIT-level airway problem it did not know was coming, is a planning failure dressed up as a clinical emergency. A written neonatal plan that is lost between sites or shifts produces the same harm as no plan at all. [2]
Counselling failures are planning failures too. Over-promising a prognosis when functional severity is unknowable before birth damages trust and corrodes the therapeutic relationship. Forgetting the family's values and support — or, worse, imposing a single outcome narrative — is not neutral; it is poor care. Honest, non-directive counselling that holds open uncertainty is the standard. [2] [20]
Prognosis & Disposition
Prognosis after an antenatal diagnosis is shaped by four things: the diagnosis itself, its associated anomalies and karyotype, the gestational age at delivery, and the completeness of the plan. A diagnosis is fixed; the preparedness and the gestation are not, which is why the same condition can carry very different outcomes depending on whether the loop closed. [1] [2]
Hypoplastic left heart syndrome, once nearly universally fatal, now carries a staged-surgery survival that would have been unimaginable a generation ago — but it depends on the staged strategy being executed, which depends in turn on antenatal diagnosis and a cardiac-centre delivery. Congenital diaphragmatic hernia stratifies sharply by predicted lung volume and pulmonary-hypertension severity; standardised postnatal protocols improve survival, which is why a prepared tertiary NICU matters. [1] [7] [19]
The MOMS trial changed the prognosis for myelomeningocele: prenatal repair improved hindbrain herniation and reduced the need for a ventricular shunt, at the cost of prematurity and maternal morbidity. Gastroschisis with modern neonatal and surgical care has a favourable prognosis in most cases, provided the bowel is protected and the surgical pathway is smooth. [6] [9] [13]
Disposition is "plan owned, loop closed, surveillance open." A delivery-critical diagnosis goes home only with a documented multidisciplinary plan, a neonatal alert executed, and pre-booked follow-up. A surveillance-only diagnosis goes home with routine care and an open door. In both, the paediatrician holds the medical-home role, coordinating the disease-specific and developmental follow-up that carries the loop beyond birth. [20]
Residual uncertainty after a normal karyotype is real and must be counselled honestly. Structural and single-gene disease can persist, and neurodevelopmental outcomes — especially after congenital heart disease — are tracked over years, not days. The safety-net ensures a family returns if concerns arise. [10] [20]
Special Populations
Adolescent, advanced-maternal-age and assisted-reproduction pregnancies each carry different counselling weights and different likelihoods of a syndromic rather than isolated finding. Pre-test probability differs, and so does the family's readiness to make decisions under pressure. [1]
Cultural safety changes whether a plan is completed. Indigenous, Māori, Pacific, migrant, refugee and asylum-seeking families need interpreter-supported counselling at the moment of the diagnosis and the planning meeting, not a translated letter days later, and care that respects family decision-making structures. [2]
Rurality and remoteness change place-of-delivery and retrieval planning most of all. A diagnosis that demands a tertiary centre may be hours of retrieval away, and the plan must account for real travel times, weather, and the capability at the referring site rather than an idealised map. Socioeconomic disadvantage and out-of-home care reduce plan completion and follow-up; identify these barriers early and design the pathway around them. [2]
Consanguinity and known familial genetic conditions move the conversation toward targeted genetic testing and recurrence counselling, ideally before a future pregnancy. Families connected to Deaf or disability communities may frame outcomes differently from clinicians, and good care is accurate information delivered without ableism. A multiple pregnancy with an affected fetus raises the ethics of discordant outcomes and the technical complexities of chorionicity, and demands specialist fetal-medicine input. [10] [18]
Maternal chronic disease — pre-gestational diabetes, autoimmune disease, anticonvulsant therapy — interacts with the fetal diagnosis and the planning, sometimes as a cause and sometimes as a compounding factor. A history of infertility or prior loss adds emotional weight to every counselling visit, and a young person without a supportive adult needs structured support through decisions and consent. [2]
Evidence, Guidelines & Regional Differences
The MOMS trial (Adzick 2011) established that prenatal myelomeningocele repair improves hindbrain herniation and reduces shunt need, with the full-cohort 30-month paediatric outcomes confirming the benefit and quantifying the costs. It is the landmark that brought fetal surgery for spina bifida from experiment to selected practice, performed at specialist centres. [6] [13]
The American Heart Association scientific statement on fetal cardiac disease (Donofrio 2014) sets the framework for antenatal cardiac diagnosis, counselling and the planning of place and capability of delivery for ductal-dependent lesions. It underpins why prostaglandin readiness and cardiac-centre delivery are the standard. [1]
The Cochrane review of antenatal corticosteroids (McGoldrick 2020) and the updated Cochrane review of magnesium sulfate for fetal neuroprotection (Shepherd 2024) anchor the gestation-gated bundle when delivery timing is brought forward. The Seidler 2023 individual-participant-data network meta-analysis informs deferred cord clamping at preterm birth, weighed against the thermoregulation trade-off. [5] [14] [15]
Standardised postnatal CDH protocols (Snoek 2016) and the CDH-associated pulmonary-hypertension review (Holden 2024) shape the NICU management that turns a planned delivery into a survivor. The ERNICA consensus on esophageal atresia (Dingemann 2020) standardises perioperative management, and the omphalocele prenatal-diagnosis study (Conner 2018) quantifies how prenatal detection changes outcomes. [7] [8] [16] [18]
Controversies remain in fetal intervention. Fetal aortic valvuloplasty for evolving hypoplastic left heart (Tulzer 2022) and fetal endoscopic tracheal occlusion for severe CDH are performed at specialist centres in selected cases, with real benefits and real risks; the general paediatrician's role is to refer appropriately and counsel honestly, not to offer the intervention. [8] [19]
Australia and Aotearoa New Zealand plan perinatal care through neonatal networks with defined capability tiers and retrieval services; quote the local network's place-of-delivery and retrieval policy rather than an idealised map. [2]
United Kingdom uses managed clinical networks for fetal and neonatal care, with defined referral pathways for surgical and cardiac diagnoses through specialist centres. [2]
United States and Canada follow AAP, ACOG and CPS guidance; operational detail on capability, retrieval and place of delivery varies by region, institution and insurer. [1]
State only differences you have verified against current official perinatal-network guidance. Do not invent a fixed operative window or a universal prostaglandin protocol. [7]
Exam Pearls
- The paediatrician's antenatal role is to translate a prenatal diagnosis into a postnatal plan — place, time and capability of delivery. [2]
- A ductal-dependent circulation collapses when the duct closes; antenatal diagnosis enables prostaglandin E1 before collapse. [1]
- Do not mask-ventilate a diaphragmatic hernia — intubate early, decompress the stomach, ventilate gently. [7]
- Gastroschisis is right-sided, no sac, normal cord, usually isolated; omphalocele is midline, with a sac, and carries chromosomal and cardiac associations. [9] [18]
- An EXIT procedure secures the airway on placental support before cord division for a predicted airway obstruction. [2]
- The MOMS trial showed benefit of prenatal myelomeningocele repair for hindbrain herniation and shunt need, at the cost of prematurity and maternal morbidity. [6] [13]
- A normal karyotype does not exclude structural or single-gene disease. [10]
- Antenatal corticosteroids and magnesium for neuroprotection are gated by gestational age when delivery is brought forward. [5] [14]
- Name an owner and write the neonatal alert so the plan survives shift and site changes. [2]
- Residual uncertainty is the rule — counsel honestly and keep developmental surveillance open. [20]
PLAN-IT package
References
- [1]Donofrio MT, Moon-Grady AJ, Hornberger LK, et al. Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American Heart Association. Circulation, 2014.PMID 24763516
- [2]Benachi A, Sarnacki S. Prenatal counselling and the role of the paediatric surgeon. Seminars in pediatric surgery, 2014.PMID 25459006
- [3]Lees CC, Romero R, Stampalija T, et al. Clinical Opinion: The diagnosis and management of suspected fetal growth restriction: an evidence-based approach. American journal of obstetrics and gynecology, 2022.PMID 35026129
- [4]American College of Obstetricians and Gynecologists. Fetal Growth Restriction: ACOG Practice Bulletin, Number 227. Obstetrics and gynecology, 2021.PMID 33481528
- [5]McGoldrick E, Stewart F, Parker R, et al. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. The Cochrane database of systematic reviews, 2020.PMID 33368142
- [6]Adzick NS, Thom EA, Spong CY, et al. A randomized trial of prenatal versus postnatal repair of myelomeningocele. The New England journal of medicine, 2011.PMID 21306277
- [7]Snoek KG, Reiss IK, Greenough A, et al. Standardized Postnatal Management of Infants with Congenital Diaphragmatic Hernia. Neonatology, 2016.PMID 27077664
- [8]Holden KI, Rintoul NE, McNamara PJ, et al. Congenital diaphragmatic hernia-associated pulmonary hypertension. Seminars in pediatric surgery, 2024.PMID 39018718
- [9]Bhat V, Moront M, Bhandari V. Gastroschisis: A State-of-the-Art Review. Children (Basel), 2020.PMID 33348575
- [10]Copp AJ, Adzick NS, Chitty LS, et al. Spina bifida. Nature reviews. Disease primers, 2015.PMID 27189655
- [11]Leblanc C, Baron M, Desselas E, et al. Congenital pulmonary airway malformations: state-of-the-art review for paediatricians. European journal of pediatrics, 2017.PMID 29046943
- [12]David M, Lamas-Pinheiro R, Henriques-Coelho T, et al. Prenatal and Postnatal Management of Congenital Pulmonary Airway Malformation. Neonatology, 2016.PMID 27070354
- [13]Farmer DL, Thom EA, Brock JW 3rd, et al. The Management of Myelomeningocele Study: full cohort 30-month pediatric outcomes. American journal of obstetrics and gynecology, 2018.PMID 29246577
- [14]Shepherd ES, Goldsmith S, Doyle LW, et al. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. The Cochrane database of systematic reviews, 2024.PMID 38726883
- [15]Seidler AL, Aberoumand M, Hunter KE, et al. Deferred cord clamping, cord milking, and immediate cord clamping at preterm birth: a systematic review and individual participant data network meta-analysis. Lancet, 2023.PMID 37977169
- [16]Dingemann C, Eaton S, Aksnes G, et al. ERNICA Consensus Conference on the Management of Patients with Esophageal Atresia and Tracheoesophageal Fistula: Diagnosis, Preoperative, Operative and Postoperative Management. European journal of pediatric surgery, 2020.PMID 31266084
- [17]Prefumo F, Fichera A, Fratelli N, et al. Fetal anemia: Diagnosis and management. Best practice & research. Clinical obstetrics & gynaecology, 2019.PMID 30718211
- [18]Conner P, Vejde JH, Burgos CM, et al. Accuracy and impact of prenatal diagnosis in infants with omphalocele. Pediatric surgery international, 2018.PMID 29637257
- [19]Tulzer A, Huhta JC, Hochpoechl A, et al. Hypoplastic Left Heart Syndrome: Is There a Role for Fetal Therapy? Frontiers in pediatrics, 2022.PMID 35874565
- [20]Martinez-Biarge M, Jowett VC, Cowan FM, et al. Neurodevelopmental outcome in children with congenital heart disease. Seminars in fetal & neonatal medicine, 2013.PMID 23706956