Paeds · growth-development-and-behaviour
Hearing impairment and development
Also known as Permanent childhood hearing impairment · Childhood deafness · Sensorineural hearing loss children · Conductive hearing loss development · Auditory neuropathy spectrum disorder · Cochlear implant paediatric development · Otitis media with effusion hearing · Hard of hearing child
Fellowship-level approach to childhood hearing impairment and development: permanent versus temporary loss, classification, critical-period language effects, early amplification and cochlear implants, OME, family-centred intervention, and regional practice differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Hearing links the child to language, learning and social connection. Permanent childhood hearing impairment (PCHI) is uncommon relative to otitis media, but its developmental stakes are high: delayed access to a clear language signal costs months of neural and communicative development that are hard to recover fully. Your role as a general paediatrician is to suspect, confirm, protect language access, coordinate specialists, and support the family — not to run every audiology booth yourself. [1] [3] [7]
Permanent childhood hearing impairment means lasting reduction in hearing thresholds that is not expected to resolve with simple middle-ear clearance alone. Temporary conductive loss is often due to otitis media with effusion (OME) or wax and may still harm language if prolonged or recurrent. Deaf or hard of hearing (D/HH) is the person-first community language many families prefer; use the family’s terms. Newborn screening pathways are detailed on the dedicated newborn hearing screening topic — this page owns developmental impact and ongoing paediatric management after confirmation or later presentation. [1] [3]
Classification
Organise every case on four axes: type, laterality, severity, and onset/trajectory. Those axes drive urgency, device choice and educational supports. [3] [7]
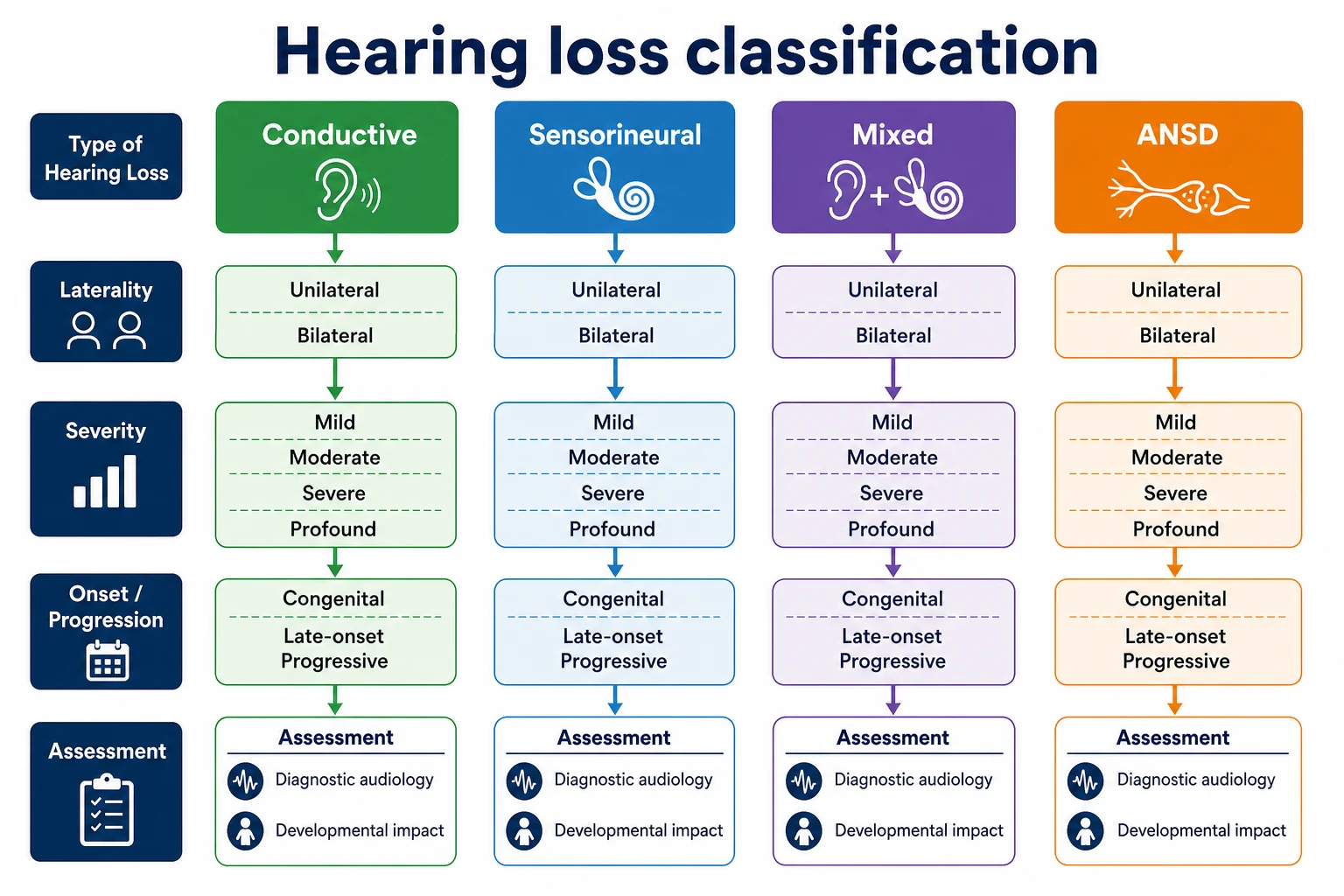
| Axis | Categories that change care |
|---|---|
| Type | Conductive · sensorineural · mixed · ANSD (neural dyssynchrony) |
| Laterality | Unilateral · bilateral |
| Severity | Mild · moderate · severe · profound (use local audiology bands) |
| Onset | Congenital · delayed-onset · progressive · acquired (e.g. meningitis) |
Screening refer versus diagnosis. A newborn or school screen that refers means “needs diagnostic audiology,” not “is deaf.” Counselling before confirmation must stay provisional. [1]
Epidemiology & Risk Factors
Questionnaire-based UK ascertainment showed permanent childhood hearing impairment is more prevalent than older estimates assumed once progressive and later-identified cases are counted — a core argument for universal newborn screening plus ongoing vigilance. Exact percentages vary by definition and age; quote local epidemiology in viva rather than a single global number. [7]
High-yield risk clusters: family history of childhood hearing loss; craniofacial anomalies; NICU/ECMO/ototoxic exposure; congenital infection (especially CMV); syndromes; bacterial meningitis; recurrent OME; neurodegenerative or storage disease with progressive loss. [3] [7]
School-entry hearing screens have limited accuracy and cost-effectiveness in some health-technology assessments; they never replace clinical suspicion or EHDI follow-up discipline. [12]
Pathophysiology
Spoken language networks expect timely, consistent auditory input. Prolonged deprivation or a poor signal-to-noise ratio during critical early years alters the efficiency of speech perception and language learning. That is why programme design pushes early confirmation and early intervention. [1] [2] [5]
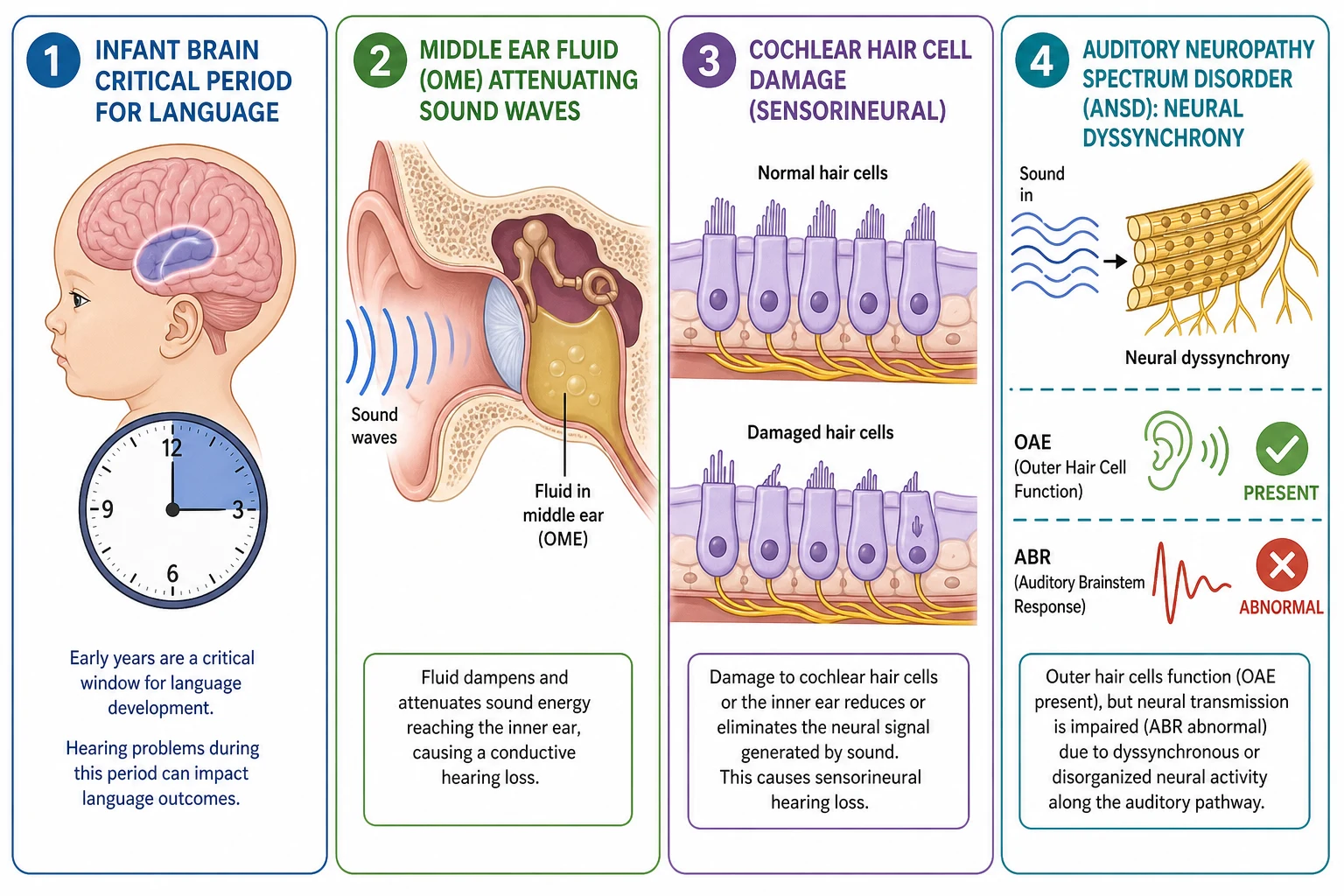
Conductive loss reduces effective loudness (wax, OME, ossicular problems). Sensorineural loss reflects cochlear or neural pathway injury. ANSD disrupts temporal coding; otoacoustic emissions may be present while ABR is abnormal — a classic trap if only OAE-based thinking is used after the newborn period. [3] [11]
OME fills the middle ear with fluid, damping transmission. Even when thresholds look “only mild,” classroom noise multiplies the functional handicap. [9]
Clinical Presentation
Parents may report not startling to noise, delayed babble-to-words transition, unclear speech, saying “what?” often, loud media volume, or behaviour problems when listening load is high. Teachers notice daydreaming in noise or falling behind phonics. [2] [8]
Classic examiner patterns: [1] [3]
- Infant after newborn refer without completed diagnostics
- Toddler with language delay and normal motor milestones
- Preschooler with recurrent OME and fluctuating attention
- School-age child with “selective hearing” that is actually bilateral mild loss
- Post-meningitis recovery with new hearing concerns
- Progressive CMV-related loss after an early pass
Never accept “it is just bilingualism” as a reason to skip audiology when language is delayed. [2]
Differential Diagnosis
| Presentation | Hearing-favouring clues | Key alternatives |
|---|---|---|
| Language delay | Risk factors, screen history, unclear speech | Primary DLD, autism, ID, neglect of language input |
| Inattention | Worse in noise, loud TV, ear findings | ADHD, sleep disorder, learning disorder |
| Social communication concern | Concurrent language delay, device non-use | Autism spectrum (can coexist with hearing loss) |
| Fluctuating school performance | Seasonal colds, flat tympanograms | Attendance, anxiety, specific learning disorder |
Hearing loss and neurodevelopmental conditions coexist. Diagnosing one never excuses missing the other. [2]
Clinical & Bedside Assessment
Open with partnership: “We always check hearing when speech or school listening is hard, because treatable barriers are easy to miss.” [3]
Five-minute hearing–development assessment
Screen and risk history
Newborn screen result, NICU, family history, CMV risk, meningitis, ototoxins, craniofacial features.
Communication milestones
Babble, first words, phrases, speech clarity, home languages, parent concern.
Listening behaviour
Name response, TV volume, classroom noise, localisation, fatigue after school.
Ear examination
Canals, drums, effusion clues, pits/tags, microtia.
Function and devices
If already aided/implanted: hours of use, feedback, school supports.
Plan and teach-back
Book audiology urgency, interim communication tips, who owns follow-up.
Observe how the child responds to quiet speech versus gesture. Document developmental status fully — hearing care sits inside whole-child developmental surveillance. [2]
Investigations
Diagnostic audiology is the decision test. Age-appropriate methods include diagnostic ABR/ASSR in infants, visual reinforcement and play audiometry in toddlers/preschoolers, and pure-tone plus speech testing in older children, with tympanometry and OAEs as adjuncts. [3]
Read reports for: type, laterality, severity, reliability, speech perception if available, and recommended next step. If the report is unclear, call the audiologist — do not guess. [3]
Aetiology evaluation is individualised: congenital CMV timing strategies, genetics, imaging, ophthalmology and related tests when indicated by history and local protocols. Sequence them so they do not block amplification. [3]
For OME, combine otoscopy/tympanometry with hearing thresholds and developmental impact when deciding on watchful waiting versus surgical referral under guideline frameworks. [9]
Management — Resuscitation
Bacterial meningitis: treat infection first, then secure urgent audiology because hearing can decline rapidly and cochlear ossification can close implant windows. Escalate ENT/implant pathways early when loss is confirmed. [3] [4]
Sudden sensorineural hearing loss and complicated mastoid disease are ENT emergencies — medical stabilisation plus specialist review, not watchful waiting in clinic. [3]
Management — Definitive & Stepwise
The developmental ladder is simple to state and hard to execute without a team. [3] [10]
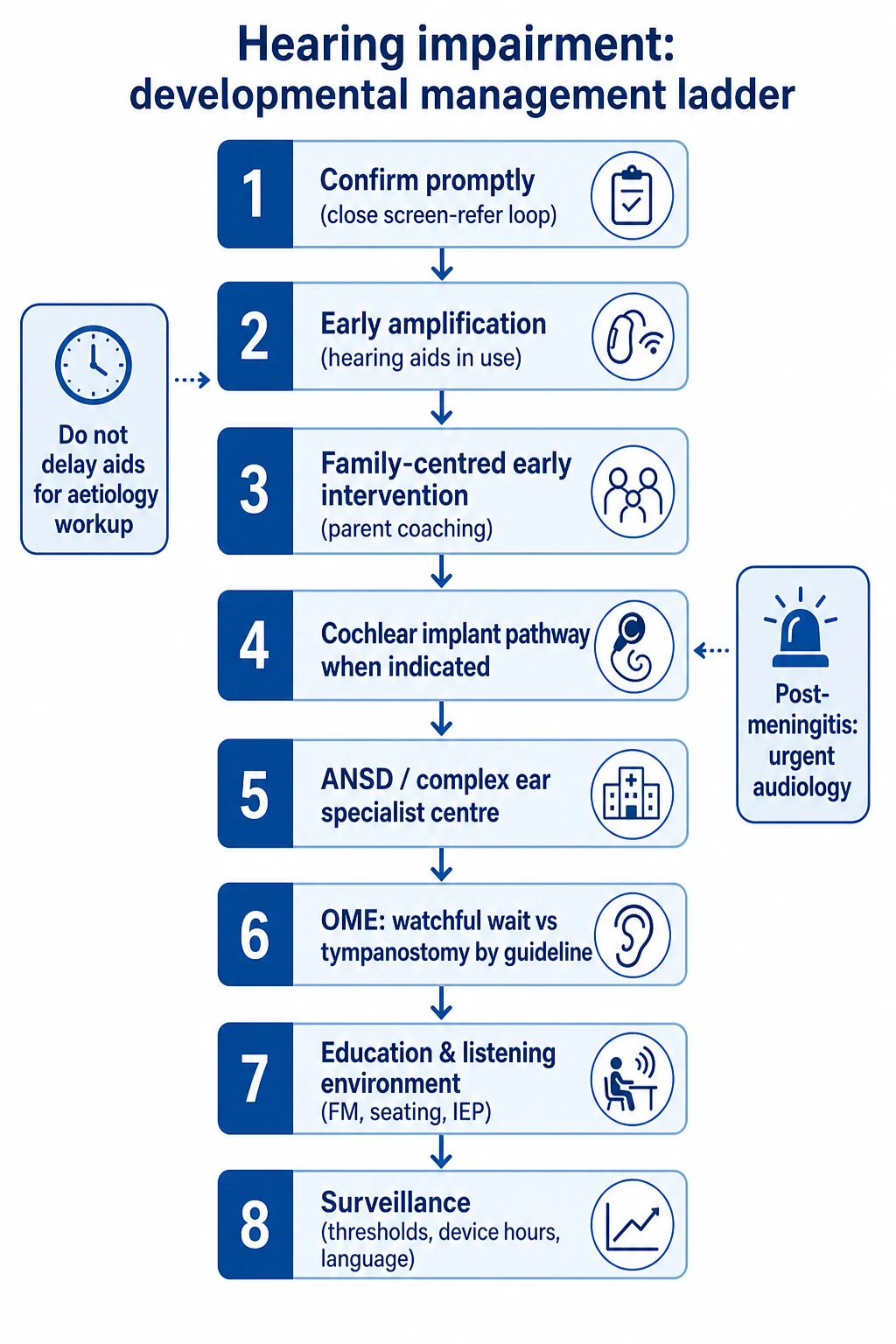
1. Confirm promptly. Close the loop after any refer or clinical suspicion. Own lost-to-follow-up as a system failure you help fix. [1]
2. Early amplification for permanent bilateral loss. Hearing aids fitted and used — not merely dispensed — are the default first step unless candidacy immediately points to implant pathways. [3] [5]
3. Family-centred early intervention. Parent talk quantity and quality, coaching, and structured early intervention associate with pragmatic language gains. Device without family support underperforms. [2] [10]
4. Cochlear implant pathway when indicated. Prospective multicentre data (CDaCI) showed spoken language trajectories after implantation related to age and baseline factors — earlier implantation generally supports better spoken language growth in appropriate candidates. Ongoing cohort work links preschool speech-in-noise skills to later language. Exact eligibility is programme-specific. [4] [6]
5. ANSD and complex ears. Outcomes after CI can differ by neural integrity; counsel uncertainty and use specialist centres. [11]
6. OME management. Updated tympanostomy tube guidance emphasises appropriate candidates — recurrent/persistent OME with hearing impact and developmental risk, not tubes for every cold. Align with local NICE/AAP-style frameworks. [9]
7. Education and environment. Preferential seating, remote microphone/FM systems, acoustic classroom measures, captioning, and individual education plans. Mild/unilateral loss still deserves a written listening plan. [8]
8. Surveillance. Recheck thresholds if speech stalls, after meningitis, with CMV risk, and whenever device use falls. Support adolescent identity and transition. [3]
What each intervention actually achieves
- Restores usable acoustic access
- Enables spoken language practice
- Fails if hours-of-use are low
- Builds parent–child communication
- Supports any modality choice with information
- Addresses stress and advocacy skills
- Option for severe-profound candidates
- Timing influences spoken language growth
- Needs lifelong mapping and support
Specific Subtypes & Scenarios
Bilateral congenital severe–profound SNHL. Fast diagnostic confirmation, early aids as bridge, implant team referral, intensive early intervention. [4] [5]
Unilateral permanent loss. Localisation and noise listening are hard; school plan and monitoring of the better ear are essential. [8]
Slight-to-mild bilateral loss. Do not dismiss. Population data link later academic and quality-of-life impacts; optimise classroom listening and review thresholds. [8]
OME-heavy preschooler. Document duration, hearing, speech, and development; apply tube guidelines rather than reflexive surgery or endless “wait and see” without thresholds. [9]
Post-meningitis. Urgent audiology and early implant discussion if severe loss evolves. [3] [4]
Deaf child in a signing family. Respect language choice; ensure early rich language access (signed and/or spoken) and developmental surveillance without forcing a single modality ideology. [3] [10]
Complications & Pitfalls
Developmental complications include lasting language gaps, literacy risk, social isolation, and secondary behaviour labels. Device complications and surgical risks belong with ENT counselling. [2] [4]
Prognosis & Disposition
Children who receive earlier effective language access — through devices, rich parent input and early intervention — show better communication outcomes on average, though individual trajectories vary with additional disabilities, consistency of use and social determinants. [1] [2] [5]
Disposition is usually outpatient multidisciplinary care. Admit or urgently refer for acute ear complications, sudden loss, or post-meningitis pathways. Document the next audiology date and the named early-intervention contact. [3]
Special Populations
EHDI infants. Cross-link newborn screening for 1-3-6 clocks; this page owns what happens after confirmation for development. [1] [3]
Additional disabilities. Cognitive, motor or visual impairment changes test choice and intervention design — still prioritise communication access. [2]
Rural and disadvantaged families. Travel, device batteries, and appointment cascades drive inequity; tele-audiology and local champions help. [3]
Indigenous and multilingual families. Use interpreters, cultural brokers and materials in home languages; never equate non-English home language with neglect of speech therapy need. [10]
Evidence, Guidelines & Regional Differences
Anchors include Yoshinaga-Itano’s programme and early-intervention language work, JCIH early-intervention principles after confirmation, Niparko’s CDaCI spoken-language study, Ching’s UNHS/early-intervention and cochlear-implant language analyses, Fortnum’s UK prevalence study, Wang’s mild-loss population outcomes, Rosenfeld’s tympanostomy guideline update, and family-centred early intervention structure principles. [1] [2] [3] [4] [5] [6] [7] [8] [9] [10]
Universal newborn screening is standard in Australia and Aotearoa New Zealand with local audiology and implant networks. Use national/state EHDI targets and NICE-adjacent OME thinking where adopted; quote local CI criteria rather than US labels. Equity for rural and Māori/Pacific/Aboriginal families is a core viva theme. [1] [5]
Controversies. Optimal CI age continues to move earlier for many candidates; communication modality debates require informed family choice, not clinician ideology; school-entry screens are not a substitute for clinical pathways. [4] [5] [12]
Exam Pearls
HEARWELL
If you remember only one chain: undetected or untreated hearing loss → degraded language input in a critical window → preventable communicative disability. Your job is to open the language pathway early and keep it open. That is the fellowship answer. [1] [2] [4]
References
- [1]Yoshinaga-Itano C Outcomes of Universal Newborn Screening Programs: Systematic Review. Journal of clinical medicine, 2021.PMID 34202909
- [2]Yoshinaga-Itano C Early Intervention, Parent Talk, and Pragmatic Language in Children With Hearing Loss. Pediatrics, 2020.PMID 33139440
- [3]Joint Committee on Infant Hearing of the American Academy of Pediatrics Supplement to the JCIH 2007 position statement: principles and guidelines for early intervention after confirmation that a child is deaf or hard of hearing. Pediatrics, 2013.PMID 23530178
- [4]Niparko JK Spoken language development in children following cochlear implantation. JAMA, 2010.PMID 20407059
- [5]Ching TYC Considering the impact of Universal Newborn Hearing Screening and early intervention on language outcomes for children with congenital hearing loss. Hearing, balance and communication, 2020.PMID 34249584
- [6]Ching TYC Predicting 9-Year Language Ability from Preschool Speech Recognition in Noise in Children Using Cochlear Implants. Trends in hearing, 2022.PMID 36285469
- [7]Fortnum HM Prevalence of permanent childhood hearing impairment in the United Kingdom and implications for universal neonatal hearing screening: questionnaire based ascertainment study. BMJ (Clinical research ed.), 2001.PMID 11546698
- [8]Wang J Academic, behavioural and quality of life outcomes of slight to mild hearing loss in late childhood: a population-based study. Archives of disease in childhood, 2019.PMID 31079073
- [9]Rosenfeld RM Executive Summary of Clinical Practice Guideline on Tympanostomy Tubes in Children (Update). Otolaryngology--head and neck surgery, 2022.PMID 35138976
- [10]Szarkowski A Family-Centered Early Intervention Deaf/Hard of Hearing (FCEI-DHH): Structure Principles. Journal of deaf studies and deaf education, 2024.PMID 38422449
- [11]Jafari Z Pediatric Cochlear Implant Outcomes in Auditory Neuropathy, Cochlear Nerve Deficiency, and Sensorineural Hearing Loss: An 8-Year Longitudinal Study. Ear and hearing, 2026.PMID 42260698
- [12]Bamford J Current practice, accuracy, effectiveness and cost-effectiveness of the school entry hearing screen. Health technology assessment (Winchester, England), 2007.PMID 17683682