Paeds · growth-development-and-behaviour
Motor delay, hypotonia and the floppy infant
Also known as Floppy infant · Infantile hypotonia · Neonatal hypotonia · Low tone baby · Motor developmental delay · Central hypotonia · Peripheral hypotonia · Floppy baby syndrome
Fellowship approach to motor delay, hypotonia and the floppy infant: bedside localisation of central versus peripheral tone problems, can't-miss differentials including SMA and infant botulism, first-line investigations, airway and feeding protection, disease-modifying pathways and early intervention without cloning dedicated CP tool chapters.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Parents often say the baby feels like a rag doll. That sentence is a clinical starting gun, not a diagnosis. Hypotonia means reduced resistance to passive movement. Weakness means reduced active force. Joint hypermobility can mimic low tone if you never ask the infant to move against gravity. The floppy infant is the neonate or young infant in whom low tone dominates the first impression. Motor delay is the later story: rolling, sitting, crawling or walking arrive late, with or without ongoing low tone. [1] [3]
Your job is not to name every rare myopathy on day one. Your job is to answer four questions fast. Is the infant safe to breathe and feed? Is this central or peripheral? Is the course static, progressive or fluctuating? Which tests change management this week rather than decorate the chart? Modern reviews still start with that bedside logic, even as genome sequencing expands the diagnostic yield. [5] [6]
First five moves with a floppy infant
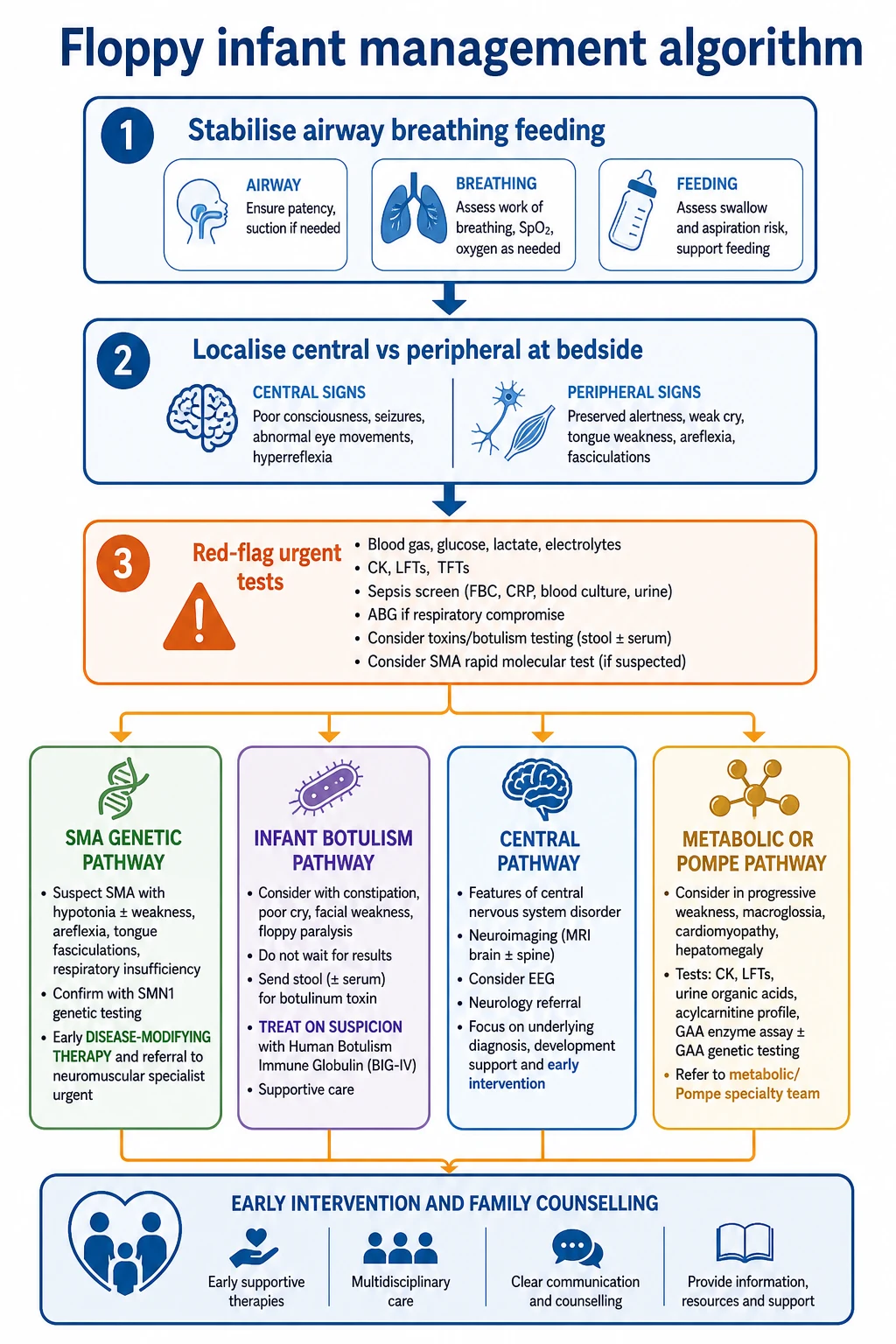
Protect airway and feeding
Assess work of breathing, cough, secretions, suck–swallow and aspiration risk before any long history.
Localise at the bedside
Separate central from peripheral using power, reflexes, antigravity posture and systemic clues.
Hunt can't-miss causes
SMA, infant botulism, congenital myotonic dystrophy, infantile Pompe, metabolic or encephalopathic disease.
Test with purpose
Choose first-line labs and genetics that match the phenotype; avoid endless observation if the phenotype is progressive.
Start supports early
Physiotherapy, feeding support, respiratory plan and specialist referral run in parallel with diagnosis.
Classification
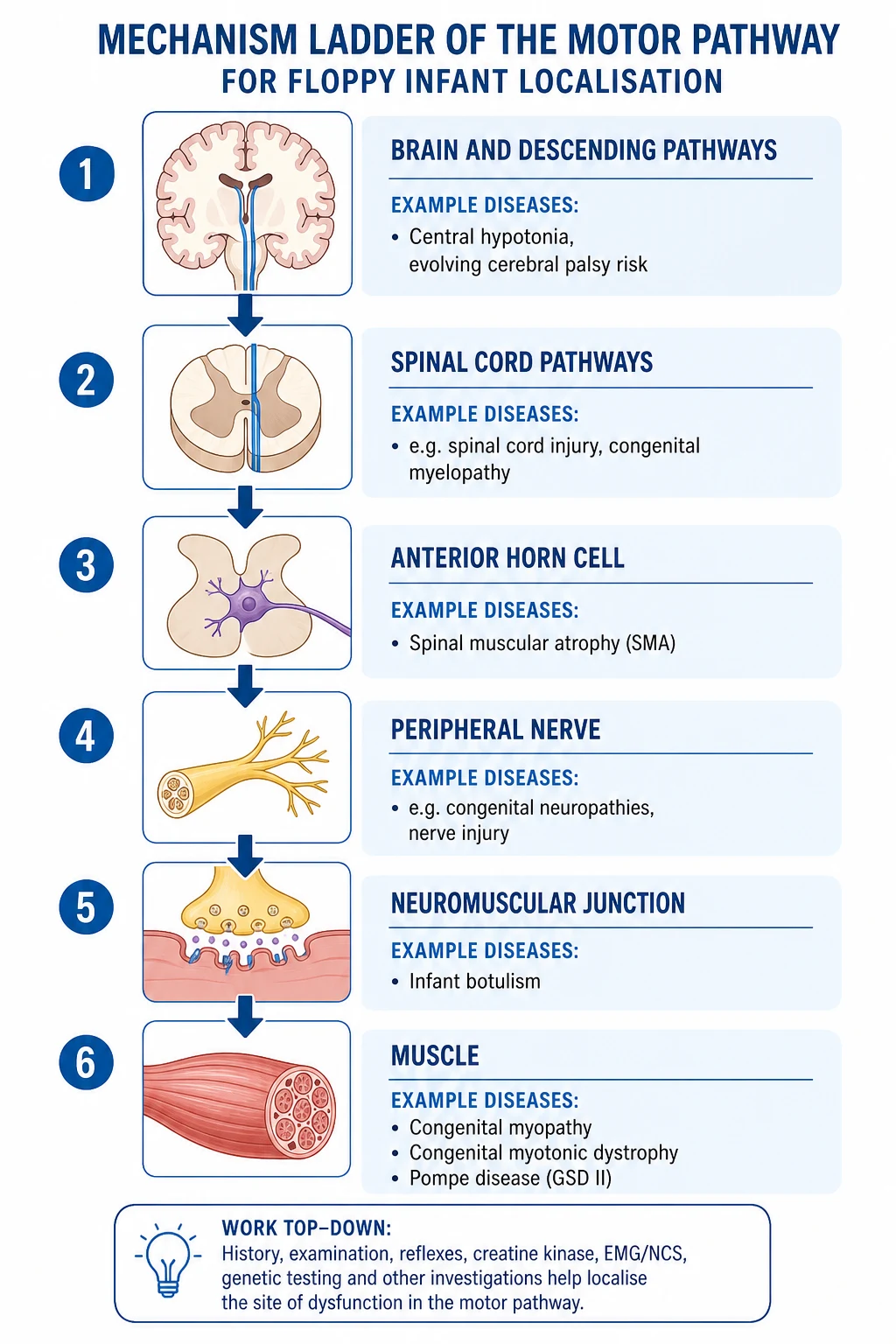
Start with pattern, not eponym. Central hypotonia arises from brain or spinal pathways above the anterior horn cell. Early on the infant may be floppy, but reflexes are often preserved and tone can later rise. Encephalopathy, seizures, microcephaly, dysmorphic features or a perinatal brain injury story push you here. Peripheral hypotonia arises from anterior horn cell, peripheral nerve, neuromuscular junction or muscle. These infants are weak. Antigravity movement fails. Reflexes are reduced or absent. Fasciculations, especially of the tongue, matter. [1] [2] [3]
Also classify by onset (congenital versus later infantile), tempo (static, progressive, fluctuating) and distribution (axial versus appendicular, bulbar versus limb). Motor delay without clear low tone is still a motor-domain problem, but the urgency ladder differs from a neonate who cannot handle secretions. Corrected age matters in preterm infants; calendar age alone misleads. [5] [19]
The phrase benign congenital hypotonia is a historical trap. It is not a safe final diagnosis while progressive neuromuscular, metabolic or syndromic disease remains possible. If you cannot yet name the cause, say “hypotonia, cause not yet established,” and keep the work-up and safety plan active. [2] [6]
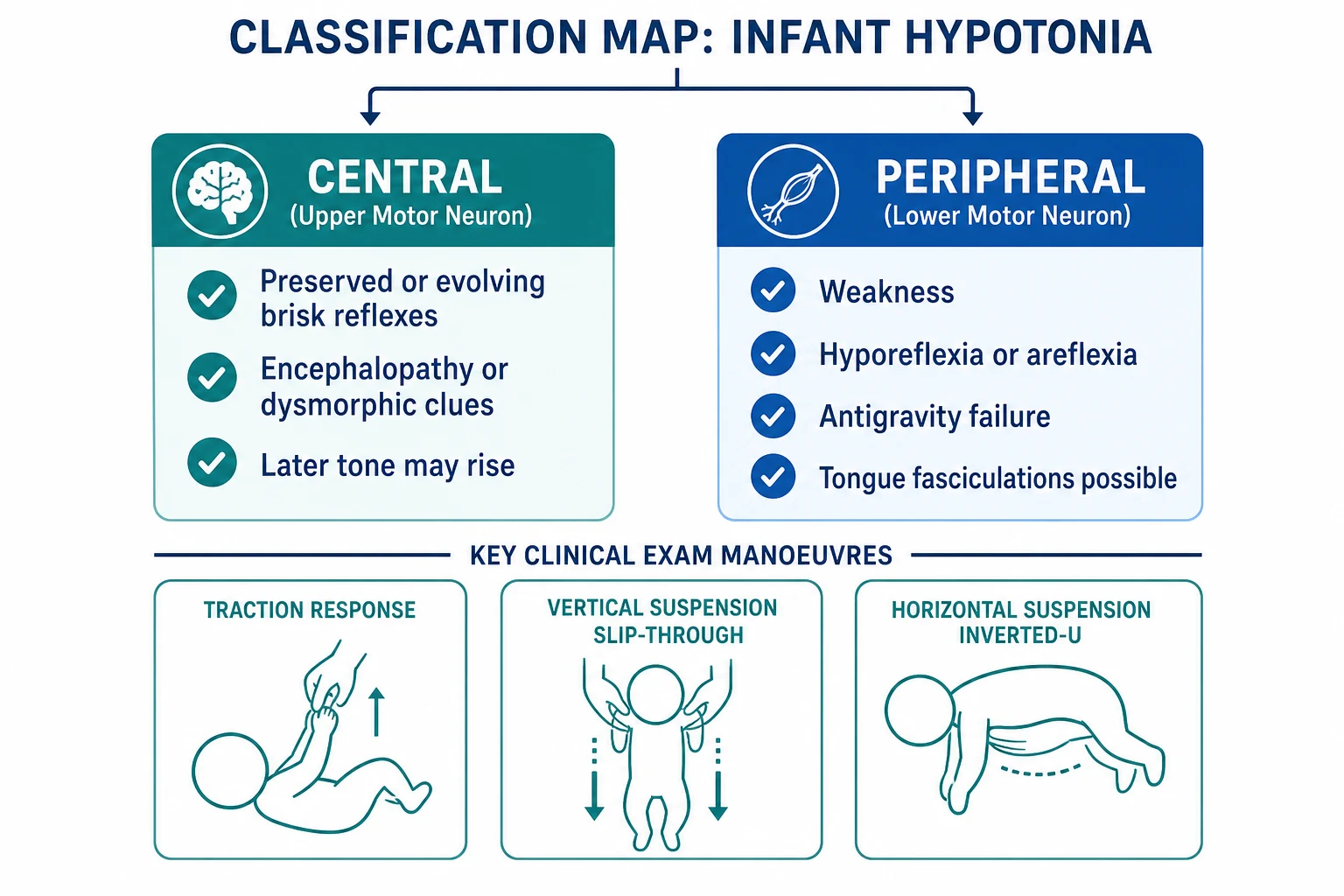
Read the figure like this: if the infant is weak and areflexic, do not spend a week reassuring the family that “tone often improves.” Peripheral patterns need a faster clock. [1] [3]
Central
Brain / upper pathways
- Tone low early, may later rise
- Reflexes often preserved or become brisk
- Encephalopathy, seizures or dysmorphology may coexist
- Motor delay with evolving CP risk is common
Peripheral
Motor unit
- True weakness with antigravity failure
- Hyporeflexia or areflexia
- Tongue fasciculations suggest anterior horn cell disease
- Breathing and feeding fail earlier
Laxity mimic
Connective tissue
- Joints move excessively
- Active antigravity power often better than expected
- Dysmorphic or skin clues may appear
- Still exclude true hypotonia carefully
Motor delay
Domain timing
- Skills late for age or corrected age
- May occur with or without low tone
- Isolate motor from global delay
- Escalate if plateau or regression appears
Epidemiology & Risk Factors
Hypotonia is a presentation, not a single disease, so incidence depends on setting. Delivery-room and NICU populations are enriched for central causes linked to encephalopathy, prematurity and congenital anomalies. Outpatient motor-delay clinics see more mixed central hypotonia, mild neuromuscular disease and environmental or positional contributors. What matters for exams is risk concentration, not a single universal percentage. [5] [6]
Family history changes the prior probability immediately. Consanguinity raises recessive neuromuscular and metabolic disease risk. A mother with grip myotonia, cataracts or an undiagnosed neuromuscular phenotype raises congenital myotonic dystrophy concern. Sibling deaths or delayed walking in relatives matter. [4] [17]
SMA epidemiology is shifting where newborn screening exists. Earlier molecular detection can move treatment into the pre-symptomatic or early symptomatic window, which is exactly why progressive weakness must not be observed away. Infant botulism remains uncommon but classic, with environmental spore exposure and honey risk still taught; absence of honey does not exclude the diagnosis. [9] [15] [16]
System factors create late diagnosis as often as biology does. Rural distance to neuromuscular centres, incomplete perinatal records in out-of-home care, language barriers and long genetics waitlists all compress treatment windows after the phenotype is already obvious. Equity is part of the epidemiology. [6] [8]
Children with developmental central hypotonia also carry later musculoskeletal risk, including hip problems. Tone management is therefore not only a neurology puzzle; it is a long-term body-structure problem. [20]
Pathophysiology
Resting tone is set by descending pathways, segmental stretch-reflex circuits and the mechanical properties of muscle and connective tissue. When brain pathways are injured or immature, resting tone falls. That does not mean the lower motor unit is dead. Over time, many central lesions produce spasticity or mixed tone as the nervous system reorganises. That is why a floppy young infant can later declare a cerebral palsy phenotype. [2] [12]
Peripheral lesions break the motor unit. Anterior horn cell loss in SMA removes the final common pathway to muscle. The infant cannot generate force. Reflexes vanish. Fasciculations reflect sick motor neurons. Neuromuscular junction blockade in infant botulism prevents acetylcholine release, so a previously well infant becomes weak, often with bulbar and autonomic features. Muscle membrane and contractile failure in congenital myotonic dystrophy or congenital myopathies reduce force even when the nerve is intact. In infantile Pompe disease, lysosomal glycogen storage injures muscle and myocardium together. [7] [9] [17]
Early motor maps need practice. Prolonged low tone and weakness steal that practice. Hips that are not loaded and stabilised become vulnerable. Feeding and breathing inefficiency create secondary injury through aspiration, sleep-disordered breathing and poor growth. Mechanism therefore links directly to urgency: every week of untreated progressive denervation is a week of lost motor neurons and lost skill. [9] [20]
Clinical Presentation
The classic floppy neonate lies in a frog-leg posture, handles like a soft parcel and may need help with airway positioning. Suck may be weak. The cry may be thin. Some infants look alert; others are encephalopathic. Alertness with profound weakness is a peripheral clue, not reassurance. [1] [3]
SMA type 1 often declares in the first months with progressive weakness, poor head control, bell-shaped chest mechanics, tongue fasciculations and preserved social interest early on. Infant botulism often starts in a previously well infant with constipation, weak cry, poor feeding and descending paralysis. Congenital myotonic dystrophy presents with neonatal floppiness and respiratory weakness; the diagnostic gold is sometimes in the mother’s handshake, not only the baby’s CK. Prader–Willi syndrome presents with profound neonatal hypotonia and feeding failure, later evolving toward hyperphagia — but the neonatal phase is the floppy phase. Infantile Pompe adds cardiomyopathy clues to the weakness story. [9] [16] [17] [18]
Later motor delay looks quieter. A toddler may not sit or walk on time, slip through hands when held under the arms, or fatigue on the floor. Language and social skills may be intact. That pattern still needs a structured motor examination, not a shrug that “boys walk late.” Atypical traps include sepsis-associated tone change, drug effects, spinal cord lesions that look like generalised floppiness, and central hypotonia hidden under a “cute flexible baby” label. [5] [19]
Differential Diagnosis
Build the differential from localisation. [1] [2]
- Central brain injury or developmental brain disorder — perinatal encephalopathy, structural brain anomalies, genetic neurodevelopmental disorders; later CP risk.
- Anterior horn cell disease — SMA until proven otherwise in progressive areflexic weakness.
- Neuromuscular junction disorder — infant botulism; rarer congenital myasthenic syndromes.
- Muscle disease — congenital myopathies, congenital myotonic dystrophy, infantile Pompe and other metabolic myopathies.
- Nerve disease — congenital or infantile neuropathies, less common but real.
- Syndromic hypotonia — Prader–Willi and many other syndromes with multi-system clues.
- Mimics — ligamentous laxity, acute systemic illness, medication effects, spinal lesions. [4] [7] [18]
Discriminators that earn marks: tongue fasciculations and areflexia favour SMA; constipation with descending paralysis favours botulism; maternal myotonia favours congenital myotonic dystrophy; hepatomegaly or cardiomyopathy clues favour Pompe or metabolic disease; encephalopathy and dysmorphology favour central disease. If several domains of development are delayed from the start, reopen the global developmental delay pathway rather than forcing a pure motor label. [1] [5]
Clinical & Bedside Assessment
History first, but not forever. Ask about fetal movements, polyhydramnios, delivery course, resuscitation, age at first concern, plateau versus progression, constipation, weak cry, choking, family neuromuscular disease and maternal symptoms of myotonia. Review medications and any honey or soil/dust exposures relevant to botulism teaching cases. [3] [15] [17]
Examine with the infant as calm as possible. Observe posture, spontaneous antigravity movement and respiratory pattern before you touch. Then assess passive tone in limbs and axial muscles. Perform traction response, vertical suspension and horizontal suspension as teaching manoeuvres, and interpret them with power and reflexes rather than as party tricks. Check deep tendon reflexes carefully. Inspect the tongue. Assess suck, swallow and cough. Examine the spine and look for dysmorphic or neurocutaneous clues. If congenital myotonic dystrophy is possible, examine the mother. [1] [3] [17]
Document motor milestones with corrected age in preterm infants. When the question is early cerebral palsy risk rather than acute neuromuscular collapse, tools such as the General Movements Assessment and Hammersmith Infant Neurological Examination add structured probability — use them as adjuncts and cross-link the dedicated GMA/HINE leaf for scoring detail rather than inventing cut-offs here. [12] [13] [14]
Investigations
Investigations follow localisation. In significant neonatal or infantile hypotonia, first-line bedside and laboratory evaluation often includes glucose and blood gas context as needed, electrolytes, calcium, septic work-up when infection is possible, CK, and chest imaging or blood gas support when respiratory failure is near. CK can be high in some myopathies and still normal in SMA or many congenital myopathies, so a normal CK never closes the case. [1] [2] [5]
If the phenotype is progressive, areflexic and weak, urgent SMN1 deletion testing with SMN2 copy-number context is a priority, especially where newborn screening has not already answered the question. If Prader–Willi is plausible, ordered methylation testing belongs early because the neonatal phenotype is dominated by hypotonia and poor feeding. If Pompe is plausible, pair clinical suspicion with enzyme assay and molecular confirmation pathways used by your metabolic service, and obtain cardiac assessment. [4] [9] [18]
For suspected infant botulism, send stool for toxin testing according to public-health pathways, but do not wait for the result to treat when clinical suspicion is high. Neuroimaging and EEG belong when central disease, seizures or encephalopathy are in play. Metabolic labs are guided by systemic clues rather than infinite panels on every mild outpatient delay. Genomic sequencing increasingly diagnoses monogenic neonatal hypotonia when the first-line targeted tests are negative; consortium data support a structured genomic approach rather than endless low-yield repetition. EMG/NCS and muscle biopsy remain useful in selected peripheral phenotypes after specialist input. [8] [15] [16]
Management — Resuscitation
Airway and breathing come before the perfect differential. Position the airway, clear secretions, support ventilation if needed and escalate to NICU or PICU early when cough is weak or fatigue is rising. Protect feeds: if swallow is unsafe, stop oral trials and use nasogastric or intravenous support rather than “seeing if the next feed goes better.” [5] [7]
If infant botulism is likely, treat on suspicion with the jurisdiction’s botulism antitoxin pathway and supportive care. Avoid drugs that further impair neuromuscular transmission when alternatives exist, and involve public health as required. If the infant is encephalopathic, run the full critical-illness ladder in parallel: glucose, seizure control, sepsis treatment and imaging as indicated. For suspected SMA with respiratory vulnerability, stabilise and move rapidly toward confirmatory genetics and a neuromuscular centre rather than prolonged local observation. [9] [15] [16]
Family distress is part of resuscitation. Sit down. Name what you are protecting today. Separate “we do not yet have the final gene name” from “we are acting on the dangerous pattern in front of us.” [5] [9]
Management — Definitive & Stepwise
After stabilisation, manage by branch. [1] [6]
Step 1 — Localise and document. Central, peripheral, mixed or still unclear.
Step 2 — Keep the infant safe. Respiratory plan, feeding plan, monitoring intensity.
Step 3 — Targeted urgent tests. SMA genetics, botulism pathway, cardiac/metabolic tests, neuroimaging or methylation studies as the phenotype demands.
Step 4 — Disease-specific therapy. For infantile-onset SMA, disease-modifying therapy is time-critical. Nusinersen improved motor milestones versus sham control in ENDEAR, and later-onset data support treatment benefit beyond the classic type 1 window. Onasemnogene abeparvovec gene-replacement therapy improved survival and motor outcomes in the pivotal early SMA type 1 gene-therapy experience. Exact product choice, eligibility and dosing are specialist-protocol decisions; your general-paediatric job is recognition, rapid referral and not losing days. [9] [10] [11]
Step 5 — Supportive multidisciplinary care. Physiotherapy, occupational therapy, speech and feeding therapy, respiratory support, orthopaedics/hip surveillance thinking in central hypotonia, genetics counselling and, when appropriate, palliative care partnership. [19] [20]
Step 6 — Early intervention and follow-up clocks. Static central hypotonia still needs developmental therapy. Progressive disease needs tighter review. Safety-net for breathing change, feed refusal and loss of skills.
Specific Subtypes & Scenarios
Neonatal profound floppiness with respiratory failure. Think congenital myotonic dystrophy, severe congenital myopathy, central nervous system catastrophe and early-onset SMA phenotypes. Examine the mother. Support ventilation and feeding first. [17]
Three-month-old with progressive weakness and tongue fasciculations. This is an SMA pattern until genetics say otherwise. Do not reassure based on a social smile. [9]
Previously well infant with constipation and descending paralysis. Infant botulism pathway: antitoxin and support on clinical suspicion. Honey history helps when present but is not required. [15] [16]
Poor feeding neonate evolving toward Prader–Willi. Profound hypotonia and suck failure dominate early life; order the correct methylation pathway and support nutrition. [18]
Hypotonia plus cardiomyopathy clues. Consider infantile Pompe and involve metabolic and cardiology services early. [4]
Ex-preterm infant with central hypotonia. Use corrected age, screen for evolving motor impairment, and deploy early CP detection tools when risk is high without delaying therapy access. [12] [13]
Toddler with isolated delayed walking. Re-examine tone, power, reflexes and symmetry. Mild central hypotonia, muscle disease and normal late walking variants all live here; red flags still escalate. [19]
Complications & Pitfalls
The classic pitfall is false reassurance. Families hear “low tone is common” and leave without a safety plan. Progressive disease then declares as respiratory failure. A second pitfall is CP-only thinking: every floppy infant is not early cerebral palsy, and SMA or botulism will not forgive that assumption. A third is laboratory delay: waiting for botulism confirmation, or waiting for a “repeat clinic visit” before SMA testing, burns the therapeutic window. [9] [16]
Other frequent errors: never examining the mother; treating a normal CK as exclusionary; ordering every test at once without localisation; ignoring aspiration risk; forgetting hip and posture surveillance in long-standing central hypotonia; and writing “benign congenital hypotonia” as if it were a molecular diagnosis. [2] [20]
Prognosis & Disposition
Prognosis follows cause, severity of bulbar and respiratory involvement, and treatment timing. Historical natural history for untreated infantile SMA was grim; disease-modifying therapy has shifted survival and motor outcomes when started early, which is the practical reason this topic is time-critical. Infant botulism is potentially life-threatening in the acute phase but often recovers with meticulous supportive care and timely antitoxin. Central hypotonia outcomes range from near-normal function with therapy to lifelong neurodisability, depending on the brain diagnosis. [9] [10] [15]
Disposition options are home with urgent outpatient work-up, ward observation, PICU, or direct transfer to a neuromuscular or metabolic centre. Choose by airway risk and tempo, not by diagnostic pride. After diagnosis, the medical home still owns vaccines, growth, hip and bone health thinking, equipment access, school planning and family mental health. Genetic counselling belongs in the disposition plan whenever a heritable disease is confirmed or likely. [6] [20]
Special Populations
Preterm infants need corrected-age interpretation and careful separation of transient immaturity from true pathology. NICU graduates may carry both central injury risk and ICU-acquired vulnerability. Rural families need explicit transfer triggers and named contacts for neuromuscular centres. Indigenous, migrant and language-discordant families need culturally safe explanations and interpreters; diagnostic complexity is not an excuse for inaccessible counselling. Children in out-of-home care may lack maternal history that would have revealed myotonic dystrophy. Technology-dependent survivors of infantile neuromuscular disease need coordinated acute-care plans so that later ED visits do not restart the diagnostic maze from zero. [5] [12] [17]
Evidence, Guidelines & Regional Differences
The clinical skeleton of floppy-infant evaluation is long-standing: Peredo, Bodensteiner and Crawford all centre localisation, power, reflexes and a disciplined test sequence. Prasad extends the genetic logic. Newer syntheses by Laverty and by Cicala and Mercuri integrate bedside reasoning with genomic diagnosis. Morton and colleagues show that exome and genome sequencing can define the genetic basis of neonatal hypotonia in a substantial modern cohort when used in a structured diagnostic pathway. [1] [2] [3] [4] [5] [6] [8]
SMA evidence is interventional, not only descriptive. ENDEAR demonstrated motor-milestone benefit of nusinersen versus sham in infantile-onset disease; CHERISH supported benefit in later-onset SMA; gene-replacement therapy data from Mendell and longer-term safety reports support early targeted treatment pathways. Exact formulary access differs by country and year — state the principle and use local neuromuscular networks. [9] [10] [11]
For early cerebral palsy risk within the hypotonic or motor-delay spectrum, Novak’s early diagnosis framework and HINE-related work support structured detection and earlier intervention. Full GMA/HINE technique lives on the dedicated leaf. Infant botulism teaching rests on clinical suspicion plus epidemiology series, not on waiting for a perfect exposure history. [12] [13] [15]
In Australia and Aotearoa New Zealand, link local SMA newborn-screening status, neuromuscular referral networks and botulism public-health pathways. Do not invent stock maps for antitoxin; use the active jurisdictional process. Child development services and early intervention access vary by state and district health board — name an owner for the referral. [9]
Exam Pearls
FLOPPY
References
- [1]Peredo DE, Hannibal MC The floppy infant: evaluation of hypotonia. Pediatrics in review, 2009.PMID 19726697
- [2]Bodensteiner JB The evaluation of the hypotonic infant. Seminars in pediatric neurology, 2008.PMID 18342256
- [3]Crawford TO Clinical evaluation of the floppy infant. Pediatric annals, 1992.PMID 1620559
- [4]Prasad AN, Prasad C Genetic evaluation of the floppy infant. Seminars in fetal & neonatal medicine, 2011.PMID 21131247
- [5]Laverty CG Hypotonia in the Newborn Infant. Pediatric clinics of North America, 2025.PMID 40619196
- [6]Cicala G, Mercuri E The floppy infant revisited: From bedside to genome. Developmental medicine and child neurology, 2026.PMID 41495003
- [7]Kaler J, Hussain A, Patel S Neuromuscular Junction Disorders and Floppy Infant Syndrome: A Comprehensive Review. Cureus, 2020.PMID 32071826
- [8]Morton SU, Costain G, French CE Exome and Genome Sequencing to Diagnose the Genetic Basis of Neonatal Hypotonia: An International Consortium Study. Neurology, 2025.PMID 39700446
- [9]Finkel RS, Mercuri E, Darras BT Nusinersen versus Sham Control in Infantile-Onset Spinal Muscular Atrophy. The New England journal of medicine, 2017.PMID 29091570
- [10]Mendell JR, Al-Zaidy S, Shell R Single-Dose Gene-Replacement Therapy for Spinal Muscular Atrophy. The New England journal of medicine, 2017.PMID 29091557
- [11]Mercuri E, Darras BT, Chiriboga CA Nusinersen versus Sham Control in Later-Onset Spinal Muscular Atrophy. The New England journal of medicine, 2018.PMID 29443664
- [12]Novak I, Morgan C, Adde L Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and Treatment. JAMA pediatrics, 2017.PMID 28715518
- [13]Fehlings D, Makino A, Church P The Hammersmith Infant Neurological Exam Scoring Aid supports early detection for infants with high probability of cerebral palsy. Developmental medicine and child neurology, 2024.PMID 38818710
- [14]Romeo DM, Velli C, Sini F Neurological assessment tool for screening infants during the first year after birth: The Brief-Hammersmith Infant Neurological Examination. Developmental medicine and child neurology, 2024.PMID 38287208
- [15]Panditrao MV, Dabritz HA, Kazerouni NN Descriptive Epidemiology of Infant Botulism in California: The First 40 Years. The Journal of pediatrics, 2020.PMID 32800814
- [16]Sarintra N, Ekdahl R, Sanders SC More Than Just a Floppy Baby: Maintaining High Clinical Suspicion of Infant Botulism. Cureus, 2026.PMID 41728439
- [17]Suzui R, Wada I, Matsubara M Undiagnosed Maternal Myotonic Dystrophy Type 1 Revealed by Congenital Myotonic Dystrophy in the Neonate. Cureus, 2026.PMID 42037975
- [18]Driscoll DJ, Miller JL, Cassidy SB Prader-Willi Syndrome. GeneReviews, 1993.PMID 20301505
- [19]Hidalgo Robles Á, Paleg GS, Livingstone RW Identifying and Evaluating Young Children with Developmental Central Hypotonia: An Overview of Systematic Reviews and Tools. Healthcare (Basel, Switzerland), 2024.PMID 38391868
- [20]Livingstone RW, Paleg GS, Shrader MW Incidence of hip problems in developmental central hypotonia: A scoping review. Developmental medicine and child neurology, 2025.PMID 39429029