Paeds · investigations-procedures-and-technology
Radiation protection and imaging stewardship
Also known as Radiation protection in children · Imaging stewardship · ALARA in paediatric imaging · Image Gently · Justification and optimisation of imaging · Diagnostic reference levels
Fellowship guide to radiation protection and imaging stewardship in children — the discipline of getting the right image, at the right time, with the lowest radiation, and only when it changes management. Covers the three pillars of radiological protection (justification, optimisation, dose limitation) and why dose limits do not apply to patients, the linear-no-threshold model and the Brenner, Pearce, Meulepas and EPI-CT risk cohorts, the dose quantities used to measure and benchmark CT and fluoroscopy (CTDIvol, DLP, SSDE, KAP, reference air kerma) and diagnostic reference levels set at the 75th percentile, the practical optimisation levers in paediatric computed tomography, the modern phasing-out of gonadal shielding, the Image Gently, Image Wisely and Choosing Wisely stewardship programmes, the substitution of ultrasound and MRI to remove ionising radiation entirely, the justification and consent conversation with families, and the regional regulatory frameworks (ICRP, IAEA, ARPANSA, IRMER, ACR).
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the eight-year-old who has had a ventriculoperitoneal shunt since infancy and is back in the emergency department with a headache, the two-year-old sent for a recurrent chest infection, and the adolescent being worked up for recurrent abdominal pain. Each generates another imaging request, and each request is a stewardship decision about whether the image is needed, what it will change, and what it will cost the child in radiation across a lifetime. That recurring decision is the territory this page owns. [3] [8]
Radiation protection is the set of principles and practices that keep ionising-radiation dose as low as reasonably achievable while preserving the diagnostic benefit the image provides. Imaging stewardship is the broader clinical discipline of requesting the right test, at the right time, for the right reason, and at the lowest harm — of which radiation is one component, alongside sedation, contrast, cost and the cascade of incidental findings. In children, the two are inseparable, because the child's radiosensitivity and the cumulative burden of a long life ahead make every ionising request a deliberate act. [6] [7]
Ionising radiation carries enough photon energy to strip electrons from atoms and damage DNA. Computed tomography (CT), plain radiography, fluoroscopy and nuclear medicine all use it; ultrasound and magnetic resonance imaging (MRI) do not. The paediatric skill is to choose a non-ionising modality wherever it answers the question, and — when ionising imaging is the modality that answers the question — to justify it, optimise its dose, and limit its repetition. [3] [7]
The reason this is a distinct paediatric topic is that a given dose delivered to a child carries a measurably higher lifetime attributable cancer risk than the same dose delivered to an adult. The cohorts that established this — Brenner and Hall's New England Journal analysis, the UK retrospective cohort of Pearce, and the Dutch and pan-European EPI-CT cohorts — did not forbid paediatric ionising imaging. They made every paediatric ionising request a deliberate, justified, dose-optimised decision, and they gave the discipline of imaging stewardship its scientific foundation. [1] [2] [3]
Classification
The cleanest way to hold this topic is to classify it twice — first by the three pillars of radiological protection that govern every ionising exposure, and second by the imaging modality spectrum that ranks the tests from zero radiation to the highest dose. Holding both in mind lets a candidate defend any single request on the principles that apply to it. [8] [9]
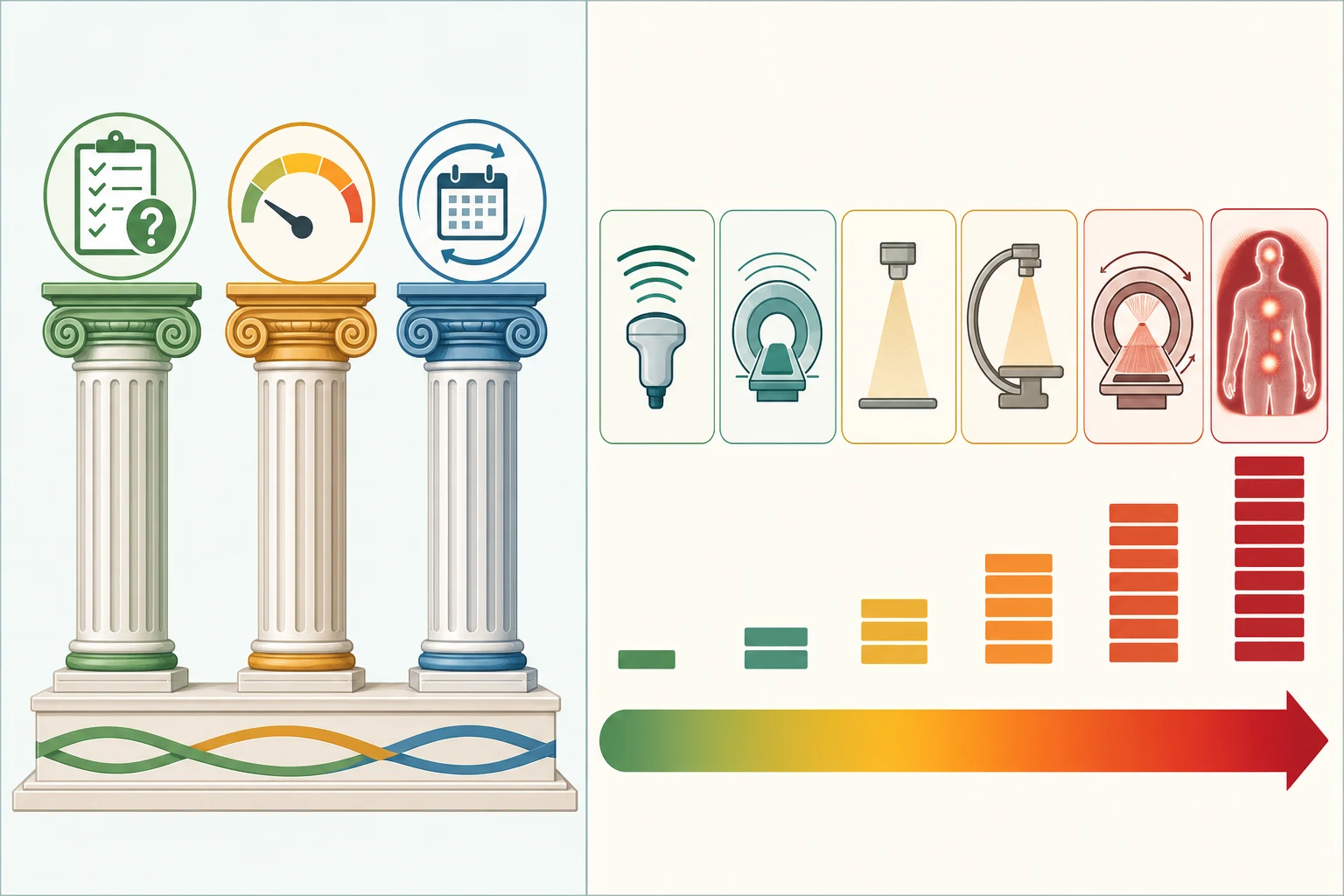
Justification asks whether any ionising exposure is warranted — whether it will do more good than harm, and whether the information it yields will change management. The requesting clinician carries the first responsibility to justify, and the radiologist carries the second to confirm the request and select the optimal technique, a principle of double justification. Optimisation is the ALARA principle: once an exposure is justified, the dose must be kept as low as reasonably achievable while still producing a diagnostic image, achieved through paediatric protocols, size-specific settings and modern reconstruction. Dose limitation sets numeric exposure limits for occupationally exposed staff and for the public — and the examinable point is that dose limits do not apply to patients: a justified patient investigation may exceed a staff dose limit, because the limit exists to protect those who receive no benefit, whereas the patient receives the diagnostic benefit that justified the exposure. [8] [9]
The second classification is the modality spectrum, ranked by the effective dose each delivers. Ultrasound and MRI sit at the zero end — no ionising radiation, and the first stewardship thought whenever they can answer the question. Plain radiography delivers a small dose (a chest or limb radiograph is a fraction of a millisievert). Fluoroscopy delivers a dose that scales with screening time — low for a brief barium study, substantial for a prolonged interventional procedure. CT delivers the highest routine diagnostic dose, and is the single largest contributor to the paediatric medical radiation burden. Nuclear medicine delivers an internal dose from the radiotracer that decays over hours to days. Knowing where a test sits on this spectrum is the first step in choosing the lowest-harm modality that answers the question. [3] [7]
Non-ionising versus ionising imaging — the stewardship choice
Non-ionising (ultrasound, MRI)
- Zero ionising-radiation dose — zero attributable cancer risk
- First thought whenever the modality answers the clinical question
- Ultrasound: fast, bedside, operator-dependent, no sedation
- MRI: exquisite soft-tissue and fluid detail; may need sedation; device and gadolinium issues
- Stewardship lever: substitute to remove radiation entirely
Ionising (radiograph, fluoroscopy, CT, nuclear medicine)
- Small but real stochastic cancer risk — no assumed safe threshold
- Justified only when the non-ionising modality cannot answer the question
- Radiograph: very low dose; fluoroscopy: scales with screening time
- CT: highest routine diagnostic dose; nuclear medicine: internal tracer dose
- Stewardship lever: justify, then optimise the dose and limit repetition
The dose numbers that anchor your viva
Epidemiology & Risk Factors
Medical imaging has become the largest artificial source of ionising-radiation exposure in the population, and CT is the dominant contributor. Brenner and Hall estimated that, at the utilisation rates of the early 2000s, computed tomography could contribute of the order of one to two per cent of all cancers in populations with high CT use — a projection that placed stewardship squarely in the domain of public health, not just individual risk. [3] [9]
The child at greatest cumulative dose is not the one scanned once for an emergency, but the one scanned repeatedly across years: the shunted child, the oncology patient on surveillance, the complex chronic patient with recurrent presentations, and the child with a chronic inflammatory or renal condition followed with serial imaging. For each, the dose accumulates across a lifetime, and each repeat request is a stewardship decision that must be justified on its own merits. [1] [2]
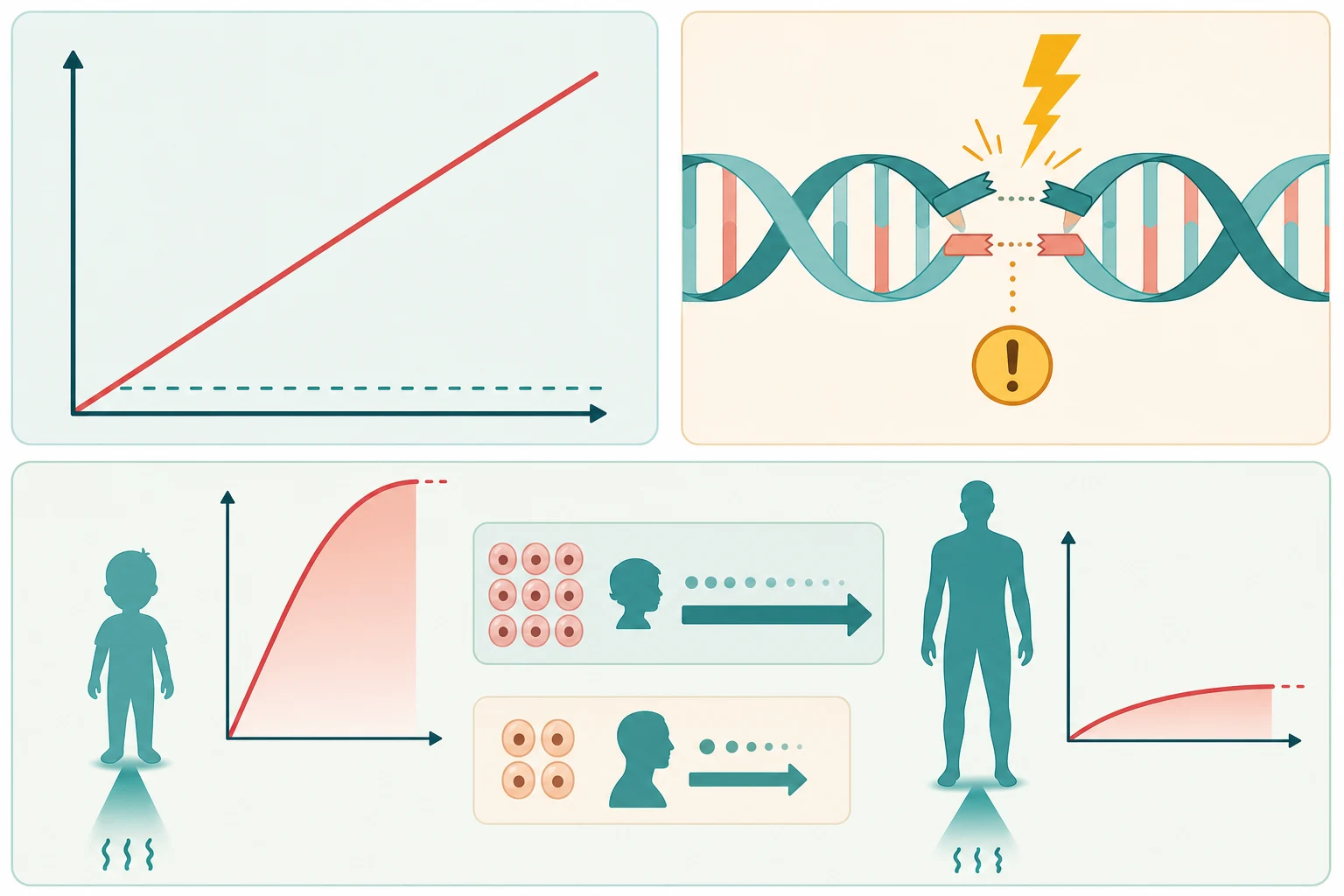
The child at greatest per-scan risk is the youngest. The attributable cancer risk from a given effective dose falls with age at exposure, so the infant and young child carry the highest per-scan risk — more rapidly dividing tissue, a longer remaining lifespan over which a radiation-induced cancer can express, and a smaller body that scatters the dose less effectively than an adult's. This age-sensitivity is the physiological reason paediatric protocols must reduce the milliampere-seconds and kilovoltage peak rather than apply an adult setting, and the reason stewardship matters most in the youngest children. [3] [7]
Miglioretti and colleagues quantified the population burden of paediatric CT in the United States, projecting that the millions of paediatric CT examinations performed each year could give rise to a few thousand excess future cancers — a figure that is small against the population but drives the stewardship imperative to scan only when justified, and to optimise every scan that is performed. [4]
Pathophysiology
To explain why radiation protection matters, follow the dose from the X-ray tube to the DNA, and then to the cancer that may, or may not, follow decades later. In CT, the tube rotates a fan of photons around the child; the photons are attenuated to different degrees by bone, soft tissue, fat and air, and a computer reconstructs the attenuation map into the image. The photons that pass through deposit a small amount of energy in the tissue along the way — that deposition is the dose — and after the scan no residual radiation remains in the child. [3] [7]
The carcinogenic lesion is the misrepaired DNA double-strand break. Ionising radiation damages DNA in two ways: directly, by cleaving the phosphodiester backbone, and indirectly, by generating free radicals that injure the bases. Most damage is repaired faithfully, but a small fraction is misrepaired, and a misrepaired break in a critical gene can, years to decades later, initiate a malignancy. The modern understanding of low-dose diagnostic risk is stochastic — the probability of harm rises with dose, with no threshold assumed below which the risk is zero. This non-threshold assumption, formalised as the linear-no-threshold model, is the scientific basis for the ALARA principle: it is not that a single CT is dangerous, but that no dose is free of risk, so every dose must be justified and minimised. [3] [1]
The cohort evidence quantifies the risk the model predicts. Pearce and colleagues reported the United Kingdom retrospective cohort of CT scans in childhood and subsequent leukaemia and brain tumour risk, demonstrating a dose-response with cumulative organ dose. The Dutch cohort of Meulepas and colleagues, with longer follow-up and refined dose estimates, confirmed a small but real attributable risk across a broader range of cancers. The international EPI-CT consortium has extended this with pooled European data. None of these studies forbid CT; together they justify the discipline that every paediatric ionising request is a deliberate, justified, dose-optimised decision. [1] [2]
[3] [7]Clinical Presentation
The child who needs imaging comes to you as a clinical question, not a modality request. The stewardship skill is to translate each presentation into the question the imaging must answer, and to choose the lowest-harm modality that answers it — which, in a large fraction of paediatric presentations, is a non-ionising one or no imaging at all. [6] [8]
The presentations that drive ionising requests cluster into a few patterns. The trauma child asks whether there is an intracranial, thoracic or abdominal injury. The shunted or complex chronic child asks whether the hardware is working or the disease has progressed. The recurrent infection or inflammatory child asks whether there is a structural or obstructive cause. The oncology child asks whether there is response, relapse or complication. Each is a different question, each has a preferred modality, and each repeat request in a chronic patient is a stewardship checkpoint. [1] [9]
The red-flag features that mandate a justified ionising scan rather than observation or a non-ionising modality are constant across presentations: a clinically unstable child, a high-risk mechanism, focal or progressive signs, and a presentation where the imaging will change an immediate management decision. These are the children for whom the scan is non-negotiable; the radiation risk is real but it is never a reason to delay a necessary, justified scan. [8] [9]
The atypical presentations deserve a stewardship pause. The non-verbal or developmentally delayed child cannot describe symptoms, so the threshold to image is set by behaviour and examination — and the threshold to substitute a non-ionising modality, or to defer, is lower still. The complex chronic child arrives with a long imaging history, and the cumulative dose is part of the present decision. The pregnant adolescent requires a pregnancy check and a documented justification before any ionising exposure. Each of these is a moment to apply the three pillars deliberately rather than by reflex. [7] [9]
Differential Diagnosis
The differential in a stewardship topic is not a list of diseases but a list of the reasonable alternatives to an ionising request — the choices a candidate must name and defend when asked why the child is being scanned at all. [6] [8]
The first alternative is no imaging. A large fraction of paediatric ionising requests are avoidable: the well child with a low-risk mechanism, the simple febrile seizure that has returned to baseline, the chest that will clear with time, the constipation that explains the abdominal pain. The validated clinical decision rules — PECARN for minor head injury among them — exist precisely to identify the very-low-risk child in whom imaging can safely be omitted. Choosing not to image is the most powerful stewardship decision, and it is the first one to name. [8]
The second alternative is a non-ionising modality. Ultrasound answers many paediatric questions — pyloric stenosis, intussusception, hip effusion, renal tract dilation, soft-tissue and vascular assessment — without radiation. MRI answers the soft-tissue, neurological and oncological questions that CT used to dominate, including rapid-sequence ventricular assessment in the shunted child. Naming the non-ionising substitute for a given clinical question is a viva-ready skill. [6] [9]
The third alternative is a lower-dose ionising technique. A single-phase CT in place of a multiphase protocol, a limited radiograph series, a short fluoroscopic screening time, or a reduced-activity nuclear-medicine acquisition each lowers the dose while answering the question. When ionising imaging is justified, the question becomes how to deliver the lowest diagnostic dose, not whether to scan. [5] [8]
Clinical & Bedside Assessment
Before any ionising request, run a structured bedside and clinical assessment that turns the child's presentation into a justified decision. The aim is to answer three questions: is any imaging needed, what question will it answer, and what will it change. [6] [8]
Begin with the focused history and examination that defines the clinical question — the mechanism and time course, the presence of red flags, the child's baseline and chronic conditions, and the previous imaging that contributes to the cumulative dose. In the infant, the open fontanelle and the head circumference trajectory may redirect the request from CT to ultrasound. The examination refines the threshold: a well child with a normal examination and a low-risk presentation avoids imaging; an abnormal finding or a high-risk mechanism escalates it. [7] [8]
Assess the cumulative imaging history explicitly in the chronic child. A shunted, oncology or complex chronic patient may have accumulated tens of millisievert across years of surveillance, and the present request is judged against that total. Where available, the cumulative dose should be reviewed, and a non-ionising substitute preferred where it answers the question — the shift from serial CT to rapid MRI for shunt surveillance is the worked example. [1] [2]
The consent and counselling step belongs at the bedside. For any justified ionising exposure, the family is told in plain language why the test is needed, what the small radiation risk amounts to, and what the alternatives were — and the discussion is documented. In the adolescent of childbearing potential, a pregnancy check precedes any ionising request, and a documented negative is part of the justification. [8] [9]
Investigations
The investigations section of this topic is the dose-measurement and dose-benchmarking toolkit itself — the quantities and the benchmarks that let a clinician understand, compare and optimise the dose a child receives. The fellowable content is the dose quantities, the diagnostic reference level, and the optimisation levers. [3] [10]
How a CT dose is measured
The dose a CT delivers is described by three linked quantities. The computed tomography dose index (CTDIvol), expressed in milligray, estimates the average dose within a single rotation of the scanner for a standard reference phantom. The dose-length product (DLP), expressed in milligray-centimetres, multiplies the CTDIvol by the scan length and approximates the total energy delivered. A rough conversion to effective dose in millisievert applies age-dependent coefficients to the DLP. Because the standard phantoms are adult-sized, the size-specific dose estimate (SSDE) corrects the CTDIvol for the actual size of the child — an essential correction in paediatrics, where a small body receives a markedly higher dose than the adult phantom suggests for the same scanner setting. [5] [7]
In fluoroscopy, the dose is tracked by the kerma-area product (KAP, also called the dose-area product, in gray-centimetres squared), which reflects both the dose rate and the field size, and by the reference air kerma (in milligray) at the interventional reference point, which reflects the cumulative skin dose and is the quantity watched for deterministic skin injury in long procedures. In nuclear medicine, the dose is the internal dose from the radiotracer, estimated by the administered activity and the radiopharmaceutical's residence time, summarised as the effective dose per administered activity. [11]
The diagnostic reference level
The diagnostic reference level (DRL) is the central benchmarking tool of optimisation. It is set, for a defined examination on a defined patient group, at around the seventy-fifth percentile — the third quartile — of the observed dose distribution across a sample of centres. It is not a dose limit and not a regulatory ceiling; it is an investigational trigger. A centre or a protocol whose typical dose sits above the DRL is flagged for review, on the understanding that the dose can almost always be reduced without sacrificing diagnostic quality. Diagnostic reference levels must be size- or age-stratified in children, because a single adult-derived DRL applied to a child obscures the very over-dosing the benchmark exists to detect. Kanal and colleagues established national paediatric CT diagnostic reference levels across ten common examinations, and Strauss and colleagues estimated them for paediatric fluoroscopically guided procedures — the benchmarks against which a local paediatric protocol is judged. [10] [11]
[10] [11]The optimisation levers in paediatric CT
When CT is the justified modality, the dose is optimised to the child through a set of well-established levers. A size-specific paediatric protocol scales the milliampere-seconds and the kilovoltage peak to the child's size rather than applying an adult setting. Automatic tube current modulation reduces the milliampere-seconds as the tube rotates through thin body regions. A lower kilovoltage peak — typically eighty to one hundred kilovolts in children, rather than the adult hundred and twenty — reduces dose and increases the contrast of iodinated contrast media, which is favourable in children. Limiting the scan length to the region of interest and preferring a single phase over a multiphase protocol each avoid unnecessary dose, because every additional phase multiplies it. Iterative reconstruction algorithms allow a lower-dose acquisition to produce a diagnostic image. These levers, operationalised by the Image Gently alliance, are now standard on modern paediatric scanners. [6] [7]
Management — Resuscitation
The immediate priority when a justified, urgent ionising scan is needed is the order of operations that protects both the child and the integrity of the examination: the child is stabilised before transfer, and the request is justified and optimised before it is acquired. An unstable child is never taken to the scanner before the airway and circulation are secured, because the scanner is an isolated, inaccessible environment in which resuscitation is harder. [8] [9]
A child with a compromised airway or a falling conscious state is intubated before transfer, with a rapid-sequence neuroprotective technique where raised pressure is a concern. If there are signs of herniation, an immediate osmolar agent is given while imaging is arranged, per local protocol — the accepted options are 3 percent hypertonic saline (commonly 2 to 5 mL per kg intravenously over 10 to 30 minutes) or mannitol (commonly 0.25 to 1 g per kg intravenously) — alongside urgent specialist referral. The modality in this setting is CT, because it is fast, available, and answers the question that drives the immediate surgical decision. [8]
The stewardship discipline applies even here. A justified urgent CT is acquired with a paediatric protocol, a single phase, and a limited scan length wherever the clinical question allows, because the radiation risk is small but real even in an emergency, and optimisation costs nothing in time. The request names the question, and the radiographer applies the size-appropriate technique. [7] [8]
Management — Definitive & Stepwise
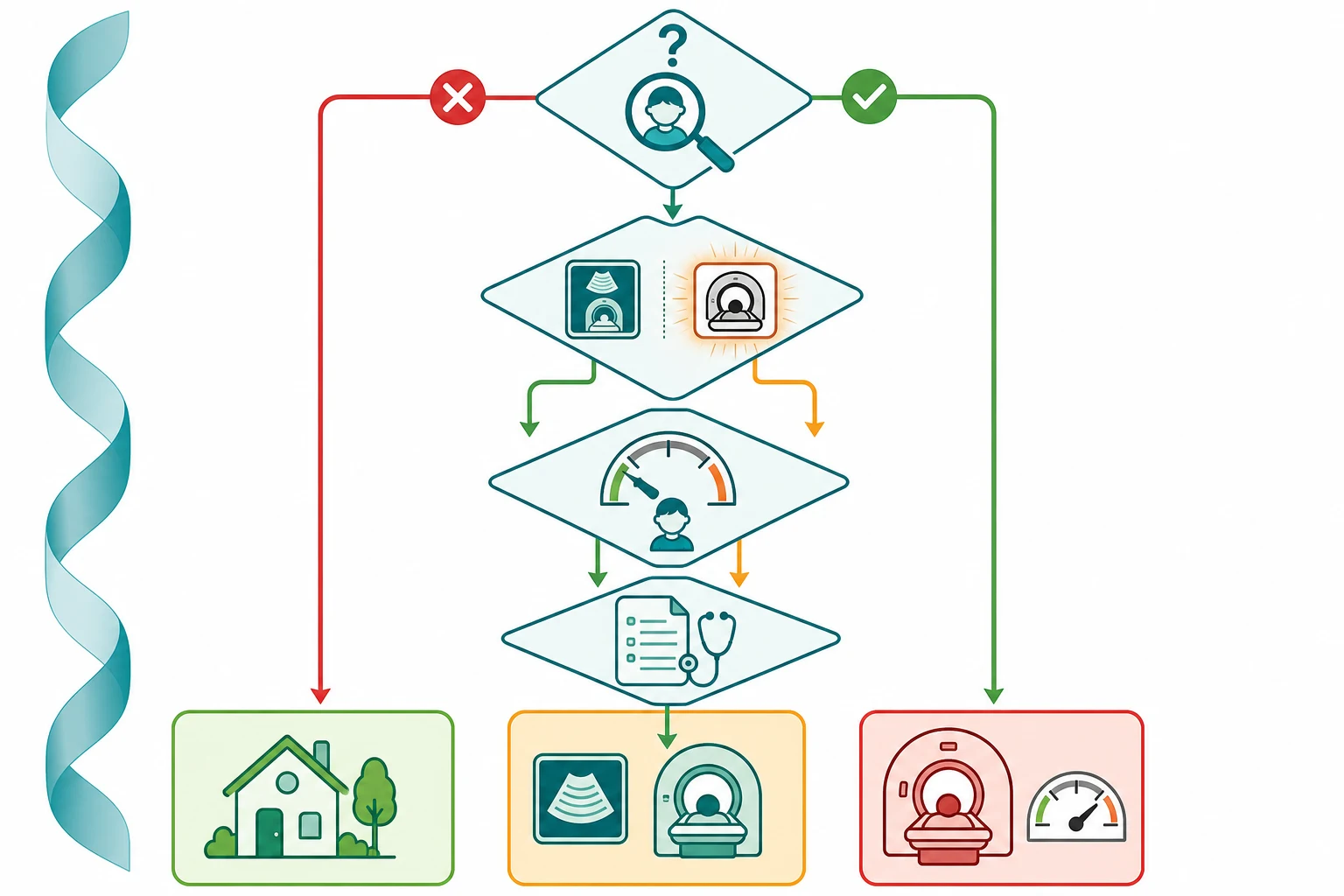
The definitive skill is a stepwise stewardship pathway that turns the clinical question into the right test at the lowest harm. The pathway has four steps, and it encodes the three pillars at each one. [6] [8]
Step 1 — Justify every request
Ask whether any imaging is needed, whether it is needed now, and what question it will answer. A justified request names the clinical question and the expected change in management. An unjustified request — for reassurance, for defensive medicine, or to satisfy a parent or a protocol — is the commonest source of avoidable paediatric radiation. The validated decision rules justify not scanning the very-low-risk child; Choosing Wisely and the RACP Evolve programmes name the tests that are commonly requested without benefit. [8] [9]
Step 2 — Choose the lowest-harm modality
Where a non-ionising modality answers the question, choose it. Ultrasound for the pyloric mass, the intussusception, the hip effusion and the renal tract; MRI for the first unprovoked seizure, the developmental delay, the elective tumour surveillance, and the rapid ventricular assessment of the shunted child. Where ionising imaging is the modality that answers the question — acute trauma, acute haemorrhage, the unstable abdomen, the acute chest — choose it without hesitation; the radiation risk is real but it is not a reason to delay a necessary scan. [6] [7]
Step 3 — Optimise the dose
When ionising imaging is the modality, the dose is optimised to the child. This means a size-specific paediatric protocol that scales the milliampere-seconds and kilovoltage peak to the child, a lower kilovoltage peak, automatic tube current modulation, a limited scan length, a single phase wherever multiphase is unnecessary, and iterative reconstruction. The requesting clinician's contribution is to communicate the clinical question clearly so the radiographer applies the right protocol, and to avoid the multiphase request when a single phase answers the question. The local protocol is benchmarked against the paediatric diagnostic reference level. [6] [10]
Step 4 — Limit repetition and track cumulative dose
Cumulative dose accumulates across years in the child who is scanned repeatedly. The shunted child, the oncology patient and the complex chronic patient are the highest-cumulative-dose groups, and each repeat request must be justified on its own merits. The modern shift is to rapid MRI protocols for surveillance that once required serial CT, and to track the cumulative dose in the chronic patient so the present decision is made against the lifetime total. The repeat request that is not justified by a change in management is the request to question. [1] [2]
Gonadal and patient shielding — the modern position
The advice on gonadal shielding has reversed. For decades, a lead shield over the gonads was routine paediatric practice. Current ACR-AAPM and national guidance now recommends discontinuing routine gonadal and fetal shielding. The reasons are technical: modern equipment keeps the dose outside the field of view negligible, a shield can slide into the beam and degrade the image or trigger the automatic exposure control to raise the dose, and the shield offers a false reassurance that distracts from the real optimisation levers. Shielding of staff and of a pregnant carer who holds the child remains appropriate; routine patient gonadal shielding does not. The stewardship lesson is that protection is achieved by justification and optimisation, not by adding a shield to an over-dosed exposure. [12]
Communicating radiation risk to a family
The communication is the fellowship skill the viva examines, and it hinges on framing the dose in plain language. A single paediatric head CT delivers an effective dose of the order of 1 to 2 mSv, comparable to several months of natural background radiation, with an attributable lifetime cancer risk of the order of one excess cancer per several thousand to ten thousand scans — a real but very small increase over the background lifetime cancer risk of roughly one in three. The framing that lands is the comparison: the risk of a justified scan is far smaller than the risk of missing the condition it is looking for, and far smaller than everyday risks a family accepts. The paediatrician documents the justification, the alternatives considered, and the discussion. [3] [1] [2]
Specific Subtypes & Scenarios
Each subtype is the stewardship pathway applied to a common scenario; the steps above resolve each one. [6] [8]
Paediatric CT in acute trauma is the scenario in which a justified ionising scan is non-negotiable. The clinical question — is there an intracranial, thoracic or intra-abdominal injury that needs surgery — is answered by CT in seconds in the unstable child, and the radiation risk is not a reason to delay. The stewardship contribution is to apply the validated decision rule that avoids the scan in the very-low-risk child, and to acquire the justified scan with a single phase and a paediatric protocol. [8]
Serial imaging in the shunted child is the scenario in which the cumulative-dose principle bites hardest. A rapid cranial CT excludes acute hydrocephalus in seconds, but the shunted child will be scanned many times across a lifetime; the modern shift is to rapid MRI protocols (single-shot fast spin-echo sequences) that deliver a diagnostic ventricular image without ionising radiation. Each surveillance request is a stewardship decision, and the baseline scan against which an acute change is read is documented and accessible. [1] [2]
Fluoroscopically guided procedures — vascular access, interventional radiology, cardiac catheterisation, and contrast studies — are the scenarios in which the dose scales with screening time and the cumulative skin dose is watched for deterministic injury. Optimisation means collimating tightly to the region of interest, using the lowest acceptable pulse rate and dose rate, storing the last image-hold and fluoro-loop instead of re-screening, and monitoring the reference air kerma. The diagnostic reference levels of Strauss and colleagues provide the benchmark. [11]
Oncology surveillance is the scenario in which the balance between the radiation dose of surveillance and the detection of recurrence is most acute. The shift towards MRI-based surveillance, and the use of dose-optimised, single-phase CT where CT is unavoidable, is the radiation-aware strategy, and the cumulative dose is tracked across the treatment and follow-up trajectory. [2] [4]
The pregnant adolescent is the scenario in which the modality choice includes the fetus. MRI and ultrasound, which carry no ionising dose, are preferred wherever they answer the question; a justified, optimised ionising scan is performed only when the benefit to the young woman outweighs the small fetal dose, and the dose to the fetus from a distant scan (a head or chest CT) is negligible because of geometric shielding and distance. The request is preceded by a documented pregnancy check and counselling. [9] [12]
Nuclear medicine is the scenario of an internal dose from a radiotracer. Optimisation means using the minimum activity that yields a diagnostic study, choosing the radiopharmaceutical with the lowest effective dose per activity where alternatives exist, and ensuring hydration and timely voiding to reduce the bladder and gonadal dose. The stewardship question is whether a non-ionising modality answers the question before the tracer is administered. [9]
Complications & Pitfalls
The complications and pitfalls of radiation protection and imaging stewardship fall into four categories: the over-imaged child, the under-imaged child, the obsolete practice, and the communication failure. [6] [8]
The over-imaged child is the most common pitfall. The request driven by defensive medicine, by parental anxiety, or by an unexamined protocol accumulates dose across years in the chronic patient and across populations. The counterweight is justification: every request names the clinical question and the expected change in management, and the validated decision rules and Choosing Wisely lists name the requests that are commonly made without benefit. [4] [9]
The under-imaged child is the pitfall at the other extreme, and it is the one the radiation-aware discipline is sometimes unfairly blamed for. A justified, urgent scan is delayed or refused because the radiation risk has been exaggerated to the family, or because the clinician is over-cautious about dose. The lifetime attributable risk of a single paediatric CT is small, and a necessary scan is never withheld on radiation grounds; the discipline is to justify accurately and to communicate the risk honestly. [3] [8]
The obsolete practice is the trap of applying yesterday's protection to today's equipment. The clearest example is routine gonadal shielding, now recommended for discontinuation on modern equipment. Applying an adult CT protocol to an infant, requesting a multiphase scan where a single phase suffices, and relying on bismuth breast shields that interfere with automatic exposure control are further examples. The counterweight is to keep the technique current with the evidence and the equipment. [12]
The communication failure is the trap of the unrecorded discussion. A family that is told the scan is "completely safe", or that is frightened with a risk quoted several orders of magnitude too high, is a family poorly served either way. The accurate plain-language framing — the dose, the comparison with natural background and everyday risk, the alternatives considered — is documented as part of the justification. [3] [1]
Prognosis & Disposition
The disposition after an imaging decision follows the result and the child's clinical state, and the stewardship record travels with the child. [8] [9]
After a scan that was avoided, the disposition is a documented safety-net. The child who met no high-risk criterion and in whom imaging was deferred is discharged or observed with explicit return precautions, and the decision and the safety-net are recorded. This is the most common and the most defensible stewardship outcome. [8]
After a justified ionising scan, the disposition is driven by the result and the cumulative dose is added to the child's imaging history. In the chronic patient, the running total informs the next request, and the threshold to substitute a non-ionising modality falls as the cumulative dose rises. The repeat scan is justified by a change in management, not by habit. [1] [2]
After an elective non-ionising study, the disposition is the communication of the result and the appropriate pathway for a significant or incidental finding — the latter managed without a cascade of unnecessary further ionising imaging, because the stewardship discipline applies to the workup of the incidentaloma as much as to the original request. [9]
Special Populations
Several populations carry a distinct imaging trade-off, and the fellowship viva examines the reasoning. [3] [8]
The neonate and young infant is the population in whom ultrasound through the open fontanelle and the shallow body surface replaces CT for many questions, in whom feed-and-wrap techniques allow MRI without sedation, and in whom the per-scan radiation risk is highest. The threshold to substitute a non-ionising modality is lowest, and the dose-optimisation is most exacting. [7]
The shunted or complex chronic child is the population at greatest cumulative dose, and the radiation-aware intervention is the shift from serial CT to rapid MRI for surveillance, the explicit tracking of the cumulative dose, and the justification of each repeat request against the lifetime total. [1] [2]
The oncology patient is the population in whom the balance between surveillance dose and the detection of recurrence is most acute. The shift towards MRI-based surveillance, and the dose-optimised single-phase CT where CT is unavoidable, is the strategy, and the cumulative dose is audited across the trajectory. [2] [4]
The pregnant adolescent is the population in whom the modality choice includes the fetus. MRI and ultrasound are preferred where they answer the question; a justified ionising scan is preceded by a documented pregnancy check and counselling, and the fetal dose from a distant scan is negligible. [9] [12]
The rural and remote child is the population in whom the stewardship decision is entangled with access. A long transfer to a CT scanner or an MRI is itself a risk, and the decision to image locally with a justified ionising study, to transfer for a non-ionising study, or to defer imaging with a safety-net is made with the access constraint explicit. Tele-radiology and clinical decision support narrow but do not remove the trade-off. [8] [9]
Evidence, Guidelines & Regional Differences
The evidence base for radiation protection and imaging stewardship rests on the risk cohorts and the consensus programmes, and the regional frameworks converge on a shared core with local implementation. [3] [6]
The radiation-risk cohorts quantify the harm the stewardship discipline exists to reduce. Brenner and Hall, in the New England Journal of Medicine in 2007, framed computed tomography as an increasing source of population radiation exposure and projected a small but real attributable cancer burden. Pearce and colleagues, in The Lancet in 2012, reported the United Kingdom retrospective cohort linking CT in childhood to subsequent leukaemia and brain tumours with a dose-response. The Dutch cohort of Meulepas and colleagues, in the Journal of the National Cancer Institute in 2019, refined the estimate with longer follow-up. Miglioretti and colleagues, in JAMA Pediatrics in 2013, quantified the projected population burden of paediatric CT in the United States. None of these forbid CT; together they justify the three pillars and the ALARA principle. [1] [2] [3] [4]
The dose variation evidence drove the benchmarking movement. Smith-Bindman and colleagues, in the Archives of Internal Medicine in 2009, showed wide variation in the dose of common CT examinations and the associated lifetime attributable risk — demonstrating that the same examination delivered very different doses in different centres, and that the dose could be reduced without sacrificing the diagnosis. This is the empirical foundation of the diagnostic reference level. [5]
The consensus and benchmarking programmes operationalised the principle. The Image Gently campaign of Goske and colleagues built the alliance for radiation safety in pediatric imaging and embedded the paediatric CT protocol in routine practice. Brody and colleagues, writing for the American Academy of Pediatrics, set out the radiation risk to children from computed tomography for the general paediatric audience. Frush and Frush codified the ALARA concept as the bridge between radiology and emergency medicine. Hricak and colleagues framed the management of radiation use in medical imaging as a multifaceted challenge spanning technology, policy and education. Kanal and colleagues established the national paediatric CT diagnostic reference levels, and Strauss and colleagues those for paediatric fluoroscopically guided procedures. Thakur and colleagues set out the modern case for discontinuing gonadal and fetal shielding. [6] [7] [8] [9] [10] [11] [12]
The controversies are real but bounded. The magnitude and extrapolation of the low-dose risk — the linear-no-threshold assumption versus a possible threshold — is debated, but the consensus is to operate on the non-threshold assumption because it is the conservative one. The discontinuation of gonadal shielding is recent and is still being adopted; the principle is that protection is achieved by optimisation, not by a shield on an over-dosed exposure. The trade-off between sedation risk and radiation risk in the young child who needs imaging is a per-child decision, made with the family and documented. [3] [12]
Exam Pearls
A candidate who holds these one-liners answers the viva and the single-best-answer question. [3] [8]
- The three pillars are justification, optimisation (ALARA), and dose limitation — and dose limits apply to staff and the public, never to a justified patient investigation.
- The risk is stochastic, non-threshold, and age-sensitive: it rises with dose with no assumed safe threshold (the linear-no-threshold model), and the infant carries a higher per-scan risk than the adult.
- A single paediatric head CT carries an effective dose of the order of 1 to 2 mSv — comparable to months of natural background (around 2 to 3 mSv per year) — and a small attributable lifetime cancer risk of the order of one in several thousand to ten thousand.
- Ultrasound and MRI deliver zero ionising dose, and substituting them is the most effective stewardship lever; CT is the single largest contributor to the paediatric medical radiation burden.
- CTDIvol, DLP and the size-specific dose estimate (SSDE) describe the CT dose; the kerma-area product and the reference air kerma describe the fluoroscopy dose.
- The diagnostic reference level sits at the 75th percentile of the dose distribution — it is a benchmark for review, not a legal limit, and it must be size-stratified in children.
- Optimise with a size-specific paediatric protocol, lower kilovoltage peak, automatic tube current modulation, a limited scan length, a single phase, and iterative reconstruction.
- Routine gonadal shielding is now recommended for discontinuation on modern equipment; shield the staff and the pregnant carer, not the patient's gonads.
- Justify, then communicate: name the clinical question and the change in management, prefer the non-ionising modality where it answers the question, and document the radiation-risk discussion and the pregnancy check.
- A justified, urgent scan is never withheld on radiation grounds alone; the under-imaged child is as much a stewardship failure as the over-imaged child.
References
- [1]Pearce MS, Salotti JA, Little MP, et al Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study Lancet, 2012.PMID 22681860
- [2]Meulepas JM, Ronckers CM, Smets AMJB, et al Radiation Exposure From Pediatric CT Scans and Subsequent Cancer Risk in the Netherlands J Natl Cancer Inst, 2019.PMID 30020493
- [3]Brenner DJ, Hall EJ Computed tomography--an increasing source of radiation exposure N Engl J Med, 2007.PMID 18046031
- [4]Miglioretti DL, Johnson E, Williams A, et al The use of computed tomography in pediatrics and the associated radiation exposure and estimated cancer risk JAMA Pediatr, 2013.PMID 23754213
- [5]Smith-Bindman R, Lipson J, Marcus R, et al Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer Arch Intern Med, 2009.PMID 20008690
- [6]Goske MJ, Applegate KE, Boylan J, et al The Image Gently campaign: working together to change practice AJR Am J Roentgenol, 2008.PMID 18212208
- [7]Brody AS, Frush DP, Huda W, et al Radiation risk to children from computed tomography Pediatrics, 2007.PMID 17766543
- [8]Frush DP, Frush KS The ALARA concept in pediatric imaging: building bridges between radiology and emergency medicine Pediatr Radiol, 2008.PMID 18810422
- [9]Hricak H, Brenner DJ, Adelstein SJ, et al Managing radiation use in medical imaging: a multifaceted challenge Radiology, 2011.PMID 21163918
- [10]Kanal KM, Butler PF, Chatfield MB, et al U.S. Diagnostic Reference Levels and Achievable Doses for 10 Pediatric CT Examinations Radiology, 2022.PMID 34928733
- [11]Strauss KJ, Racadio JM, Johnson N, et al Estimates of diagnostic reference levels for pediatric peripheral and abdominal fluoroscopically guided procedures AJR Am J Roentgenol, 2015.PMID 26001261
- [12]Thakur Y, Schofield SC, Bjarnason TA, et al Discontinuing Gonadal and Fetal Shielding in X-Ray Can Assoc Radiol J, 2021.PMID 33573394