Paeds · growth-development-and-behaviour
Attention-deficit hyperactivity disorder
Also known as ADHD · Attention-deficit/hyperactivity disorder · Attention deficit hyperactivity disorder · Hyperkinetic disorder · ADD · Attention deficit disorder
Fellowship guide to paediatric ADHD: multi-setting diagnosis, differentials including sleep and learning mimics, age-banded multimodal care, stimulant and non-stimulant frameworks with monitoring, comorbidity, school partnership, regional pathway differences and exam pearls.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the child who is bright but cannot finish a worksheet, who loses every jumper, who blurts answers, who is exhausted by homework battles, or who looks “fine” in a quiet clinic and falls apart in a busy classroom. That functional story — not a single teacher email — is the starting point for ADHD assessment. [1] [2]
ADHD is a neurodevelopmental condition. Persistent inattention and/or hyperactivity-impulsivity are inconsistent with developmental level, present for months, appear in two or more settings, and cause clear impairment in learning, safety, relationships or family life. It is not laziness, not a moral failure, and not a score on a questionnaire alone. [1] [9] [11]
International consensus statements summarise a large evidence base that ADHD is a valid clinical construct with genetic, developmental and functional consequences when untreated. Your job as a general paediatrician is not to debate whether ADHD “exists”, but to diagnose carefully, avoid both under- and over-labelling, and build a plan the family and school can actually run. [11] [12]
Classification
Current teaching uses presentation type as a cross-section of symptoms now, not a lifetime tattoo. Combined presentation meets both inattention and hyperactivity-impulsivity thresholds. Predominantly inattentive presentation meets only the inattention threshold. Predominantly hyperactive-impulsive presentation meets only the hyperactivity-impulsivity threshold. Severity and partial remission are separate axes — a teenager may no longer leave their seat constantly yet still fail every deadline. [1] [2]
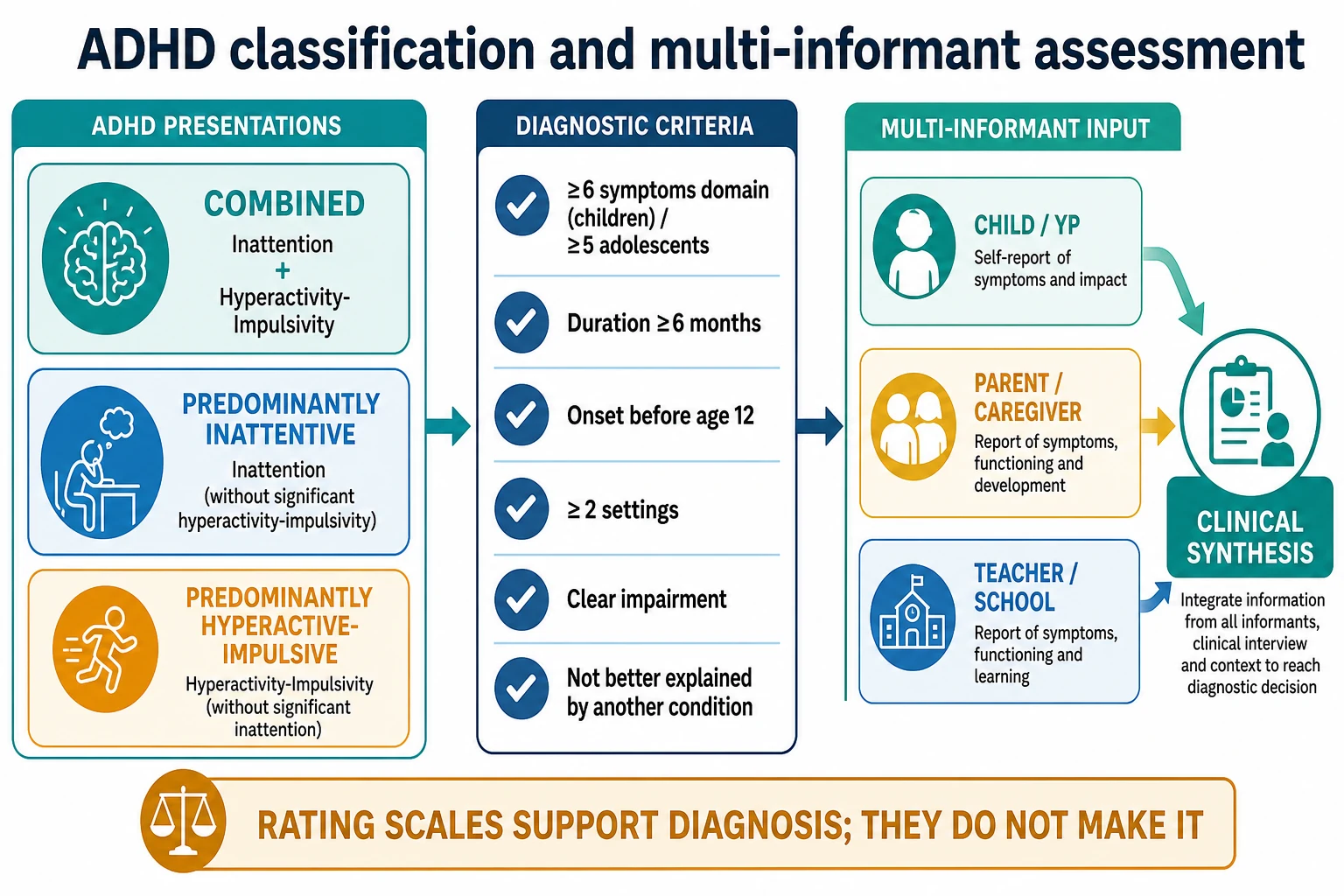
Diagnostic criteria framework (exam-level DSM-5-TR style). For children, require six or more inattention symptoms and/or six or more hyperactivity-impulsivity symptoms for at least six months. For older adolescents and adults, many frameworks use a five-symptom threshold in a domain. Symptoms must have been present before age 12, occur in two or more settings, cause clear interference, and not be better explained by another mental or medical condition. ICD-11 similarly frames inattentive, hyperactive-impulsive and combined presentations and allows careful adult diagnosis when developmental history supports childhood onset. [1] [2] [28]
Combined
Both domains threshold
- Common clinic presentation in school-age boys
- Often the MTA-style phenotype
- Hyperactivity may internalise with age
- High functional impact at home and school
Predominantly inattentive
Inattention threshold only
- Often missed in girls
- Daydreaming, unfinished work, time-blindness
- Homework and organisation failures dominate
- Common residual adolescent/adult pattern
Predominantly hyperactive-impulsive
Hyperactivity-impulsivity threshold only
- More visible in younger children
- Injury and social friction risk
- Often evolves toward combined or residual inattentive features
- Still requires multi-setting impairment
Historical trap. DSM-IV used onset before age 7. DSM-5/DSM-5-TR moved the threshold to before age 12. Quoting “before 7” loses easy marks. [1] [9]
Epidemiology & Risk Factors
Worldwide childhood prevalence sits near 5% in metaregression work that accounts for study methods; local clinic rates vary with referral filters and diagnostic practice. Adult residual prevalence is lower but still substantial in population surveys. Clinic-referred children are more often boys; the sex ratio narrows later as inattentive presentations are recognised. [6] [25]
Headline numbers for viva
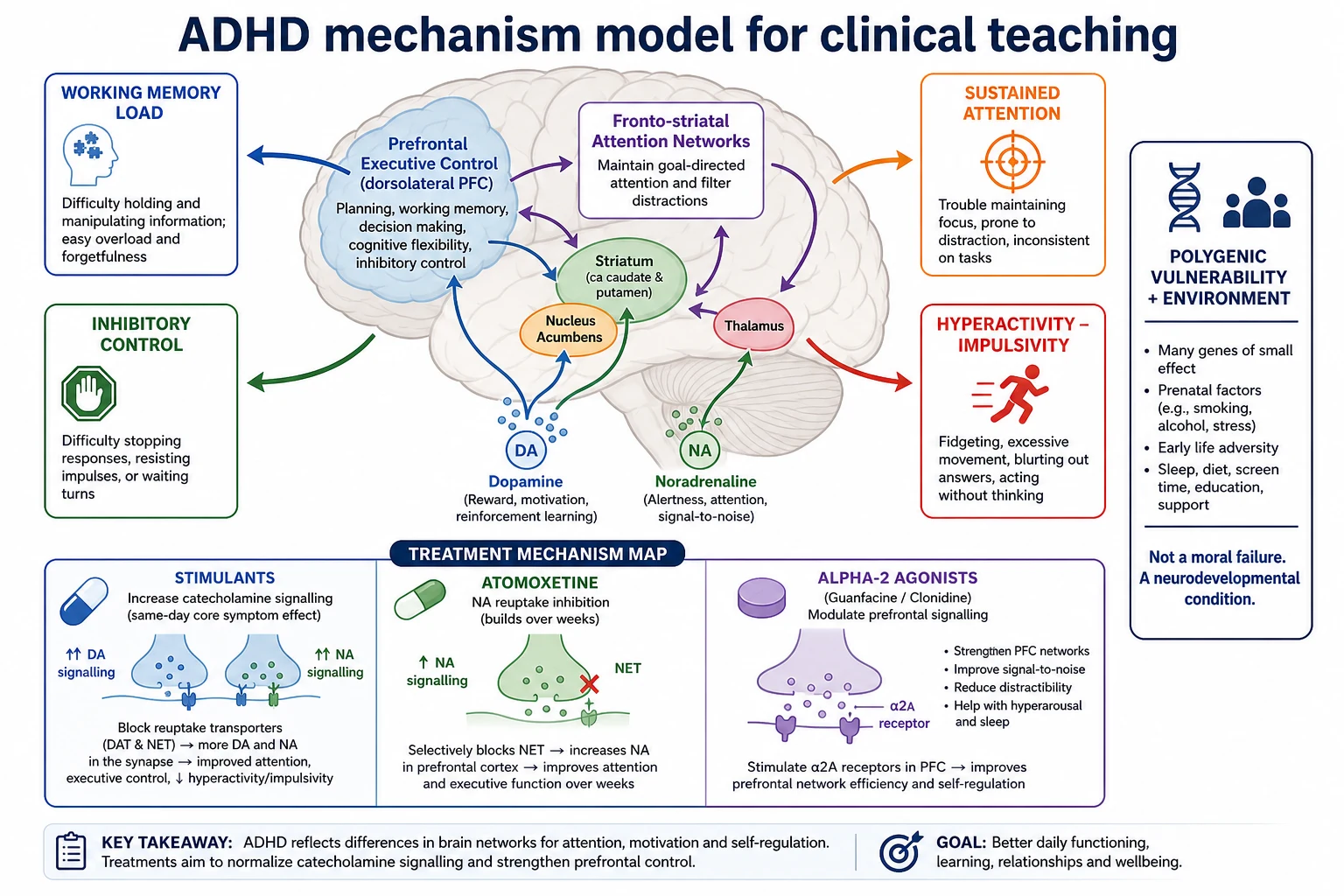
Heritability is high and polygenic. Family history is a risk clue, not destiny. Prenatal exposures, prematurity, psychosocial adversity and chaotic environments can amplify phenotype. Poverty, racism, language barriers and school mismatch change who gets labelled and who gets support. Overdiagnosis and underdiagnosis coexist — careful multi-setting assessment is the antidote, not cynicism or automatic prescribing. [7] [11] [12] [30]
Pathophysiology
You do not need a molecular monologue in clinic. You do need a working model that explains symptoms and drug classes. Executive-function research links ADHD to difficulties with inhibitory control, working memory and cognitive flexibility, without claiming a single deficit explains every child. Catecholamine signalling in fronto-striatal networks is the teaching bridge to stimulants (which increase synaptic dopamine/noradrenaline signalling with often same-day core-symptom effect) and to atomoxetine (noradrenaline reuptake inhibition with benefit building over weeks). [2] [3] [8]
Sleep debt, iron deficiency, chronic stress and classroom mismatch can amplify ADHD-like behaviour. Treat those amplifiers, but do not dismiss true multi-setting developmental ADHD as “just sleep” when the developmental story is long and impairing. [1] [20]
Clinical Presentation
Preschool. High activity is common. Worry more when regulation is extreme across settings, when safety is repeatedly compromised, and when caregivers cannot manage despite consistent strategies. Many preschool presentations still deserve behavioural support first rather than immediate medication. [1] [21]
School-age. Combined presentations show unfinished work, lost belongings, calling out, playground friction and homework wars. Predominantly inattentive children — especially girls — may look quiet, “spacey” or underachieving while internal work is chaotic. Teachers often notice first; parents may have adapted at home and under-report until secondary school load rises. [1] [2]
Adolescent. Outward hyperactivity often softens into inner restlessness. Organisation failure, late assignments, conflict, risky driving, substance exposure and mood symptoms dominate. Partial remission of childhood criteria can still leave major functional impairment. [23] [27] [28]
| Presentation story | Do not stop here | Must still map |
|---|---|---|
| 'Only at school' | May still be ADHD if school is the only structured demand setting | Sleep, vision/hearing, learning disorder, classroom fit, bullying |
| 'Lazy / unmotivated' | Motivation language often hides executive failure | Task initiation, working memory, anxiety, depression |
| 'Fine in clinic' | Short visits under-sample attention load | Teacher report, homework samples, multi-setting history |
| 'Screen time caused this' | Screens may worsen sleep and regulation | Developmental onset timeline before device use |
| 'Sibling is worse' | Relative comparison is not a threshold | Absolute impairment and safety risk |
Differential Diagnosis
Build the differential in four piles: what looks like ADHD but is reversible, what coexists with ADHD, what is dangerous to miss, and what is normal development. Sleep insufficiency is the classic reversible mimic — a school-age child sleeping far under AASM consensus needs is not ready for a stimulant trial until sleep opportunity is fixed or a sleep disorder pathway is clear. [1] [20]
Reversible mimics
- Short sleep or delayed sleep phase
- Uncorrected vision or hearing problems
- Iron deficiency or thyroid disease when clinically indicated
- Medication or substance effects
- Acute grief, chaos or school trauma
Common co-travellers
- Specific learning disorder
- Anxiety or depression
- Autism and language disorders
- ODD / conduct problems
- Tics; developmental coordination difficulties
Can't-miss alternatives
- Absence seizures presenting as 'daydreaming'
- Significant substance use
- Bipolar spectrum or emerging psychosis
- Safeguarding / trauma presentations
- Lead or other toxic exposures in high-risk contexts
Oppositional behaviour can be secondary to ADHD frustration or a separate ODD pathway. Canadian guidance on disruptive and aggressive behaviour stresses treating ADHD when present as part of aggression management, rather than jumping straight to antipsychotics. [19]
Overdiagnosis literature warns that expanding labels, single-informant diagnoses and school pressure can inflate prevalence without true multi-setting impairment. That is an argument for better diagnosis, not for refusing care to children who clearly meet criteria. [12]
Clinical & Bedside Assessment
Structure every assessment the same way so you do not skip a domain under time pressure. [1] [9]
Bedside ADHD assessment sequence
Child and young person voice first
Ask about school, friends, sleep, worries and what they want help with. Private time for adolescents when safe.
Developmental symptom map
Walk inattention and hyperactivity-impulsivity domains with age-appropriate examples and onset before 12.
Multi-setting function
Home, classroom, playground, homework, sport, community and safety. Seek teacher information in writing when possible.
Mimic and comorbidity screen
Sleep duration and snoring, vision/hearing, learning, anxiety, mood, autism traits, tics, substances, trauma, safeguarding.
Examination and baselines
Growth, BP, HR, focused neurodevelopmental exam, cardiac history before medication, hearing/vision pathway as indicated.
Synthesis and shared plan
State the working diagnosis, uncertainty, supports now, medication decision if any, school partnership and review date.
Tools support diagnosis; they do not make it. Vanderbilt, Conners, SNAP-IV and ADHD rating scales help baseline and response tracking. A high score from one teacher with a calm home and normal sleep is a hypothesis, not a prescription. Complex ADHD — marked comorbidity, diagnostic uncertainty, treatment resistance — benefits from SDBP-style comprehensive pathways rather than primary-care-only titration. [1] [9] [10]
Use professional interpreters for language-discordant families. Caregiver history quality and consent quality both fall when you rely on a child as translator. [30]
Investigations
There is no diagnostic blood test, EEG or MRI for uncomplicated ADHD. Investigations exist to find mimics, comorbidity and medication safety issues. [1] [9]
Before medication. Plot height and weight. Measure blood pressure and heart rate with an appropriate cuff. Take personal cardiac history (exertional chest pain, unexplained syncope, known congenital heart disease) and family history of sudden cardiac death or serious arrhythmia. Large cohorts have not shown a clear population excess of serious cardiovascular events with ADHD drugs, but individual risk assessment still matters and ECG is used when history or examination raises concern rather than as a universal reflex. [1] [15] [16]
Consider ferritin/FBC, TSH, audiology, vision assessment, sleep evaluation and formal psychoeducational testing when the history points there. Urine drug screen when substance use is plausible. Neuroimaging or EEG only for neurological red flags such as seizures, focal signs or regression — not routine. [1] [9] [10]
Management — Resuscitation
ADHD itself is rarely the emergency. The emergencies are comorbid crises: suicidal ideation, severe aggression with injury risk, stimulant intoxication or diversion crisis, unsafe adolescent driving, and safeguarding emergencies. Stabilise safety first. Do not start a stimulant into an unexamined bipolar, psychotic or heavy substance-use landscape. [1] [18] [27]
Management — Definitive & Stepwise
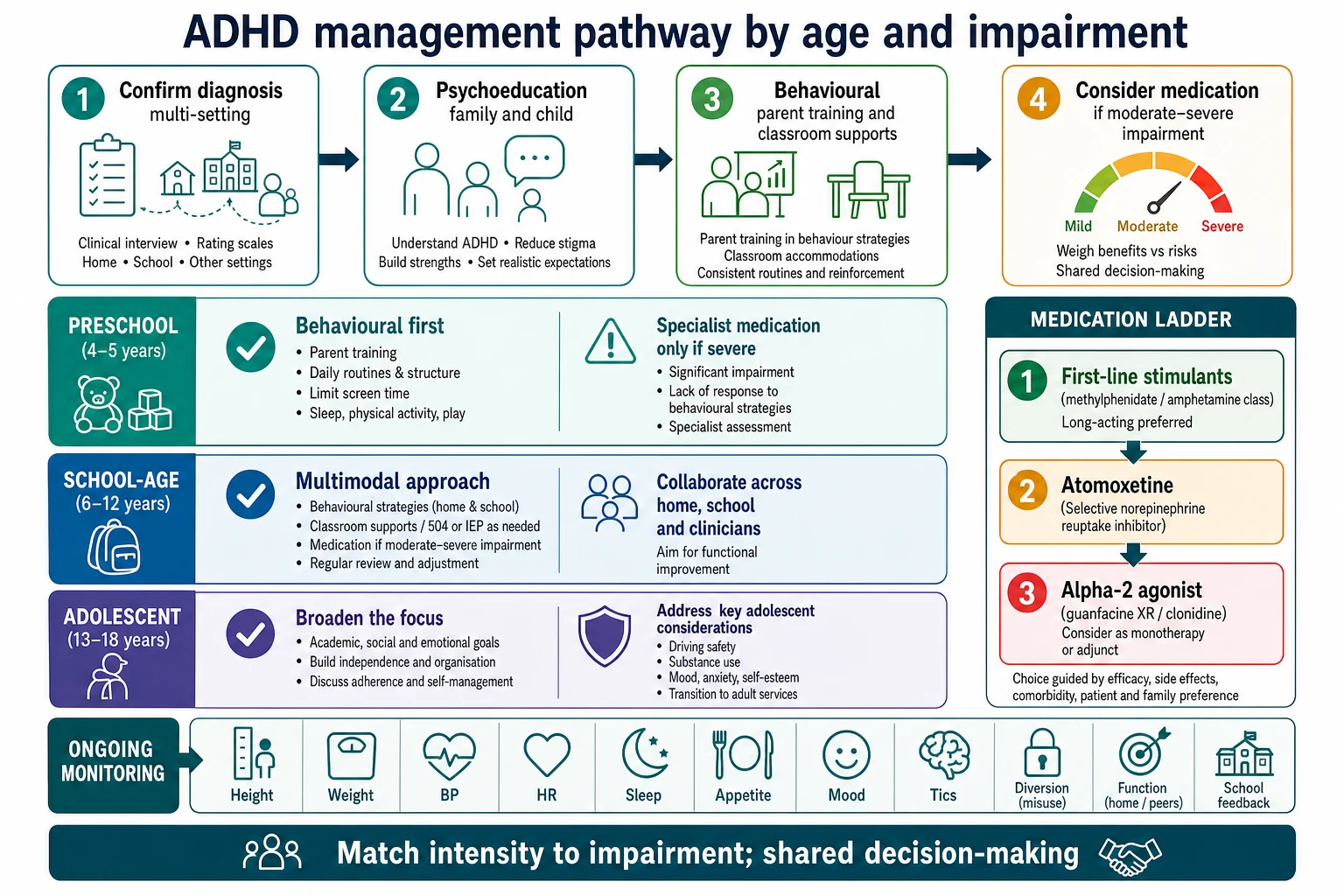
Match intensity to impairment. Every family needs psychoeducation: ADHD is real, treatable and not the child’s fault or the parent’s moral failure. Behavioural parent training and classroom strategies are foundational in childhood. School accommodations — preferential seating, chunked tasks, movement breaks, extended time, clear instructions — reduce impairment even when medication is used. [1] [4] [9]
Age bands (AAP-aligned teaching)
Preschool (4–5 years). Evidence-based parent training and behavioural interventions first. Medication is specialist territory after careful diagnosis when impairment is severe and behavioural therapy has not been sufficient or is not available. [1]
Elementary school-age. For moderate to severe ADHD, FDA-approved medications have the strongest short-term effect on core symptoms, ideally combined with behavioural and educational supports. Methylphenidate class agents are commonly first-line in many paediatric pathways; amphetamine-class agents are alternatives. [1] [3] [22]
Adolescents. Same multimodal logic, with explicit adherence work, diversion counselling, substance education, mood screening and driving advice. Shared decision-making with the young person is essential. [1] [27] [28]
Stimulants — exam frameworks
Network meta-analysis shows most ADHD medications outperform placebo for core symptoms at about 12 weeks; stimulants generally show the largest effect sizes, with methylphenidate highly effective in children and adolescents. Cochrane review evidence supports methylphenidate efficacy while highlighting study-quality limits — use that nuance in viva. [3] [22]
| Agent class | Typical exam start framework | Titration / range notes | Key teaching points |
|---|---|---|---|
| Methylphenidate IR | Often 5 mg orally 2–3 times daily in school-age children | Titrate weekly; many labels max around 60 mg/day (check product information) | Short coverage; higher diversion risk than long-acting |
| Methylphenidate long-acting | Product-specific morning dose | Titrate to school-day coverage and function | Prefer for adherence and lower diversion |
| Lisdexamfetamine | Often 20–30 mg orally each morning | Titrate weekly; common max 70 mg/day on many labels | Prodrug; useful when diversion risk is a concern |
| Dexamfetamine / mixed amphetamine salts | Low morning start; product-specific | Divide IR doses; titrate carefully | Strong efficacy signal; monitor appetite/sleep |
| These are exam-level frameworks — always individualise for age, formulation, comorbidities and local product information or authority rules. [1] [3] [9] |
Onset teaching point. Stimulant benefit on core symptoms is often evident the same day at an adequate dose. Use that fact when judging early response. [3] [9]
Atomoxetine
Atomoxetine is a non-stimulant noradrenaline reuptake inhibitor useful when stimulants are poorly tolerated, contraindicated, diversion risk is high, or continuous coverage without a controlled drug is preferred. In the pivotal once-daily RCT, atomoxetine separated from placebo over weeks, not hours. [13]
Dosing framework. Approximate start 0.5 mg/kg/day orally for at least 3 days, then increase toward a target near 1.2 mg/kg/day; usual maximum about 1.4 mg/kg/day or 100 mg/day (whichever is less) in many product labels — confirm local PI. Counsel on gastrointestinal upset, fatigue, rare hepatic injury (stop if jaundice or dark urine), and mood/suicidality monitoring in youth. [1] [13]
Guanfacine XR and clonidine
Extended-release guanfacine has placebo-controlled RCT evidence in children and adolescents. It is useful as monotherapy alternative or adjunct, and is often discussed when tics, aggression or sleep-onset problems complicate the picture. [14]
Guanfacine XR framework. Often start 1 mg orally once daily, increase by 1 mg/week as tolerated; trial ranges commonly 1–4 mg/day (higher adolescent maxima exist on some labels). Monitor for sedation, hypotension and bradycardia; taper after prolonged use rather than stopping abruptly. Clonidine (including extended-release where available) is a related alpha-2 option with more sedation. [1] [14]
Monitoring schedule
At baseline and follow-up track height/weight, BP, HR, appetite, sleep, tics, mood/anxiety/irritability, adherence, diversion signals (early refills, lost scripts), school function and substance use. Review more often after initiation or dose changes, then space visits when stable. [1] [15] [16]
Australian and New Zealand practice follows local stimulant prescribing authority and shared-care norms that vary by jurisdiction and age. State principles in exams: specialist initiation or endorsement where required, documented diagnosis, monitoring plan, and GP shared care when stable. Do not invent a single national form number. [1]
Specific Subtypes & Scenarios
Preschool severe impairment. Maximise parent training, early childhood supports and safety planning. Medication only under specialist oversight after failed or unavailable behavioural care. [1]
School-age ADHD plus learning disorder. Treat ADHD and pursue psychoeducational assessment; medication alone will not teach decoding. Coordinate IEP/learning-support language with the school. [1] [10]
Inattentive girl with anxiety. Do not miss either diagnosis. Anxiety can look like inattention; untreated ADHD can feed anxiety. Sequence care by dominant impairment and safety. [1] [10]
ADHD with tics. Stimulants are often still usable with monitoring; alpha-2 agonists can help both ADHD and tics in selected children. [1] [14]
ADHD with aggression/ODD. Optimise ADHD treatment and behavioural strategies first; Canadian disruptive-behaviour guidance supports careful adjunctive pharmacotherapy only after ADHD treatment and behavioural foundations. [19]
Adolescent diversion or SUD risk. Prefer supervised long-acting formulations or non-stimulants; treat substance use in parallel; counsel driving risk. Meta-analysis does not support the myth that stimulant therapy causes later substance abuse; untreated ADHD raises SUD risk. [17] [18] [27]
Complex ADHD. Multimorbidity, diagnostic uncertainty or treatment resistance belongs on an SDBP-style comprehensive pathway with allied health and mental-health partners. [10]
Language-discordant or refugee families. Use interpreters, gather school history carefully, and avoid mistaking trauma or interrupted schooling for primary ADHD without developmental timeline. [12] [30]
Complications & Pitfalls
Classic errors: diagnosing from one questionnaire; missing sleep or sensory deficits; starting short-acting stimulants into a diversion network; ignoring growth charts; promising a cure; stopping treatment the week exams finish without functional review; omitting driving advice; using stigmatising language that the child is “naughty”. [1] [12] [27]
Within-individual Swedish registry analyses found lower rates of criminality during periods of ADHD medication use versus non-medication periods — useful for discussing functional benefits, not for claiming medication alone prevents all crime. [26]
ADHD also associates with higher obesity risk in meta-analytic work; address sleep, impulsivity around food and activity without weight stigma. [24]
Prognosis & Disposition
A substantial minority remit; many have partial remission with residual inattention and executive impairment into adolescence and adulthood. Severity, comorbidity and adversity predict worse trajectories. Disposition ranges from shared-care primary follow-up on stable long-acting medication to specialist clinics for complex comorbidity, SUD risk or diagnostic uncertainty. Define response by function — learning, peer safety, family stress, self-esteem — not only a parent scale score. [5] [23] [28]
Plan titration reviews tightly, then maintenance monitoring with open access for crisis comorbidity. Transition planning for residual adult ADHD should start before the young person falls out of paediatric care. [1] [28]
Special Populations
Girls and women need active case-finding for inattentive presentations. Children with autism or intellectual disability need adapted tools and careful dual diagnosis without diagnostic overshadowing. Out-of-home care and multiple caregivers raise both true ADHD risk and label risk — demand multi-setting evidence. Indigenous and migrant families need culturally safe assessment and equity of access, not stereotype-based diagnosis. Rural-remote care may use telehealth for follow-up but still needs reliable growth/vitals measurement and clear shared-care ownership. [1] [10] [12] [30]
Evidence, Guidelines & Regional Differences
MTA one-liner. At 14 months, carefully managed medication (alone or combined) beat behavioural treatment alone for core ADHD symptoms; combination helped broader outcomes and sometimes lower dose. At 8 years, initial randomisation advantages attenuated — early gains do not guarantee lifelong automatic remission. [4] [5]
Cardiac safety one-liner. Cooper cohort work did not demonstrate increased serious cardiovascular events overall; Hennissen meta-analysis quantifies small mean increases in BP/HR with stimulants and atomoxetine — monitor, do not panic, and individualise cardiac work-up. [15] [16]
Pandemic-era European ADHD Guidelines Group advice reinforced continuity of care, remote monitoring pragmatism and avoiding abrupt treatment gaps — principles that still apply to telehealth shared care. [29]
Exam Pearls
FOCUS
Self-test: school-age moderate-severe ADHD plan
Psychoeducation + classroom strategies + parent behavioural supports + long-acting methylphenidate product-specific morning start with weekly titration; monitor height/weight, BP, HR, appetite, sleep, mood/tics and diversion; review teacher and parent function. If stimulants fail or are unsuitable: atomoxetine toward about 1.2 mg/kg/day or guanfacine XR from 1 mg with BP/HR/sedation checks. [1] [3] [13] [14]
References
- [1]Wolraich ML Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics, 2019.PMID 31570648
- [2]Posner J Attention-deficit hyperactivity disorder. Lancet (London, England), 2020.PMID 31982036
- [3]Cortese S Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry, 2018.PMID 30097390
- [4]The MTA Cooperative Group A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. The MTA Cooperative Group. Multimodal Treatment Study of Children with ADHD. Archives of general psychiatry, 1999.PMID 10591283
- [5]Molina BSG The MTA at 8 years: prospective follow-up of children treated for combined-type ADHD in a multisite study. Journal of the American Academy of Child and Adolescent Psychiatry, 2009.PMID 19318991
- [6]Polanczyk G The worldwide prevalence of ADHD: a systematic review and metaregression analysis. The American journal of psychiatry, 2007.PMID 17541055
- [7]Faraone SV Molecular genetics of attention-deficit/hyperactivity disorder. Biological psychiatry, 2005.PMID 15950004
- [8]Willcutt EG Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biological psychiatry, 2005.PMID 15950006
- [9]Pliszka S Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 2007.PMID 17581453
- [10]Barbaresi WJ Society for Developmental and Behavioral Pediatrics Clinical Practice Guideline for the Assessment and Treatment of Children and Adolescents with Complex Attention-Deficit/Hyperactivity Disorder. Journal of developmental and behavioral pediatrics : JDBP, 2020.PMID 31996577
- [11]Faraone SV The World Federation of ADHD International Consensus Statement: 208 Evidence-based conclusions about the disorder. Neuroscience and biobehavioral reviews, 2021.PMID 33549739
- [12]Kazda L Overdiagnosis of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents: A Systematic Scoping Review. JAMA network open, 2021.PMID 33843998
- [13]Michelson D Once-daily atomoxetine treatment for children and adolescents with attention deficit hyperactivity disorder: a randomized, placebo-controlled study. The American journal of psychiatry, 2002.PMID 12411225
- [14]Sallee FR Guanfacine extended release in children and adolescents with attention-deficit/hyperactivity disorder: a placebo-controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 2009.PMID 19106767
- [15]Cooper WO ADHD drugs and serious cardiovascular events in children and young adults. The New England journal of medicine, 2011.PMID 22043968
- [16]Hennissen L Cardiovascular Effects of Stimulant and Non-Stimulant Medication for Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis of Trials of Methylphenidate, Amphetamines and Atomoxetine. CNS drugs, 2017.PMID 28236285
- [17]Wilens TE Does stimulant therapy of attention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic review of the literature. Pediatrics, 2003.PMID 12509574
- [18]Wilens TE Attention deficit hyperactivity disorder and substance use disorders. The American journal of psychiatry, 2006.PMID 17151154
- [19]Gorman DA Canadian guidelines on pharmacotherapy for disruptive and aggressive behaviour in children and adolescents with attention-deficit hyperactivity disorder, oppositional defiant disorder, or conduct disorder. Canadian journal of psychiatry. Revue canadienne de psychiatrie, 2015.PMID 25886657
- [20]Paruthi S Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine, 2016.PMID 27250809
- [21]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [22]Storebø OJ Methylphenidate for children and adolescents with attention deficit hyperactivity disorder (ADHD). The Cochrane database of systematic reviews, 2023.PMID 36971690
- [23]Sibley MH Defining ADHD symptom persistence in adulthood: optimizing sensitivity and specificity. Journal of child psychology and psychiatry, and allied disciplines, 2017.PMID 27642116
- [24]Cortese S Association Between ADHD and Obesity: A Systematic Review and Meta-Analysis. The American journal of psychiatry, 2016.PMID 26315982
- [25]Kessler RC The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. The American journal of psychiatry, 2006.PMID 16585449
- [26]Lichtenstein P Medication for attention deficit-hyperactivity disorder and criminality. The New England journal of medicine, 2012.PMID 23171097
- [27]Vaa T ADHD and relative risk of accidents in road traffic: a meta-analysis. Accident; analysis and prevention, 2014.PMID 24238842
- [28]Kooij JJS Updated European Consensus Statement on diagnosis and treatment of adult ADHD. European psychiatry : the journal of the Association of European Psychiatrists, 2019.PMID 30453134
- [29]Cortese S ADHD management during the COVID-19 pandemic: guidance from the European ADHD Guidelines Group. The Lancet. Child & adolescent health, 2020.PMID 32311314
- [30]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387