Paeds · respiratory-sleep-and-airway
Acute severe and life-threatening asthma
Also known as Acute severe asthma · Life-threatening asthma · Near-fatal asthma · Status asthmaticus · Acute asthma exacerbation
Fellowship guide to acute severe and life-threatening asthma in children: grading severity from the whole child, the pathophysiology of the failing airway, the stepwise escalation from oxygen and continuous salbutamol through ipratropium and systemic steroid to IV magnesium, IV salbutamol or aminophylline and PICU, recognising the silent chest and the exhausted child, avoiding the pitfalls that kill, and the ANZ, UK and North American guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the eight-year-old carried into the resus bay hunched forward, too breathless to answer you, using every accessory muscle, with a chest that is wheezing everywhere and oxygen saturations of 88% on air. His mother says his reliever stopped working an hour ago. That scene — a child in obvious respiratory distress from asthma who is no longer responding to their usual treatment — is acute severe asthma, and the speed and order of what you do next decides whether he improves or arrests. [1] [11]
Acute severe asthma is an exacerbation of asthma severe enough that inhaled bronchodilator alone is failing and the child shows objective signs of serious airflow limitation: inability to talk in sentences, marked work of breathing, tachypnoea and tachycardia, and hypoxaemia. Life-threatening asthma is the next tier — a silent chest, poor respiratory effort, cyanosis, exhaustion, confusion or hypotension — and near-fatal asthma describes the child with a raised PaCO₂ who needs mechanical ventilation. [1] [12]
Why this matters at fellowship level is that asthma is one of the commonest paediatric emergencies, most exacerbations respond well to prompt inhaled therapy and steroid, and the deaths are largely preventable — they cluster in children whose severity was underestimated, whose treatment was delayed, or whose deterioration was misread. The skill being tested is recognising severity early, escalating in the right order, and never mistaking a fading child for a recovering one. [11] [12]
Classification
Grade acute asthma two ways at once: how obstructed the child is right now and whether the airway is merely severe or has crossed into life-threatening territory, because that judgement drives the whole escalation pathway. [1] [12]
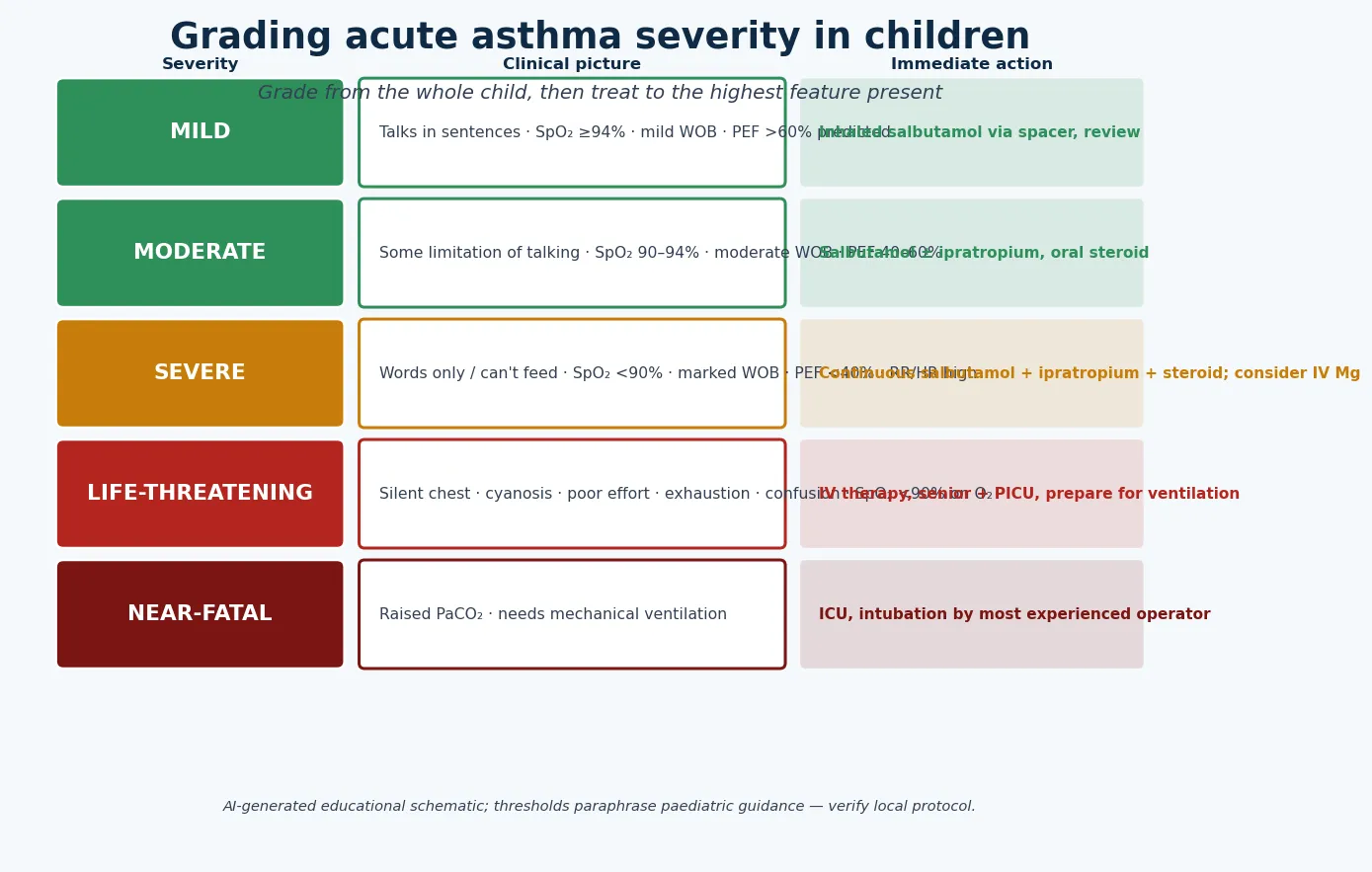
Mild and moderate exacerbations are children who are still talking, saturating at or above 90%, and working only mild-to-moderately hard; they usually respond to inhaled salbutamol via a spacer and a course of oral corticosteroid. Severe asthma is the child who can manage only words or single phrases, is saturating below 90% or working very hard, and needs continuous bronchodilator, ipratropium and systemic steroid with early thought about intravenous therapy. [1] [12]
Life-threatening asthma is defined by the ominous signs — a silent chest, cyanosis, feeble respiratory effort, exhaustion, agitation or a reduced conscious level, and persisting hypoxaemia despite oxygen. Near-fatal asthma adds a raised or rising PaCO₂ and the need for ventilatory support. These categories are a shared language for escalation, not an arithmetic gate, and a child can move between them within minutes. [1] [11]
The numbers that anchor your viva
Epidemiology & Risk Factors
Acute asthma is a leading cause of paediatric emergency presentations and hospital admission, peaking in school-age children and in the autumn and winter viral seasons; most children recover fully, but a small number deteriorate to life-threatening disease and, rarely, to death. [11] [1]
The children who die or come close share recognisable features. A previous near-fatal episode (an ICU admission or the need for ventilation), a recent hospital admission or emergency visit, heavy reliever use with poor preventer adherence, and a background of poorly controlled or "brittle" asthma all mark a child at higher risk of a severe or fatal exacerbation. Psychosocial adversity, food allergy, and a failure to recognise or act on deterioration compound that risk. [1] [11]
The precipitants are usually the familiar triggers writ large: a respiratory virus (by far the commonest), allergen exposure, exercise, air pollution or smoke, and abrupt cessation of preventer therapy. The child who runs out of, or stops responding to, their reliever and keeps re-dosing without improvement is the classic path to a severe presentation. [1] [12]
Pathophysiology
The teaching model runs from the trigger to the failing airway, and it turns on three simultaneous processes that narrow the bronchi and one consequence — air trapping — that does most of the harm. [1] [12]
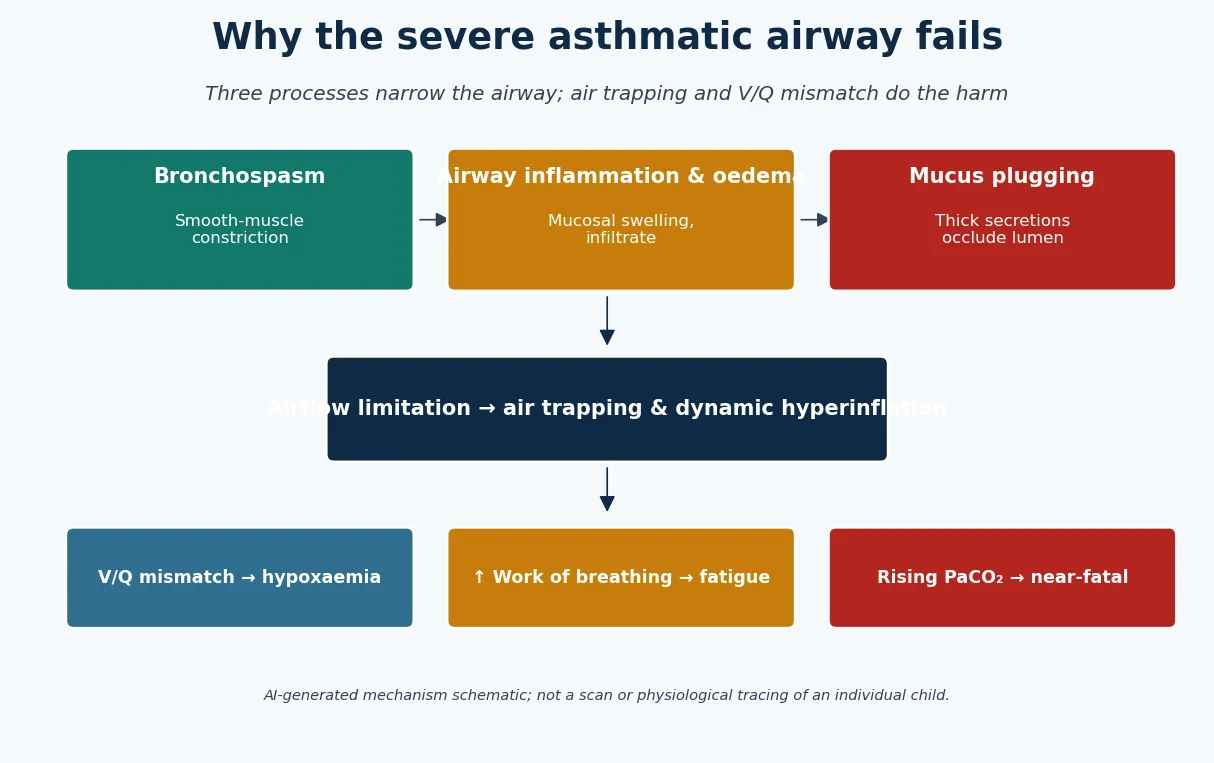
A trigger, most often a respiratory virus, provokes bronchial smooth-muscle constriction, mucosal inflammation and oedema, and increased mucus secretion. Together these narrow the airway lumen, and because resistance to airflow rises steeply as the radius falls, even modest narrowing sharply increases the work of breathing and turns smooth flow into the turbulent flow heard as wheeze. [1] [12]
The dangerous physiology is expiratory. The narrowed airways collapse and obstruct on expiration, so the child cannot empty the lungs before the next breath; air is trapped, the chest becomes hyperinflated, and each breath starts from a mechanically disadvantaged position. Ventilation–perfusion mismatch produces hypoxaemia, while the escalating work of breathing drains the child's reserves. [1] [12]
A common misconception is that the loudest chest is the sickest. In fact, as obstruction becomes critical, air movement falls and the wheeze quietens: the silent chest signals dangerously reduced ventilation, and confusing it with improvement is one of the ways children die. [1] [12]
Clinical Presentation
The classic presentation is a child, often with a viral coryza, whose wheeze and breathlessness have escalated over hours to days despite increasing reliever use, now in obvious distress and no longer responding to salbutamol at home. The single most useful assessment is to gauge severity from the end of the bed before you touch the child. [1] [11]
Watch the ability to talk (sentences, phrases, words, or not at all), the respiratory rate and effort, the use of accessory muscles and subcostal or intercostal recession, the colour, the alertness, and the oxygen saturation. Auscultation adds the character of the wheeze and, crucially, the quality of air entry — a widespread wheeze that becomes quiet is a warning, not a reassurance. [1] [12]
| Severity | Bedside picture | Immediate action |
|---|---|---|
| Mild–moderate | Talks in sentences/phrases, SpO₂ ≥ 90%, mild-to-moderate work of breathing | Inhaled salbutamol via spacer, oral corticosteroid, reassess |
| Severe | Words only or cannot feed, SpO₂ < 90%, marked work of breathing, tachycardia | Oxygen, continuous salbutamol + ipratropium + systemic steroid; consider IV magnesium |
| Life-threatening | Silent chest, cyanosis, poor effort, exhaustion, confusion, SpO₂ < 90% on oxygen | IV therapy, senior + anaesthetic + PICU, prepare for ventilation |
| Near-fatal | Raised/rising PaCO₂, needs ventilatory support | ICU, controlled intubation by the most experienced operator |
The trap is the exhausted, quiet child. A youngster who was noisy, distressed and tachypnoeic and who becomes still, drowsy and quiet with a softening wheeze is not settling — the reduced noise and effort reflect fatigue and falling ventilation. Drowsiness, confusion or a feeble respiratory effort in an acutely asthmatic child is a peri-arrest state. [1] [11]
Presentations that should make you think twice about the diagnosis include a very sudden onset with choking (foreign body), focal signs or asymmetry (pneumothorax, foreign body or consolidation), a first-ever wheeze in an infant (bronchiolitis or a congenital cause), and stridor rather than wheeze (an upper-airway problem). Each points away from a simple asthma exacerbation. [1] [12]
Differential Diagnosis
Sort the differential into the mimics that obstruct the lower airway, the mimics that obstruct the upper airway, and the complications of asthma itself. The aim is to treat the severe asthmatic confidently while never anchoring on asthma in the child whose story or signs do not fit. [1] [12]
Acute severe asthma
the usual answer
- Known asthma or recurrent wheeze
- Expiratory wheeze, prolonged expiration
- Responds (at least partly) to salbutamol
- Escalates with the classic pathway
Anaphylaxis
- Sudden onset after exposure
- Urticaria, angio-oedema, hypotension
- Wheeze plus other systems involved
- Give IM adrenaline first
Foreign body / pneumothorax
- Sudden choke or asymmetry
- Focal or unilateral signs
- Poor response to bronchodilator
- Imaging and senior review
Upper airway / other
- Stridor not wheeze (croup, anaphylaxis)
- Bronchiolitis in the young infant
- Cardiac failure, aspiration
- Story and age guide you
Anaphylaxis is the can't-miss mimic: wheeze that comes on suddenly after an exposure, especially with urticaria, angio-oedema, vomiting or hypotension, is anaphylaxis until proven otherwise, and it needs intramuscular adrenaline first — not just bronchodilator. Treating anaphylactic bronchospasm as an asthma exacerbation and withholding adrenaline is a lethal error. [1] [12]
A foreign body gives a sudden onset, often with a choking episode and asymmetric or focal findings; a pneumothorax (which can also complicate severe asthma) causes sudden deterioration with reduced air entry on one side; and upper-airway obstruction produces stridor rather than expiratory wheeze. In infants, a first episode of wheeze is more often bronchiolitis, and cardiac failure or aspiration should be considered when the story is atypical. [1] [11]
Clinical & Bedside Assessment
Assessment is rapid, structured and repeated. Take a focused history while you begin treatment — the current illness and trigger, reliever use and response, preventer adherence, previous severe episodes or ICU admissions, and any allergy — and assess severity by observation, auscultation and oxygen saturation, then reassess after every intervention. [1] [11]
Objective measures support but never override the clinical picture. Pulse oximetry guides oxygen therapy and severity, but hypoxaemia can be a late feature and a normal saturation on oxygen does not mean the child is safe. Peak expiratory flow can be useful in older, cooperative children as a trend, but a severely breathless child cannot perform it and should not be forced to try. [1] [12]
Reading the child, not just the number
Life-threatening
Silent chest, cyanosis, exhaustion, confusion
Deliberately avoid what wastes time or harms: do not delay bronchodilator and steroid to obtain a chest radiograph in a typical exacerbation, do not force spirometry on an exhausted child, and do not rely on a single reassuring saturation. A blood gas is reserved for the child who is failing to respond or tiring, where a rising PaCO₂ informs the decision to escalate. [1] [12]
Investigations
Acute asthma is a clinical diagnosis and most children need no investigations before treatment starts. The default in a typical exacerbation is oxygen saturation and clinical assessment alone, with treatment given immediately rather than waited upon. [1] [12]
A chest radiograph is not routine and can dangerously delay care; reserve it for suspected pneumothorax, focal or asymmetric signs, a possible foreign body, or a child failing to respond as expected. A blood gas (usually venous or capillary, with arterial reserved for the ventilated child) is indicated in severe or life-threatening disease to detect a rising PaCO₂ and acidosis — but a child who is tiring needs escalation regardless of the number. [1] [11]
When intravenous bronchodilators are used, remember their metabolic footprint: high-dose beta-agonists cause hypokalaemia and a lactic acidosis with tachycardia, so monitor potassium and interpret a raised lactate in that context; aminophylline needs level monitoring and cardiac observation. These are expected effects to anticipate, not reasons to withhold escalation in a failing child. [10] [1]
Management — Resuscitation
For the child in severe or life-threatening asthma, resuscitation and definitive treatment happen together: give oxygen, start bronchodilator and steroid immediately, and call for senior, anaesthetic and PICU support early rather than waiting to see if simple measures work. Sit the child up, keep them calm, and do not leave them unobserved. [1] [12]
Oxygen is titrated to keep SpO₂ at or above 94% using the least-distressing method the child tolerates. Inhaled salbutamol is given continuously (or as back-to-back nebulisers) in severe disease, nebulised ipratropium is added for severe and life-threatening exacerbations, and a systemic corticosteroid is given as early as possible because its benefit takes hours to appear. [9] [5]
Acute severe asthma drugs (confirm against local protocol)
If the child continues to deteriorate — persisting hypoxaemia, exhaustion, a silent chest or a rising PaCO₂ — move to intravenous bronchodilators (intravenous salbutamol as a bolus and/or infusion, or intravenous aminophylline) in a monitored HDU or PICU setting, and prepare for ventilatory support. Intubation is high-risk in severe asthma — induction and positive-pressure ventilation can worsen air trapping and cause hypotension or barotrauma — so it is performed by the most experienced operator available, with careful attention to slow ventilation and permissive hypercapnia. [10] [12]
Management — Definitive & Stepwise
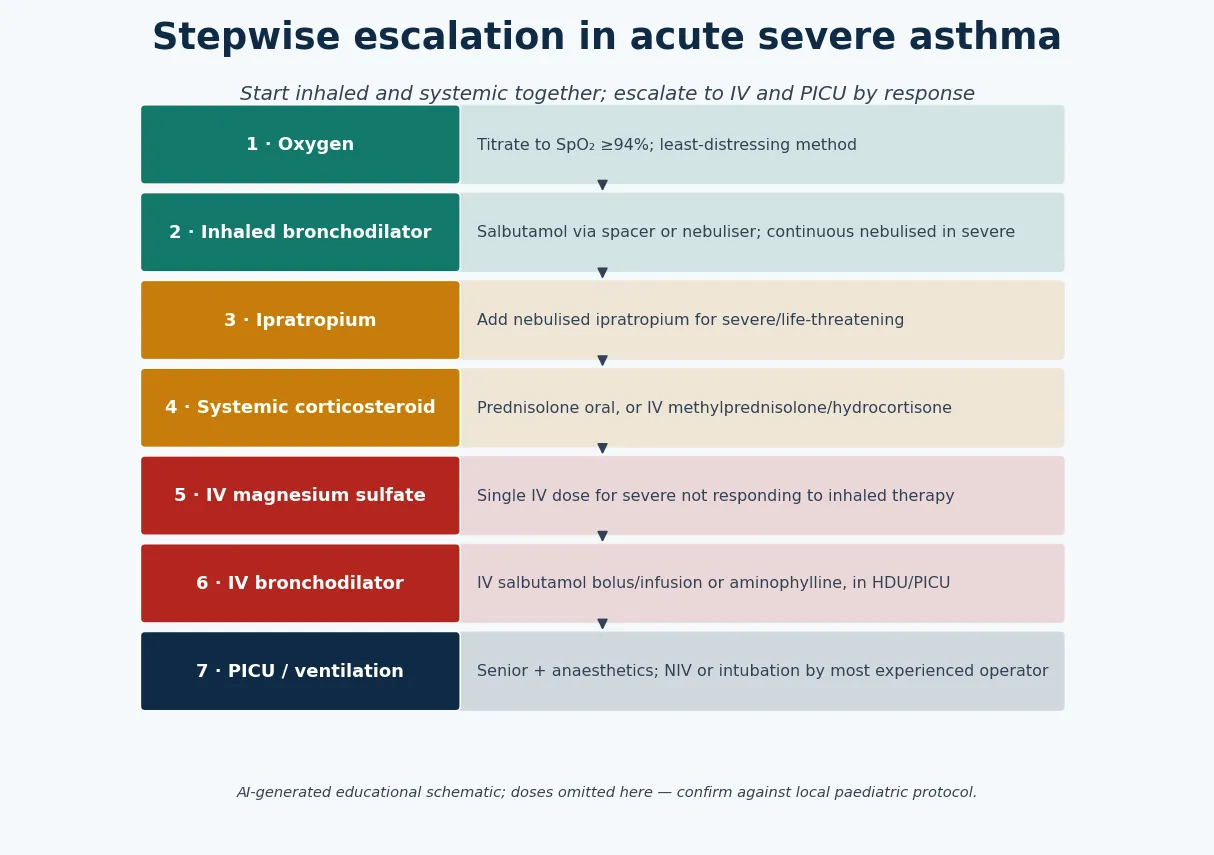
The definitive management is a disciplined escalation: oxygen and continuous inhaled bronchodilator with ipratropium and an early systemic steroid for everyone who is severe, then intravenous magnesium, then intravenous salbutamol or aminophylline and critical care for those who do not respond. Reassess after each step and step up quickly if the child is not improving. [12] [1]
Inhaled salbutamol is the backbone. Continuous nebulised salbutamol is more effective than intermittent dosing in severe exacerbations, and combining it with nebulised ipratropium in the first hours further reduces admissions in children with severe asthma; ipratropium is an early add-on, not a rescue. As the child improves, salbutamol is spaced out and the response guides disposition. [9] [5]
The stepwise pathway
Give oxygen titrated to SpO₂ ≥ 94% and start continuous or frequent inhaled salbutamol.
Add nebulised ipratropium for severe or life-threatening exacerbations in the first hour.
Give a systemic corticosteroid early — oral prednisolone, or IV steroid if not tolerated.
If severe and not responding: give a single IV dose of magnesium sulfate.
If still failing: IV salbutamol and/or aminophylline in HDU/PICU with monitoring.
Escalate to PICU, NIV or controlled intubation for exhaustion, silent chest or rising PaCO₂.
Systemic corticosteroids change the trajectory of the exacerbation and should be given early: prednisolone 1–2 mg/kg orally is standard, with intravenous methylprednisolone or hydrocortisone when the oral route is not tolerated, and a short oral course (typically three to five days) suffices without tapering for most children. Early emergency-department steroid reduces the need for admission, and the different oral regimens are broadly equivalent, so the priority is giving it promptly rather than choosing between them. [7] [8]
Intravenous magnesium sulfate is the usual first intravenous escalation for severe asthma not responding to inhaled therapy; a single dose is safe and reduces the need for further escalation, and the MAGNETIC trial showed that nebulised magnesium added to standard therapy gives a modest benefit in the most severe children. For the child who still fails, intravenous salbutamol and intravenous aminophylline are the next options, delivered in a critical-care setting with cardiac and electrolyte monitoring. [3] [2]
O-SHIMA
Specific Subtypes & Scenarios
The child who arrives in extremis — silent chest, cyanosis, barely responsive — needs simultaneous oxygen, continuous salbutamol and ipratropium, immediate intravenous access with magnesium and intravenous bronchodilator, and the airway team at the bedside. Do not wait for a stepwise trial; treat at the top of the pathway from the outset while preparing for ventilation. [12] [1]
Anaphylaxis presenting as bronchospasm must be actively excluded in any sudden-onset wheeze after an exposure. If there is any suspicion, give intramuscular adrenaline first, because it treats the whole reaction and the bronchospasm, and only then continue asthma therapy; withholding adrenaline while escalating asthma drugs is a fatal trap. [1] [12]
Powell 2013 — Lancet Respiratory Medicine (MAGNETIC; PMID 24429155)
Randomised, placebo-controlled trial of nebulised magnesium added to salbutamol and ipratropium in children with severe exacerbations
Key finding
Nebulised magnesium produced a modest improvement in an asthma severity score, with the benefit concentrated in the most severe children and those with a shorter duration of symptoms.
Practice change
Magnesium has a real but limited role as an add-on in severe disease; intravenous magnesium remains the usual first escalation, and neither replaces prompt inhaled therapy and steroid.
The child failing intravenous therapy who is exhausted or hypercapnic needs critical-care support: non-invasive ventilation can buy time in a cooperative child, but intubation and mechanical ventilation are hazardous in asthma and are undertaken by the most experienced operator, ventilating slowly with a long expiratory time and accepting permissive hypercapnia to avoid dynamic hyperinflation. [12] [1]
The remote or retrieval scenario is a common exam vignette: a severe asthmatic a long way from a PICU. The priorities are to start full therapy immediately including intravenous magnesium, to involve the retrieval service early, and to escalate treatment during transfer rather than deferring it — because the child can deteriorate faster than the distance can be covered. [11] [12]
Complications & Pitfalls
The complications of severe asthma and its treatment are real. Untreated obstruction leads to respiratory failure and, rarely, cardiac arrest; air trapping can cause a pneumothorax or pneumomediastinum, especially once the child is ventilated; and high-dose beta-agonists produce hypokalaemia, tachycardia and a lactic acidosis that can be mistaken for worsening illness. [1] [10]
The dominant pitfall is underestimating severity — being reassured by a talking child with a loud wheeze while missing rising effort, or by a saturation that is normal on oxygen. The corollary pitfall is misreading deterioration as improvement: the silent chest, the quietening wheeze, the tiring child and the normalising PaCO₂ are all danger signs, and each has killed children treated as though they were settling. [1] [11]
[12]Other avoidable errors include delaying steroid while focusing on bronchodilator, delaying escalation to intravenous therapy in a child who is not responding, obtaining a chest radiograph before treating, and failing to plan discharge and prevention — sending home a child who has recovered without addressing why they deteriorated, without a preventer plan, and without a written action plan and follow-up. [7] [11]
Prognosis & Disposition
The prognosis of acute asthma is generally excellent: the great majority of children respond to prompt inhaled therapy and a course of oral steroid and recover fully, and even most severe exacerbations settle without needing intubation. Deaths are rare and are largely preventable, clustering in children whose severity or deterioration was missed. [11] [1]
Disposition follows response, not a fixed rule. A child whose exacerbation settles, who can space bronchodilator to several hours apart, is saturating well on air and is feeding and comfortable can be discharged with a short steroid course, a clear plan and follow-up; a child who needed continuous salbutamol, intravenous therapy, or oxygen, or who is not improving, is admitted, and the severe or deteriorating child goes to HDU or PICU. [12] [1]
Discharge is itself part of the treatment. Before a child leaves, check inhaler and spacer technique, ensure a preventer plan and a written asthma action plan are in place, address the trigger and the adherence gap that led to the exacerbation, and arrange early review — because the period after an exacerbation is exactly when the next one is prevented. [7] [11]
Special Populations
Children with a previous near-fatal episode — an ICU admission or ventilation — carry a markedly higher risk of another life-threatening exacerbation, so treat them at the severe end from the outset, escalate early, and involve senior and critical-care teams sooner than the current appearance alone would suggest. [1] [11]
The younger, smaller child obstructs sooner and tires faster, and the diagnosis is less certain in the preschool wheezer where a viral-triggered wheeze overlaps with early asthma; treat the acute obstruction on its merits while keeping the differential (bronchiolitis, foreign body) open, and reassess frequently because deterioration can be rapid. [1] [12]
Indigenous, rural, remote and socioeconomically disadvantaged children face the same illness with a thinner safety net — greater distances to critical care, higher rates of poorly controlled asthma, and more barriers to preventer therapy and follow-up. The equity interventions are to start full treatment promptly, arrange retrieval early, and ensure a realistic, resourced prevention and follow-up plan on discharge. [11] [1]
The adolescent brings adherence and risk-taking into play: heavy reliever use with poor preventer adherence, smoking or vaping, and psychosocial stress all raise the risk of a severe or fatal exacerbation, so the acute episode is also an opportunity to re-engage the young person with their asthma care. [1] [11]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | First-line emphasis | Escalation emphasis |
|---|---|---|---|
| ANZ | Australian Asthma Handbook; RCH and state CPGs | Frequent/continuous salbutamol + ipratropium + early steroid | IV magnesium first, then IV salbutamol/aminophylline, PICU |
| UK | NICE / BTS / SIGN joint guideline | Salbutamol + ipratropium + early systemic steroid by severity | IV magnesium, then IV bronchodilators under senior/critical-care input |
| North America | GINA-aligned and NAEPP evidence | Inhaled beta-agonist + ipratropium + systemic steroid | IV magnesium; IV/SC beta-agonist and ICU for the refractory |
| Low-resource | WHO-aligned approaches | Ensure oxygen, bronchodilator and steroid are given | Access to escalation and retrieval is the limiting factor |
The evidence backbone you should be able to name starts with the Cochrane reviews of the acute pathway: continuous versus intermittent beta-agonists favours continuous dosing in severe disease, combined ipratropium and salbutamol reduces admissions in children with severe exacerbations, and early emergency-department corticosteroids reduce admission. The Cochrane review of intravenous magnesium in children supports its role as an escalation, and the MAGNETIC trial defines the modest add-on benefit of nebulised magnesium in the most severe. [9] [5] [7] [3] [2]
For refractory disease, the Cochrane reviews of intravenous beta2-agonists and the overview of escalation interventions in children map the evidence for intravenous salbutamol and aminophylline, both of which show benefit but carry metabolic and cardiac effects that demand monitoring. The PREDICT cohort describes how these therapies are actually used across emergency departments and highlights the variability that the guidelines aim to reduce. [10] [12] [11]
The live areas of nuance are the choice and sequence of intravenous agents (magnesium, salbutamol, aminophylline), the exact role of nebulised versus intravenous magnesium, and the threshold and technique for ventilation — an area where the evidence is thin and the emphasis is on avoiding intubation where possible and ventilating cautiously when it is unavoidable. [12] [2]
Exam Pearls
The single move that keeps children safe is the disciplined one: recognise severity early, treat immediately and in the right order, reassess after every step, and escalate before the child collapses rather than after. [1] [12]
And when you teach acute asthma, teach the danger signs as loudly as the drugs — the quiet chest, the tiring child and the rising carbon dioxide — because the deaths come not from a lack of medicines but from a failure to see the child who is slipping away. [11] [1]
References
- [1]Leung JS. Paediatrics: how to manage acute asthma exacerbations. Drugs Context, 2021.PMID 34113386
- [2]Powell C, Kolamunnage-Dona R, Lowe J, et al. Magnesium sulphate in acute severe asthma in children (MAGNETIC): a randomised, placebo-controlled trial. Lancet Respir Med, 2013.PMID 24429155
- [3]Griffiths B, Kew KM. Intravenous magnesium sulfate for treating children with acute asthma in the emergency department. Cochrane Database Syst Rev, 2016.PMID 27126744
- [4]Knightly R, Milan SJ, Hughes R, et al. Inhaled magnesium sulfate in the treatment of acute asthma. Cochrane Database Syst Rev, 2017.PMID 29182799
- [5]Griffiths B, Ducharme FM. Combined inhaled anticholinergics and short-acting beta2-agonists for initial treatment of acute asthma in children. Cochrane Database Syst Rev, 2013.PMID 23966133
- [6]Vézina K, Chauhan BF, Ducharme FM. Inhaled anticholinergics and short-acting beta2-agonists versus short-acting beta2-agonists alone for children with acute asthma in hospital. Cochrane Database Syst Rev, 2014.PMID 25080126
- [7]Edmonds ML, Milan SJ, Camargo CA Jr, et al. Early use of inhaled corticosteroids in the emergency department treatment of acute asthma. Cochrane Database Syst Rev, 2012.PMID 23235589
- [8]Normansell R, Kew KM, Mansour G. Different oral corticosteroid regimens for acute asthma. Cochrane Database Syst Rev, 2016.PMID 27176676
- [9]Camargo CA Jr, Spooner CH, Rowe BH. Continuous versus intermittent beta-agonists in the treatment of acute asthma. Cochrane Database Syst Rev, 2003.PMID 14583926
- [10]Travers A, Jones AP, Kelly K, et al. Intravenous beta2-agonists for acute asthma in the emergency department. Cochrane Database Syst Rev, 2001.PMID 11406055
- [11]Craig S, Powell CVE, Nixon GM, et al. Treatment patterns and frequency of key outcomes in acute severe asthma in children: a Paediatric Research in Emergency Departments International Collaborative (PREDICT) multicentre cohort study. BMJ Open Respir Res, 2022.PMID 35301198
- [12]Craig SS, Dalziel SR, Powell CV, et al. Interventions for escalation of therapy for acute exacerbations of asthma in children: an overview of Cochrane Reviews. Cochrane Database Syst Rev, 2020.PMID 32767571