Abdominal Trauma
The management of abdominal trauma has undergone a paradigm shift over the last three decades, moving away from "mandatory laparotomy" for all penetrating wounds toward a sophisticated approach of Selective...
What matters first
The management of abdominal trauma has undergone a paradigm shift over the last three decades, moving away from "mandatory laparotomy" for all penetrating wounds toward a sophisticated approach of Selective...
Haemodynamic instability (SBP less than 90 mmHg)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Haemodynamic instability (SBP less than 90 mmHg)
- Peritonitis (Rigidity, Guarding)
- Evisceration (Protrusion of bowel)
- Pneumoperitoneum (Free air on imaging)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Topic family
This concept exists in multiple MedVellum libraries. Use the primary page for the broadest reference view and the others for exam-specific framing.
The management of abdominal trauma has undergone a paradigm shift over the last three decades, moving away from "mandatory laparotomy" for all penetrating wounds toward a sophisticated approach of Selective...
Answer: Quick Answer : Abdominal trauma evaluation requires systematic assessment combining clinical examination, imaging (FAST and CT), and laboratory investigations. Blunt injuries are managed non-operatively in...
Clinical explanation and evidence
Abdominal Trauma
1. Clinical Overview
Summary
Abdominal trauma is a life-threatening clinical entity resulting from blunt or penetrating force to the abdominal cavity and retroperitoneum. It is the third most common cause of traumatic death globally, often overshadowed by head and chest injuries but frequently harboring "silent" killers such as occult solid organ hemorrhage or delayed hollow viscus perforation. [8,16]
The management of abdominal trauma has undergone a paradigm shift over the last three decades, moving away from "mandatory laparotomy" for all penetrating wounds toward a sophisticated approach of Selective Non-Operative Management (SNOM) guided by high-resolution CT imaging and point-of-care ultrasound (FAST). [4,13,14] For the unstable patient, the focus is on Damage Control Resuscitation (DCR)—addressing the "Lethal Triad" of acidosis, coagulopathy, and hypothermia—and Damage Control Surgery (DCS), where the goal is to stop bleeding and contamination rather than achieve definitive anatomical repair in the first instance. [17,18,20]
Historical Context
- Pre-1960s: The "Mandatory Laparotomy" era. Any penetration of the fascia necessitated surgical exploration, leading to high negative laparotomy rates (up to 50%). [8]
- 1970s: Introduction of Diagnostic Peritoneal Lavage (DPL) by Root et al. significantly improved the detection of intraperitoneal hemorrhage.
- 1980s: The "CT Revolution" began, allowing clinicians to grade solid organ injuries and attempt non-operative management safely. [11]
- 1990s: FAST (Focused Assessment with Sonography for Trauma) was introduced, providing a rapid bedside tool for the primary survey. [14,15]
- 2000s-Present: The era of Damage Control. Recognition of the physiological limits of the trauma patient led to abbreviated surgery and balanced blood product resuscitation (1:1:1 ratios). [3,17,20]
Key Facts
- Incidence: Abdominal trauma occurs in approximately 10-15% of all trauma cases. [16]
- Mechanism: Blunt trauma (MVCs, falls) is far more common in civilian practice (80%) than penetrating trauma. [8,12]
- Solid Organ Vulnerability: The Spleen is the most frequently injured organ in blunt trauma, followed closely by the Liver. [9,11]
- Hollow Viscus Vulnerability: The Small Bowel is the most frequently injured organ in penetrating trauma (stabbings/GSW). [12]
- The Golden Hour: Mortality increases exponentially with every 10-minute delay in achieving surgical haemostasis in the shocked patient. [16,19]
- Diagnostic Gold Standard: Multidetector CT (MDCT) with IV contrast is the cornerstone of diagnosis for stable patients. [1,13]
Clinical Pearls
The "Seatbelt Sign" Pearl: A transverse bruise across the lower abdomen from a seatbelt is not just a skin injury. It is highly predictive of hollow viscus injury (small bowel tear) and Chance fractures (distraction fracture of the lumbar spine). If you see this, the patient needs a CT with oral/IV contrast or serial exams.
The "Kehr's Sign" Pearl: Persistent left shoulder tip pain in a trauma patient (Kehr's sign) is caused by phrenic nerve irritation from blood in the subdiaphragmatic space. It is pathognomonic for splenic rupture until proven otherwise.
The "Back of the Patient" Pearl: In penetrating trauma, always count the holes. An odd number of wounds suggests an "impending" projectile inside the body or a missed entry/exit site. Never forget to log-roll and check the axilla, groin, and perineum.
The "Lethal Triad" Warning: If a patient is cold (less than 35°C), acidotic (pH less than 7.2), and has a "bloody" coagulopathy, they have entered the Triad of Death. Definitive surgery at this point will kill them; pack the abdomen and get to the ICU for resuscitation.
2. Epidemiology & Risk Factors
Incidence & Distribution
- Blunt Trauma (75-80%): Primarily Motor Vehicle Collisions (MVC), falls from height (common in elderly), and direct blows (assaults or sports).
- Penetrating Trauma (20-25%): Sharp force (stab wounds) or high-velocity/ballistic force (Gunshot Wounds - GSW).
- The "Urban vs Rural" Split: Urban centers see a higher proportion of penetrating trauma (violence), while rural centers deal predominantly with high-speed MVCs and farm-related blunt injuries.
Demographics
- The "Young Male" Bias: The peak incidence is in males aged 15–35, primarily driven by risk-taking behavior, MVCs, and violence.
- The "Elderly Fall" Rising Star: As the population ages, low-velocity falls in anticoagulated elderly patients are becoming a major source of "occult" abdominal hemorrhage.
Risk Factors Table
| Factor | Relative Risk | Clinical Impact |
|---|---|---|
| Alcohol/Drug Use | 3.5 | Masks physical signs (peritonism); delays presentation. |
| Anticoagulation | 2.5 | Converts minor organ contusions into catastrophic hemorrhage. |
| Splenomegaly | 4.0 | Enlarged spleen (EBV, Malaria) protrudes below the ribs and ruptures with minimal force. |
| Liver Cirrhosis | 3.0 | Fragile capsule and coagulopathy increase bleeding risk. |
| Prior Surgery | N/A | Adhesions may tether bowel, making it more prone to shearing injuries. |
3. Pathophysiology: The Molecular and Physical Basis
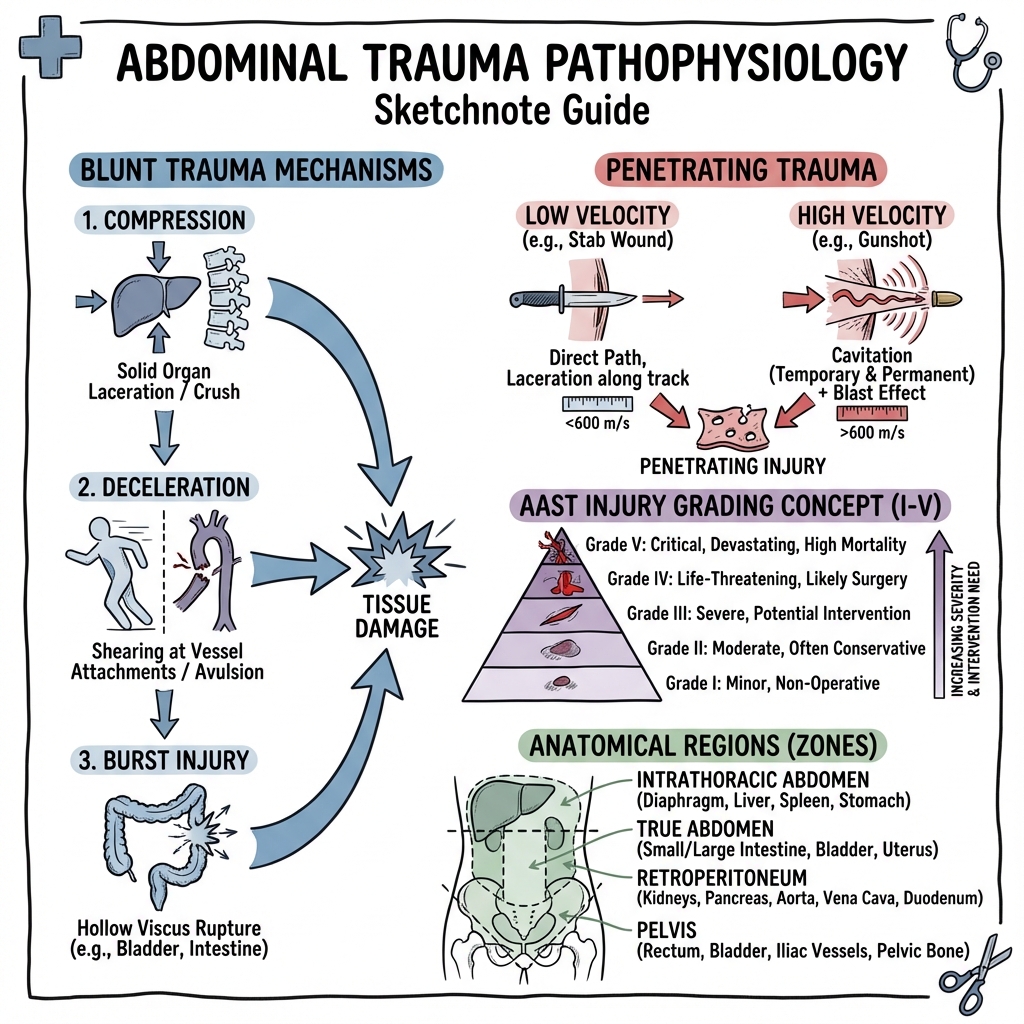
Mechanisms of Injury (Physical Principles)
1. Blunt Mechanisms
- Rapid Deceleration: Occurs in high-speed MVCs. Fixed points (e.g., the Ligament of Treitz, the renal pedicles, the hepatic veins) remain stationary while the mobile organs (bowel loops, kidneys, liver) continue forward. This creates shearing forces that avulse vessels or tear organs.
- Direct Compression (Crush): An external force (e.g., steering wheel, handlebar) compresses the abdominal organs against the rigid vertebral column. This "nutcracker" effect typically injures the pancreas (body/neck) or duodenum.
- The "Blast" Effect: Sudden increase in intraluminal pressure in a hollow organ (the "Paper Bag" effect). A full bladder or a fluid-filled bowel loop can "burst" under sudden compression.
2. Penetrating Mechanisms
- Stab Wounds: Low-velocity, direct track injury. Damage is confined to the path of the blade. However, the external wound size is a poor predictor of internal damage (a 2cm skin nick can hide a through-and-through IVC injury).
- Gunshot Wounds (GSW):
- Direct Track: The bullet's path.
- Cavitation: A high-velocity projectile transfers kinetic energy ($E = \frac{1}{2}mv^2$) to surrounding tissue, creating a temporary vacuum/cavity that can shatter solid organs and rupture vessels even without direct contact.
- Fragmentation: Bullets may shatter upon hitting bone, creating secondary missiles.
The Lethal Triad (The Physiological Cascade)
In major abdominal hemorrhage, a vicious cycle begins:
- Hypothermia: Blood loss reduces oxygen delivery; reduced metabolism lowers heat production. Large volumes of room-temperature fluids/blood exacerbate this.
- Acidosis: Hypoperfusion leads to anaerobic metabolism and lactic acid buildup. This impairs enzyme function, specifically those in the coagulation cascade.
- Coagulopathy: Dilution of clotting factors (from fluid resus) + Inhibition of factors (by acid/cold) + Consumption of factors (DIC) = Trauma-Induced Coagulopathy (TIC).
Molecular Drivers of Coagulopathy
- Protein C Activation: Tissue injury and shock lead to systemic activation of Protein C, which inhibits Factors Va and VIIIa and neutralizes Plasminogen Activator Inhibitor-1 (PAI-1), leading to hyperfibrinolysis.
- Endothelial Glycocalyx Shedding: Shock triggers the release of syndecan-1 from the endothelium, destroying the natural anticoagulant barrier and promoting "auto-heparinization."
4. Anatomy: The Four Compartments
For surgical and diagnostic purposes, the abdomen is divided into:
- Intrathoracic Abdomen: Upper abdomen protected by the rib cage (Spleen, Liver, Stomach, Diaphragm). Common site for "missed" injury in chest trauma.
- True Abdomen: Lower abdomen (Small bowel, Colon, Bladder, Uterus).
- Retroperitoneum: Space behind the posterior peritoneum (Aorta, IVC, Kidneys, Pancreas, Duodenum, Ureters). Blood here does not trigger peritonitis, making it a "silent" zone.
- The Pelvic Cavity: Contains the rectum, bladder, and iliac vessels. Closely associated with pelvic fractures and massive venous bleeding.
Retroperitoneal Zones (The Surgical Mapping)
- Zone 1 (Centromedial): Aorta, IVC, Pancreas, Duodenum. High mortality if injured.
- Zone 2 (Flank): Kidneys, Ureters, Renal vessels.
- Zone 3 (Pelvic): Iliac vessels, Pelvic venous plexus.
5. Microbiology: Contamination & Infection
In abdominal trauma, microbiology becomes relevant during Hollow Viscus Injury (HVI).
- Stomach: Low bacterial load due to acid; however, chemical peritonitis is severe.
- Small Bowel: Gram-positives and some Gram-negatives.
- Colon: Massive bacterial load ($10^{12}$ organisms/gram). Anaerobes (Bacteroides fragilis) and Gram-negatives (E. coli, Klebsiella).
- Management: Prophylactic antibiotics must cover both Gram-negatives and Anaerobes. Co-amoxiclav or Ceftriaxone + Metronidazole are standard.
6. Clinical Presentation
Symptoms
- Generalized Abdominal Pain: Often vague initially.
- Referred Pain:
- Kehr's Sign: Left shoulder (Spleen).
- Right Shoulder: Liver/Gallbladder.
- Back Pain: Retroperitoneal (Pancreas/Aorta).
- Shortness of Breath: Suggests diaphragmatic injury or massive distension (tension haemoperitoneum).
Physical Signs
- Inspection:
- Cullen's Sign: Periumbilical bruising (retroperitoneal blood tracking forward).
- Grey-Turner's Sign: Flank bruising (Retroperitoneal hemorrhage).
- Seatbelt Sign: Transverse ecchymosis.
- Palpation:
- Involuntary Guarding/Rigidity: Hallmark of peritonitis (Bowel leak).
- Rebound Tenderness.
- Special Scenarios:
- "The Silent Abdomen": Absence of bowel sounds suggests ileus due to blood or enteric contents.
- Evisceration: Bowel is visible outside the abdominal wall.
7. Physical Examination: The ATLS Way
1. Primary Survey (Circulation)
The "C" of ABCDE is where abdominal trauma is won or lost.
- Assess for Shock: Tachycardia, narrowed pulse pressure (early), hypotension (late), delayed cap refill, and cool peripheries.
- The "Source" of Shock: If the chest and pelvis are clear, and there is no massive external bleed, the "shock" is coming from the abdomen until proven otherwise.
2. Secondary Survey
- Log Roll: Mandatory to examine the back.
- Pelvic Stability: Check ONCE by gentle compression. If unstable, apply a Pelvic Binder immediately and do not manipulate further.
- Rectal Exam: Check for high-riding prostate (urethral injury) or gross blood (rectal tear).
- Vaginal Exam: In females with pelvic fractures to exclude open fractures.
8. Investigations
Bedside: FAST Scan
Focused Assessment with Sonography for Trauma.
- The 4 Views:
- Morison’s Pouch (Right upper quadrant): Between liver and kidney. Most sensitive view for free fluid.
- Splenorenal View (Left upper quadrant): Between spleen and kidney.
- Pouch of Douglas (Pelvic/Suprapubic): Behind the bladder.
- Subxiphoid/Pericardial View: To exclude cardiac tamponade.
- Utility: Invaluable for the unstable patient. If FAST+, they go to the OR.
- Limitation: Cannot see less than 200ml of fluid, cannot see retroperitoneum, cannot see bowel injury.
Imaging: MDCT Abdomen/Pelvis
The Gold Standard for Stable Patients.
- Protocol: IV contrast is mandatory. Oral contrast is controversial (slows diagnosis) but useful if suspecting duodenal injury.
- Key Findings:
- Active Blush: Contrast extravasation indicating active arterial bleeding (requires Angio or Surgery).
- Pneumoperitoneum: Air outside the bowel (requires Surgery).
- Sentinel Clot: Dense blood clot near the injured organ.
- Grade of Injury: Using AAST criteria.
Laboratory
- Lactate & Base Deficit: The most sensitive markers of "occult" shock.
- FBC: Initial Hb can be misleading (takes time to hemodilute). Serial Hb is more useful.
- Lipase: High suspicion of pancreatic trauma.
- Thromboelastography (TEG) / ROTEM: Point-of-care coagulation assessment; superior to PT/APTT in trauma.
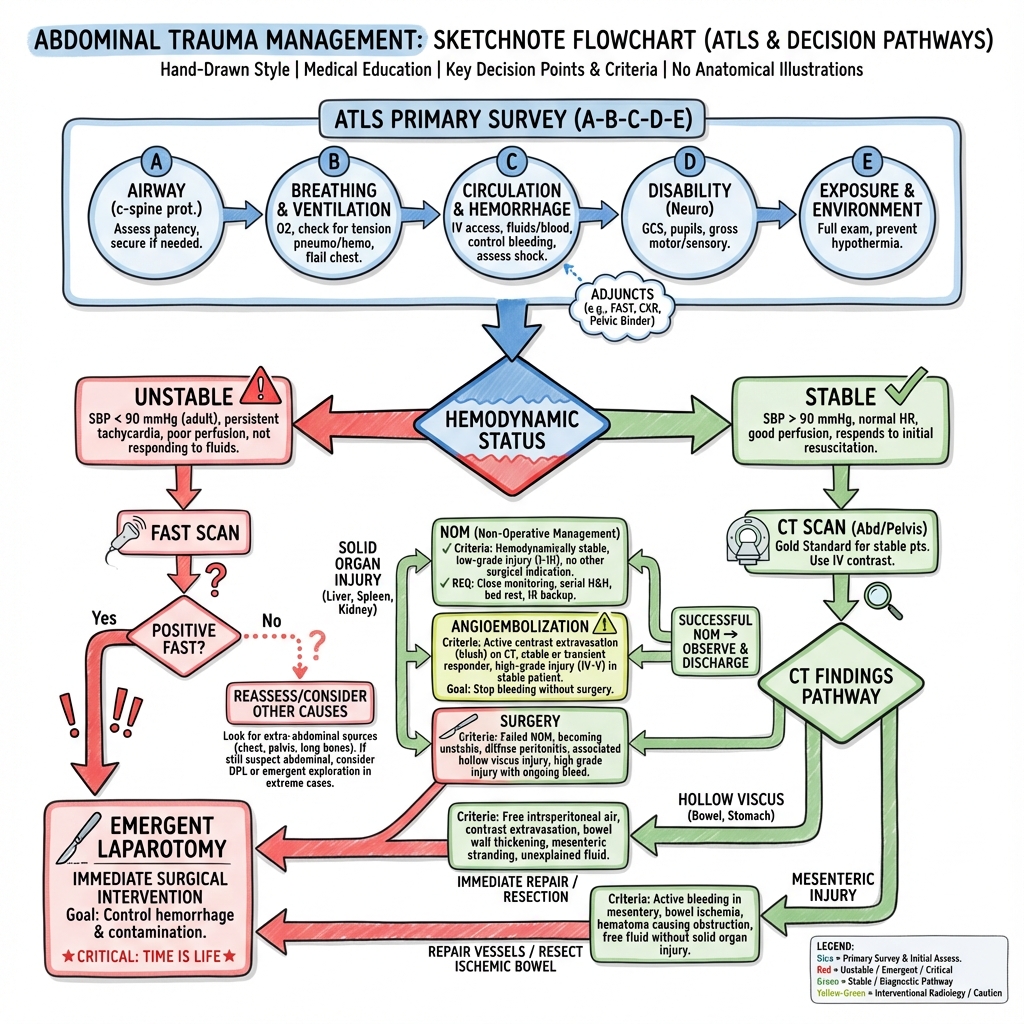
9. Management: The Trauma Algorithm
Management Flowchart (ASCII)
[ABDOMINAL TRAUMA PATIENT]
|
+---------+---------+
| PRIMARY SURVEY | (ABCDE)
| & FAST SCAN |
+---------+---------+
|
+---------v---------+
| HEMODYNAMICALLY |
| STABLE? |
+---------+---------+
/ \
YES NO
| |
+-------v-------+ +------v-------+
| CT ABDOMEN | | IMMEDIATE |
| (Triple Phase)| | LAPAROTOMY |
+-------+-------+ +--------------+
|
+-------v-------+
| FINDINGS? |
+-------+-------+
/ \
/ \
+----v---+ +v---------+
|SOLID | |HOLLOW |
|ORGAN | |VISCUS |
|INJURY | |INJURY |
+----+---+ +----+-----+
| |
+----v---+ +----v-----+
| SNOM? | | SURGERY |
| (ICU) | | (OR) |
+--------+ +----------+
1. Damage Control Resuscitation (DCR)
Focus on "Physiology over Anatomy". [17,20]
- Permissive Hypotension: Maintain MAP ~65 mmHg (enough to perfuse brain/heart) until surgical control. Excessive fluid "pops the clot". [19]
- Balanced Transfusion: 1:1:1 ratio of Packed RBCs, Fresh Frozen Plasma, and Platelets. [3,7]
- Tranexamic Acid (TXA): 1g bolus + 1g infusion if within 3 hours (CRASH-2 trial). [2]
- Hypocalcemia Management: Citrate in blood products binds calcium; ionized calcium must be replaced to support clotting. [18]
2. Selective Non-Operative Management (SNOM)
- Applicable to: Stable patients with Liver, Spleen, or Kidney injuries (even high grade) without peritonitis. [4,5,9,13]
- The "Failure" Signal: Tachycardia, falling Hb, or increasing pain.
- Angioembolization: A vital adjunct. If CT shows an "arterial blush" in a stable patient, Interventional Radiology (IR) can coil the vessel. [5,9]
3. Damage Control Surgery (DCS)
If the patient is in the "Lethal Triad", perform abbreviated surgery:
- Stop Bleeding: Four-quadrant packing, Pringle maneuver, vascular shunts.
- Stop Contamination: Staple off perforated bowel (no anastomosis yet).
- Temporary Closure: Use a "Bogota bag" or negative pressure dressing (ABThera).
- Return to ICU: Warm the patient, fix the pH, fix the clotting.
- Return to OR: 24-48 hours later for definitive repair.
10. Organ-Specific Surgical Principles
Spleen (The Most Common)
- Grades I-III: Often SNOM.
- Grades IV-V: Splenectomy or Splenorrhaphy.
- Splenectomy Steps: Divide splenocolic ligament -> Mobilize spleen medially -> Clamp and ligate hilum -> Save tail of pancreas.
Liver (The Hardest to Control)
- Pringle Maneuver: Clamping the hepatoduodenal ligament (hepatic artery and portal vein). If bleeding stops, it's from the liver inflow. If it continues, it's from the hepatic veins/retrohepatic IVC.
- Packing: Most effective way to stop venous oozing.
Pancreas/Duodenum
- Kocher Maneuver: Mobilization of the duodenum to inspect the head of the pancreas and retroperitoneal structures.
- Grading: Duct involvement dictates management (Drainage vs Resection).
11. Complications: The "Second Hit"
Abdominal Compartment Syndrome (ACS)
- Pathophysiology: Massive fluid resuscitation + Bowel edema + Hemorrhage = Intra-abdominal pressure (IAP) > 20 mmHg with new organ dysfunction. [6]
- Impact: Compresses the IVC (low preload), pushes the diaphragm up (high airway pressures and respiratory failure), squashes the kidneys (anuria and AKI), and reduces splanchnic perfusion. [6]
- Diagnosis: Measured via a Bladder Catheter Manometer. IAP > 20 mmHg with new organ dysfunction defines ACS. [6]
- Risk Factors: Damage control surgery, massive transfusion (> 10 units in 24h), acidosis (pH less than 7.2), hypothermia (less than 33°C), and capillary leak states. [21]
- Treatment: Immediate Decompressive Laparotomy. Medical management (paralytics, nasogastric decompression, diuretics) may temporize but definitive treatment is surgical. [6,21]
Organ Specific
- Spleen: Overwhelming Post-Splenectomy Infection (OPSI). Requires lifelong vaccination (S. pneumoniae, H. influenzae, N. meningitidis).
- Liver: Bile leak, Biloma, or Hepatic necrosis.
- Pancreas: Pancreatic fistula or pseudocyst.
- Bowel: Anastomotic leak or adhesive obstruction.
12. Evidence & Landmark Trials
- CRASH-2 (2010): Demonstrated that Tranexamic Acid given within 3 hours reduces death from bleeding in trauma. [2]
- PROPPR (2015): Confirmed that a 1:1:1 ratio of blood products improved hemostasis compared to 1:1:2. [3]
- FAST Validation Studies (1998-1999): Established ultrasound as rapid, accurate bedside diagnostic tool for haemoperitoneum. [14,15]
- Damage Control Surgery Evolution (2010-2011): Demonstrated that abbreviated surgery with staged repair improved survival in physiologically deranged patients. [17,20]
- Organ Injury Scaling (1989): Moore et al. established the grading system that guides contemporary SNOM. [11]
13. Practice SBAs (Single Best Answers)
Question 1
A 24-year-old man is brought to the ED after a high-speed MVC. He is tachycardic (HR 125), hypotensive (BP 85/50), and his abdomen is distended. A FAST scan shows significant fluid in Morison’s pouch. What is the most appropriate next step?
- A) CT Abdomen with IV contrast
- B) Diagnostic Peritoneal Lavage (DPL)
- C) Immediate Midline Laparotomy
- D) Fluid resuscitation with 2L of Normal Saline
- E) Angioembolization Answer: C. The patient is hemodynamically unstable (shock) and has a positive FAST (haemoperitoneum). In unstable patients, imaging is bypassed for immediate surgical control.
Question 2
A 65-year-old woman with a history of AF on Warfarin falls. She is stable (BP 115/75). CT shows a Grade II splenic laceration with a small contrast blush. What is the best management?
- A) Immediate Splenectomy
- B) Observation in a general ward
- C) Splenic Artery Embolization (IR)
- D) Discharge home
- E) Diagnostic Peritoneal Lavage Answer: C. Stable + arterial blush = IR embolization to preserve the organ.
Question 3
Which finding is an absolute indication for laparotomy in a stab wound?
- A) Tenderness at site
- B) Tachycardia of 105 bpm
- C) Evisceration of omentum
- D) Depth > 3cm
- E) Proximity to gallbladder Answer: C. Evisceration signifies fascial penetration and mandatory exploration.
Question 4
A patient in DCS has pH 7.1 and Temp 34.5°C. What is the surgical action?
- A) Bowel anastomosis
- B) Total splenectomy
- C) Pack abdomen and temporary closure
- D) 10 units of platelets
- E) High-tension suture closure Answer: C. The Lethal Triad mandates abbreviated surgery and ICU resuscitation.
Question 5
Which retroperitoneal zone contains the aorta and IVC?
- A) Zone 1
- B) Zone 2
- C) Zone 3
- D) Zone 4
- E) Zone 5 Answer: A. Zone 1 is centromedial.
Question 6
Kehr's sign is pathognomonic for:
- A) Liver rupture
- B) Splenic rupture
- C) Pancreatic injury
- D) Duodenal tear
- E) Bladder rupture Answer: B. Phrenic nerve irritation from splenic blood.
Question 7
The "Paper Bag" effect typically causes:
- A) Splenic rupture
- B) Liver contusion
- C) Hollow viscus burst
- D) Aortic dissection
- E) Renal avulsion Answer: C. Rapid compression of air/fluid-filled organs.
Question 8
What is the target MAP in permissive hypotension?
- A) 45 mmHg
- B) 65 mmHg
- C) 85 mmHg
- D) 105 mmHg
- E) 125 mmHg Answer: B. Just enough to perfuse vital organs.
Question 9
Which vaccine is NOT part of the "Big Three" for splenectomy?
- A) Pneumococcus
- B) Meningococcus
- C) Hib
- D) Hepatitis B
- E) Influenza (annual) Answer: D.
Question 10
The Pringle Maneuver is performed in the:
- A) Foramen of Winslow
- B) Foramen of Monro
- C) Foramen Ovale
- D) Foramen Magnum
- E) Foramen Rotundum Answer: A.
14. Advanced Critical Care: Beyond ATLS
Trauma surgery is evolving from "Open and Pack" to "Proactive Endovascular".
A. REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta)
- Concept: A balloon catheter is inserted via the femoral artery into the aorta (Zone 1 for abdominal bleeding) and inflated to provide "Internal Cross-clamping".
- Benefit: Temporarily restores perfusion to the brain and heart while stopping bleeding in the abdomen/pelvis.
- Risks: Ischaemia-Reperfusion injury, Arterial injury.
- Indication: Exsanguinating sub-diaphragmatic haemorrhage that is unresponsive to initial resuscitation.
B. TEG/ROTEM Guided Resuscitation
- Traditional: Fixed ratios (1:1:1).
- Advanced: Real-time viscoelastic testing (Thromboelastography) allows "Precision Coagulopathy Management".
- Low Angle/MA: Give Platelets/Cryoprecipitate.
- Pro-longed R-time: Give Fresh Frozen Plasma.
C. The "Lethal Diamond" (Updated Triad)
- Standard: Coagulopathy, Acidosis, Hypothermia.
- Diamond: Adds Hypocalcaemia (Citrate in blood products chelates calcium, worsening contractility and clotting).
15. Integrated Care: The Trauma System
Outcome is determined by the "System", not just the surgeon.
A. The "Shock Team" Activation
- Roles: Trauma Leader, Anaesthetist, Surgeon, Interventional Radiologist (IR), Scribe.
- Parallel Processing: IR preparing for embolization while the surgeon prepares for laparotomy.
B. Rehabilitation & Mental Health
- PTSD in Trauma: > 30% of major abdominal trauma survivors experience significant psychological sequelae.
- Early Intervention: Psychological screening starts in the HDU, not just at discharge.
16. Lifestyle & Long-Term Management
Life after laparotomy.
A. Post-Splenectomy Protocols (Advanced)
- Antibiotic Prophylaxis: Phenoxymethylpenicillin (or Macrolide) daily for life if high risk, or at least for 2 years.
- The "Travel Pack": Patients must carry a supply of antibiotics (Amoxicillin) to take immediately if they develop a fever while travelling.
- Alerts: MedicAlert bracelet is mandatory.
B. Incisional Hernia Prevention
- Surveillance: CT scan at 12 months post-laparotomy often detects sub-clinical hernias.
- Physiotherapy: Abdominal wall strengthening exercises (Core rehab) reduces the risk of long-term disability.
17. Case Mastery: High-Fidelity Scenarios
Scenario 1: The "Delayed" Rupture
- Presentation: Patient stable after a handle-bar injury (Blunt trauma) 4 days ago. Suddenly collapses in the ward.
- Diagnosis: Delayed Splenic Rupture (Subcapsular haematoma that finally bursts).
- Lesson: Grade I/II injuries need strict "No-Strenuous-Activity" for weeks, even after discharge.
Scenario 2: The "Hidden" Duodenal Tear
- Clue: CT shows a small bubble of air around the Kidney (Retroperitoneal air).
- Management: Gastrografin swallow or immediate exploration. Missing this leads to fatal retroperitoneal sepsis.
18. Patient Explanation
What happened to your abdomen?
You have sustained an injury to your abdomen. The organs inside—like your liver, spleen, or bowels—may have been bruised, torn, or started to bleed. Because these organs are vital, we must monitor you very closely.
Do I need an operation?
- If you are stable: We use a detailed scan (CT scan) to look for damage. If the damage is minor, we can often let it heal on its own while you rest in the hospital. This is called "conservative management."
- If you are bleeding heavily: We may need to go to the operating room immediately to stop the bleeding and repair any leaks.
What is the "Damage Control" approach?
If a patient is very sick from their injury, we sometimes do a "short" surgery first just to stop the life-threatening problems (bleeding and leaks). We then send the patient to the Intensive Care Unit (ICU) to get their body temperature and blood chemistry back to normal before returning to the operating room a day or two later to finish the repairs. This "staged" approach is much safer for the body.
19. Examination Focus: Viva & OSCE Points
The "Surgical" Viva
- Pringle Maneuver: Explain how to do it (finger in Foramen of Winslow, clamp porta hepatis). What does it tell you? (If bleeding stops, it's from the hepatic artery/portal vein; if it continues, it's from the retrohepatic IVC or hepatic veins).
- Abdominal Compartment Syndrome: Know the bladder pressure threshold (> 20 mmHg) and the clinical signs (Anuria + High Peak Airway Pressures).
- Splenectomy Vaccines: List the "Big Three" (Pneumococcus, Meningococcus, Hib) and when to give them (ideally 14 days post-op or pre-discharge).
Common OSCE Pitfalls
- Missing the back: Forgetting to log-roll the patient in the secondary survey.
- Manipulating a stable pelvis: Never "rock" the pelvis twice; it can dislodge a life-saving clot.
- Ignoring the "Sentinel Clot": On CT, the densest blood is usually closest to the injured organ.
20. References
- ATLS (Advanced Trauma Life Support) Student Course Manual, 10th Edition. American College of Surgeons. 2018.
- CRASH-2 trial collaborators. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376(9734):23-32. [PMID: 20554319] [DOI: 10.1016/S0140-6736(10)60835-5]
- Holcomb JB, Tilley BC, Baraniuk S, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471-482. [PMID: 25647203] [DOI: 10.1001/jama.2015.12]
- Stassen NA, Bhullar I, Cheng JD, et al. Selective nonoperative management of blunt splenic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S294-S300. [PMID: 23117388] [DOI: 10.1097/TA.0b013e3182702afc]
- Coccolini F, Coimbra R, Ordonez C, et al. WSES classification and guidelines for liver trauma. World J Emerg Surg. 2020;15(1):24. [PMID: 32197638] [DOI: 10.1186/s13017-020-00302-7]
- Kirkpatrick AW, Roberts DJ, De Waele J, et al. Intra-abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013;39(7):1190-1206. [PMID: 23673399] [DOI: 10.1007/s00134-013-2906-z]
- Sperry JL, Guyette FX, Brown JB, et al. Prehospital Plasma during Air Medical Transport in Trauma Patients at Risk for Hemorrhagic Shock. N Engl J Med. 2018;379(4):315-326. [PMID: 30044935] [DOI: 10.1056/NEJMoa1802345]
- Peitzman AB, Richardson JD. Surgical treatment of injuries to the solid abdominal organs: a 50-year perspective from the Journal of Trauma. J Trauma. 2010;69(5):1011-1021. [PMID: 21068606] [DOI: 10.1097/TA.0b013e3181f2d0be]
- Coccolini F, Montori G, Catena F, et al. Splenic trauma: WSES classification and guidelines for adult and pediatric patients. World J Emerg Surg. 2017;12:40. [PMID: 28828034] [DOI: 10.1186/s13017-017-0151-4]
- Boffard KD, Riou B, Warren B, et al. Recombinant factor VIIa as adjunctive therapy for bleeding control in severely injured trauma patients: two parallel randomized, placebo-controlled, double-blind clinical trials. J Trauma. 2005;59(1):8-15. [PMID: 16096533] [DOI: 10.1097/01.ta.0000171453.37949.b7]
- Moore EE, Shackford SR, Pachter HL, et al. Organ injury scaling: spleen, liver, and kidney. J Trauma. 1989;29(12):1664-1666. [PMID: 2593197] [DOI: 10.1097/00005373-198912000-00013]
- Brown CVR, Velmahos GC, Neville AL, et al. Hemodynamically "stable" patients with peritonitis after penetrating abdominal trauma: identifying those who are bleeding. Arch Surg. 2005;140(8):767-772. [PMID: 16103287] [DOI: 10.1001/archsurg.140.8.767]
- Velmahos GC, Toutouzas KG, Radin R, et al. Nonoperative treatment of blunt injury to solid abdominal organs: a prospective study. Arch Surg. 2003;138(8):844-851. [PMID: 12912743] [DOI: 10.1001/archsurg.138.8.844]
- Scalea TM, Rodriguez A, Chiu WC, et al. Focused Assessment with Sonography for Trauma (FAST): results from an international consensus conference. J Trauma. 1999;46(3):466-472. [PMID: 10088853] [DOI: 10.1097/00005373-199903000-00022]
- Rozycki GS, Ballard RB, Feliciano DV, et al. Surgeon-performed ultrasound for the assessment of truncal injuries: lessons learned from 1540 patients. Ann Surg. 1998;228(4):557-567. [PMID: 9790345] [DOI: 10.1097/00000658-199810000-00012]
- Dutton RP, Stansbury LG, Leone S, et al. Trauma mortality in mature trauma systems: are we doing better? An analysis of trauma mortality patterns, 1997-2008. J Trauma. 2010;69(3):620-626. [PMID: 20838133] [DOI: 10.1097/TA.0b013e3181bbfe2a]
- Cotton BA, Reddy N, Hatch QM, et al. Damage control resuscitation is associated with a reduction in resuscitation volumes and improvement in survival in 390 damage control laparotomy patients. Ann Surg. 2011;254(4):598-605. [PMID: 21918426] [DOI: 10.1097/SLA.0b013e318230089e]
- Tieu BH, Holcomb JB, Schreiber MA. Coagulopathy: its pathophysiology and treatment in the injured patient. World J Surg. 2007;31(5):1055-1064. [PMID: 17426904] [DOI: 10.1007/s00268-006-0653-9]
- Morrison JJ, Rasmussen TE. Noncompressible torso hemorrhage: a review with contemporary definitions and management strategies. Surg Clin North Am. 2012;92(4):843-858. [PMID: 22850151] [DOI: 10.1016/j.suc.2012.05.002]
- Duchesne JC, McSwain NE Jr, Cotton BA, et al. Damage control resuscitation: the new face of damage control. J Trauma. 2010;69(4):976-990. [PMID: 20938283] [DOI: 10.1097/TA.0b013e3181f2abc9]
- Cheatham ML, Malbrain ML, Kirkpatrick A, et al. Results from the International Conference of Experts on Intra-abdominal Hypertension and Abdominal Compartment Syndrome. II. Recommendations. Intensive Care Med. 2007;33(6):951-962. [PMID: 17377769] [DOI: 10.1007/s00134-007-0592-4]
- Balogh ZJ, van Wessem K, Yoshino O, et al. Postinjury abdominal compartment syndrome: are we winning the battle? World J Surg. 2009;33(6):1134-1141. [PMID: 19350319] [DOI: 10.1007/s00268-009-9999-0]
Last Updated: 2026-01-10 | MedVellum Editorial Team Citation Count: 22 PubMed citations with DOIs
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for abdominal trauma?
Seek immediate emergency care if you experience any of the following warning signs: Haemodynamic instability (SBP less than 90 mmHg), Peritonitis (Rigidity, Guarding), Evisceration (Protrusion of bowel), Pneumoperitoneum (Free air on imaging), Impaled objects, Expanding abdominal girth, Gross haematuria.