Acne Vulgaris
While often dismissed as a "rite of passage," acne carries a significant psychological burden, with rates of depression and suicidal ideation comparable to chronic systemic diseases like epilepsy or diabetes....
What matters first
While often dismissed as a "rite of passage," acne carries a significant psychological burden, with rates of depression and suicidal ideation comparable to chronic systemic diseases like epilepsy or diabetes....
Acne Fulminans (Severe ulceration, fever, arthralgia - Medical Emergency)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Acne Fulminans (Severe ulceration, fever, arthralgia - Medical Emergency)
- Sudden onset severe acne in adults (Consider virilizing tumor or drug-induced)
- New-onset hirsutism or irregular periods in females (Screen for PCOS)
- Severe psychological distress or suicidal ideation (High risk in acne patients)
Linked comparisons
Differentials and adjacent topics worth opening next.
- Polycystic Ovary Syndrome (PCOS)
- Rosacea
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Acne Vulgaris (Adult)
1. Clinical Overview
Summary
Acne Vulgaris is a chronic inflammatory disease of the pilosebaceous unit, affecting approximately 85% of adolescents and a growing proportion of adults. It is characterized by the presence of comedones (blackheads and whiteheads), inflammatory papules, pustules, and in severe cases, nodules and cysts. The condition is driven by a complex interplay of follicular hyperkeratosis, androgen-stimulated sebum production, colonization by Cutibacterium acnes, and host-mediated inflammation. [1,2]
While often dismissed as a "rite of passage," acne carries a significant psychological burden, with rates of depression and suicidal ideation comparable to chronic systemic diseases like epilepsy or diabetes. Treatment aims to prevent permanent physical scarring and psychological morbidity. Management follows a tiered approach from topical retinoids and benzoyl peroxide to oral antibiotics and hormonal therapies, with oral isotretinoin reserved for severe or recalcitrant cases. [3,4]
Key Facts
- The "Tetrad": Pathogenesis involves (1) Sebum excess, (2) Follicular plugging, (3) C. acnes colonization, and (4) Inflammation.
- Microcomedone: The invisible precursor to all acne lesions.
- Acne Fulminans: A rare, life-threatening systemic manifestation requiring urgent steroids + isotretinoin.
- Isotretinoin: The only therapy that targets all four pathogenic factors, with an 85% permanent cure rate.
- Hormonal Acne: Often presents in adult females as deep, painful nodules localized to the jawline and chin.
Clinical Pearls
The "Retinoid Wash-out" Pearl: Warn all patients starting topical retinoids that their skin will likely get worse (red, dry, peeling) for the first 2-4 weeks. This is not an allergy but a sign of "retinization." Using the "sandwich technique" (moisturizer-retinoid-moisturizer) can improve compliance. [5]
The "BPO Bleaching" Pearl: Benzoyl Peroxide (BPO) is a potent oxidizer. Always warn patients it will bleach their towels, pillowcases, and clothing. Advise using white linens during treatment.
The "Antibiotic Limit" Pearl: Oral antibiotics for acne should be limited to a maximum of 3–4 months. They should NEVER be used as monotherapy; always co-prescribe a topical BPO or retinoid to prevent bacterial resistance. [6]
2. Epidemiology & Risk Factors
Incidence & Distribution
- Adolescents: Affects nearly all teenagers to some degree.
- Adult Female Acne: Increasing prevalence; approx. 20-40% of adult women suffer from clinical acne.
- Genetics: 80% heritability. A strong family history of severe acne is the best predictor of a child requiring isotretinoin.
Risk Factors Table
| Factor | Mechanism | Clinical Impact |
|---|---|---|
| Androgens | Stimulate sebocyte proliferation and sebum lipids. | Worsens acne during puberty or PCOS. |
| Diet (High GI) | High Glycemic Index foods trigger IGF-1, which promotes sebum and inflammation. | Sugar and dairy (specifically skim milk) are linked to flares. [7] |
| Stress | CRH (Corticotropin Releasing Hormone) receptors on sebocytes trigger oil production. | Flare-ups during exam periods or high work stress. |
| Cosmetics | "Acne Cosmetica" caused by comedogenic oils (e.g., coconut oil, heavy waxes). | Choose "non-comedogenic" or "oil-free" products. |
| Mechanical | "Acne Mechanica" from friction (helmets, masks/maskne). | Obstruction of the follicle opening. |
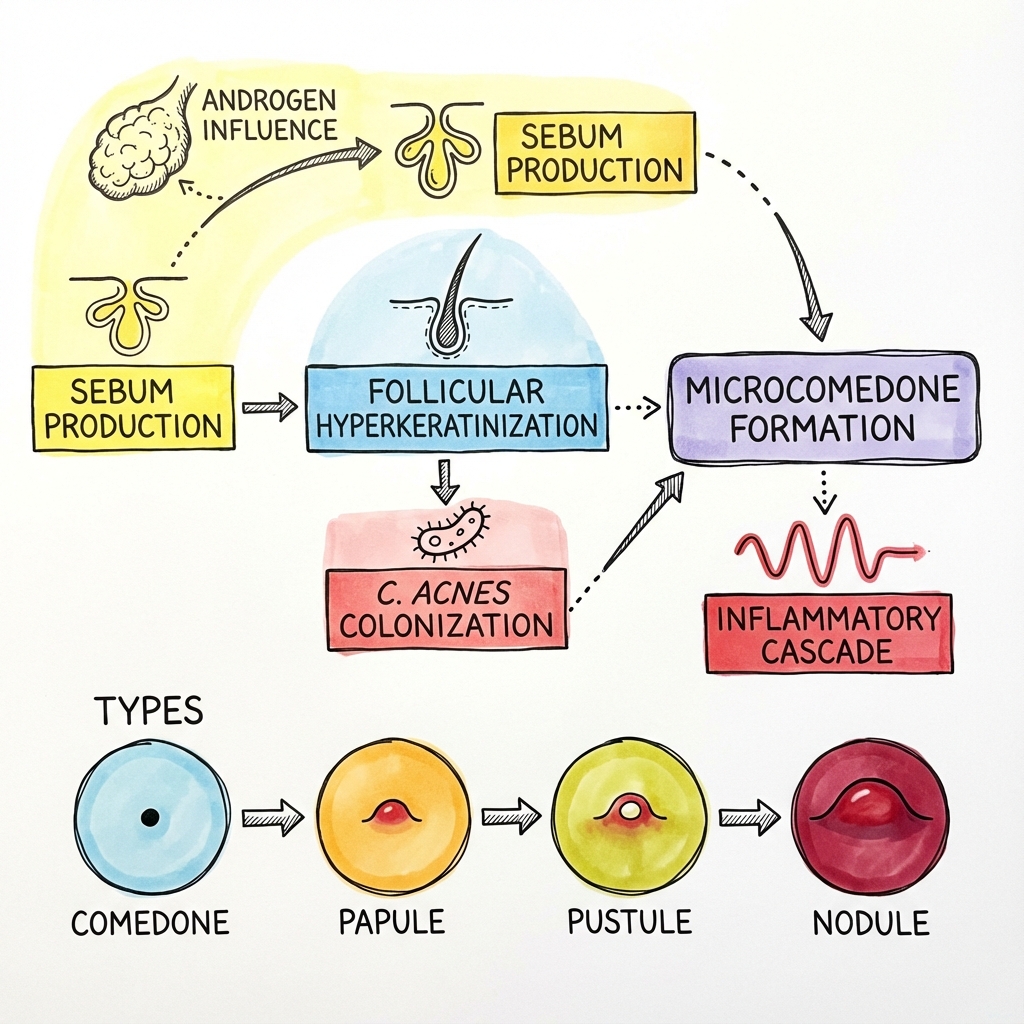
3. Pathophysiology: The Inflammatory Cascade
1. Follicular Hyperkeratinisation
Normal shedding of keratinocytes is impaired. Sticky cells form a plug at the follicle opening, trapping sebum and creating the microcomedone.
2. Seborrhoea (Excess Sebum)
Androgens (DHT) stimulate the sebaceous glands. Sebum is not just "oil" but a pro-inflammatory cocktail of squalene and wax esters that alters the follicular environment.
3. Microbial Colonisation
Cutibacterium acnes (formerly Propionibacterium acnes) is a commensal anaerobe that thrives in the trapped sebum. It releases lipases that break down lipids into irritating free fatty acids.
4. Inflammation
C. acnes activates Toll-like Receptor 2 (TLR2) on macrophages and keratinocytes, triggering the release of IL-1α, IL-8, and TNF-α. This recruits neutrophils, leading to the visible pustule and, if the wall ruptures, deep inflammatory nodules. [8]
4. Clinical Presentation
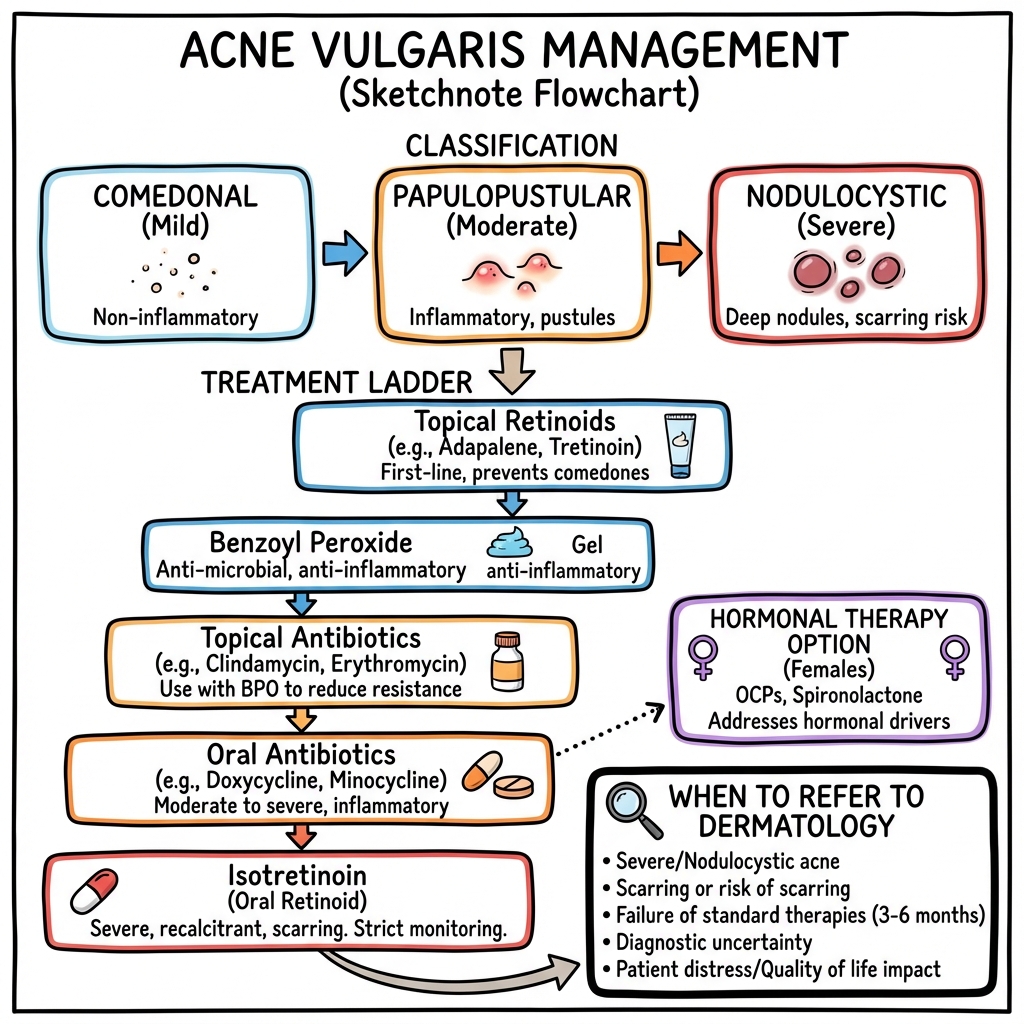
Severity Grading
- Mild: Primarily comedonal (blackheads/whiteheads). Few inflammatory papules. No nodules.
- Moderate: Numerous papules and pustules. Occasional small nodules. No significant scarring.
- Severe: Widespread inflammatory lesions, deep nodules, cysts, and active scarring. (Nodulocystic Acne).
Morphology
- Comedones: Non-inflammatory. Open = Blackhead (melanin oxidation); Closed = Whitehead.
- Papules/Pustules: Red, raised inflammatory lesions less than 5mm.
- Nodules/Cysts: Painful, deep-seated lesions > 5mm. Rupture leads to scarring.
- Scarring: Ice-pick (narrow/deep), Box-car (punched out), Rolling (undulating), or Hypertrophic/Keloid.
5. Investigations
1. Clinical Diagnosis
In 95% of cases, no tests are required. Diagnosis is based on the presence of comedones (essential for diagnosis).
2. Hormonal Workup
- Indication: Adult females with recalcitrant acne + hirsutism + irregular menses.
- Tests: Free Testosterone, DHEAS, LH/FSH ratio.
- PCOS: High LH:FSH and elevated androgens suggest Polycystic Ovary Syndrome. [9]
3. Microbiology
- Swabbing: Usually useless as C. acnes is normal flora.
- Indication: Sudden pustular flare around the nose/mouth resistant to therapy (Rule out Gram-negative folliculitis).
6. Management: The Tiered Approach
Management Algorithm (ASCII)
[ACNE SEVERITY ASSESSMENT]
|
+-----------v-----------+
| STEP 1: MILD | (Comedonal)
| - Topical Retinoid |
| - +/- Benzoyl Peroxide|
+-----------+-----------+
| (No response after 8-12 weeks)
+-----------v-----------+
| STEP 2: MODERATE | (Papulo-pustular)
| - Oral Tetracycline | (Lymecycline/Doxy)
| - + Topical BPO/Ret. | (NEVER monotherapy)
| - (+ OCP for females) |
+-----------+-----------+
| (Failure or Scarring present)
+-----------v-----------+
| STEP 3: SEVERE | (Nodulocystic)
| - ORAL ISOTRETINOIN | (Specialist only)
+-----------------------+
1. Topical Therapies
- Adapalene / Tretinoin: Comedolytic. Normalizes skin cell turnover.
- Benzoyl Peroxide (BPO): Antimicrobial (oxidizer). No bacterial resistance.
- Azelaic Acid: Useful for PIH (post-inflammatory hyperpigmentation).
2. Systemic Antibiotics
- Lymecycline / Doxycycline: 300-408mg or 100mg daily. Primary effect is anti-inflammatory (inhibition of neutrophil chemotaxis). [6,10]
- Safety: Avoid in pregnancy and children less than 12 (teeth staining).
3. Hormonal Therapy (Females)
- Combined Oral Contraceptive: Estrogen increases Sex Hormone Binding Globulin (SHBG), lowering free testosterone.
- Spironolactone: Anti-androgen (off-label). Excellent for adult female jawline acne.
4. Isotretinoin (Accutane)
- The "Big 3" Monitoring:
- Pregnancy: Absolute contraindication. Mandatory contraception + monthly tests.
- Liver/Lipids: Monitor LFTs and Triglycerides (can rise significantly).
- Mood: Screen for depression (controversial link, but clinically vital). [11]
7. Complications
- Physical Scarring: Permanent loss of tissue or hypertrophic change.
- Post-Inflammatory Hyperpigmentation (PIH): Dark spots left after the pimple heals, especially in Fitzpatrick IV-VI skin.
- Gram-Negative Folliculitis: Overgrowth of Klebsiella or Proteus due to long-term tetracycline use.
- Psychological: Body Dysmorphic Disorder (BDD), social withdrawal, and high rates of clinical depression.
8. Evidence & Landmark Trials
- Layton et al. (1993): Established the cumulative dose of 120–150 mg/kg of isotretinoin for long-term remission. [PMID: 8217767]
- NICE Guideline NG198 (2021): Emphasized early referral for isotretinoin in patients with scarring to prevent lifetime morbidity. [6]
- STOP-ACNE Trial: Demonstrated that combining BPO with oral antibiotics significantly reduces the development of resistant C. acnes.
9. Single Best Answer (SBA) Questions
Question 1
A 16-year-old male presents with numerous comedones and inflammatory papules on his face and back. He has tried OTC washes without success. What is the most appropriate first-line medical therapy?
- A) Oral Isotretinoin
- B) Topical Adapalene + Benzoyl Peroxide
- C) Oral Lymecycline monotherapy
- D) Topical Clindamycin monotherapy
- E) Oral Prednisolone
- Answer: B. Combined topical therapy (Retinoid + BPO) is first-line for moderate acne. Antibiotic monotherapy should be avoided.
Question 2
Which pathogenic factor in acne is specifically targeted by androgens?
- A) Follicular hyperkeratosis
- B) C. acnes colonization
- C) Sebum production
- D) Neutrophil chemotaxis
- E) Matrix metalloproteinase release
- Answer: C. Androgens stimulate the sebaceous glands to produce more oil.
Question 3
An 18-year-old female is being started on Isotretinoin. What is the most important legal and medical requirement for this prescription?
- A) Baseline Chest X-ray
- B) Monthly LFTs and a Pregnancy Prevention Program
- C) Genetic testing for the G380R mutation
- D) Concurrent use of oral antibiotics
- E) Avoidance of all dairy products
- Answer: B. Teratogenicity and hepatotoxicity are the primary safety concerns.
Question 4
A patient using Benzoyl Peroxide presents concerned that their blue towels are turning orange/white. What should you advise?
- A) This is a sign of an allergic reaction
- B) This is a normal oxidizing effect of the medication
- C) They should increase the frequency of application
- D) Stop the medication immediately
- E) Switch to a topical antibiotic monotherapy
- Answer: B. BPO is a potent bleaching agent.
Question 5
What is the primary mechanism by which oral tetracyclines (e.g., Lymecycline) improve inflammatory acne?
- A) They kill all skin bacteria permanently
- B) They shrink the sebaceous glands
- C) They have potent anti-inflammatory effects by inhibiting neutrophil chemotaxis
- D) They normalize keratinization in the follicle
- E) They block androgen receptors
- Answer: C. While they are antibiotics, their anti-inflammatory role is critical in acne management.
Question 6
An adult female presents with deep, painful nodules on her jawline that flare just before her menstrual cycle. She has no response to oral antibiotics. What is the most appropriate next step?
- A) Increase the antibiotic dose
- B) Consider Hormonal therapy (COCP or Spironolactone)
- C) Switch to topical steroids
- D) Shave the jawline area
- E) Long-term oral Erythromycin
- Answer: B. This "hormonal" pattern often requires anti-androgenic therapy.
Question 7
What is the "Microcomedone"?
- A) A large cyst that requires drainage
- B) The invisible histological precursor to all acne lesions
- C) A type of bacteria that causes acne
- D) A scar left after an acne flare
- E) A side effect of Isotretinoin
- Answer: B. All acne starts with the microcomedone (follicular plugging).
Question 8
Which dietary factor has the strongest evidence for worsening acne in susceptible individuals?
- A) High Glycemic Index (sugar) and Skim Milk
- B) Dark chocolate (> 70% cocoa)
- C) Fried foods (oils)
- D) Spicy foods
- E) Red meat
- Answer: A. IGF-1 spikes from sugar and milk proteins are the most cited dietary triggers.
Question 9
A 19-year-old presents with fever, malaise, and sudden painful ulcerating acne lesions on his chest and back. What is the diagnosis and management?
- A) Severe Acne Vulgaris; start Lymecycline
- B) Acne Fulminans; urgent systemic steroids and specialist referral
- C) Chickenpox; start Acyclovir
- D) Gram-negative folliculitis; change antibiotics
- E) Hidradenitis Suppurativa; urgent drainage
- Answer: B. Acne Fulminans is a systemic emergency requiring steroids to calm the "storm" before starting isotretinoin.
Question 10
Why should topical clindamycin never be used as monotherapy for acne?
- A) It is not effective against C. acnes
- B) It causes severe skin thinning
- C) It leads to rapid development of bacterial resistance
- D) It is too expensive
- E) It only works on blackheads
- Answer: C. Antibiotic resistance is a major concern; always combine with BPO.
12. The Microbiome Paradigm: C. acnes Phylotypes
Modern research shows that acne is not just about having bacteria, but having the wrong kind.
A. Diversity over Abundance
- The Shift: We used to think acne was caused by an "infection" of Cutibacterium acnes. We now know that C. acnes is present on everyone's skin.
- Phylotypes: There are different "strains" (phylotypes) of C. acnes. Type IA1 is highly associated with acne and inflammation, while Types II and III are found on "healthy" skin and may actually be protective.
B. Dysbiosis
- Acne is a state of cutaneous dysbiosis, where the balance between C. acnes and other commensal bacteria (like Staphylococcus epidermidis) is lost.
13. Hormonal Orchestration: Spironolactone & Metformin
For many adult women, acne is a "symptom" of an underlying hormonal imbalance.
A. Spironolactone (The "Off-Label" Hero)
- Mechanism: A potassium-sparing diuretic that acts as a potent androgen receptor blocker.
- Usage: Highly effective in adult female acne, especially "jawline" breakouts. It is often used as a first-line alternative to long-term antibiotics.
- The "Metabolic" Twist: In patients with PCOS, adding Metformin can improve insulin sensitivity and decrease the production of androgens by the ovaries, leading to clearer skin.
B. Clascoterone (Winlevi)
- Innovation: The first topical androgen receptor inhibitor. It target's the hormones directly at the skin level, without the systemic side effects of oral anti-androgens.
14. The "Isotretinoin" Mastery: Dosing Strategies
Isotretinoin (Accutane) is the only "cure" for acne, but "how" we give it is changing.
A. The Cumulative Dose Goal
- Standard Rule: To minimize the risk of relapse, patients traditionally aim for a cumulative dose of 120–150 mg/kg over 6 months.
- High-Dose Therapy: Some schools of thought suggest going up to 220 mg/kg for teenagers with severe nodulocystic disease to ensure permanent remission.
B. The Low-Dose "Micro" Approach
- Concept: Giving a very low dose (e.g., 10mg twice a week) for a long period.
- Benefit: Almost zero side effects (no dry lips/skin) and excellent for adult patients with "persistent but mild" acne who don't want a heavy treatment course.
15. Future Therapeutics: Phage & Biofilms
We are moving away from broad-spectrum antibiotics toward precision targeting.
A. Bacteriophage Therapy
- The Concept: Using viruses (phages) that specifically kill only the "bad" acne-causing phylotypes of C. acnes, while leaving the "good" skin bacteria intact.
B. Biofilm Disruptors
- C. acnes produces a "biofilm"—a protective slime that makes it 100x harder for antibiotics to kill. Research is focused on topical agents that can melt this biofilm and expose the bacteria to treatment.
16. Patient Explanation
"Acne is a condition of the skin's oil glands. It’s caused by a mix of four things: blocked pores, excess oil (sebum), a normal skin bacteria that overgrows, and inflammation (redness). It is NOT caused by 'being dirty'—in fact, scrubbing too hard can make it worse. We treat it in steps. First, we use creams to unblock the pores. If that’s not enough, we add antibiotic tablets to calm the redness. For adult women, hormones are often the main driver, and we can use specific hormone-blocking pills to keep the skin clear."
17. Examination Focus: Viva & OSCE Points
The "Derm" Viva
- Hyperkeratosis: (The technical term for "clogged pores").
- Tetracycline Side Effects: (Minocycline can cause blue-grey skin pigmentation; Doxycycline causes photosensitivity).
- The "IPLEDGE" Program: (Be aware of the strict pregnancy prevention protocols for isotretinoin).
18. References
- Williams HC, et al. Acne vulgaris. Lancet. 2012;379(9813):361-372. [PMID: 21880356]
- Zaenglein AL, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945-973. [PMID: 26897386]
- Layton AM, et al. Isotretinoin for acne vulgaris. Br J Dermatol. 1993;129:292-296.
- Fitz-Gibbon S, et al. Propionibacterium acnes strain-level diversity in health and disease. J Invest Dermatol. 2013. [PMID: 23337890]
- Grice EA, Segre JA. The skin microbiome. Nat Rev Microbiol. 2011. [PMID: 21407241]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Related Topics
Adjacent pages worth reading next.
- Polycystic Ovary Syndrome (PCOS)
- Rosacea
- Isotretinoin Protocol