Atrial Fibrillation
Atrial Fibrillation (AF) is a supraventricular tachyarrhythmia characterised by uncoordinated atrial electrical activati... MRCP exam preparation.
What matters first
Atrial Fibrillation (AF) is a supraventricular tachyarrhythmia characterised by uncoordinated atrial electrical activati... MRCP exam preparation.
Haemodynamic instability (Hypotension, Shock)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Haemodynamic instability (Hypotension, Shock)
- Acute heart failure (Pulmonary oedema)
- Pre-excitation (WPW) with rapid response
- Acute stroke or TIA
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Atrial Flutter
- MAT (Multifocal Atrial Tachycardia)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Atrial Fibrillation (Adult)
1. Overview
Atrial Fibrillation (AF) is a supraventricular tachyarrhythmia characterised by uncoordinated atrial electrical activation and consequently, ineffective atrial contraction. It is the most common sustained arrhythmia in clinical practice, affecting millions worldwide and carrying a 5-fold increased risk of ischaemic stroke. [1]
The 2024 AHA/ACC/HRS guidelines have redefined AF as a staged disease (Stages 1-4), moving beyond simple temporal patterns to a holistic view of "Atrial Myopathy." This shift emphasizes that structural and electrical changes often precede the first clinical episode of AF. [2]
Management is anchored in the ABC pathway: Anticoagulation (to avoid stroke), Better symptom management (rate/rhythm control), and Cardiovascular risk factor modification. The emergence of Early Rhythm Control (EAST-AFNET 4) and Pulsed Field Ablation (PFA) represents the new frontier in halting the progression of the "AF begets AF" cycle. [3]
2. Epidemiology
The AF Pandemic
- Prevalence: Global prevalence is ~2-4%, but this rises to > 10% in those over 80 years. It is estimated that 1 in 3 adults of European descent will develop AF in their lifetime. [4]
- The Burden: AF-related strokes are more severe, more disabling, and more likely to recur than strokes from other causes.
New 2024 Staging System
| Stage | Definition | Clinical Implication |
|---|---|---|
| Stage 1 | At Risk | Modifiable factors (HTN, Obesity, OSA) present but no AF. |
| Stage 2 | Pre-AF | Structural/electrical changes found (e.g. LA enlargement) but no clinical AF. |
| Stage 3 | AF | Clinical AF (Paroxysmal, Persistent, Long-standing persistent). |
| Stage 4 | Permanent | Permanent AF where rhythm control is no longer pursued. |
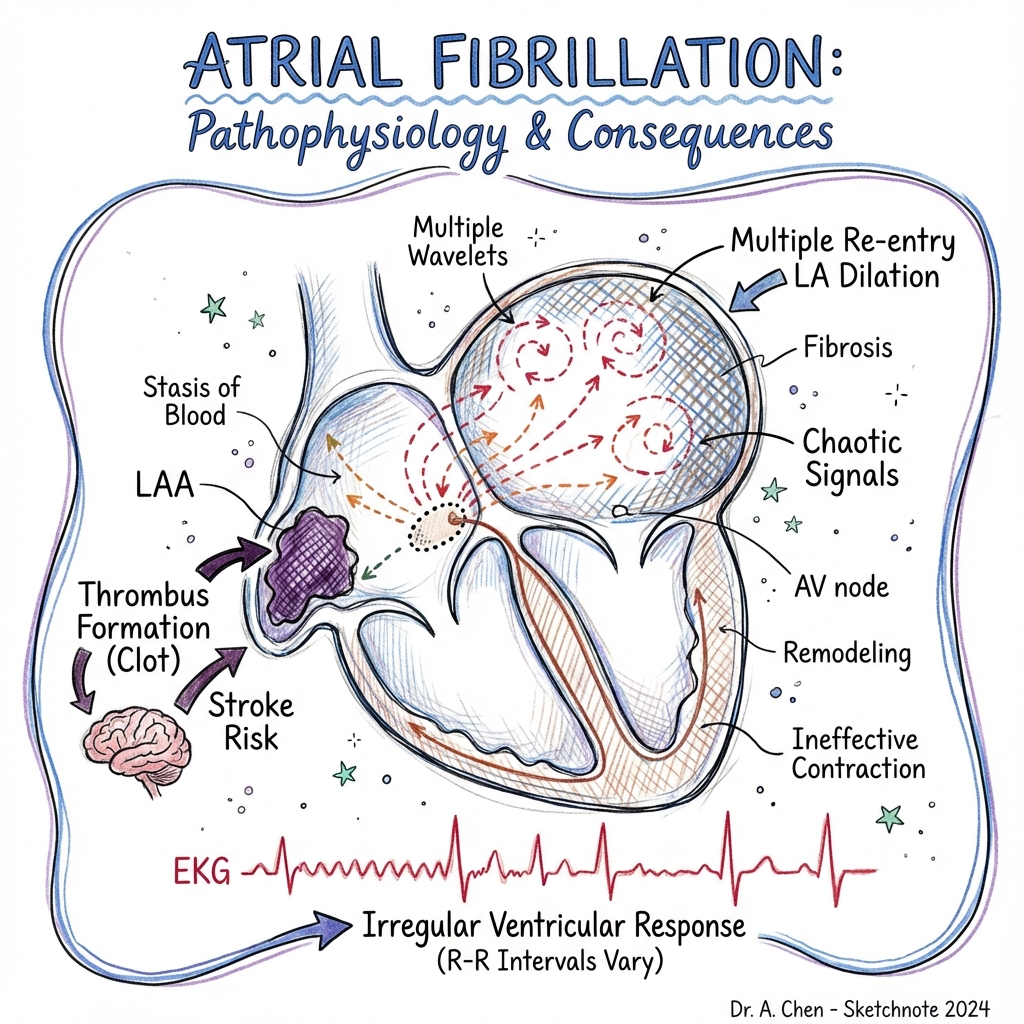
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- Pulmonary Vein Ectopy: Myocardial "sleeves" extending into the pulmonary veins possess unique ion channel properties, making them the primary source of high-frequency triggers.
- Ion Channel Shift (Electrical Remodelling): Within hours of rapid firing, L-type Calcium channels (I_Ca,L) are downregulated to protect myocytes from Ca2+ overload. This dramatically shortens the Atrial Effective Refractory Period (AERP).
- Wavelength Shortening: According to the equation Wavelength = Conduction Velocity x AERP, a shorter AERP allows multiple independent "re-entrant wavelets" to coexist within the atria simultaneously.
- CaMKII Activation: Chronic rapid atrial rates activate Calmodulin Kinase II, which hyperphosphorylates the Ryanodine Receptor (RyR2), causing "leaky" calcium release during diastole.
- The Delayed After-Depolarisation (DAD): Spontaneous Ca2+ leaks trigger the Na+/Ca2+ exchanger (NCX) to expel 1 Ca2+ for 3 Na+, creating an inward positive current that triggers new ectopic beats.
- Fibroblast Activation (Structural Remodelling): Atrial stretch and inflammation stimulate the RAAS system and TGF-β, causing fibroblasts to transform into myofibroblasts, which deposit excessive collagen.
- Lateral Dissociation: Fibrotic strands "insulate" healthy myocyte bundles from one another, causing tortuous conduction paths that stabilize high-frequency "rotors" or spiral waves. [5, 6, 7]
4. Clinical Presentation
Symptoms
- Palpitations: Irregularly irregular, "thumping" or "racing" sensation.
- Exercise Intolerance: Due to the loss of the atrial kick (20-30% of CO) and tachycardia-mediated reduction in diastolic filling time.
- Syncope: May indicate Sick Sinus Syndrome (Tachy-Brady) or rapid AF with outflow obstruction.
Physical Signs
- Irregularly Irregular Pulse: The hallmark sign.
- Pulse Deficit: Apical heart rate > radial pulse (not every beat creates a peripheral pulse).
- Absent 'a' Wave in JVP: Due to loss of coordinated atrial contraction.
- Variable S1 Intensity: S1 varies beat-to-beat depending on the preceding R-R interval.
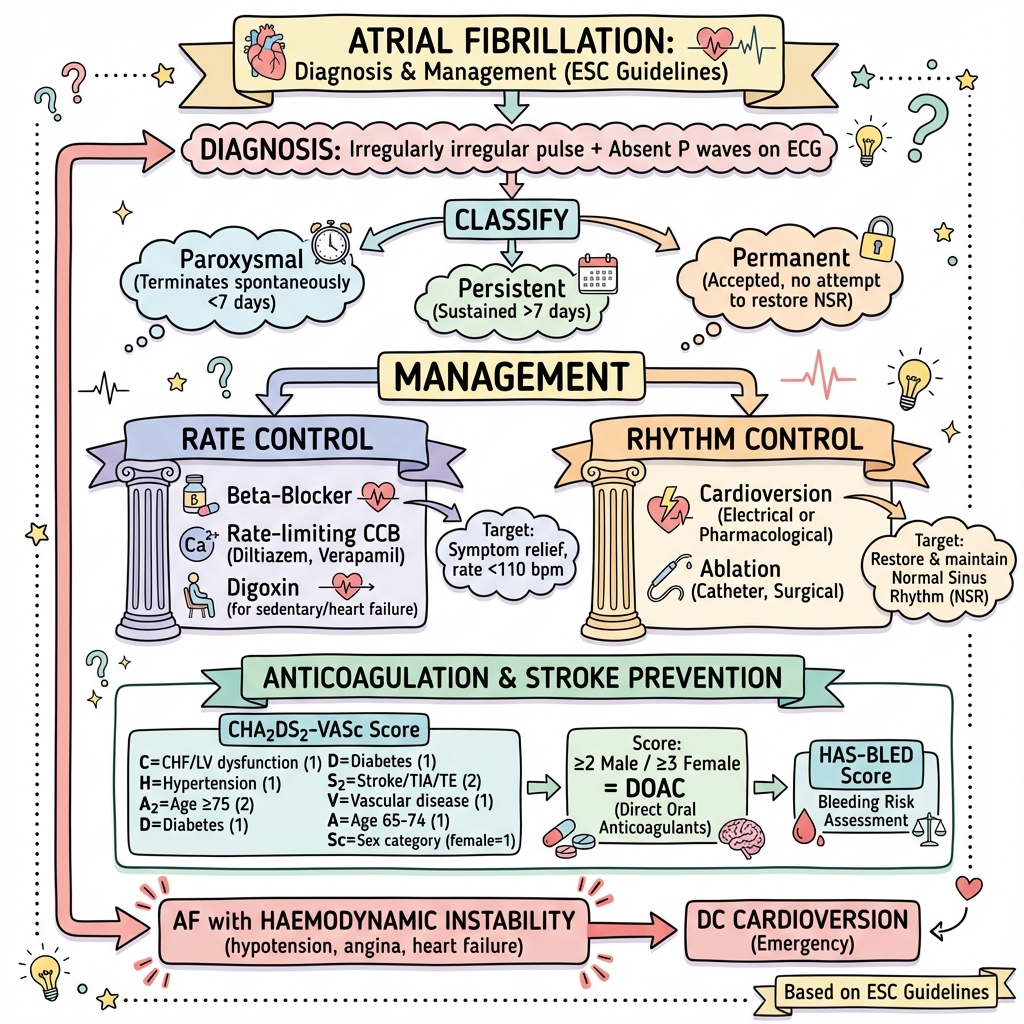
5. Investigations
The Diagnostic Strip
- 12-Lead ECG: Absent P-waves, replaced by fibrillatory 'f' waves (350-600 bpm), and irregular R-R intervals. A strip of ≥30 seconds is required for formal diagnosis.
Assessing the Substrate
- Transthoracic Echo (TTE): Essential to measure LA Volume Index (LAVI) and exclude structural heart disease.
- Thyroid Function (TFTs): Mandatory to exclude thyrotoxicosis as a trigger.
- Sleep Study (Polysomnography): Highly recommended if OSA suspected, as it is a major driver of ablation failure.
6. Management: The ABCDE Pathway
A: Anticoagulation (Avoid Stroke)
- CHA2DS2-VASc: Score ≥2 (M) or ≥3 (F) mandates OAC.
- DOAC First: Apixaban, Dabigatran, Rivaroxaban are superior to Warfarin in non-valvular AF.
- LAA Closure: For high-risk patients with absolute contraindications to OAC.
B: Better Symptom Management (Rate vs. Rhythm)
- Early Rhythm Control: The EAST-AFNET 4 trial proved that early rhythm control (Ablation/AAD) reduces CV death/stroke compared to rate control. [8]
- Rate Control: Target HR less than 110 bpm (Lenient - RACE II trial). First-line: Beta-blockers or Diltiazem.
C: Cardiovascular Risk Modification
- Weight Loss: The LEGACY trial showed > 10% weight loss yields a 6-fold reduction in AF burden.
- Alcohol: AF-ALCOHOL trial proved that abstinence significantly reduces AF recurrence. [9]
7. Catheter Ablation: The New Standard
- PVI (Pulmonary Vein Isolation): The cornerstone procedure.
- PFA (Pulsed Field Ablation): The latest "non-thermal" modality using irreversible electroporation. Safer (virtually zero risk of oesophageal fistula) and faster than traditional RF or Cryo. [10]
8. Complications
- Ischaemic Stroke: High risk due to LAA stasis.
- Tachycardiomyopathy: Chronic high HR (> 120) leading to a dilated, weak LV. Often reversible with rate control or PVI.
- Dementia: AF is an independent risk factor for cognitive decline, even in the absence of clinical stroke.
9. Evidence: Landmark Trials
| Trial | Year | Intervention | Result | Impact |
|---|---|---|---|---|
| AFFIRM | 2002 | Rate vs. Rhythm | No Difference | Made Rate Control the "safe" default for 20 years. |
| EAST-AFNET 4 | 2020 | Early Rhythm | ↓ CV Death/Stroke | Shifted paradigm: Rhythm control is now 1st line. |
| CASTLE-AF | 2018 | PVI in HFrEF | 38% ↓ Death/Hosp | Made PVI Class I for Heart Failure patients. |
| AUGUSTUS | 2019 | DOAC + P2Y12 | Less Bleeding | Ended routine Triple Therapy (OAC+ASA+P2Y12). |
| ADVENT | 2023 | PFA vs. Thermal | Non-inferior | Validated PFA as a primary ablation modality. |
10. Single Best Answer (SBA) Questions
Question 1
A 45-year-old male presents with paroxysmal AF. He is a non-smoker, BP 120/80, no history of diabetes, stroke, or heart failure. His BMI is 34. What is his CHA2DS2-VASc score and what is the primary management priority?
- A) Score 0; Warfarin
- B) Score 1; Apixaban
- C) Score 0; Weight loss and rhythm control
- D) Score 2; Digoxin
- E) Score 1; Aspirin
- Answer: C. His CHA2DS2-VASc is 0 (low risk, no OAC). Per the 2024 staging, he is Stage 3 AF with modifiable Stage 1 risks. Priority is weight loss (LEGACY trial) and early rhythm control (EAST-AFNET 4).
Question 2
You see a very fast, wide-complex, irregularly irregular rhythm on an ECG. The rate is 260 bpm. Which medication should be strictly avoided?
- A) Procainamide
- B) Adenosine
- C) Normal Saline
- D) Heparin
- E) Magnesium
- Answer: B. This describes pre-excited AF (WPW). Adenosine (and other AV-nodal blockers like BB/CCBs) can precipitate VF by forcing all impulses down the bypass tract.
11. Viva Scenario: The "WPW Alert"
Examiner: "You are in the ED and a 20-year-old presents with a heart rate of 280 bpm. The ECG is broad-complex and extremely irregular. What is your diagnosis and immediate management?"
Candidate:
- Diagnosis: This is Pre-excited Atrial Fibrillation (AF in a patient with an accessory pathway/WPW). The irregularity confirms AF, and the width is due to conduction via the bypass tract.
- Danger: I must avoid AV-nodal blocking agents (Adenosine, Beta-blockers, Calcium channel blockers, Digoxin) as they can cause a 1:1 conduction down the bypass tract, resulting in Ventricular Fibrillation.
- Management:
- If stable: IV Procainamide or Ibutilide.
- If unstable (Hypotensive/Syncope): Immediate Synchronised DC Cardioversion.
- Follow-up: Electrophysiology (EP) referral for catheter ablation of the accessory pathway.
12. Patient Explanation
"Atrial Fibrillation means the top chambers of your heart are 'shivering' instead of beating strongly. This causes blood to pool and potentially form a clot, which can travel to the brain and cause a stroke. We use 'blood thinners' to prevent this. We also want to treat the rhythm early to prevent your heart from stretching and scarring over time. The most important thing you can do is manage the 'drivers'—losing weight, treating sleep apnoea, and cutting back on alcohol are just as important as any medication we give you."
13. References
- Joglar JA, et al. 2024 AHA/ACC/AM/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation. Circulation. 2024. [PMID: 38033089]
- Kirchhof P, et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation (EAST-AFNET 4). N Engl J Med. 2020. [PMID: 32861544]
- Marrouche NF, et al. Catheter Ablation for Atrial Fibrillation with Heart Failure (CASTLE-AF). N Engl J Med. 2018. [PMID: 29412540]
- Lopes RD, et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation (AUGUSTUS). N Engl J Med. 2019. [PMID: 30883055]
- Pathak RK, et al. Long-term effect of goal-directed weight management in an AF cohort (LEGACY). J Am Coll Cardiol. 2015. [PMID: 25773166]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for atrial fibrillation?
Seek immediate emergency care if you experience any of the following warning signs: Haemodynamic instability (Hypotension, Shock), Acute heart failure (Pulmonary oedema), Pre-excitation (WPW) with rapid response, Acute stroke or TIA, Syncope or near-syncope.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Atrial Flutter
- MAT (Multifocal Atrial Tachycardia)
Consequences
Complications and downstream problems to keep in mind.
- Ischaemic Stroke
- Tachycardiomyopathy