Anal Fissure
An anal fissure is a longitudinal tear in the squamous epithelium (anoderm) of the anal canal, extending from the dentat... FRCS exam preparation.
What matters first
An anal fissure is a longitudinal tear in the squamous epithelium (anoderm) of the anal canal, extending from the dentat... FRCS exam preparation.
Lateral fissure location — consider Crohn's disease, HIV, tuberculosis, malignancy
9 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Lateral fissure location — consider Crohn's disease, HIV, tuberculosis, malignancy
- Multiple fissures — secondary cause likely
- Severe pain preventing examination — may need EUA
- Non-healing despite treatment — biopsy to exclude malignancy
Exam focus
Current exam surfaces linked to this topic.
- FRCS
Linked comparisons
Differentials and adjacent topics worth opening next.
- Crohn's Disease
- Anal Cancer
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Anal Fissure
1. Clinical Overview
Summary
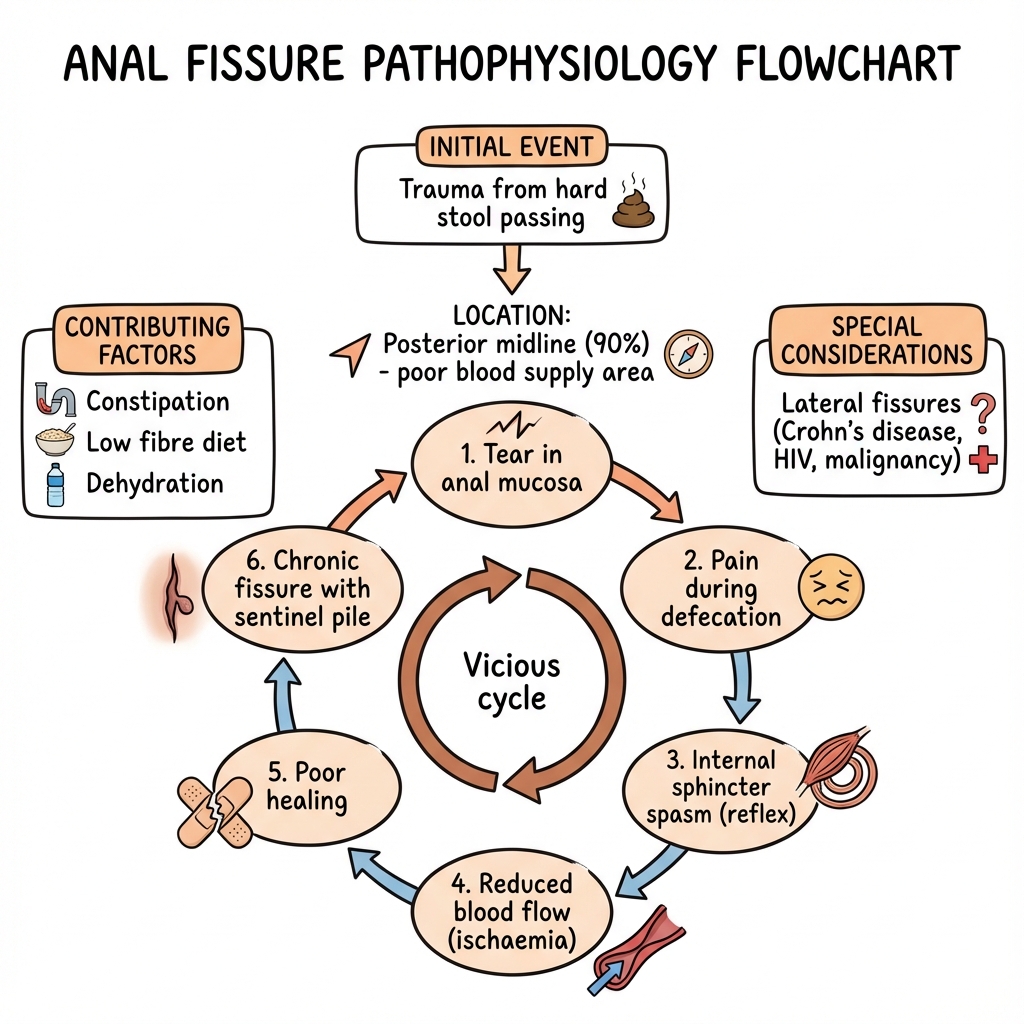
An anal fissure is a longitudinal tear in the squamous epithelium (anoderm) of the anal canal, extending from the dentate line to the anal verge, most commonly located at the posterior midline. [1,2] It represents one of the most common anorectal conditions causing severe pain and rectal bleeding, affecting approximately 11% of the general population during their lifetime. [3] The condition is characterised by an exquisitely painful tearing sensation during and after defecation, classically described as "passing broken glass," accompanied by bright red bleeding on wiping.
Fissures are classified as acute (symptoms less than 6 weeks, superficial tear with clean edges) or chronic (symptoms > 6-8 weeks, with the characteristic triad of deep ulcer with exposed internal anal sphincter fibres, sentinel pile externally, and hypertrophied anal papilla proximally). [1,4] The pathophysiology centres on internal anal sphincter (IAS) hypertonia leading to ischaemia, particularly at the relatively avascular posterior midline where blood flow is most compromised. [5,6]
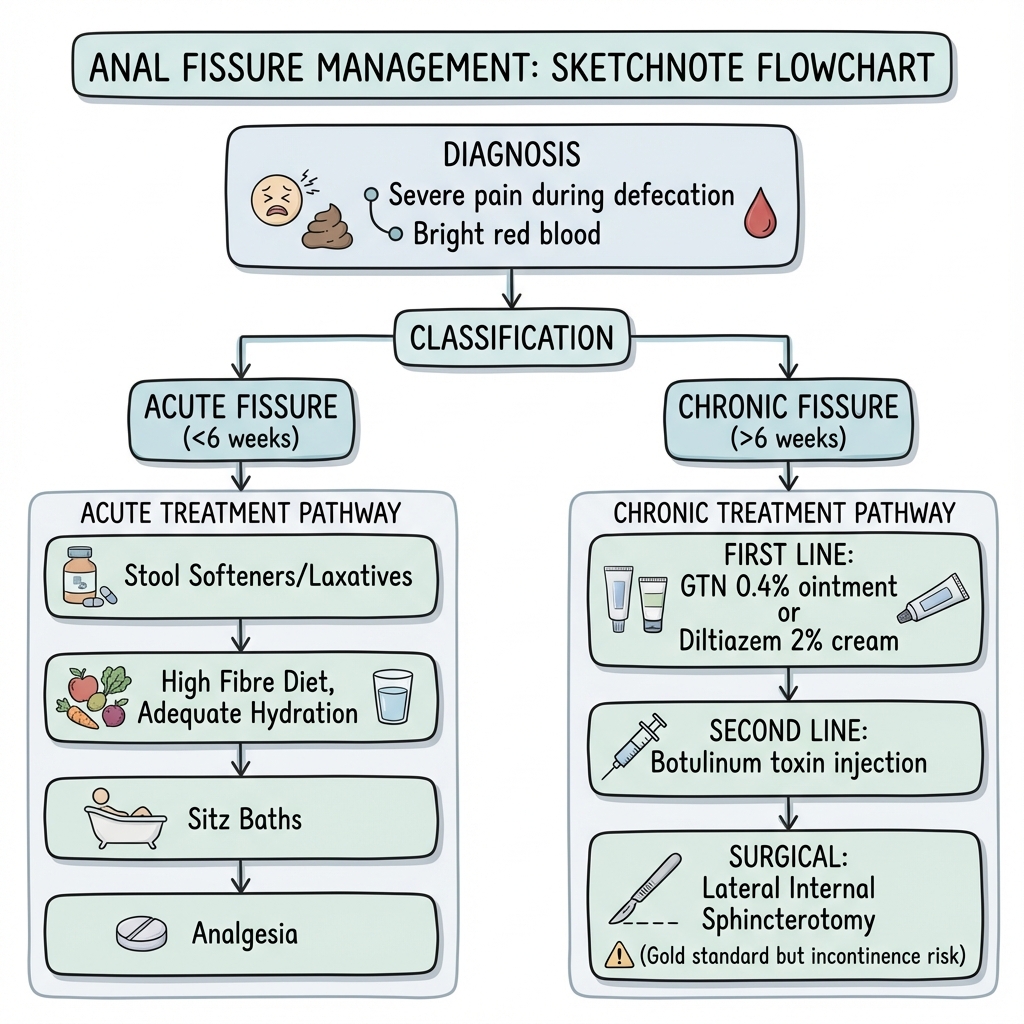
Management follows a stepwise approach: conservative measures (fibre, fluids, stool softeners, sitz baths) for acute fissures; pharmacological sphincter relaxation (topical GTN, diltiazem, or nifedipine) for chronic fissures; and surgical intervention (lateral internal sphincterotomy) for medically refractory cases. [1,7] Recognition of atypical fissures (lateral position, multiple, painless) is critical as these require investigation for secondary causes including Crohn's disease, tuberculosis, HIV, syphilis, and malignancy. [8,9]
Key Facts
| Feature | Details |
|---|---|
| Definition | Longitudinal tear in anoderm distal to dentate line |
| Lifetime Prevalence | 10-11% of general population [3] |
| Peak Age | 20-40 years; bimodal (young adults, elderly) |
| Sex Distribution | Equal in young adults; anterior fissures more common in women |
| Location | Posterior midline 85-90%; Anterior midline 10-15% (25% in women) [1,10] |
| Classic Symptom | Severe tearing pain during/after defecation + bright red blood |
| Acute vs Chronic | less than 6 weeks vs > 6-8 weeks; chronic has triad features |
| First-Line Medical Rx | Topical GTN 0.2-0.4% or Diltiazem 2% BD for 6-8 weeks |
| Gold-Standard Surgery | Lateral internal sphincterotomy (> 95% healing) [11] |
| Critical Finding | Lateral/atypical fissures = ALWAYS investigate secondary cause |
Clinical Pearls
"Posterior Midline Predominance": 85-90% of primary fissures occur at the posterior midline due to poor blood supply in this watershed zone. The posterior commissure receives terminal branches of the inferior rectal artery, creating a relatively ischaemic area vulnerable to trauma and poor healing. [5,6]
"The Vicious Cycle": Fissure → pain → sphincter spasm → elevated resting anal pressure → reduced blood flow → ischaemia → impaired healing → chronic fissure. Breaking this cycle through chemical or surgical sphincter relaxation is the cornerstone of treatment. [5]
"The Chronic Triad": A chronic fissure demonstrates three pathognomonic features visible on examination: (1) deep ulcer with exposed white internal anal sphincter fibres at base, (2) sentinel pile (skin tag) at external margin, (3) hypertrophied anal papilla at proximal margin. [1,4]
"Never Miss Secondary Causes": Lateral fissures, multiple fissures, painless presentation, non-healing despite optimal treatment, or associated perianal disease should prompt investigation for Crohn's disease (most common), tuberculosis, HIV/AIDS, syphilis, or malignancy. [8,9]
"Anterior Fissures in Women": Up to 25% of fissures in women are anterior, often related to obstetric trauma. These have higher rates of surgical failure and incontinence risk with sphincterotomy. [10,12]
Why This Matters Clinically
Anal fissure causes disproportionate suffering relative to its pathological severity. Patients experience severe pain leading to fear of defecation, stool withholding, worsening constipation, and a self-perpetuating cycle of trauma and chronicity. Despite its benign nature, untreated chronic fissures significantly impair quality of life. Accurate diagnosis (usually clinical) and appropriate stepwise management lead to rapid symptom relief and high healing rates. Failure to recognise atypical fissures can delay diagnosis of serious underlying conditions including inflammatory bowel disease and malignancy.
2. Epidemiology
Incidence and Prevalence
| Measure | Value | Source |
|---|---|---|
| Lifetime prevalence | 10-11% | [3] |
| Annual incidence | 1.1 per 1,000 person-years | [13] |
| Peak incidence age | 20-40 years | [1,3] |
| GP consultations | Common; accounts for 6-15% of proctology referrals | [1] |
| Sex ratio | M:F = 1:1 overall; anterior more common in females | [10] |
| Recurrence rate (conservative) | 30-40% | [7] |
| Recurrence rate (post-LIS) | less than 5% | [11] |
Demographics
| Factor | Details |
|---|---|
| Age | Bimodal distribution: young adults (20-40), second peak in elderly; also common in infants (0-1 year) |
| Sex | Equal overall; anterior fissures 3x more common in women (25% vs 8% in men) |
| Ethnicity | No significant ethnic variation documented |
| Geography | More prevalent in developed countries; associated with Western low-fibre diet |
| Socioeconomic | No clear association |
Risk Factors
Non-Modifiable Risk Factors:
| Factor | Relative Risk | Mechanism |
|---|---|---|
| Previous anal fissure | 2-3x | Scarring, fibrosis, reduced compliance |
| Childbirth (vaginal) | 2.5x | Perineal trauma, sphincter injury [10] |
| Instrumental delivery | 3-4x | Direct sphincter damage |
| Previous anal surgery | Variable | Altered anatomy, scarring |
| Female sex (anterior fissures) | 3x for anterior | Anatomical: shorter perineal body |
Modifiable Risk Factors:
| Risk Factor | Mechanism | Prevention Strategy |
|---|---|---|
| Constipation | Hard stool causes mechanical trauma | High fibre diet (25-30g/day), adequate fluids |
| Chronic diarrhoea | Chemical irritation, frequent wiping | Treat underlying cause, barrier cream |
| Low fibre diet | Promotes hard stools | Dietary modification, fibre supplements |
| Dehydration | Contributes to hard stools | 2-3L fluid daily |
| Prolonged straining | Elevated intra-anal pressure, venous congestion | Avoid straining, limit toilet time less than 5 minutes |
| Anal intercourse | Direct mechanical trauma | Adequate lubrication |
| Obesity | Associated constipation, pelvic floor dysfunction | Weight management |
Associated Conditions
Primary Associations:
| Condition | Association Type | Clinical Significance |
|---|---|---|
| Crohn's disease | Strong | Lateral/multiple fissures, fistulae, non-healing; 10-30% of Crohn's patients develop fissures [9] |
| Ulcerative colitis | Moderate | Less common than Crohn's; posterior predominance preserved |
| Constipation disorders | Strong | Both cause and consequence |
| Irritable bowel syndrome | Moderate | Altered bowel habit contributes |
Secondary/Atypical Fissure Associations:
| Condition | Fissure Characteristics | Key Features |
|---|---|---|
| HIV/AIDS | Multiple, lateral, non-healing | Consider CMV, HSV co-infection; CD4 count correlates with healing [14] |
| Tuberculosis | Chronic, non-healing, multiple | Rare; consider in endemic areas; biopsy shows caseating granulomas |
| Syphilis | Painless chancre (primary) | Serology essential; consider in MSM |
| Anal carcinoma | Non-healing, indurated edges | Biopsy mandatory for non-healing fissures [8] |
| Leukaemia | Poor healing, infection | Neutropaenia impairs healing |
| Chemotherapy/immunosuppression | Atypical, non-healing | Healing correlates with immune recovery |
3. Pathophysiology
Anatomical Basis
Relevant Anatomy of the Anal Canal:
The anal canal is approximately 4cm in length, extending from the anorectal junction to the anal verge. Key anatomical structures relevant to fissure pathophysiology include:
- Anoderm: Modified squamous epithelium distal to the dentate line, richly innervated by somatic sensory nerves (inferior rectal nerve) — accounting for the severe pain of fissures
- Internal Anal Sphincter (IAS): Smooth muscle; continuation of circular muscle of rectum; involuntary control; responsible for 70-85% of resting anal tone
- External Anal Sphincter (EAS): Striated muscle; voluntary control; encircles IAS
- Posterior Commissure: Area of anatomical vulnerability where external sphincter fibres diverge, creating a potential weak point
Vascular Anatomy (Critical to Pathophysiology):
The blood supply to the anal canal demonstrates important regional variation: [5,6]
| Region | Blood Supply | Clinical Significance |
|---|---|---|
| Upper anal canal | Superior rectal artery (branch of IMA) | Well-perfused |
| Lower anal canal | Inferior rectal artery (branch of internal pudendal) | Terminal branches; less robust |
| Posterior midline | Watershed zone; terminal branches of inferior rectal | Relatively ischaemic; 85% lower perfusion than lateral quadrants |
| Anterior midline | Similar watershed territory | Second most common fissure location |
| Lateral quadrants | Best perfusion | Fissures here suggest secondary cause |
Exam Detail: Klosterhalfen Angiographic Studies: Seminal work by Klosterhalfen et al. demonstrated that the posterior midline receives significantly reduced blood flow compared to other quadrants. Angiographic studies showed perfusion of the posterior commissure was 85% lower than lateral quadrants. This "watershed zone" theory explains both the posterior predominance of primary fissures and the mechanism of ischaemia-driven poor healing. [5]
Pathophysiological Mechanism
The Ischaemia-Hypertonia Cycle:
The pathophysiology of anal fissure centres on a self-perpetuating cycle of trauma, pain, sphincter spasm, and ischaemia: [5,6,15]
Step 1: Initial Trauma
- Hard stool passage causes mechanical tear in the anoderm
- Occurs preferentially at posterior midline (90%) due to:
- Poorest blood supply (watershed zone)
- Posterior divergence of external sphincter fibres creates weak point
- Direction of faecal stream during defecation
Step 2: Pain Response
- Anoderm is richly innervated with somatic sensory fibres (inferior rectal nerve)
- Intense sharp pain during and for hours after defecation
- Pain triggers protective sphincter contraction
Step 3: Internal Anal Sphincter Hypertonia
- Reflex spasm of IAS in response to pain
- Mean resting anal pressure elevated to 90-120 mmHg (normal: 40-70 mmHg) [5,15]
- Hypertonia persists beyond acute pain episode
- Creates sustained compression of intramural blood vessels
Step 4: Ischaemia and Impaired Healing
- Elevated IAS tone compresses terminal branches of inferior rectal artery
- Anodermal blood flow reduced by up to 85% at posterior midline [5]
- Hypoxic wound environment prevents healing
- Exposed wound base subject to repeated trauma with each defecation
Step 5: Chronic Fissure Formation
- Acute fissure fails to heal; becomes chronic (> 6-8 weeks)
- Development of characteristic chronic triad:
- "Sentinel pile (skin tag): Oedematous external skin at distal wound margin from chronic inflammation"
- "Hypertrophied anal papilla: Fibrotic overgrowth at proximal (internal) wound margin"
- "Exposed sphincter fibres: Deep ulcer exposes white IAS muscle at wound base"
- Fibrosis develops at wound margins, further impairing healing
Step 6: Cycle Perpetuation
- Fear of pain leads to stool withholding
- Constipation worsens; stools become harder
- Further trauma to unhealed fissure with each defecation
- Cycle continues until sphincter tone is reduced (medically or surgically)
Exam Detail: Manometric Evidence: Studies consistently demonstrate that patients with chronic anal fissure have significantly elevated maximum resting anal pressure (MRAP) compared to controls:
- Normal MRAP: 40-70 mmHg
- Chronic fissure MRAP: 90-120 mmHg
- After successful treatment (medical or surgical): MRAP normalises
- This elevated tone is the therapeutic target of all treatments [5,15]
Classification
Temporal Classification:
| Type | Duration | Pathological Features | Treatment Approach |
|---|---|---|---|
| Acute Fissure | less than 6 weeks | Superficial tear; clean, sharp edges; minimal fibrosis; healthy base | Conservative management (fibre, fluids, stool softeners, sitz baths); 50-60% heal spontaneously [7] |
| Chronic Fissure | > 6-8 weeks | Deep ulcer; exposed IAS fibres; sentinel pile; hypertrophied papilla; fibrotic edges | Medical therapy (GTN, diltiazem) ± botulinum toxin; surgery if refractory [1] |
Aetiological Classification:
| Type | Location | Characteristics | Causes |
|---|---|---|---|
| Primary (Idiopathic) | Posterior midline (85-90%) or Anterior midline (10-15%) | Single; typical chronic features; associated with IAS hypertonia | Constipation, hard stool trauma, childbirth |
| Secondary | Lateral; off-midline; multiple | Atypical features; may be painless; associated pathology | Crohn's disease, HIV, TB, syphilis, malignancy, leukaemia |
Location Significance
| Location | Frequency | Clinical Implications |
|---|---|---|
| Posterior midline | 85-90% males; 75% females | Primary fissure; standard management pathway |
| Anterior midline | 8-10% males; 20-25% females | Primary fissure; higher incontinence risk with surgery; consider obstetric history in women |
| Lateral | less than 2% of primary | ALWAYS investigate for secondary cause |
| Multiple | Rare in primary | ALWAYS investigate — Crohn's disease, HIV, immunosuppression |
| Circumferential | Very rare | Severe Crohn's disease or other IBD; rarely primary |
4. Clinical Presentation
Symptoms
Cardinal Symptoms:
| Symptom | Frequency | Characteristics |
|---|---|---|
| Pain | 95-100% | Severe, sharp, tearing quality; "like passing broken glass"; occurs during defecation and persists for minutes to hours afterwards; may be incapacitating |
| Bleeding | 70-80% | Bright red blood; on toilet paper or surface of stool; small volume (streaking); rarely significant blood loss |
| Constipation | 50-60% | Often pre-existing (cause); may worsen due to fear of defecation (consequence) |
| Pruritus ani | 20-30% | Mild perianal itching between bowel movements; from discharge/moisture |
| Discharge | 10-20% | Minimal mucoid or serosanguinous; more common in chronic fissures |
Symptom Characteristics:
Pain Pattern:
- Begins with passage of stool through anal canal
- Sharp, cutting quality during defecation
- Persists as dull ache or burning for 30 minutes to several hours post-defecation
- May be so severe patient avoids defecation (exacerbating constipation)
- Pain-free interval between bowel movements (distinguishes from other conditions)
Bleeding Pattern:
- Bright red (arterial)
- Small volume — streaks on toilet paper or surface of stool
- Occurs with each bowel movement
- Rarely causes anaemia (consider alternative diagnosis if significant)
Atypical Presentations
| Presentation | Clinical Significance | Likely Cause |
|---|---|---|
| Painless fissure | Suggests denervation or secondary cause | Crohn's disease, neurological disorder, HIV, diabetes |
| Lateral location | Secondary cause mandatory to exclude | Crohn's (most common), TB, HIV, malignancy, syphilis |
| Multiple fissures | Secondary cause highly likely | Crohn's disease, HIV/AIDS, immunosuppression |
| Minimal/no bleeding | Can occur with chronic, fibrotic fissures | Chronic fissure or secondary cause |
| Purulent discharge | Associated abscess or fistula | Crohn's disease, cryptoglandular abscess |
| Weight loss, systemic symptoms | Malignancy or IBD | Requires urgent investigation |
Signs
Examination Findings (Inspection):
| Finding | Acute Fissure | Chronic Fissure | Significance |
|---|---|---|---|
| Fissure | Superficial tear; clean edges | Deep ulcer; exposed white IAS fibres | Defines chronicity |
| Sentinel pile | Absent | Present (external skin tag at distal margin) | Indicates chronic fissure |
| Hypertrophied papilla | Absent | Present (at proximal margin — seen on anoscopy) | Indicates chronic fissure |
| Location | Usually posterior midline | Usually posterior midline | Lateral = investigate |
| Surrounding skin | Normal | May show excoriation, dermatitis | Chronic irritation |
Digital Rectal Examination:
- Often not possible due to severe pain and sphincter spasm
- If tolerable:
- High resting tone (hypertonia)
- Marked tenderness at fissure site
- Palpable fibrous band (chronic fissure)
- Exclude rectal mass
- Important: Do NOT force examination if severe pain — defer or perform under anaesthesia (EUA)
Anoscopy/Proctoscopy:
- Usually deferred in acute setting due to pain
- If tolerated (with topical anaesthetic):
- Visualises fissure directly
- Identifies hypertrophied papilla at proximal margin
- Excludes other pathology (haemorrhoids, polyps, masses)
- May require EUA if pain prohibitive
Red Flags
[!CAUTION] Red Flags Requiring Further Investigation:
Location:
- Lateral or off-midline fissure → Crohn's disease, HIV, TB, malignancy
- Multiple fissures → Secondary cause (Crohn's most common)
Symptoms:
- Painless fissure → Unusual; consider Crohn's, neuropathy, malignancy
- Systemic symptoms (weight loss, fatigue, night sweats) → IBD, malignancy
- Fever → Associated abscess, systemic infection
Examination:
- Indurated or raised edges → Malignancy — biopsy mandatory
- Associated fistula or abscess → Crohn's disease
- Multiple skin tags → Crohn's disease
- Severe pain preventing any examination → May need EUA
Response to Treatment:
- Non-healing despite 8+ weeks optimal medical therapy → Biopsy to exclude malignancy
- Recurrent fissures despite treatment → Consider secondary cause
5. Differential Diagnosis
Key Differentials
| Diagnosis | Key Distinguishing Features | Investigations |
|---|---|---|
| Haemorrhoids | Painless bleeding (unless thrombosed); prolapsing tissue; no fissure on inspection | Clinical examination; anoscopy |
| Perianal abscess | Continuous throbbing pain (not just defecation-related); swelling; fluctuance; fever | Examination; CT/MRI if deep |
| Anal fistula | Persistent discharge from external opening; may have history of abscess | Probe; MRI pelvis |
| Crohn's disease | Multiple/lateral fissures; associated GI symptoms; fistulae; "elephant ear" skin tags | Colonoscopy; biopsies; inflammatory markers |
| Anal cancer (SCC) | Non-healing ulcer; indurated edges; bleeding; weight loss | Biopsy mandatory |
| Solitary rectal ulcer | Lower rectal pain; mucus; tenesmus; prolapse history | Proctoscopy; biopsy |
| Proctalgia fugax | Severe episodic rectal pain; no structural lesion; no bleeding | Clinical diagnosis; normal examination |
| Perianal herpes (HSV) | Vesicles; multiple shallow ulcers; immunocompromised patient | Viral PCR; serology |
| Syphilitic chancre | Painless ulcer (primary syphilis); MSM risk factors | Syphilis serology; dark-field microscopy |
| TB (anorectal) | Chronic non-healing; endemic region; pulmonary TB | Biopsy with AFB; PCR; CXR |
Must Not Miss Diagnoses
- Anal cancer — Non-healing fissure > 8 weeks despite treatment; indurated edges; irregular ulcer → Biopsy
- Crohn's disease — Lateral/multiple fissures; associated fistulae; GI symptoms → Colonoscopy
- HIV-related fissures — Atypical features; immunosuppression; poor healing → HIV test
- Malignancy — Weight loss; mass; lymphadenopathy → Urgent investigation
6. Investigations
Clinical Diagnosis
For typical primary anal fissures:
- History and careful inspection are usually diagnostic
- No routine investigations required if classic presentation
- Digital rectal examination if tolerated (assess tone, exclude mass)
Indications for Further Investigation
Investigation is required for:
- Atypical location (lateral, multiple)
- Non-healing despite optimal treatment (> 8 weeks)
- Clinical suspicion of secondary cause
- Systemic symptoms (weight loss, change in bowel habit)
- High-risk features for malignancy
- Pre-operative assessment before surgery
Laboratory Investigations
| Test | Purpose | When to Order |
|---|---|---|
| FBC | Anaemia screen; infection; leukaemia | Significant bleeding; systemic symptoms; non-healing |
| CRP/ESR | Inflammatory markers | Suspected Crohn's disease or IBD |
| HIV test | Immunodeficiency screen | Atypical/lateral/multiple fissures; risk factors |
| Syphilis serology (RPR/TPHA) | Exclude primary chancre | Painless ulcer; MSM; risk factors |
| HbA1c | Diabetes (impairs healing) | Chronic non-healing; risk factors |
| Stool cultures | Exclude infectious diarrhoea | Diarrhoea-associated fissure |
| Faecal calprotectin | IBD screening | Suspected Crohn's or UC |
Imaging
| Modality | Findings | Indications |
|---|---|---|
| Endoanal ultrasound | Sphincter anatomy; defects; previous injury | Pre-operative assessment for sphincterotomy; women with obstetric history; recurrent fissure |
| MRI Pelvis | Fistula mapping; sphincter anatomy; perianal inflammation | Suspected Crohn's; associated fistula; complex perianal disease |
| CT abdomen/pelvis | Exclude abscess; staging if malignancy | Deep abscess suspected; malignancy staging |
Endoscopy
| Investigation | Purpose | Indications |
|---|---|---|
| Anoscopy | Visualise fissure and upper anal canal | Confirm diagnosis; visualise papilla; exclude other pathology |
| Proctoscopy | Lower rectal examination | Exclude rectal pathology |
| Flexible sigmoidoscopy | Left colon/rectum assessment | Suspected IBD; atypical presentation |
| Colonoscopy | Full colonic assessment | Confirmed/suspected IBD; change in bowel habit; iron deficiency anaemia |
Biopsy
Indications for Biopsy:
- Non-healing fissure after 8+ weeks of optimal medical treatment
- Atypical location (lateral)
- Raised, indurated, or irregular edges
- Clinical suspicion of malignancy
- Suspected Crohn's disease (may show granulomas)
- Suspected TB (caseating granulomas, AFB)
Anorectal Physiology (Manometry)
| Test | Purpose | Findings in Fissure |
|---|---|---|
| Anorectal manometry | Measure resting and squeeze pressures | Elevated resting pressure (90-120 mmHg); normal squeeze pressure |
| Rectal sensory testing | Assess rectal compliance | Usually normal |
Clinical Use: Manometry is not routinely required but may be useful for:
- Pre-operative assessment (identify low baseline pressure — incontinence risk)
- Research purposes
- Recurrent fissures with failed surgery
- Assessment of continence pre-operatively in high-risk patients
7. Management
Management Principles
- Break the ischaemia-hypertonia cycle — Reduce IAS tone to improve blood flow and healing
- Promote soft, painless bowel movements — Prevent further trauma
- Stepwise approach — Conservative → Medical → Surgical (increasing efficacy but also risks)
- Address underlying cause — Essential for secondary fissures
- Informed consent — Especially for surgery (incontinence risk)
Management Algorithm
ACUTE ANAL FISSURE (less than 6 weeks)
↓
Conservative Management (8 weeks)
- Dietary fibre 25-30g/day
- Fluids 2-3L/day
- Stool softeners (lactulose/macrogol)
- Sitz baths (warm water 10-15 min post-defecation)
- Topical lidocaine (short-term analgesia)
↓
┌──────┴──────┐
Healed Not Healed
↓ ↓
Maintain Becomes CHRONIC FISSURE
lifestyle (> 6-8 weeks)
measures ↓
Topical Medical Therapy (6-8 weeks)
GTN 0.2-0.4% OR Diltiazem 2% BD
↓
┌─────┴─────┐
Healed Not Healed
↓ ↓
Continue Second-line:
lifestyle - Switch agent (GTN ↔ Diltiazem)
measures - Botulinum Toxin Injection
↓
┌─────┴─────┐
Healed Still Not Healed
↓ ↓
Lifestyle SURGICAL MANAGEMENT
measures Lateral Internal Sphincterotomy
(after counselling re incontinence risk)
Conservative Management (All Patients)
| Intervention | Details | Evidence |
|---|---|---|
| Dietary fibre | 25-30g/day; fruits, vegetables, wholegrain; or supplements (ispaghula, psyllium) | Softens stool; reduces straining [1,7] |
| Fluid intake | 2-3L water/day | Prevents stool hardening |
| Stool softeners | Lactulose 15-30mL BD; Macrogol (Movicol) 1-2 sachets daily | Osmotic laxatives preferred [7] |
| Sitz baths | Warm water soak for 10-15 minutes after defecation; 2-3x daily | Relaxes sphincter; reduces pain; improves blood flow |
| Analgesia | Oral paracetamol/NSAIDs 30 min before defecation; avoid opioids (constipating) | Reduces defecation anxiety |
| Topical anaesthetics | Lidocaine gel 2% (short-term only) | Temporary pain relief; may mask symptoms |
| Avoid straining | Limit toilet time less than 5 minutes; do not defer urge | Reduces further trauma |
Efficacy of Conservative Management:
- Acute fissures: 50-60% heal with conservative measures alone [7]
- Chronic fissures: less than 10% heal without pharmacological intervention [1]
Medical Management (Chronic Fissure)
First-Line Topical Agents:
| Agent | Dose/Application | Mechanism | Healing Rate | Side Effects |
|---|---|---|---|---|
| GTN 0.2-0.4% (Rectogesic) | Apply pea-sized amount to anal margin BD for 6-8 weeks | Nitric oxide donor → smooth muscle relaxation → IAS relaxation | 49-68% | Headache (20-50%); tolerance; hypotension [7,16] |
| Diltiazem 2% | Apply BD for 6-8 weeks | Calcium channel blocker → IAS relaxation | 65-75% | Headache (10-20%); perianal itch; better tolerated than GTN [7,16] |
| Nifedipine 0.2-0.3% | Apply BD for 6-8 weeks | Calcium channel blocker → IAS relaxation | 60-70% | Similar to diltiazem; less headache [17] |
Exam Detail: Evidence Summary: GTN vs Diltiazem
The Cochrane systematic review by Nelson et al. (2012) analysed 75 RCTs with 5,031 participants. Key findings: [7]
- GTN 0.4% healed 48.9% of fissures vs 35.5% with placebo (pless than 0.0009)
- Calcium channel blockers (diltiazem, nifedipine) showed equivalent efficacy to GTN
- Diltiazem had significantly fewer headaches (10-20% vs 20-50%)
- All medical therapies had high recurrence rates (30-50% within 1 year)
- "Medical therapy is marginally better than placebo but far less effective than surgery"
ASCRS Guidelines Recommendation (2023): [1]
- Topical GTN or calcium channel blockers are first-line for chronic anal fissure (Strong recommendation, moderate-quality evidence)
- Diltiazem may be preferred due to better tolerability
Application Technique:
- Wash hands before and after application
- Apply pea-sized amount to external anal margin and lower anal canal
- Do NOT insert deeply into anal canal
- Apply after defecation and at bedtime (BD)
- Continue for full 6-8 week course even if symptoms improve
- Warn patient about headache — often improves after first week
Second-Line Medical Therapy:
| Agent | Dose/Technique | Mechanism | Healing Rate | Notes |
|---|---|---|---|---|
| Botulinum Toxin A (Botox) | 20-100 units injected into IAS (under local/sedation) | Inhibits acetylcholine release → temporary sphincter paralysis | 65-85% | Effect lasts 3-4 months; may repeat; 5-10% temporary incontinence to flatus [11,18] |
Botulinum Toxin Injection Details:
- Dose: 20-100 units (commonly 40-80 units) [18]
- Site: Injected directly into IAS, typically at two sites (lateral quadrants) to avoid fissure base
- Onset: 2-3 days; maximum effect at 2-4 weeks
- Duration: 3-4 months (reversible)
- Advantages: Avoids permanent sphincterotomy; repeatable
- Disadvantages:
- Temporary (recurrence 40-50% at 2 years) [11]
- Cost of Botox
- Temporary incontinence to flatus (5-10%)
- Best candidates: Patients with high incontinence risk; bridge to surgery; patients declining surgery
Exam Detail: Meta-analysis: Botox vs Lateral Sphincterotomy [18]
Sajid et al. (2012) systematic review findings:
- LIS: 94.8% healing rate
- Botox: 69.5% healing rate
- Recurrence: Higher with Botox (25% vs 2%)
- Incontinence: Similar rates between groups
- Conclusion: LIS more effective but Botox viable for patients refusing or unsuitable for surgery
Surgical Management
Indications for Surgery:
- Failure of medical therapy (> 8-12 weeks of optimised treatment)
- Recurrent chronic fissure
- Patient preference (informed consent regarding efficacy vs risks)
- Severe symptoms affecting quality of life
- Intolerance of medical therapy
Lateral Internal Sphincterotomy (LIS):
| Feature | Details |
|---|---|
| Procedure | Division of IAS at lateral position (away from fissure) to level of dentate line |
| Approach | Open or closed (subcutaneous) technique; similar efficacy |
| Anaesthesia | Local + sedation, regional, or general |
| Setting | Day case surgery |
| Healing rate | 95-98% [1,11] |
| Recurrence | less than 5% |
| Recovery | 1-2 weeks until full activity |
Surgical Technique:
Open Technique:
- Patient in lithotomy or left lateral position
- Identify intersphincteric groove at lateral position (3 or 9 o'clock)
- Make radial incision (1-2cm) over intersphincteric groove
- Identify and isolate lower IAS fibres
- Divide IAS from lower edge to dentate line (tailored/controlled)
- Achieve haemostasis
- Close skin with absorbable suture
Closed Technique:
- Small stab incision at intersphincteric groove
- Insert blade (No. 11 or cataract knife) into intersphincteric plane
- Divide IAS under digital guidance
- Smaller wound; similar outcomes
Division Length:
- Tailored sphincterotomy (division to level of fissure apex) reduces incontinence while maintaining efficacy [1]
- Full sphincterotomy (to dentate line) has highest healing but also highest incontinence rates
- Modern practice favours tailored approach
Complications of Lateral Internal Sphincterotomy:
| Complication | Incidence | Management |
|---|---|---|
| Minor incontinence (flatus, soiling) | 8-12% | Usually temporary; pelvic floor exercises |
| Major incontinence (faeces) | 1-3% | Rare; may require further surgery if persistent |
| Recurrence | 2-5% | Repeat sphincterotomy or alternative procedure |
| Bleeding | less than 5% | Usually minor; pressure |
| Infection | less than 2% | Antibiotics; drainage if abscess |
| Keyhole deformity | Rare | May affect continence |
Pre-operative Assessment for LIS:
- Endoanal ultrasound: Assess sphincter integrity, identify pre-existing defects
- Anorectal manometry: Identify low resting tone (higher incontinence risk)
- Detailed history: Obstetric trauma, previous anal surgery, baseline continence
- Counsel all patients about permanent incontinence risk
High-Risk Patients for Incontinence:
- Women (especially multiparous, instrumental delivery)
- Previous sphincter injury
- Low baseline resting pressure on manometry
- Elderly patients
- Pre-existing minor incontinence symptoms
- Anterior fissures (avoid anterior sphincterotomy)
Alternative Surgical Procedures:
| Procedure | Indication | Advantages | Disadvantages |
|---|---|---|---|
| Fissurectomy | Chronic fissure with sentinel pile | Removes chronic wound; allows fresh healing | Does not address sphincter hypertonia |
| Fissurectomy + advancement flap | High incontinence risk; prior sphincterotomy | Preserves sphincter; good healing rates | More complex; donor site morbidity |
| Anal advancement flap | Failed sphincterotomy; incontinence risk | Covers defect with healthy tissue | Technical; variable results |
| Posterior midline sphincterotomy | Historical; rarely used | Direct access to fissure | Higher incontinence; keyhole deformity |
Management of Secondary Fissures
Crohn's Disease:
- Treat underlying Crohn's disease (immunomodulators, biologics)
- Conservative measures for fissure
- Avoid sphincterotomy (high failure rate; incontinence risk)
- Consider Botox if fissure symptomatic and Crohn's controlled
- Fistula/abscess management may take priority
- Involve IBD specialist
HIV/AIDS:
- Optimise antiretroviral therapy (healing correlates with immune reconstitution)
- Conservative management
- Avoid surgery if CD4 less than 200 (poor healing)
- Investigate for opportunistic infections (CMV, HSV)
Tuberculosis:
- Anti-tuberculous chemotherapy
- Fissure often heals with systemic treatment
- Biopsy to confirm diagnosis
Malignancy:
- Urgent biopsy and staging
- Oncological treatment (chemoradiation for SCC)
- Surgical excision if appropriate
- Multidisciplinary team management
Disposition and Follow-up
| Setting | Recommendation |
|---|---|
| Acute fissure (GP) | Conservative management; review at 4-6 weeks; refer if not healing |
| Chronic fissure (GP/Specialist) | Medical therapy 8 weeks → surgical referral if failed |
| Post-medical therapy | Review at 8 weeks; assess healing; if healed, maintain lifestyle measures |
| Post-LIS | Review at 6 weeks; assess healing and continence |
| Long-term | Maintain high fibre diet; adequate fluids; avoid constipation to prevent recurrence |
8. Complications
Complications of Untreated Anal Fissure
| Complication | Incidence | Clinical Features | Management |
|---|---|---|---|
| Chronicity | 40% of untreated acute fissures | Persistent symptoms > 6-8 weeks; chronic triad features | Medical therapy → surgery |
| Sentinel pile | Common in chronic | External skin tag at distal fissure margin | Excision if symptomatic; usually with fissure treatment |
| Anal stenosis | Rare (less than 5%) | Difficulty passing stool; narrowed anal canal; fibrosis | Anal dilation; stricturoplasty; flap surgery |
| Quality of life impairment | Very common | Fear of defecation; avoidance behaviours; depression | Definitive fissure treatment |
| Chronic constipation | Common | Stool withholding from pain | Address fissure; laxatives |
| Abscess/fistula | Rare (unless Crohn's) | New pain; swelling; discharge | Surgical drainage |
Complications of Treatment
Medical Therapy Complications:
| Treatment | Complication | Incidence | Management |
|---|---|---|---|
| GTN | Headache | 20-50% | Often improves after 1-2 weeks; reduce dose; switch to CCB |
| GTN | Tachyphylaxis | Variable | Drug holiday; switch agent |
| GTN | Hypotension | less than 5% | Caution with concurrent nitrates; phosphodiesterase inhibitors contraindicated |
| Diltiazem | Headache | 10-20% | Reduce dose; switch agent |
| Diltiazem | Perianal itch/dermatitis | 5-10% | Barrier cream; consider alternative |
| Botox | Temporary incontinence (flatus) | 5-10% | Resolves as effect wears off (3-4 months) |
| Botox | Failure to heal | 20-30% | Repeat injection or surgery |
Surgical Complications (LIS):
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Minor incontinence (flatus, soiling) | 8-12% | Obstetric trauma; prior surgery; excessive division | Usually temporary; pelvic floor exercises; biofeedback |
| Major incontinence (faeces) | 1-3% | As above; full sphincterotomy | May require repair surgery if persistent |
| Recurrence | 2-5% | Insufficient division; secondary cause | Investigate; consider repeat surgery |
| Bleeding | less than 5% | Anticoagulants | Pressure; cautery; rarely exploration |
| Infection | less than 2% | Immunosuppression; diabetes | Antibiotics; drainage |
| Keyhole deformity | Rare | Posterior sphincterotomy | Avoid posterior approach |
| Delayed wound healing | 5-10% | Diabetes; immunosuppression; smoking | Wound care; optimise risk factors |
9. Prognosis and Outcomes
Natural History
- Acute fissures: 50-60% heal spontaneously within 4-6 weeks with conservative measures alone [7]
- Untreated acute fissures: ~40% progress to chronic fissures [1]
- Chronic fissures: Rarely heal spontaneously (less than 10%) due to persistent ischaemia-hypertonia cycle [7]
- Recurrence: Common if underlying risk factors (constipation, diet) not addressed
Outcomes with Treatment
| Treatment | Healing Rate | Recurrence Rate | Time to Healing |
|---|---|---|---|
| Conservative (acute) | 50-60% | 30-40% if risk factors persist | 4-6 weeks |
| GTN 0.4% | 49-68% | 30-50% within 1 year | 6-8 weeks |
| Diltiazem 2% | 65-75% | 30-40% within 1 year | 6-8 weeks |
| Botulinum toxin | 65-85% | 40-50% within 2 years | 8-12 weeks |
| Lateral internal sphincterotomy | 95-98% | less than 5% | 6-8 weeks |
Exam Detail: Cochrane Review Summary (Nelson et al., 2012): [7]
GTN vs placebo: NNT = 8 (need to treat 8 patients to heal one additional fissure beyond placebo) Medical therapy (any) vs surgery: Surgery significantly more effective (OR 5.5, 95% CI 3.4-8.7) Clinical implication: Medical therapy is acceptable first-line but surgery should be offered for failures
Prognostic Factors
Good Prognosis:
- Acute fissure (first episode)
- Posterior midline location
- No previous fissure history
- Addresses constipation and dietary risk factors
- Good compliance with treatment
- No underlying inflammatory bowel disease
- Response to medical therapy
Poor Prognosis:
- Chronic fissure (> 6-8 weeks)
- Lateral or off-midline location (secondary cause likely)
- Recurrent fissures
- Underlying Crohn's disease (healing rates 50-60% even with optimal therapy)
- Immunosuppression (HIV, chemotherapy)
- Risk factors not addressed (persistent constipation)
- Failed medical therapy
- Previous failed surgery
Long-Term Outcomes
- Post-LIS: > 90% remain healed at 5 years with appropriate lifestyle maintenance [11]
- Incontinence post-LIS: Most minor incontinence resolves within 6-12 months; 2-3% have persistent symptoms
- Quality of life: Significant improvement post-treatment; surgical patients report highest satisfaction despite incontinence risk
10. Evidence and Guidelines
Key Clinical Practice Guidelines
-
American Society of Colon and Rectal Surgeons (ASCRS) Clinical Practice Guidelines: Management of Anal Fissure (2023 update) [1]
- Strong recommendation for conservative measures in all patients
- Strong recommendation for topical GTN or calcium channel blockers as first-line medical therapy for chronic fissure
- Strong recommendation for lateral internal sphincterotomy for medically refractory chronic fissure
- Conditional recommendation for botulinum toxin for patients at high risk of incontinence
-
Association of Coloproctology of Great Britain and Ireland (ACPGBI) [4]
- Stepwise management approach endorsed
- Emphasis on informed consent regarding incontinence with surgery
- Tailored sphincterotomy recommended
-
NICE Clinical Knowledge Summaries (CKS): Anal Fissure [19]
- Primary care guidance on diagnosis and initial conservative management
- Referral criteria for specialist care
Landmark Trials and Systematic Reviews
1. Cochrane Review: Non-surgical therapy for anal fissure (Nelson et al., 2012) [7]
- 75 RCTs, 5,031 participants
- GTN healed 48.9% vs 35.5% placebo (pless than 0.0009)
- All medical therapies less effective than surgery
- High recurrence rates with medical therapy
- Clinical Impact: Established that medical therapy is marginally better than placebo; surgery remains most effective
2. Meta-analysis: Botulinum toxin vs lateral sphincterotomy (Sajid et al., 2012) [18]
- LIS: 94.8% healing; Botox: 69.5% healing
- Recurrence higher with Botox (25% vs 2%)
- Similar incontinence rates
- Clinical Impact: LIS remains gold standard but Botox viable alternative
3. Randomised trial: GTN vs placebo (Lund & Scholefield, 1997) [16]
- First major RCT establishing GTN efficacy
- 68% healing with GTN vs 8% placebo
- Headache in 58% of GTN group
- Clinical Impact: Established chemical sphincterotomy concept
4. Systematic review: Diltiazem vs GTN (Brisinda et al., 2007) [17]
- Similar efficacy between agents
- Diltiazem better tolerated (fewer headaches)
- Clinical Impact: Diltiazem increasingly preferred first-line
Evidence Levels Summary
| Intervention | Level of Evidence | Recommendation Strength |
|---|---|---|
| Conservative measures (fibre, fluids) | Level IV (expert consensus) | Strong recommendation |
| GTN/Diltiazem for chronic fissure | Level 1a (meta-analysis of RCTs) | Strong recommendation |
| Botulinum toxin injection | Level 1b (RCTs) | Moderate recommendation |
| Lateral internal sphincterotomy | Level 1a (meta-analysis) | Strong recommendation for refractory cases |
| Tailored vs full sphincterotomy | Level 2 (cohort studies) | Conditional recommendation (tailored preferred) |
| Biopsy of non-healing fissure | Level V (expert opinion) | Strong recommendation |
11. Exam-Focused Content
Common Exam Questions
1. "What are the causes of anal fissure?"
Primary (Idiopathic):
- Constipation and hard stool passage (most common)
- Chronic diarrhoea (irritation)
- Childbirth (particularly traumatic/instrumental)
- Anal intercourse
- Previous anal surgery
Secondary (Suspect if lateral/multiple/atypical):
- Crohn's disease (most common secondary cause)
- Ulcerative colitis (less common than Crohn's)
- Tuberculosis
- HIV/AIDS
- Syphilis
- Anal carcinoma
- Leukaemia/lymphoma
- Chemotherapy/immunosuppression
2. "Describe the pathophysiology of chronic anal fissure."
Model Answer: "The pathophysiology centres on a self-perpetuating cycle of trauma, pain, sphincter spasm, and ischaemia.
Initial trauma from hard stool passage causes a tear in the anoderm, typically at the posterior midline. The posterior commissure is vulnerable because it represents a watershed zone with terminal blood supply from the inferior rectal artery, receiving up to 85% less perfusion than lateral quadrants.
The tear causes severe pain, which triggers reflex spasm of the internal anal sphincter. This results in elevated resting anal pressure—studies show pressures of 90-120 mmHg compared to normal values of 40-70 mmHg.
The sustained sphincter hypertonia compresses intramural blood vessels, causing ischaemia at the already poorly perfused fissure base. This hypoxic wound environment prevents healing, and the exposed wound is re-traumatised with each defecation.
A chronic fissure develops with characteristic features: a deep ulcer with exposed internal sphincter fibres, a sentinel pile (skin tag) at the external margin, and a hypertrophied anal papilla proximally. Breaking this cycle through pharmacological or surgical sphincter relaxation is the key to treatment."
3. "How would you manage a patient with chronic anal fissure refractory to medical therapy?"
Model Answer: "For a patient with chronic anal fissure refractory to 8-12 weeks of optimal medical therapy (topical GTN or diltiazem plus conservative measures), I would:
First, confirm the diagnosis and exclude secondary causes—I would examine to confirm the fissure is in a typical location and consider investigations for Crohn's disease, HIV, or malignancy if atypical features are present. A non-healing fissure should have biopsy to exclude carcinoma.
Second, discuss treatment options with the patient:
Option 1: Botulinum toxin injection
- Less invasive; can be performed in outpatient setting
- 65-85% healing rate
- Reversible; effect lasts 3-4 months
- Higher recurrence than surgery (40-50%)
- 5-10% temporary incontinence to flatus
- Particularly suitable for patients concerned about permanent incontinence
Option 2: Lateral internal sphincterotomy
- Gold standard surgery with 95-98% healing rate
- Low recurrence (less than 5%)
- Day case procedure
- Risk of minor incontinence (flatus, soiling) in 8-12%
- Risk of major incontinence in 1-3%
Pre-operative assessment would include detailed history (obstetric trauma, baseline continence), and I would consider endoanal ultrasound to assess sphincter integrity, particularly in women with obstetric history.
My recommendation for most patients would be lateral internal sphincterotomy given its superior efficacy and low recurrence. However, for patients at high risk of incontinence (multiparous women, prior sphincter injury, low resting pressure), I would offer botulinum toxin first.
I would counsel the patient thoroughly about the permanent incontinence risk with surgery and document informed consent."
Viva Points
Viva Point: Opening Statement: "Anal fissure is a longitudinal tear in the anoderm distal to the dentate line, most commonly occurring at the posterior midline due to the relatively ischaemic watershed blood supply in this region. It is one of the commonest anorectal conditions, affecting approximately 11% of the population, and is characterised by severe pain during defecation and bright red rectal bleeding."
Key Classification to State:
- Acute (less than 6 weeks) vs Chronic (> 6-8 weeks with sentinel pile, exposed sphincter fibres, hypertrophied papilla)
- Primary (posterior/anterior midline) vs Secondary (lateral, multiple—investigate for Crohn's, HIV, TB, malignancy)
Key Statistics to Cite:
- 85-90% posterior midline (Klosterhalfen studies show 85% reduced blood flow at posterior commissure)
- Medical therapy: 49-68% healing (GTN), 65-75% (diltiazem)
- Lateral internal sphincterotomy: 95-98% healing, less than 5% recurrence
- Incontinence risk post-LIS: 8-12% minor, 1-3% major
Key Evidence to Reference:
- Cochrane review (Nelson 2012): 75 RCTs, GTN marginally better than placebo, all medical therapy less effective than surgery
- ASCRS guidelines (2023): Stepwise approach, GTN/diltiazem first-line, LIS for failures
Common Mistakes to Avoid
❌ Mistakes that fail candidates:
- Missing secondary causes: Not investigating a lateral or atypical fissure for Crohn's disease or malignancy
- Recommending surgery first-line: Most examiners expect stepwise approach (conservative → medical → surgical)
- Not counselling about incontinence: Failure to mention permanent incontinence risk with sphincterotomy
- Confusing IAS and EAS: The procedure divides the internal (smooth muscle, involuntary) sphincter, not the external
- Wrong posterior commissure anatomy: The posterior midline is ischaemic because of reduced blood supply, not increased tension
- Performing posterior sphincterotomy: Modern practice uses lateral approach to avoid keyhole deformity
- Missing the diagnosis in atypical presentations: Painless fissures, multiple fissures, or off-midline fissures
- Not examining high-risk patients before surgery: Missing pre-existing sphincter injury that increases incontinence risk
Model Answers
Q: A 35-year-old woman presents with severe anal pain during defecation for 3 months. On examination, you see a fissure at the left lateral position. What is your approach?
A: "A lateral fissure is atypical and should be considered secondary until proven otherwise. My immediate concern would be Crohn's disease, which is the commonest cause of lateral fissures.
My approach would be:
History: I would ask about gastrointestinal symptoms (abdominal pain, diarrhoea, weight loss), extra-intestinal manifestations of IBD (arthralgia, skin rashes, mouth ulcers), and any family history of inflammatory bowel disease. I would also enquire about HIV risk factors, TB exposure, and sexual history.
Examination: I would examine the perianal area for other features of Crohn's (multiple skin tags, fistulae, abscess), perform an abdominal examination, and look for extra-intestinal manifestations.
Investigations: I would arrange inflammatory markers (FBC, CRP), faecal calprotectin, HIV serology, and refer for colonoscopy with biopsies to exclude Crohn's disease. If the fissure has atypical features (indurated edges), I would biopsy it to exclude malignancy.
Management: I would initiate conservative treatment for the fissure while investigations are undertaken. Definitive management would depend on the underlying cause. If Crohn's disease is confirmed, I would involve the IBD team, and sphincterotomy would generally be avoided due to high failure rates and risk of non-healing wounds."
12. Special Populations
Pregnancy and Postpartum
- Prevalence: Common during pregnancy (increased constipation) and postpartum (delivery trauma)
- Location: Anterior fissures more common in postpartum women (up to 40%)
- Management:
- "First-line: Conservative measures (fibre, fluids, stool softeners)"
- Topical lidocaine for analgesia
- GTN and diltiazem generally avoided in pregnancy (limited safety data); may consider in third trimester or postpartum if essential
- Surgery avoided during pregnancy unless emergency
- "Postpartum: Standard management pathway; consider sphincter assessment before surgery if instrumental/traumatic delivery"
Elderly Patients
- Considerations:
- Higher incontinence risk with surgery (age-related sphincter weakness)
- Pre-existing continence issues more common
- Lower tolerance of headache from GTN
- Polypharmacy considerations (nitrate interactions)
- Management:
- Favour conservative and medical management
- Botulinum toxin may be preferred over surgery if refractory
- If surgery required, consider more conservative/tailored sphincterotomy
- Pre-operative manometry to assess baseline function
Immunocompromised Patients
HIV/AIDS:
- Atypical presentations common; may be painless
- Healing correlates with immune status and viral control
- Optimise antiretroviral therapy
- Avoid surgery if CD4 less than 200 (poor healing)
- Consider opportunistic infections (CMV, HSV)—may need biopsy
Chemotherapy/Transplant:
- Poor healing during active immunosuppression
- High infection risk with surgery
- Conservative management preferred
- Timing of any surgery to coincide with immune recovery
Crohn's Disease
- Key Principle: Treat underlying Crohn's first
- Characteristics: Lateral/multiple fissures; associated fistulae; "elephant ear" skin tags
- Management:
- Medical therapy for Crohn's (immunomodulators, biologics)
- Conservative fissure management
- Avoid sphincterotomy (high failure rate 50%; risk of non-healing wound)
- Botulinum toxin may be considered if Crohn's controlled
- Often requires multidisciplinary approach with gastroenterology
13. Patient/Layperson Explanation
What is an Anal Fissure?
An anal fissure is a small tear or crack in the lining of the back passage (anus). It's a very common condition—about 1 in 10 people will experience one at some point in their lives. The tear usually happens when passing a hard or large stool. It causes intense pain during and after bowel movements, often described as "like passing broken glass," and you may notice small amounts of bright red blood on the toilet paper.
Why Does It Happen?
The tear usually occurs at the back of the anal opening, where the blood supply is naturally weaker. When the tear happens:
- It causes severe pain
- The muscle around the back passage goes into spasm to protect the area
- This spasm reduces blood flow even further
- The wound can't heal properly
- Each time you have a bowel movement, the wound opens again
This creates a vicious cycle. Common triggers include:
- Constipation and hard stools
- Straining on the toilet
- Pregnancy and childbirth
- Chronic diarrhoea
- Sometimes, underlying conditions like Crohn's disease
How is it Diagnosed?
Your doctor can usually diagnose an anal fissure simply by hearing your symptoms and gently examining the area. Often the tear can be seen by carefully separating the buttocks. Because of the pain, more invasive examinations may not be possible initially.
How is it Treated?
For new (acute) fissures (less than 6 weeks): Most heal with simple measures:
- Eating more fibre (fruits, vegetables, wholegrain foods)
- Drinking plenty of water (2-3 litres daily)
- Using stool softeners (Movicol, lactulose)
- Taking warm baths after bowel movements (sitz baths)
- Using pain relief before opening your bowels
For older (chronic) fissures (lasting more than 6-8 weeks): These usually need medication:
- Ointments (GTN or diltiazem) applied twice daily for 6-8 weeks
- These relax the muscle and improve blood flow to help healing
- About 6-7 out of 10 people heal with these treatments
If medications don't work:
- Botox injections into the muscle (temporary; 7-8 out of 10 heal)
- Surgery (lateral sphincterotomy) — the most effective option (over 95% heal)
What About Surgery?
Surgery involves making a small cut in the muscle around the back passage to relax it permanently. It's very effective but does carry a small risk (about 1 in 10) of affecting your ability to control wind, and a very small risk (1-2 in 100) of affecting your ability to control your bowels. Your surgeon will discuss this carefully with you before any operation.
When Should I Seek Medical Help?
See your doctor if:
- Pain is severe and not improving with home treatment
- Bleeding is heavy or persistent
- You notice a fissure in an unusual position (on the side rather than back)
- You have other symptoms like weight loss, fever, or a change in bowel habits
- You have Crohn's disease or are immunocompromised
- Symptoms are not improving after 6-8 weeks of treatment
What Can I Do to Prevent It Coming Back?
- Keep stools soft with a high-fibre diet (25-30g daily)
- Drink plenty of fluids
- Don't ignore the urge to have a bowel movement
- Don't strain or spend too long on the toilet
- Consider continued use of a stool softener if you're prone to constipation
14. References
Primary Guidelines
- Stewart DB Sr, Gaertner WB, Glasgow SC, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Anal Fissures. Dis Colon Rectum. 2023;66(2):190-199. doi:10.1097/DCR.0000000000002664 [PMID: 36538662]
Systematic Reviews and Meta-Analyses
-
Gerbasi L, Ashurst JV. Anal Fissures. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. [PMID: 30252319]
-
Mapel DW, Schum M, Von Worley A. The epidemiology and treatment of anal fissures in a population-based cohort. BMC Gastroenterol. 2014;14:129. doi:10.1186/1471-230X-14-129 [PMID: 25048612]
-
Cross KL, Massey EJ, Fowler AL, Monson JR; Association of Coloproctology of Great Britain and Ireland. The management of anal fissure: ACPGBI position statement. Colorectal Dis. 2008;10 Suppl 3:1-7. doi:10.1111/j.1463-1318.2008.01681.x [PMID: 18954306]
-
Klosterhalfen B, Vogel P, Rixen H, Mittermayer C. Topography of the inferior rectal artery: a possible cause of chronic, primary anal fissure. Dis Colon Rectum. 1989;32(1):43-52. doi:10.1007/BF02554724 [PMID: 2910661]
-
Schouten WR, Briel JW, Auwerda JJ. Relationship between anal pressure and anodermal blood flow. The vascular pathogenesis of anal fissures. Dis Colon Rectum. 1994;37(7):664-669. doi:10.1007/BF02054410 [PMID: 8026232]
-
Nelson RL, Thomas K, Morgan J, Jones A. Non-surgical therapy for anal fissure. Cochrane Database Syst Rev. 2012;2012(2):CD003431. doi:10.1002/14651858.CD003431.pub3 [PMID: 22336789]
-
Hananel N, Gordon PH. Lateral internal sphincterotomy for fissure-in-ano—revisited. Dis Colon Rectum. 1997;40(5):597-602. doi:10.1007/BF02055387 [PMID: 9152191]
-
D'Haens G, Baert F, van Assche G, et al. Crohn's disease-related anal fissures: effectiveness of treatment with adalimumab. Inflamm Bowel Dis. 2013;19(3):E45-46. doi:10.1002/ibd.22826 [PMID: 22848054]
-
Corby H, Donnelly VS, O'Herlihy C, O'Connell PR. Anal canal pressures are low in women with postpartum anal fissure. Br J Surg. 1997;84(1):86-88. doi:10.1002/bjs.1800840130 [PMID: 9043464]
-
Ebinger SM, Hardt J, Warschkow R, et al. Operative and medical treatment of chronic anal fissure—a review and network meta-analysis of randomized controlled trials. J Gastroenterol. 2017;52(6):663-676. doi:10.1007/s00535-017-1335-0 [PMID: 28365855]
-
Garg P, Garg M, Menon GR. Long-term continence disturbance after lateral internal sphincterotomy for chronic anal fissure: a systematic review and meta-analysis. Colorectal Dis. 2013;15(3):e104-117. doi:10.1111/codi.12108 [PMID: 23320551]
-
Scholefield JH, Bock JU, Marla B, et al. A dose finding study with 0.1%, 0.2%, and 0.4% glyceryl trinitrate ointment in patients with chronic anal fissures. Gut. 2003;52(2):264-269. doi:10.1136/gut.52.2.264 [PMID: 12524410]
-
Barrett WL, Callahan TD, Orkin BA. Perianal manifestations of human immunodeficiency virus infection: experience with 260 patients. Dis Colon Rectum. 1998;41(5):606-611. doi:10.1007/BF02235269 [PMID: 9593245]
-
Gibbons CP, Read NW. Anal hypertonia in fissures: cause or effect? Br J Surg. 1986;73(6):443-445. doi:10.1002/bjs.1800730609 [PMID: 3719268]
-
Lund JN, Scholefield JH. A randomised, prospective, double-blind, placebo-controlled trial of glyceryl trinitrate ointment in treatment of anal fissure. Lancet. 1997;349(9044):11-14. doi:10.1016/S0140-6736(96)06090-4 [PMID: 8988115]
-
Brisinda G, Cadeddu F, Brandara F, et al. Randomized clinical trial comparing botulinum toxin injections with 0.2 per cent nitroglycerin ointment for chronic anal fissure. Br J Surg. 2007;94(2):162-167. doi:10.1002/bjs.5514 [PMID: 17256808]
-
Sajid MS, Vijaynagar B, Desai M, et al. Botulinum toxin vs glyceryl trinitrate for the medical management of chronic anal fissure: a meta-analysis. Colorectal Dis. 2008;10(6):541-546. doi:10.1111/j.1463-1318.2007.01388.x [PMID: 17868492]
-
National Institute for Health and Care Excellence. Anal fissure. NICE Clinical Knowledge Summaries. 2020. https://cks.nice.org.uk/topics/anal-fissure/
-
Perry WB, Dykes SL, Buie WD, Rafferty JF; Standards Practice Task Force of the American Society of Colon and Rectal Surgeons. Practice parameters for the management of anal fissures (3rd revision). Dis Colon Rectum. 2010;53(8):1110-1115. doi:10.1007/DCR.0b013e3181e23f43 [PMID: 20628269]
Additional Resources
- Guts UK Charity: https://www.gutscharity.org.uk
- NHS: https://www.nhs.uk/conditions/anal-fissure/
- Patient.info: https://patient.info/digestive-health/anal-fissure-leaflet
Medical Disclaimer: MedVellum content is for educational purposes and clinical reference. Clinical decisions should account for individual patient circumstances. Always consult appropriate specialists. This content does not constitute medical advice for individual patients.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Anorectal Anatomy
- Constipation
Consequences
Complications and downstream problems to keep in mind.
- Anal Stenosis
- Faecal Incontinence