Acute Appendicitis
Acute appendicitis is the most common surgical emergency worldwide, with a lifetime risk of 7-8% and an incidence of app... MRCS exam preparation.
What matters first
Acute appendicitis is the most common surgical emergency worldwide, with a lifetime risk of 7-8% and an incidence of app... MRCS exam preparation.
Peritonitis (generalised guarding)
8 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Peritonitis (generalised guarding)
- Perforation
- Appendix mass/abscess
- Sepsis (fever, tachycardia, hypotension)
Exam focus
Current exam surfaces linked to this topic.
- MRCS
Linked comparisons
Differentials and adjacent topics worth opening next.
- Mesenteric Adenitis
- Ectopic Pregnancy
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Acute Appendicitis
1. Clinical Overview
Summary
Acute appendicitis is the most common surgical emergency worldwide, with a lifetime risk of 7-8% and an incidence of approximately 100 cases per 100,000 person-years. [1] It results from obstruction of the appendiceal lumen, leading to bacterial overgrowth, inflammation, and potential perforation if untreated. The classic presentation involves periumbilical pain migrating to the right iliac fossa (RIF), accompanied by anorexia, nausea, and fever. Diagnosis is primarily clinical, supported by scoring systems (Alvarado, AIR score) and imaging when uncertainty exists. Computed tomography (CT) demonstrates sensitivity and specificity exceeding 95% in adults, significantly reducing negative appendectomy rates. [2,3]
Appendicectomy remains the gold standard treatment, with laparoscopic approach preferred in most cases due to reduced wound infection rates, shorter hospital stay, and faster recovery. [4] Recent evidence from multiple randomised controlled trials, including the landmark CODA trial, demonstrates that antibiotic-only treatment can successfully manage uncomplicated appendicitis in selected patients, though recurrence rates of 25-30% within one year necessitate careful patient selection and shared decision-making. [5,6] Perforation risk increases significantly with diagnostic delay beyond 36-48 hours, particularly in elderly and paediatric populations. [7]
Key Facts
- Lifetime Risk: 7-8% overall; slightly higher in males (8.6%) than females (6.7%) [1]
- Peak Incidence: 10-30 years, with bimodal distribution (second peak in elderly)
- Classic Triad: RIF pain, anorexia, fever
- Pain Migration: Periumbilical → RIF over 6-24 hours (50-60% of cases)
- Diagnostic Accuracy: CT sensitivity 96-98%, specificity 95-96% [2,3]
- Treatment Gold Standard: Laparoscopic appendicectomy within 24 hours
- Perforation Rate: 20-30% at presentation; > 50% in children less than 5 and adults > 65 years [7,8]
- Negative Appendectomy: Historically 15-25%, reduced to less than 5% with routine CT imaging [9]
- Mortality: less than 0.1% (uncomplicated); 1-4% (perforated, elderly) [10]
Clinical Pearls
"Migration of Pain is Diagnostic": The classic periumbilical to RIF migration occurs as inflammation progresses from visceral peritoneum (vague, midline sensation via T10) to parietal peritoneum (sharp, localised sensation via somatic nerves). This occurs in 50-60% of patients and is highly specific when present.
"Anorexia is Almost Universal": Loss of appetite occurs in 90-95% of cases. A patient with RIF pain who is hungry and requests food is unlikely to have appendicitis—consider alternative diagnoses.
"CT When in Doubt": Liberal use of CT imaging reduces negative appendectomy rates from 15-25% to less than 5% without increasing perforation risk. The benefits of accurate diagnosis outweigh radiation concerns in the acute setting. [2,9]
"Perforation at Extremes": Children less than 5 years and elderly > 65 years have perforation rates exceeding 50% due to atypical presentations, diagnostic delay, and reduced physiological reserve. [7,8]
"Time is Tissue": While appendicitis is not a "midnight emergency," every hour of delay increases perforation risk by approximately 2%. Surgery should occur within 24 hours of diagnosis. [7]
"Alvarado ≥7 Predicts Appendicitis": Scores of 7-10 have 90% positive predictive value; scores 0-4 have 95% negative predictive value. Intermediate scores (5-6) require imaging. [11,12]
2. Epidemiology
Incidence and Prevalence
Acute appendicitis represents the most common abdominal surgical emergency globally, with approximately 250,000 appendectomies performed annually in the United States and 50,000 in the United Kingdom. [1] The condition demonstrates:
- Overall Incidence: 100 per 100,000 person-years in Western populations
- Lifetime Risk: 7-8% overall (males 8.6%, females 6.7%)
- Age-Specific Incidence: Peak at 10-30 years, with second smaller peak in elderly (> 60 years)
- Geographic Variation: Higher incidence in Western countries, lower in Asian and African populations
- Temporal Trends: Declining incidence in developed nations over past 30 years, attributed to dietary changes (increased fibre intake) [1]
Demographics
Age Distribution:
- Most common: 10-30 years (60% of cases)
- Children less than 2 years: Very rare (less than 1%)
- Elderly > 70 years: 5-10% of cases, but higher morbidity and mortality
- Median age at presentation: 22 years [1]
Sex Predilection:
- Male:Female ratio = 1.4:1 overall
- Ratio approaches 1:1 in children and elderly
- Higher male predominance in teenage years (M:F = 2:1)
Seasonal Variation:
- Slight summer peak reported in some studies
- No consistent seasonal pattern in most populations
Risk Factors
Established Risk Factors:
- Low-fibre diet: Associated with increased risk in epidemiological studies [1]
- Family history: First-degree relatives have 3-fold increased risk, suggesting genetic component
- Ethnicity: Higher in Caucasian populations, lower in Asian and African populations
- Cystic fibrosis: 1-2% lifetime risk of appendicitis
- Prior viral illness: Lymphoid hyperplasia following gastroenteritis increases risk in children
Protective Factors:
- High-fibre diet (increased stool bulk prevents obstruction)
- Rural residence (possibly related to dietary differences)
Debunked Myths:
- Seeds and nuts do NOT increase appendicitis risk (large cohort studies show no association)
- No association with constipation in isolation
Perforation Epidemiology
Overall Perforation Rates:
- At presentation: 20-30% of all cases
- Children less than 5 years: 50-70% (delayed diagnosis due to atypical presentation) [8]
- Adults > 65 years: 50-65% (atypical symptoms, diagnostic delay, comorbidities) [8]
- Pregnant women: 25-35% (diagnostic challenges)
Time-Dependent Perforation Risk:
- less than 12 hours from symptom onset: 10-15%
- 12-24 hours: 20-25%
- 24-36 hours: 30-40%
- 36-48 hours: 50-60%
-
48 hours: 70-80% [7]
Consequences of Perforation:
- Hospital stay increases from 1-2 days to 5-7 days
- Complication rate increases from 3% to 15-20%
- Mortality increases 10-fold (from less than 0.1% to 1-4%) [10]
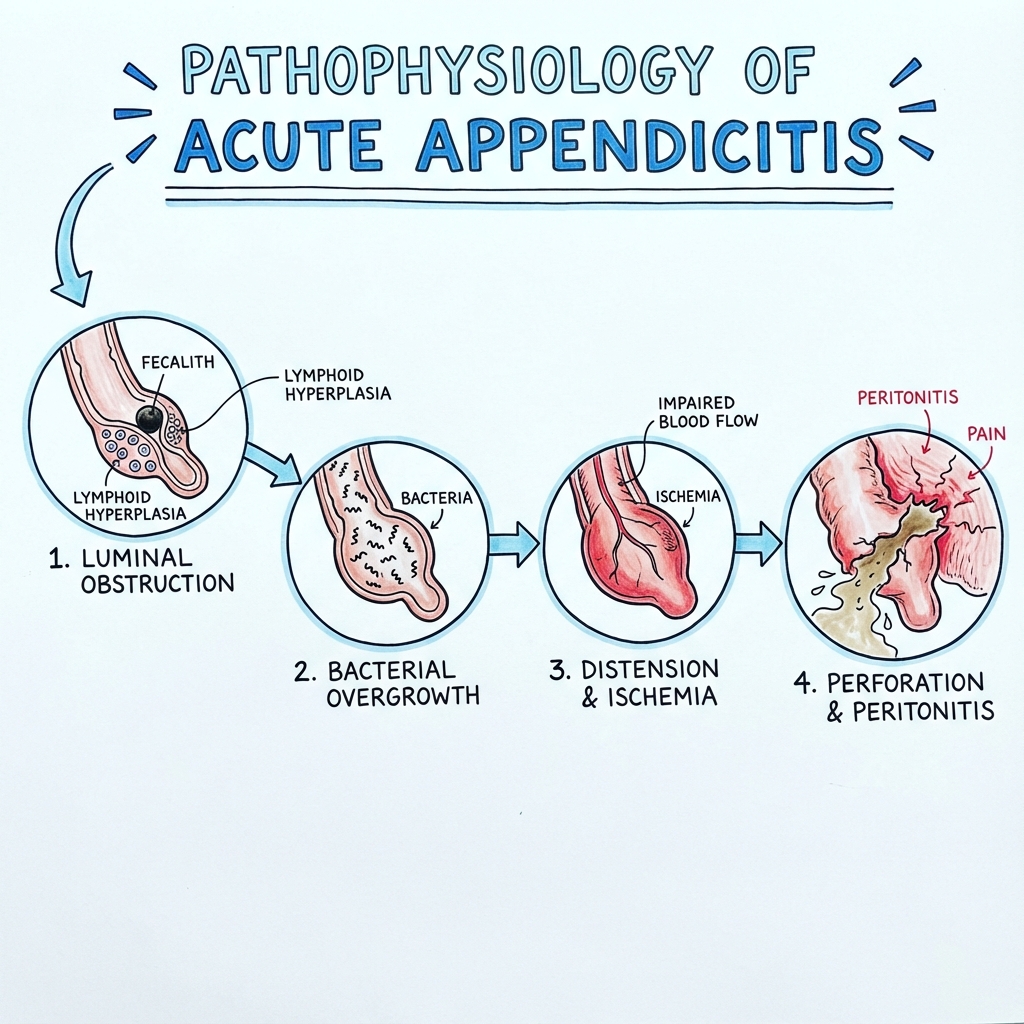
3. Pathophysiology
Molecular and Cellular Mechanisms
Acute appendicitis follows a predictable pathophysiological sequence initiated by luminal obstruction:
Stage 1: Luminal Obstruction
Primary Causes:
- Faecolith (30-40%): Inspissated faecal material calcified around vegetable matter
- Lymphoid hyperplasia (60% in children): Reactive follicular hyperplasia following viral infection (adenovirus, EBV, measles)
- Fibrous stricture (5%): Post-inflammatory scarring
- Neoplasm (less than 1%): Carcinoid tumour (most common), adenocarcinoma, lymphoma
- Parasites (rare): Enterobius vermicularis (pinworm), Ascaris
- Foreign body (rare): Seeds, fruit pips (despite myths, extremely uncommon)
Pathophysiological Consequence: Obstruction → Continued mucus secretion → Increased intraluminal pressure (normal 10 mmHg → 30-60 mmHg) → Venous and lymphatic obstruction
Stage 2: Vascular Compromise
Mechanism:
- Elevated pressure exceeds venous pressure (15-20 mmHg) → Venous congestion
- Oedema of appendiceal wall → Further pressure elevation
- Arterial supply compromised when pressure exceeds 60 mmHg
- Mucosal ischaemia develops within 6-12 hours
Inflammatory Response:
- Mucosal barrier breakdown → Bacterial translocation
- Neutrophil infiltration → Acute suppurative appendicitis
- Cytokine release (IL-1β, IL-6, TNF-α) → Systemic inflammatory response
Stage 3: Bacterial Overgrowth and Translocation
Microbiology:
- Polymicrobial infection reflecting colonic flora
- Aerobes: Escherichia coli (60-80%), Streptococcus species (40%)
- Anaerobes: Bacteroides fragilis (70%), Peptostreptococcus (50%)
- Other: Pseudomonas aeruginosa, Klebsiella species
Progression:
- Bacterial proliferation → Suppurative inflammation → Microabscesses
- Transmural inflammation → Serosal involvement → Peritoneal irritation (parietal peritonitis)
Stage 4: Gangrene and Perforation
Timeline:
- Gangrenous appendicitis: 24-48 hours after obstruction
- Perforation: 48-72 hours (earlier in extremes of age)
Perforation Patterns:
- Free perforation (30%): Spillage into peritoneal cavity → Generalised peritonitis
- Localised perforation (70%): Omental wrapping → Phlegmon or abscess formation
Complications Cascade:
Perforation
├── Free perforation → Generalised peritonitis → Septic shock
│
└── Walled-off perforation
├── Appendix mass (inflammatory phlegmon)
└── Appendix abscess (pus collection)
├── Pelvic abscess
├── Subphrenic abscess
└── Pylephlebitis (portal vein thrombophlebitis)
Why Pain Migrates: Neuroanatomical Explanation
Early Phase (Visceral Pain):
- Appendiceal distension stimulates stretch receptors
- Afferent fibres travel with sympathetic nerves (T8-T10)
- Sensory cortex interprets as poorly localised periumbilical pain
- Associated with autonomic symptoms (nausea, vomiting)
Late Phase (Somatic Pain):
- Transmural inflammation → Serosal irritation → Parietal peritoneum involvement
- Somatic nerve endings (intercostal nerves T10-L1) stimulated
- Sharp, well-localised RIF pain
- Aggravated by movement, coughing (peritoneal stretch)
Migration Time: Typically 6-24 hours, but can be as short as 2-4 hours in aggressive inflammation
Anatomical Variations and Clinical Implications
Appendix Position (affects symptom location):
- Retrocaecal (65%): Pain may be more lateral or posterior; less RIF tenderness; psoas irritation
- Pelvic (30%): Suprapubic pain; dysuria; diarrhoea; positive obturator sign
- Subcaecal (2.5%): Classic RIF presentation
- Pre-ileal/Post-ileal (1%): May mimic other pathology
- Paracaecal (0.5%): Variable presentation
Pregnancy-Related Changes:
- Appendix displaced superiorly and laterally
- First trimester: RIF pain (normal position)
- Second/Third trimester: Right upper quadrant or flank pain
- Diagnostic delay common due to atypical presentation
4. Clinical Presentation
Symptom Timeline and Evolution
Hour 0-6: Vague periumbilical or epigastric discomfort
- Dull, poorly localised visceral pain
- Anorexia develops (90% of patients)
- Nausea (60-80% of patients)
Hour 6-12: Pain migration begins
- Periumbilical pain becomes more constant
- RIF tenderness develops
- Vomiting (30-50%, typically after pain onset)
- Low-grade fever (37.5-38.5°C)
Hour 12-24: Localised RIF pain
- Sharp, well-defined RIF pain
- Aggravated by movement, coughing, walking
- Patient prefers to lie still with hips flexed
- Tenderness maximal at McBurney's point
Hour 24-48: Complications may develop
- Worsening fever (> 38.5°C suggests perforation)
- Diffuse abdominal pain (peritonitis)
- Toxicity, tachycardia, hypotension (sepsis)
Classical Symptoms
| Symptom | Frequency | Characteristics | Clinical Significance |
|---|---|---|---|
| Abdominal pain | 95-100% | Initially periumbilical, migrates to RIF | Universal, but pattern varies |
| Anorexia | 90-95% | Complete loss of appetite | Absence argues against diagnosis |
| Nausea | 60-80% | Usually follows pain onset | Typically precedes vomiting |
| Vomiting | 30-50% | 1-2 episodes, after pain starts | Excessive vomiting suggests other diagnosis |
| Fever | 70-80% | Low-grade (37.5-38.5°C) | High fever (> 39°C) suggests perforation |
| Change in bowel habit | 10-20% | Usually constipation, occasionally diarrhoea | Diarrhoea more common with pelvic appendix |
| Dysuria | 10-15% | Bladder irritation from adjacent inflammation | More common with pelvic appendix |
Atypical Presentations
Anatomical Variations:
| Appendix Position | Clinical Features | Examination Findings |
|---|---|---|
| Retrocaecal (65%) | Back/flank pain; less RIF tenderness; minimal guarding | Positive psoas sign; tenderness more lateral |
| Pelvic (30%) | Suprapubic pain; diarrhoea; urinary frequency; rectal discomfort | Positive obturator sign; tenderness on PR/PV exam |
| Subcaecal (2.5%) | Classic RIF presentation | Tenderness at McBurney's point |
| Paracaecal (0.5%) | Variable, may mimic mesenteric adenitis | Less specific findings |
Age-Related Variations:
Children (less than 5 years):
- Diffuse abdominal pain rather than localised RIF pain
- Higher fever (> 38.5°C) more common
- Vomiting and diarrhoea prominent
- Perforation rate 50-70% due to delayed diagnosis [8]
- Non-specific symptoms often attributed to gastroenteritis
Elderly (> 65 years):
- Vague abdominal discomfort, minimal pain
- Less pronounced fever and tachycardia
- Minimal peritoneal signs despite advanced disease
- Higher perforation rate (50-65%) due to delayed presentation [8]
- Increased mortality (1-4% vs less than 0.1% in young adults) [10]
Pregnancy:
- First trimester: Classic RIF presentation
- Second trimester: Pain migrates to right flank
- Third trimester: Right upper quadrant pain (appendix displaced by gravid uterus)
- Nausea/vomiting difficult to distinguish from normal pregnancy
- Physiological leucocytosis confounds laboratory diagnosis
- Perforation rate 25-35% (diagnostic challenges)
- Fetal loss risk: 1.5% (uncomplicated) vs 20-35% (perforated) [13]
Immunocompromised Patients:
- Blunted inflammatory response
- Minimal fever and leucocytosis
- Less peritoneal irritation despite advanced disease
- Higher perforation rate and mortality
Red Flag Symptoms
Immediate Surgical Consultation Required:
- Diffuse abdominal tenderness with rigidity (generalised peritonitis)
- Haemodynamic instability (tachycardia > 110, hypotension, altered mental status)
- Severe pain out of proportion to examination (consider mesenteric ischaemia)
- Bilious vomiting (consider bowel obstruction)
- Pulsatile abdominal mass (consider AAA)
- Vaginal bleeding in reproductive-age women (consider ectopic pregnancy)
5. Clinical Examination
Systematic Approach
General Inspection
- Patient position: Lying still, hips and knees flexed (peritoneal irritation)
- Movement: Reluctant to move; pain worse with coughing, walking
- Facial expression: Grimacing on movement
- Hydration status: Dry mucous membranes, reduced skin turgor (dehydration)
Vital Signs
| Parameter | Uncomplicated | Complicated/Perforated |
|---|---|---|
| Temperature | 37.5-38.5°C | > 38.5°C (often > 39°C) |
| Heart rate | 80-100 bpm | > 100 bpm (tachycardia) |
| Blood pressure | Normal | May be low (septic shock) |
| Respiratory rate | Normal | > 20/min (sepsis, pain) |
| Oxygen saturation | > 95% | May be reduced (sepsis, ARDS) |
Abdominal Examination
Inspection:
- Previous scars (important for surgical planning)
- Abdominal distension (suggests perforation with ileus)
- Respiratory movement: Reduced in RIF (splinting)
Palpation:
| Sign | Method | Positive Finding | Significance |
|---|---|---|---|
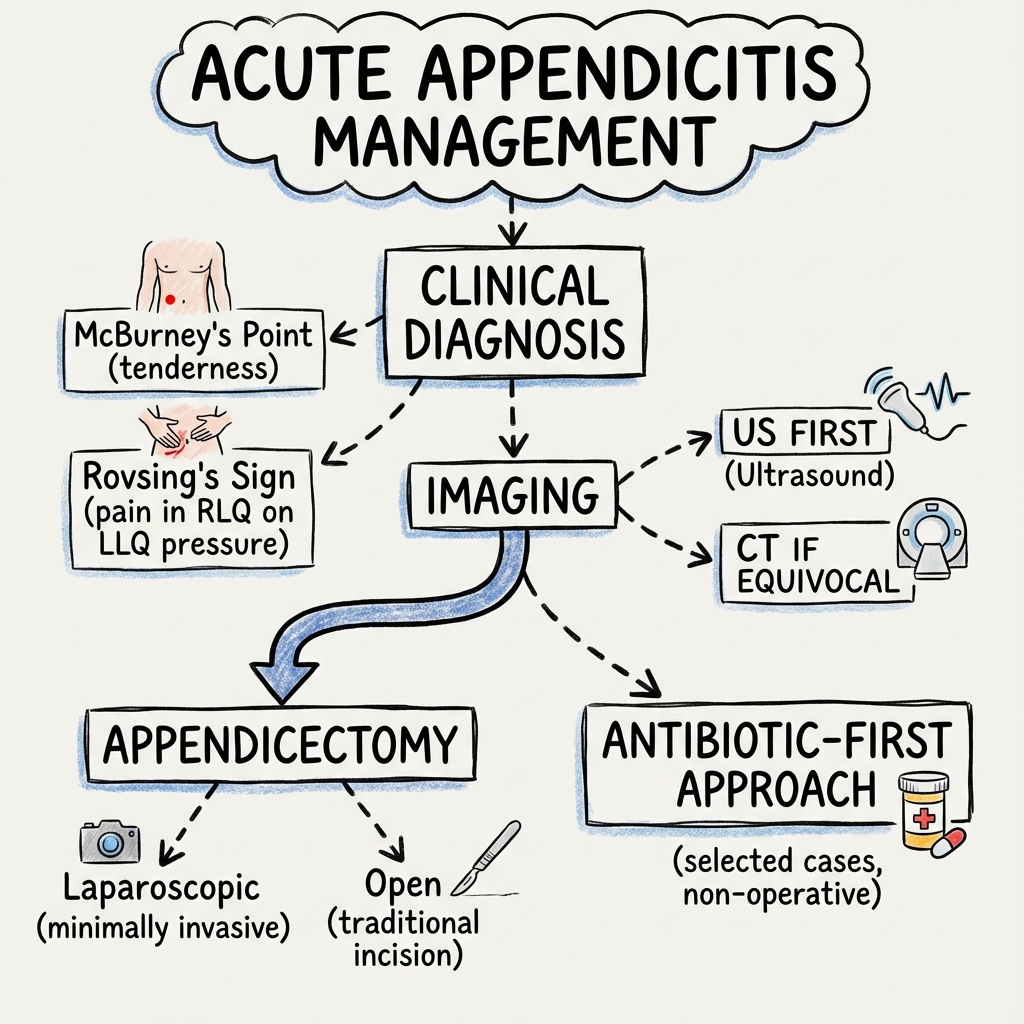
| McBurney's point | Palpate 1/3 distance ASIS to umbilicus | Maximal tenderness | Most reliable sign (80-90% sensitivity) [11] |
| Rovsing's sign | Palpate LIF, release pressure | Pain referred to RIF | Peritoneal inflammation (40-60% sensitivity) |
| Blumberg's sign | Deep palpation RIF, sudden release | Rebound pain | Peritonitis (sensitivity 60-80%) |
| Guarding | Gentle palpation | Voluntary/involuntary muscle spasm | Involuntary guarding = peritonitis |
| Rigidity | Assess muscle tone | Board-like abdomen | Generalised peritonitis (surgical emergency) |
| Appendix mass | Deep palpation RIF | Firm, tender mass | Walled-off perforation (5-10% of cases) |
Special Tests:
| Test | Method | Positive Result | Clinical Implication |
|---|---|---|---|
| Psoas sign | Hip extension against resistance (right side) | RIF pain | Retrocaecal appendix (irritation of iliopsoas) |
| Obturator sign | Internal rotation of flexed right hip | Hypogastric pain | Pelvic appendix (obturator internus irritation) |
| Dunphy's sign | Ask patient to cough | Sharp RIF pain | Peritoneal irritation (highly specific) |
| Ten sign | Light percussion over RIF | Localised pain | Alternative to rebound testing (less painful) |
Percussion:
- Tenderness on percussion over RIF (peritoneal irritation)
- Loss of liver dullness (free air if perforated—rare)
Auscultation:
- Bowel sounds usually normal or mildly reduced initially
- Absent bowel sounds suggest perforation with ileus
Rectal and Pelvic Examination
Rectal Examination (PR):
- Indications: Suspected pelvic appendix, equivocal abdominal findings, elderly patients
- Findings: Right-sided tenderness (pelvic appendix); mass (pelvic abscess)
- Utility: Limited sensitivity (30-40%), but can identify pelvic pathology
Pelvic Examination (PV):
- Essential in women of reproductive age to exclude gynaecological pathology
- Findings: Cervical excitation tenderness (PID, ectopic pregnancy); adnexal mass (ovarian cyst/torsion)
Clinical Scoring Systems
Alvarado Score (MANTRELS Mnemonic)
| Feature | Points |
|---|---|
| Migration of pain (periumbilical → RIF) | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| Tenderness RIF | 2 |
| Rebound tenderness | 1 |
| Elevated temperature (> 37.5°C) | 1 |
| Leukocytosis (WCC > 10 × 10⁹/L) | 2 |
| Shift to left (neutrophilia > 75%) | 1 |
| Total | 10 |
Interpretation:
- 0-4 points: Low probability (5-10%); consider discharge with safety-netting
- 5-6 points: Intermediate probability (30-40%); imaging recommended
- 7-10 points: High probability (80-95%); surgical consultation ± imaging [11,12]
Performance:
- Sensitivity: 81-85%
- Specificity: 75-80%
- Best validated in adults; less accurate in children and elderly
AIR Score (Appendicitis Inflammatory Response)
| Variable | Finding | Points |
|---|---|---|
| Vomiting | Present | 1 |
| RIF pain | Present | 1 |
| Rebound/guarding | Light | 1 |
| Medium | 2 | |
| Strong | 3 | |
| Temperature | ≥38.5°C | 1 |
| WCC | 10-14.9 × 10⁹/L | 1 |
| ≥15 × 10⁹/L | 2 | |
| Polymorphonuclear % | 70-84% | 1 |
| ≥85% | 2 | |
| CRP | 10-49 mg/L | 1 |
| ≥50 mg/L | 2 | |
| Total | 12 |
Interpretation:
- 0-4 points: Low probability (10%); discharge with follow-up
- 5-8 points: Intermediate (30-70%); imaging or observation
- 9-12 points: High probability (90%); surgery ± imaging [12]
Performance:
- Sensitivity: 85-90%
- Specificity: 80-85%
- Slightly superior to Alvarado in some studies, particularly in identifying low-risk patients [12]
RIPASA Score (Raja Isteri Pengiran Anak Saleha Appendicitis)
Developed for Asian populations; includes additional demographic factors. Demonstrated superior performance in Asian studies but not consistently superior in Western populations. [12]
6. Investigations
Laboratory Tests
Essential Blood Tests
| Test | Typical Finding | Clinical Utility | Limitations |
|---|---|---|---|
| WCC | 10-18 × 10⁹/L | Elevated in 80-85% | Normal WCC does not exclude diagnosis |
| Neutrophilia | > 75% neutrophils | Left shift indicates bacterial infection | Non-specific |
| CRP | > 10 mg/L (often 50-150) | More useful if symptoms > 12h | Delayed rise (6-12h) |
| U&E | Variable | Assess dehydration, pre-operative renal function | Not diagnostic |
| Pregnancy test | MANDATORY in all females of reproductive age | Excludes ectopic pregnancy | False negatives rare but possible |
| Lactate | Elevated if septic | Marker of tissue hypoperfusion/sepsis | Non-specific |
| LFTs | Usually normal | Exclude biliary pathology | Mildly elevated in severe inflammation |
Important Nuances:
- Normal WCC: Present in 10-20% of appendicitis cases; does NOT exclude diagnosis
- Very high WCC (> 18 × 10⁹/L): Suggests perforation or abscess formation
- CRP timing: Rises 6-12 hours after symptom onset; more useful in delayed presentations
- Pregnancy test: Essential even in patients denying sexual activity (unreliable history)
Specialised Tests (Selected Cases)
- Urinalysis: Exclude UTI; mild pyuria (5-10 WBC) can occur with pelvic appendicitis due to bladder irritation
- Blood cultures: If septic (perforation suspected)
- Amylase/lipase: If upper abdominal pain (exclude pancreatitis)
Imaging Modalities
Computed Tomography (CT) - Gold Standard in Adults
Indications:
- Diagnostic uncertainty (intermediate Alvarado/AIR score)
- Atypical presentation
- Elderly patients (high perforation risk)
- Obese patients (difficult clinical examination)
- Known alternative pathology requiring exclusion
Protocol:
- Contrast-enhanced CT abdomen/pelvis (IV contrast ± oral contrast)
- Oral contrast traditionally used but not essential (modern protocols often IV contrast only)
- Rectal contrast may improve visualisation of pelvic appendix
CT Findings of Acute Appendicitis:
| Finding | Sensitivity | Description |
|---|---|---|
| Appendiceal diameter > 6-7mm | 95% | Measured in axial plane, outer wall to outer wall |
| Appendiceal wall thickening | 85% | Wall > 2-3mm |
| Periappendiceal fat stranding | 90% | Hazy increased attenuation in surrounding fat |
| Appendicolith | 25-30% | Calcified faecolith (highly specific when present) |
| Appendiceal wall enhancement | 85% | After IV contrast administration |
| Free fluid | 40-60% | Small amount in RIF, pelvis |
| Abscess formation | 10-20% | Rim-enhancing fluid collection |
| Phlegmon | 5-10% | Inflammatory mass without organised abscess |
Perforation Indicators:
- Focal defect in appendiceal wall
- Periappendiceal abscess or free air
- Extraluminal appendicolith
- Diffuse peritoneal free fluid
Performance Metrics:
- Sensitivity: 95-98% [2,3]
- Specificity: 95-96% [2,3]
- Negative predictive value: > 98%
- Positive predictive value: 92-95%
Advantages:
- Highest diagnostic accuracy
- Identifies alternative diagnoses (diverticulitis, renal colic, malignancy)
- Assesses extent of disease (perforation, abscess)
- Guides intervention (drainage of abscess)
Disadvantages:
- Radiation exposure (effective dose 10-15 mSv)
- Contrast allergy/nephrotoxicity risk
- Cost
- Not suitable for pregnancy
Impact on Outcomes:
- Reduces negative appendectomy rate from 15-25% to less than 5% [9]
- Does NOT increase perforation rate despite diagnostic delay (1-2 hours for imaging)
- Reduces overall hospital costs by avoiding unnecessary surgery
Ultrasound (US)
Indications:
- First-line in:
- Children (less than 15 years)
- Pregnant women (first/second trimester)
- Young women of reproductive age (avoid radiation)
- Alternative if CT contraindicated (renal impairment, contrast allergy)
Protocol:
- Graded compression technique
- High-frequency linear probe (5-12 MHz)
- Focused RIF examination
- Pelvic transabdominal/transvaginal views if indicated
US Findings:
- Non-compressible, blind-ending tubular structure > 6mm diameter
- Hyperechoic periappendiceal fat (inflammation)
- Appendicolith with posterior acoustic shadowing
- Increased vascularity on Doppler
- Free fluid in RIF/pelvis
Performance Metrics:
- Sensitivity: 70-85% (operator-dependent) [14]
- Specificity: 85-95%
- Limitation: Obesity, bowel gas, retrocaecal appendix reduce visualisation
Advantages:
- No radiation
- No contrast required
- Bedside availability (in some centres)
- Can identify gynaecological pathology
Disadvantages:
- Operator-dependent
- Lower sensitivity than CT
- Non-diagnostic in 20-30% (appendix not visualised)
- Poor negative predictive value
Recommendation: If US non-diagnostic or negative but high clinical suspicion → Proceed to CT or MRI
Magnetic Resonance Imaging (MRI)
Indications:
- Pregnancy (all trimesters, especially second/third)
- High clinical suspicion with non-diagnostic ultrasound
- Paediatric patients when US inadequate and radiation avoidance desired
- Contraindication to CT contrast
Protocol:
- T2-weighted sequences (inflammation appears bright)
- Diffusion-weighted imaging (DWI) sequences
- No gadolinium contrast required (safe in pregnancy)
MRI Findings:
- Appendix diameter > 7mm
- Periappendiceal fluid and oedema (T2 hyperintense)
- Restricted diffusion (high signal on DWI)
- Appendicolith (T2 hypointense)
Performance Metrics:
- Sensitivity: 90-97% [13,14]
- Specificity: 95-98%
- Comparable to CT in experienced centres
Advantages:
- No ionising radiation
- No contrast nephrotoxicity
- Excellent soft tissue contrast
- Safe in pregnancy
Disadvantages:
- Limited availability (especially out of hours)
- Longer acquisition time (20-30 minutes)
- Higher cost
- Claustrophobia
- Less familiar to surgeons
Imaging Algorithm
Clinical Suspicion of Appendicitis
↓
┌───────┴──────────────────────────┐
│ High Clinical Suspicion │
│ (Alvarado ≥7, AIR ≥9) │
│ │
│ → Surgical consultation │
│ → Imaging optional (surgeon │
│ discretion) │
│ → Proceed to appendectomy if │
│ diagnosis certain clinically │
└───────────────────────────────────┘
┌───────────────────────────────────┐
│ Intermediate Suspicion │
│ (Alvarado 5-6, AIR 5-8) │
│ │
│ → IMAGING MANDATORY │
│ ├─ Adults: CT (1st line) │
│ ├─ Children: US → CT/MRI │
│ ├─ Pregnancy: US → MRI │
│ └─ Young women: US → CT/MRI │
└───────────────────────────────────┘
┌───────────────────────────────────┐
│ Low Clinical Suspicion │
│ (Alvarado 0-4, AIR 0-4) │
│ │
│ → Discharge with safety-netting │
│ → Return if worsening symptoms │
│ → Consider alternative diagnosis │
└───────────────────────────────────┘
7. Differential Diagnosis
Acute appendicitis can mimic numerous intra-abdominal and extra-abdominal conditions. A systematic approach is essential:
Gastrointestinal Causes
| Diagnosis | Distinguishing Features | Key Investigations |
|---|---|---|
| Mesenteric adenitis | Viral prodrome; diffuse/central pain; mobile tenderness; children | US: enlarged mesenteric lymph nodes; CT if doubt |
| Acute gastroenteritis | Diarrhoea precedes pain; nausea/vomiting prominent; no localisation | Stool culture; usually clinical diagnosis |
| Crohn's disease (terminal ileitis) | Chronic history; mouth ulcers; perianal disease; weight loss | CT: terminal ileum thickening; colonoscopy |
| Meckel's diverticulitis | Indistinguishable from appendicitis; may have GI bleeding history | CT: inflamed diverticulum in RIF; often diagnosed intraoperatively |
| Caecal diverticulitis | Older patients; may have known diverticular disease | CT: diverticulum with pericolonic inflammation |
| Right-sided diverticulitis | More common in Asian populations; older age | CT: colonic diverticula with inflammation |
| Inflammatory bowel disease | Chronic symptoms; bloody diarrhoea; extraintestinal manifestations | CT/MRI enterography; colonoscopy |
| Perforated peptic ulcer | Sudden onset; epigastric pain; peritonitis; upper GI history | Erect CXR: free air; CT confirms |
Gynaecological Causes (Women of Reproductive Age)
| Diagnosis | Distinguishing Features | Key Investigations |
|---|---|---|
| Ectopic pregnancy | Amenorrhoea; vaginal bleeding; shoulder tip pain; haemodynamic instability | β-hCG mandatory; TVUS; culdocentesis |
| Ovarian torsion | Sudden severe pain; nausea/vomiting; adnexal mass on exam | TVUS with Doppler: enlarged ovary, absent flow |
| Ruptured ovarian cyst | Mid-cycle pain; sudden onset; haemodynamic instability if haemorrhagic | TVUS: free fluid; CT if doubt |
| Pelvic inflammatory disease (PID) | Bilateral lower abdominal pain; vaginal discharge; cervical excitation | Pelvic exam: bilateral tenderness; high vaginal swab |
| Mittelschmerz | Mid-cycle pain (ovulation); self-limiting; recurrent history | Clinical diagnosis; TVUS shows follicular cyst |
| Endometriosis | Chronic cyclical pain; dysmenorrhoea; dyspareunia; infertility | Laparoscopy (gold standard); MRI |
| Tubo-ovarian abscess | High fever; toxic; bilateral tenderness; risk factors for PID | TVUS/CT: complex adnexal mass; blood cultures |
Urological Causes
| Diagnosis | Distinguishing Features | Key Investigations |
|---|---|---|
| Urinary tract infection/pyelonephritis | Dysuria; frequency; urgency; loin pain; suprapubic tenderness | Urinalysis: pyuria, bacteriuria; urine culture |
| Renal/ureteric calculus | Severe colicky loin-to-groin pain; haematuria; restless patient | Non-contrast CT: stone; US: hydronephrosis |
| Testicular torsion (males) | Acute scrotal pain; nausea; tender high-riding testis; absent cremasteric reflex | EMERGENCY: Doppler US; surgical exploration |
Other Causes
| Diagnosis | Distinguishing Features | Key Investigations |
|---|---|---|
| Rectus sheath haematoma | Anticoagulation; trauma; pain worse with abdominal wall contraction | CT: haematoma in rectus sheath |
| Epiploic appendagitis | Localised sharp pain; no systemic upset; self-limiting | CT: fatty lesion with inflammatory changes |
| Abdominal wall pain (myofascial) | Reproducible with palpation; Carnett's sign positive | Clinical diagnosis |
| Primary peritonitis (children) | Nephrotic syndrome; ascites; diffuse peritonitis without source | Paracentesis: neutrophils; culture |
| Pneumonia (right lower lobe) | Cough; pleuritic chest pain; respiratory signs | CXR: infiltrate; CT if abdominal signs prominent |
| Diabetic ketoacidosis | Abdominal pain; nausea/vomiting; polyuria; hyperglycaemia | ABG: metabolic acidosis; glucose; ketones |
| Henoch-Schönlein purpura (children) | Purpuric rash; arthralgia; abdominal colic; haematuria | Clinical diagnosis; biopsy if doubt |
| Intussusception (children) | Intermittent colicky pain; bloody stool ("redcurrant jelly"); sausage-shaped mass | US: target sign; contrast enema diagnostic and therapeutic |
Critical "Can't Miss" Diagnoses
- Ectopic pregnancy: Always check β-hCG in reproductive-age women
- Testicular torsion: Examine external genitalia in males
- Ruptured AAA: Pulsatile mass, hypotension, elderly
- Mesenteric ischaemia: Pain out of proportion to exam, AF, elderly
- Perforated viscus: Diffuse peritonitis, free air on imaging
8. Management
Initial Resuscitation and Stabilisation
All Patients:
- IV access: Large-bore cannula (16-18G)
- IV fluids: Crystalloid resuscitation (Hartmann's or 0.9% NaCl)
- Correct dehydration: 20-30 mL/kg bolus if signs of depletion
- Maintenance: 100-125 mL/h in adults
- Analgesia: Do NOT withhold—does not mask clinical signs [15]
- Paracetamol 1g IV/PO QDS
- NSAIDs (ibuprofen 400mg PO TDS or ketorolac 10-30mg IV) if not contraindicated
- Opioids (morphine 5-10mg IV or oxycodone 5-10mg PO) for severe pain
- Antiemetics: Ondansetron 4-8mg IV or metoclopramide 10mg IV
- NBM (nil by mouth): If surgery planned
- VTE prophrophylaxis: LMWH (enoxaparin 40mg SC daily) unless contraindicated
Septic Patients (perforation, generalised peritonitis):
- Sepsis bundle: IV fluid resuscitation, blood cultures, early antibiotics
- Consider ICU/HDU involvement
- Urinary catheter for monitoring (fluid balance)
- Lactate monitoring
Antibiotic Therapy
Prophylactic Antibiotics (Pre-Operative)
Indication: All patients undergoing appendectomy
Regimen (single pre-operative dose):
- Cefuroxime 1.5g IV + Metronidazole 500mg IV
- Alternative: Co-amoxiclav 1.2g IV
- Penicillin allergy: Gentamicin 5mg/kg IV + Metronidazole 500mg IV
Timing: Within 60 minutes of skin incision
Evidence: Reduces surgical site infection from 15-20% to 3-5% [16]
Therapeutic Antibiotics
Indications:
- Perforated appendicitis
- Gangrenous appendicitis
- Appendix mass/abscess
- Generalised peritonitis
- Conservative (non-operative) management
Regimen (empirical, broad-spectrum):
- Piperacillin-tazobactam 4.5g IV TDS (covers aerobes + anaerobes)
- Alternative: Cefuroxime 1.5g IV TDS + Metronidazole 500mg IV TDS
- Penicillin allergy: Ciprofloxacin 400mg IV BD + Metronidazole 500mg IV TDS
- Severe sepsis: Add Gentamicin 5-7mg/kg IV OD
Duration:
- Uncomplicated (if conservative management chosen): 7-10 days
- Perforated without abscess: 5-7 days (post-operative)
- Abscess: 10-14 days ± drainage
- De-escalate based on clinical response and cultures
Surgical Management
Indications for Surgery
Absolute Indications:
- Clinical/radiological diagnosis of acute appendicitis (standard approach)
- Perforated appendicitis with peritonitis
- Failed conservative management
Relative Indications:
- Appendix mass (interval appendectomy debated—see below)
- Patient preference (after discussion of conservative option)
Timing of Surgery
Evidence-Based Recommendations:
- Within 24 hours of diagnosis: Standard practice [1]
- NOT a midnight emergency: Can safely wait until next morning if stable [17]
- Every hour delay: 2% increase in perforation risk (thus avoid prolonged delay) [7]
- Optimal window: 6-12 hours balances theatre efficiency with perforation risk
Delay is Acceptable If:
- Patient stable
- No peritonitis
- Adequate analgesia achieved
- Senior surgical review completed
Laparoscopic vs Open Appendectomy
Laparoscopic Appendectomy (Preferred):
Technique:
- Three ports (umbilical, suprapubic, left lower quadrant)
- Identification of appendix via caecum
- Mesoappendix division (LigaSure, clips, or staplers)
- Appendix stump management: stapler or endoloop ligation
- Specimen retrieval in bag
- Peritoneal lavage if contaminated
Advantages (vs open): [4,18]
- Reduced wound infection: OR 0.43 (57% reduction)
- Shorter hospital stay: 0.5-1 day reduction
- Less post-operative pain: Lower opioid requirements
- Faster return to normal activity: 1-2 weeks vs 3-4 weeks
- Better cosmesis: Three small scars vs larger RIF incision
- Diagnostic advantage: Ability to inspect entire abdomen
Disadvantages:
- Longer operative time (10-15 minutes)
- Higher equipment cost
- Steeper learning curve
- Contraindications (see below)
Open Appendectomy (Gridiron or Lanz Incision):
Indications:
- Extensive peritonitis (may require lavage)
- Appendix mass (difficult dissection)
- Haemodynamic instability
- Contraindication to pneumoperitoneum (severe cardiorespiratory disease)
- Pregnancy (third trimester—relative)
- Previous extensive abdominal surgery
- Conversion from laparoscopic (5-10% conversion rate)
- Surgeon preference/experience
Technique:
- RIF incision (Gridiron: muscle-splitting; Lanz: transverse)
- Identify appendix via taeniae coli on caecum
- Divide mesoappendix and appendix base
- Ligate or staple stump
- Close in layers
Cochrane Meta-Analysis Findings (laparoscopic vs open): [4]
- Wound infection: OR 0.43 (95% CI 0.34-0.54) favouring laparoscopic
- Intra-abdominal abscess: OR 1.87 (95% CI 1.35-2.59) slightly higher with laparoscopic
- Overall complications: No significant difference
- Hospital stay: 0.9 days shorter (95% CI 0.5-1.2) with laparoscopic
- Pain: Lower in laparoscopic group
- Return to activity: 5 days faster (95% CI 3-7 days) with laparoscopic
Current Practice: Laparoscopic approach in 70-80% of cases in Western centres [18]
Special Scenarios
Appendix Mass (Phlegmon):
-
Definition: Palpable RIF mass; CT shows inflammatory phlegmon without organised abscess
-
Management Options:
- Conservative (Ochsner-Sherren regimen): IV antibiotics, NBM, observation
- Success rate: 80-90%
- Interval appendectomy at 6-12 weeks (debated)
- Immediate surgery: If mass small, early presentation (less than 3 days), patient deteriorating
- Higher morbidity (30% vs 10% conservative)
- May require ileocaecal resection if extensive inflammation
- Conservative (Ochsner-Sherren regimen): IV antibiotics, NBM, observation
-
Interval Appendectomy Debate:
- Historically recommended after conservative management
- "Recent evidence: 10-20% recurrence if no interval surgery vs 0% if performed"
- "Pathology (malignancy): Found in 1-5% (higher in > 40 years)"
- "Current consensus: Offer interval appendectomy; mandatory if > 40 years (malignancy risk); colonoscopy if mass persists"
Appendix Abscess:
- Management: Percutaneous CT-guided drainage + IV antibiotics
- Drainage if > 5cm or not responding to antibiotics alone
- "Success rate: 70-90%"
- Interval appendectomy: Similar debate as above
Pregnancy:
- Laparoscopic safe in first and second trimester [13]
- Third trimester: Open approach often preferred (uterine size limits access)
- Maternal mortality less than 1%; fetal loss 1.5% (uncomplicated) to 20-35% (perforated) [13]
Elderly:
- Higher perforation rate (50-65%) [8]
- Higher morbidity and mortality (1-4%) [10]
- Aggressive imaging and early surgery recommended
Paediatrics:
- Laparoscopic preferred (lower wound infection, faster recovery)
- Higher perforation rate in less than 5 years (50-70%) [8]
- US first-line, then CT/MRI if non-diagnostic
Intra-Operative Findings and Management
Normal Appendix:
- Frequency: 5-10% (with routine CT); 15-25% (clinical diagnosis alone)
- Management:
- Remove appendix anyway (prevents future diagnostic confusion)
- Inspect entire abdomen: terminal ileum (Crohn's), Meckel's diverticulum, ovaries/fallopian tubes, colon
- Document findings thoroughly
Appendiceal Neoplasm (1-2% of appendectomies):
- Carcinoid tumour (most common): If less than 1cm at base, appendectomy sufficient; if > 2cm or involving base, right hemicolectomy
- Mucinous cystadenoma/adenocarcinoma: Right hemicolectomy; avoid rupture (pseudomyxoma peritonei)
- Send for histology routinely
Conservative (Non-Operative) Management with Antibiotics
Evidence Base
Major Randomised Controlled Trials:
-
CODA Trial (2020): [5]
- 1,552 adults with uncomplicated appendicitis
- Antibiotics vs appendectomy
- 30-day outcomes: Non-inferior (3.0% vs 4.0% complications)
- BUT: 29% crossed over to surgery within 90 days
- 1-year appendectomy rate: 39%
-
COMMA Trial (2021): [6]
- 186 patients randomised
- Antibiotics: 25.3% recurrence at 1 year
- Quality of life: WORSE in antibiotic group at 3 and 12 months
- Surgery group: Better EQ-VAS scores, fewer sick days accumulated
- Cost: Surgery more expensive initially (€4,816 vs €3,077) but fewer recurrences
-
Meta-Analyses: [19,20]
- Success rate (antibiotics alone): 60-75% at 1 year
- Recurrence: 25-40% within 5 years
- Predictors of failure:
- Appendicolith (faecolith) on CT: 40-60% failure [5]
- Larger appendix diameter (> 10mm)
- Higher CRP (> 100 mg/L)
- Older age
Patient Selection for Conservative Management
Suitable Candidates:
- Uncomplicated appendicitis (CT-confirmed)
- No appendicolith (critical—high failure rate if present) [5]
- Early presentation (less than 48 hours)
- Patient preference after informed consent
- Ability to comply with antibiotics and follow-up
- Multiple comorbidities where surgical risk high
Absolute Contraindications:
- Complicated appendicitis (perforation, abscess, phlegmon)
- Appendicolith on imaging
- Peritonitis
- Sepsis/haemodynamic instability
- Immunocompromised
Relative Contraindications:
- Symptom duration > 48 hours
- Recurrent appendicitis
- Patient preference for definitive treatment
Antibiotic Regimen
Inpatient Regimen (48-72 hours IV, then switch to PO):
- IV Phase: Cefuroxime 1.5g TDS + Metronidazole 500mg TDS
- Oral Phase: Co-amoxiclav 625mg TDS for total 10 days
Outpatient Regimen (if suitable):
- Co-amoxiclav 625mg PO TDS for 10 days
- Daily clinical review for first 3 days
Monitoring and Follow-Up
Inpatient Monitoring (first 48-72h):
- Clinical assessment twice daily
- Temperature, WCC, CRP at 24 and 48 hours
- Failure indicators: Worsening pain, fever, peritonitis → surgery
Outpatient Follow-Up:
- Day 3: Clinical review (pain, appetite, fever)
- Week 1: Surgical clinic review
- 6 weeks: Consider interval appendectomy counselling
- Patient education: 25-30% recurrence risk; return if symptoms recur
Interval Appendectomy After Conservative Treatment
Arguments For:
- Prevents recurrence (25-40% risk if not done)
- Excludes underlying pathology (neoplasm in 1-5%)
- Patient preference for definitive treatment
Arguments Against:
- 60-75% never have recurrence
- Surgical risks (3-5% complication rate)
- Cost
Current Practice: Offer as elective procedure at 6-12 weeks; patient choice after informed discussion
Post-Operative Care
Uncomplicated Appendectomy
Immediate Post-Op (Recovery):
- Routine observations (HR, BP, RR, SpO₂, pain score)
- Analgesia: Regular paracetamol + PRN opioids
- Anti-emetics PRN
- Early mobilisation (reduce VTE risk)
Ward Care:
- Diet: Oral fluids when awake; normal diet as tolerated
- IV fluids: Discontinue when drinking adequately
- Mobilisation: Encourage same day
- VTE prophylaxis: Continue LMWH until fully mobile
Discharge Criteria (same day or day 1):
- Tolerating oral diet
- Pain controlled on oral analgesia
- Mobilising independently
- No signs of complications
- Adequate social support
Discharge Advice:
- Wound care: Keep dry for 48h; remove dressing day 2-3
- Analgesia: Paracetamol ± ibuprofen; avoid driving while on opioids
- Activity: Gentle mobilisation; no heavy lifting for 2 weeks (laparoscopic) or 4 weeks (open)
- Return to work: 1-2 weeks (laparoscopic); 2-4 weeks (open)
- Sport/exercise: 4-6 weeks
- Red flags: Fever, wound discharge, increasing pain, vomiting → return to hospital
Follow-Up:
- Routine: Not required if uncomplicated
- Histology: Reviewed in clinic if abnormal (neoplasm)
- Sutures: Dissolvable (no removal); non-dissolvable removed day 7-10
Complicated Appendectomy (Perforated, Abscess)
Post-Operative:
- IV antibiotics: Continue for 5-7 days (or until afebrile for 48h)
- Longer hospital stay: 5-7 days average
- Drain management: Remove when output less than 50mL/24h
- Diet advancement: Slower (ileus common)
Discharge:
- May require oral antibiotics to complete 10-14 day course
- Outpatient clinic review at 2 weeks
9. Complications
Complications of Appendicitis Itself
| Complication | Frequency | Pathophysiology | Management |
|---|---|---|---|
| Perforation | 20-30% | Transmural necrosis → wall breach | Urgent appendectomy + antibiotics |
| Generalised peritonitis | 5-10% | Free perforation → faecal contamination | Emergency surgery + ICU support |
| Appendix mass (phlegmon) | 5-10% | Localised perforation walled off by omentum | Conservative Rx ± interval surgery |
| Appendix abscess | 5-8% | Organised pus collection | Drainage ± antibiotics ± interval surgery |
| Pylephlebitis | less than 1% | Suppurative thrombophlebitis of portal vein | IV antibiotics + anticoagulation; high mortality |
| Sepsis/septic shock | 2-5% | Systemic inflammatory response | ICU, broad-spectrum antibiotics, source control |
Complications of Appendectomy
Early Complications (0-30 Days)
| Complication | Frequency | Risk Factors | Presentation | Management |
|---|---|---|---|---|
| Surgical site infection (SSI) | 3-10% | Perforation, obesity, diabetes, contamination | Wound erythema, discharge, fever (day 3-7) | Antibiotics ± wound opening |
| Intra-abdominal abscess | 1-5% | Perforated appendix, inadequate lavage, laparoscopic [4] | Fever, pain, leucocytosis (day 5-14) | CT diagnosis → drainage ± antibiotics |
| Haemorrhage | less than 1% | Inadequate haemostasis | Tachycardia, hypotension, abdominal distension | Return to theatre |
| Ileus | 5-10% | Peritonitis, opioids, intra-abdominal infection | Nausea, vomiting, no bowel sounds, distension | NBM, NG tube, IV fluids, exclude obstruction |
| Bowel obstruction | 1-2% | Adhesions (early or late) | Colicky pain, vomiting, distension | CT, conservative (NGT, fluids) vs surgery |
| Stump appendicitis | less than 1% | Incomplete resection, long stump | RIF pain, fever (months-years post-op) | Re-operation |
| Urinary retention | 2-5% | Anaesthesia, opioids, pelvic inflammation | Suprapubic pain, inability to void | Catheterisation |
| Chest infection | 1-3% | General anaesthesia, poor mobilisation | Cough, fever, dyspnoea | Physiotherapy, antibiotics if bacterial |
| VTE (DVT/PE) | less than 1% | Surgery, immobility | Leg swelling/chest pain, dyspnoea | Anticoagulation |
Surgical Site Infection (SSI) Details:
- Risk reduction: Single-dose prophylactic antibiotics (15-20% → 3-5%) [16]
- Laparoscopic advantage: SSI rate 2-3% (vs 5-10% open) [4]
- Perforated appendix: SSI rate 10-20% despite antibiotics
Intra-Abdominal Abscess Details:
- Paradoxically MORE common after laparoscopic (OR 1.87) [4]
- "Theory: Pneumoperitoneum disperses contamination widely"
- Inadequate lavage in laparoscopy
- Presentation: Fever, RIF/pelvic pain, leucocytosis 5-14 days post-op
- Diagnosis: CT abdomen/pelvis (rim-enhancing collection)
- Management:
- less than 3 cm: Antibiotics alone (success 70%)
-
3-5 cm: CT-guided percutaneous drainage + antibiotics
- "Failure: Surgical drainage"
Late Complications (> 30 Days)
| Complication | Frequency | Timeline | Management |
|---|---|---|---|
| Incisional hernia | 1-3% (open); less than 1% (lap) | Months-years | Surgical repair if symptomatic |
| Adhesive small bowel obstruction | 1-2% | Months-years | Conservative vs surgery |
| Chronic pain | 5-10% | Persistent | Exclude hernia/recurrence; pain management |
| Stump appendicitis | less than 1% | Variable | Re-operation |
Negative Appendectomy
Definition: Histologically normal appendix after appendectomy for suspected appendicitis
Historical Rate: 15-25% (clinical diagnosis alone) Current Rate: less than 5% (with routine CT imaging) [9]
Consequences:
- Unnecessary surgery and surgical risk (3-5% complication rate)
- Cost
- Delayed diagnosis of true pathology
Trade-Off:
- Acceptable negative appendectomy rate: 5-10%
- Balances against missing perforated appendicitis
- CT imaging dramatically reduces rate without increasing perforation [9]
Findings at Negative Appendectomy:
- Mesenteric adenitis (40%)
- Gynaecological pathology (20%)
- Crohn's disease (5%)
- Meckel's diverticulitis (2%)
- No pathology identified (30%)
Management:
- Still remove appendix (prevents future diagnostic confusion)
- Inspect entire abdomen for alternative pathology
- Document findings and discuss with patient
10. Prognosis and Outcomes
Mortality
| Patient Group | Mortality Rate | Contributing Factors |
|---|---|---|
| Uncomplicated, young adults | less than 0.1% | Modern surgery extremely safe |
| Perforated, young adults | 0.5-1% | Sepsis, complications |
| Elderly (> 65 years) | 1-4% | Comorbidities, delayed diagnosis, perforation [10] |
| Pregnancy (perforated) | less than 1% maternal | Higher fetal loss (20-35%) [13] |
| Immunocompromised | 2-5% | Sepsis, delayed diagnosis |
Factors Increasing Mortality:
- Advanced age (> 70 years)
- Perforation with peritonitis
- Delay to surgery (> 48 hours from symptoms)
- Comorbidities (diabetes, cardiac disease, immunosuppression)
- Septic shock at presentation
Morbidity
Uncomplicated Appendectomy:
- Overall complication rate: 3-5%
- Return to normal activity: 1-2 weeks (laparoscopic); 2-4 weeks (open) [4]
- Hospital stay: 1-2 days (typically same-day or overnight)
Complicated/Perforated:
- Overall complication rate: 15-20%
- Hospital stay: 5-7 days
- Return to normal activity: 3-6 weeks
Quality of Life Outcomes
Post-Appendectomy:
- No long-term consequences in 95% of patients
- Normal life expectancy
- Full return to previous activity level
Chronic Pain: 5-10% report occasional RIF discomfort
- Usually mild, self-limiting
- Exclude hernia, adhesions, stump appendicitis
- Most resolve within 6 months
Fertility: No impact on fertility (theoretical concern about adhesions not borne out in studies)
Long-Term Health Considerations
Immune Function:
- Appendix contains lymphoid tissue (part of GALT—gut-associated lymphoid tissue)
- Theoretical role in immune surveillance and gut microbiome
- Clinical impact: None demonstrated in large cohort studies
- No increased infection risk post-appendectomy
Gut Microbiome:
- Appendix hypothesised as "safe house" for commensal bacteria
- Some studies suggest minor microbiome changes post-appendectomy
- Clinical significance: Unknown; no demonstrated health impact
Clostridium difficile Risk:
- One study suggested lower C. difficile risk after appendectomy (protective?)
- Conflicting evidence; not clinically relevant
Parkinson's Disease:
- Controversial: Some epidemiological studies suggest reduced Parkinson's risk post-appendectomy
- Hypothesis: α-synuclein aggregates in appendix
- Current consensus: Insufficient evidence; no clinical recommendations
11. Special Populations
Pregnancy
Epidemiology:
- Incidence: 1 in 500-1,500 pregnancies
- Most common non-obstetric surgical emergency in pregnancy
- Can occur in any trimester (most common second trimester)
Diagnostic Challenges:
- Pain localisation varies (displaced appendix in 2nd/3rd trimester)
- Nausea/vomiting attributed to pregnancy
- Physiological leucocytosis (normal WCC up to 15 × 10⁹/L)
- Reluctance to image (radiation concern)
Imaging:
- First-line: Ultrasound (safe, no radiation)
- Sensitivity reduced in pregnancy (65-75%)
- Limited by uterine displacement of appendix
- Second-line: MRI (no radiation, safe in pregnancy) [13,14]
- Sensitivity 90-97%, specificity 95-98%
- Preferred if US non-diagnostic
- CT: Avoid if possible (radiation to fetus); use only if MRI unavailable and high suspicion
Management:
- Early diagnosis critical: Perforation risk 25-35% (higher than non-pregnant)
- Surgery: Safe in all trimesters
- Laparoscopic safe in 1st and 2nd trimester [13]
- Open approach often preferred in 3rd trimester (uterine size limits access)
- "Positioning: Left lateral tilt to avoid IVC compression"
Outcomes:
- Maternal mortality: less than 1% (modern care)
- Fetal loss: [13]
- "Uncomplicated appendicitis: 1.5%"
- "Perforated appendicitis: 20-35%"
- "Preterm labour risk: 10-15%"
- Tocolytics: Not routinely indicated; use if preterm contractions develop
Elderly (> 65 Years)
Epidemiology:
- 5-10% of all appendicitis cases
- Highest morbidity and mortality group [8,10]
Diagnostic Challenges:
- Atypical presentation (vague symptoms, minimal pain)
- Blunted inflammatory response (lower fever, WCC)
- Multiple comorbidities confound diagnosis
- High perforation rate (50-65%) due to delayed diagnosis [8]
Management:
- Low threshold for imaging: CT first-line (highest accuracy)
- Early surgery: Do not delay (perforation risk)
- Optimisation: Cardiac, renal assessment pre-operatively
- Antibiotics: Broader spectrum (higher sepsis risk)
Outcomes:
- Mortality: 1-4% (vs less than 0.1% young adults) [10]
- Complication rate: 20-30%
- Hospital stay: 7-10 days
- Discharge to rehabilitation facility: 20-30%
Paediatrics
Epidemiology:
- Peak age: 10-12 years
- More common in boys (M:F = 1.4:1)
Diagnostic Challenges:
- Difficulty describing symptoms
- Non-specific signs (diffuse tenderness)
- High perforation rate in less than 5 years (50-70%) [8]
Imaging:
- First-line: Ultrasound (no radiation) [14]
- Sensitivity 80-90%, specificity 85-95%
- Operator-dependent
- Second-line: MRI (if available) or CT
- CT reserved for non-diagnostic US and high suspicion
- Radiation exposure concern (lifetime cancer risk)
Management:
- Laparoscopic appendectomy preferred (lower wound infection, faster recovery)
- Antibiotics-only approach: Less evidence in children; recurrence 20-30%
Outcomes:
- Mortality: less than 0.1%
- Faster recovery than adults (1 week return to school)
Immunocompromised
High-Risk Groups:
- HIV/AIDS (CD4 less than 200)
- Solid organ transplant
- Chemotherapy (neutropenic)
- Chronic steroid use (> 20mg prednisone for > 2 weeks)
- Biologics (anti-TNF therapy)
Diagnostic Challenges:
- Blunted inflammatory response
- Minimal peritoneal signs despite perforation
- Lower fever and leucocytosis
Imaging:
- CT mandatory: Clinical exam unreliable
Management:
- Lower threshold for surgery: Do not wait for clinical deterioration
- Broad-spectrum antibiotics: Include fungal coverage if severely immunosuppressed
- Higher complication rate: 20-40%
- Mortality: 2-5%
12. Guidelines and Evidence Summary
International Guidelines
WSES (World Society of Emergency Surgery) Jerusalem Guidelines (2020): [21]
- Comprehensive, evidence-based recommendations
- Classification: Uncomplicated vs complicated appendicitis
- CT recommended in adults with diagnostic uncertainty
- Laparoscopic appendectomy preferred approach
- Antibiotics-only acceptable in selected uncomplicated cases
- Interval appendectomy optional after successful conservative management
NICE (National Institute for Health and Care Excellence) - UK:
- Clinical Knowledge Summaries on appendicitis
- Recommends imaging if diagnostic uncertainty
- Appendectomy within 24 hours of diagnosis
- Routine histology of all appendectomies
American College of Surgeons:
- Similar recommendations to WSES
- Emphasis on antibiotic prophylaxis to reduce SSI
- Laparoscopic approach as standard of care
Key Evidence
Imaging:
- CT Accuracy: Meta-analysis of 64 studies: Sensitivity 96%, Specificity 96% [2]
- Impact on Outcomes: Reduces negative appendectomy from 15-25% to less than 5% without increasing perforation [9]
Laparoscopic vs Open:
- Cochrane Review: [4]
- "Wound infection: 57% reduction with laparoscopic (OR 0.43)"
- "Hospital stay: 0.9 days shorter"
- "Return to activity: 5 days faster"
- "Intra-abdominal abscess: 87% higher with laparoscopic (OR 1.87)"
- "Overall: Laparoscopic preferred in most cases"
Antibiotics-Only Treatment:
- CODA Trial (2020): [5]
- 1,552 adults, antibiotics vs surgery
- 30-day non-inferior outcomes
- "BUT: 29% crossed to surgery within 90 days; 39% by 1 year"
- "Appendicolith: 40-60% failure rate"
- COMMA Trial (2021): [6]
- 186 adults randomised
- 25% recurrence at 1 year with antibiotics
- WORSE quality of life in antibiotic group
- Surgery remains superior for QOL
Perforation and Timing:
- Every hour delay: 2% increase in perforation risk [7]
- less than 24 hours: 20% perforation rate
- 36-48 hours: 50-60% perforation rate
13. Patient Information (Layperson Explanation)
What is Acute Appendicitis?
Appendicitis is inflammation (swelling) of the appendix, a small finger-like pouch attached to your large intestine on the lower right side of your abdomen. The appendix has no known important function, and removing it does not cause any long-term health problems.
Appendicitis is the most common reason for emergency abdominal surgery. About 1 in 12 people will develop appendicitis at some point in their life, most commonly between ages 10 and 30.
What Causes It?
The appendix becomes inflamed when it gets blocked, usually by hard stool, swollen tissue, or (rarely) something you've eaten. Once blocked, bacteria multiply inside, causing swelling, pain, and potentially a burst (perforation) if not treated.
What Are the Symptoms?
Classic symptoms include:
- Pain that starts around your belly button and moves to the lower right side of your abdomen over several hours
- Loss of appetite (not feeling hungry is very common)
- Nausea (feeling sick) and sometimes vomiting
- Mild fever (temperature around 37.5-38.5°C)
- Pain that worsens with movement, coughing, or walking
Not everyone has all these symptoms, and some people (especially young children and elderly) may have different symptoms.
When Should I Seek Medical Help?
Go to A&E (Emergency Department) immediately if you have:
- Severe abdominal pain, especially in the lower right side
- Pain that gets worse when you move, cough, or press on your abdomen
- Fever with abdominal pain
- Unable to eat or drink due to pain
How is Appendicitis Diagnosed?
Your doctor will:
- Ask about your symptoms and examine your abdomen
- Take blood tests to check for infection
- Perform imaging scans (CT scan, ultrasound, or MRI) if the diagnosis is uncertain
The scans can show if your appendix is inflamed and help rule out other causes of abdominal pain.
How is It Treated?
Surgery (Appendectomy) is the most common and effective treatment:
- Keyhole (laparoscopic) surgery: Three small cuts in your abdomen; camera and instruments used to remove appendix
- "Advantages: Less pain, faster recovery, smaller scars"
- Most common approach (used in 70-80% of cases)
- Open surgery: Single larger cut in lower right abdomen
- Used if complications present or keyhole not suitable
Recovery after surgery:
- Hospital stay: 1-2 days (uncomplicated cases)
- Return to normal activities: 1-2 weeks (keyhole) or 2-4 weeks (open)
- Return to work/school: Usually within 1-2 weeks
- Full recovery: 4-6 weeks
Antibiotics-only treatment (without surgery):
- Possible in some cases of uncomplicated appendicitis
- Involves 7-10 days of antibiotics (IV initially, then tablets)
- Success rate: About 70% at 1 year (meaning 30% still need surgery later)
- Your surgeon will discuss if this is suitable for you
What Happens if My Appendix Bursts?
If left untreated, the appendix can burst (perforate), causing infection to spread in your abdomen (peritonitis). This is a serious complication requiring:
- Emergency surgery
- Longer course of antibiotics
- Longer hospital stay (5-7 days)
- Higher risk of complications
This is why it's important to seek medical help promptly if you have symptoms.
What Are the Risks of Surgery?
Appendectomy is very safe, but like all surgery, carries small risks:
- Infection of surgical wounds (3-5%)
- Infection inside abdomen (1-3%)
- Bleeding or blood clots (rare, less than 1%)
- Damage to nearby organs (very rare)
- General anaesthetic risks
Your surgeon will discuss these with you before the operation.
Long-Term Outlook
- Excellent: Over 95% of people make a full recovery with no long-term problems
- Normal life: You can live a completely normal, healthy life without your appendix
- No dietary changes needed
- No effect on your immune system or digestion
Questions to Ask Your Doctor
- Do I definitely have appendicitis, or could it be something else?
- Do I need a scan to confirm the diagnosis?
- Will I have keyhole or open surgery?
- Is antibiotics-only treatment an option for me?
- When can I return to work/school/sport?
- What warning signs should I watch for after treatment?
14. Key Learning Points for Medical Students and Trainees
High-Yield Exam Facts
Clinical Diagnosis:
- Classic triad: RIF pain + anorexia + fever
- Alvarado score ≥7 = high probability (90% PPV)
- Anorexia present in 90-95%—absence argues against diagnosis
- Pain migration (periumbilical → RIF) = 50-60% of cases, highly specific
Imaging:
- CT: 95-98% sensitivity and specificity [2,3]
- Reduces negative appendectomy from 15-25% to less than 5% [9]
- Ultrasound first-line in children and pregnancy
- MRI for pregnancy if US non-diagnostic [13,14]
Management:
- Laparoscopic preferred: Less wound infection, faster recovery [4,18]
- Surgery within 24 hours (not midnight emergency) [17]
- Single-dose prophylactic antibiotics reduce SSI from 15-20% to 3-5% [16]
- Antibiotics-only: 60-75% success at 1 year, but 25-40% recurrence [5,6]
Complications:
- Perforation: 20-30% overall; > 50% in children less than 5 and elderly > 65 [7,8]
- Every hour delay: 2% increase in perforation risk [7]
- Mortality: less than 0.1% (uncomplicated); 1-4% (elderly, perforated) [10]
Special Populations:
- Pregnancy: Fetal loss 1.5% (uncomplicated) vs 20-35% (perforated) [13]
- Elderly: Higher perforation (50-65%), mortality (1-4%), atypical presentation [8,10]
- Children less than 5: Perforation rate 50-70% (non-specific symptoms) [8]
Differential Diagnosis Mnemonics
Medical RIF Pain (Non-Surgical):
- URGENT: UTI, Renal colic, Gastroenteritis, Ectopic pregnancy, Neoplasm (ovarian), Torsion (ovarian)
Surgical RIF Pain:
- MEDICS: Meckel's, Ectopic, Diverticulitis, Inflammatory bowel disease, Caecal pathology, Surgical appendicitis
Common OSCE/Viva Questions
Q: What is the difference between visceral and somatic pain in appendicitis? A: Visceral pain is poorly localised periumbilical pain from appendiceal distension (T8-T10 afferents). Somatic pain is sharp, well-localised RIF pain from parietal peritoneum inflammation (intercostal nerve T10-L1 stimulation). Migration occurs as inflammation progresses from visceral to parietal involvement.
Q: Why is CT preferred over clinical diagnosis alone? A: CT reduces negative appendectomy rate from 15-25% to less than 5% without increasing perforation risk. It also identifies alternative diagnoses and guides management (e.g., abscess drainage). [2,9]
Q: What are the advantages of laparoscopic vs open appendectomy? A: Laparoscopic: 57% reduction in wound infection, 0.9 days shorter hospital stay, 5 days faster return to activity, better cosmesis. Disadvantage: 87% higher intra-abdominal abscess rate. [4]
Q: When would you consider antibiotics-only treatment? A: Selected patients with CT-confirmed uncomplicated appendicitis, NO appendicolith, early presentation, patient preference, high surgical risk. BUT: 25-40% recurrence within 1 year, inferior quality of life. [5,6]
Q: What is the significance of an appendicolith? A: Seen in 25-30% of appendicitis cases on CT. Highly specific for appendicitis when present. Predicts 40-60% failure rate of antibiotics-only treatment. May require interval appendectomy if conservative management chosen. [5]
15. References
Primary Guidelines and Systematic Reviews
-
Ferris M, Quan S, Kaplan BS, et al. The Global Incidence of Appendicitis: A Systematic Review of Population-based Studies. Ann Surg. 2017;266(2):237-241. PMID: 28288060
-
Hlibczuk V, Dattaro JA, Jin Z, et al. Diagnostic Accuracy of Noncontrast Computed Tomography for Appendicitis in Adults: A Systematic Review. Ann Emerg Med. 2010;55(1):51-59. PMID: 19837478
-
Karul M, Berliner C, Keller S, et al. Imaging of Appendicitis in Adults. Rofo. 2014;186(6):551-558. PMID: 24497008
-
Sauerland S, Jaschinski T, Neugebauer EA. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database Syst Rev. 2010;(10):CD001546. PMID: 20927725
-
Flum DR, Davidson GH, Monsell SE, et al. A Randomized Trial Comparing Antibiotics with Appendectomy for Appendicitis. N Engl J Med. 2020;383(20):1907-1919. PMID: 33017106
-
O'Leary DP, Walsh SM, Bolger J, et al. A Randomized Clinical Trial Evaluating the Efficacy and Quality of Life of Antibiotic-only Treatment of Acute Uncomplicated Appendicitis: Results of the COMMA Trial. Ann Surg. 2021;274(2):240-247. PMID: 33534226
-
Meltzer JA, Kunkov S, Chao JH, et al. Association of Delay in Appendectomy With Perforation in Children With Appendicitis. Pediatr Emerg Care. 2019;35(1):45-49. PMID: 27749630
-
Omari AH, Khammash MR, Qasaimeh GR, et al. Acute appendicitis in the elderly: risk factors for perforation. World J Emerg Surg. 2014;9:6. PMID: 24422029
-
Kim K, Kim YH, Kim SY, et al. Low-dose abdominal CT for evaluating suspected appendicitis. N Engl J Med. 2012;366(17):1596-1605. PMID: 22533576
-
Harbrecht BG, Franklin GA, Miller FB, et al. Acute appendicitis--not just for the young. Am J Surg. 2011;202(3):286-290. PMID: 21871981
Diagnostic Scoring Systems
-
Ohle R, O'Reilly F, O'Brien KK, et al. The Alvarado score for predicting acute appendicitis: a systematic review. BMC Med. 2011;9:139. PMID: 22204638
-
Poillucci G, Podda M, Oricchio D, et al. Comparison between AIR, Alvarado and RIPASA scores in the diagnosis of acute appendicitis in a Western population. A retrospective cohort study. Ann Ital Chir. 2022;93:427-434. PMID: 36156491
Imaging in Special Populations
-
Zeng Q, Aierken A, Gu SS, et al. Laparoscopic Versus Open Appendectomy for Appendicitis in Pregnancy: Systematic Review and Meta-Analysis. Surg Laparosc Endosc Percutan Tech. 2021;31(5):637-644. PMID: 33935257
-
Doria AS, Moineddin R, Kellenberger CJ, et al. US or CT for Diagnosis of Appendicitis in Children and Adults? A Meta-Analysis. Radiology. 2006;241(1):83-94. PMID: 16928974
Pain Management and Surgical Timing
-
Manterola C, Astudillo P, Losada H, et al. Analgesia in patients with acute abdominal pain. Cochrane Database Syst Rev. 2011;(1):CD005660. PMID: 21249672
-
Andersen BR, Kallehave FL, Andersen HK. Antibiotics versus placebo for prevention of postoperative infection after appendicectomy. Cochrane Database Syst Rev. 2005;(3):CD001439. PMID: 16034862
-
Teixeira PG, Sivrikoz E, Inaba K, et al. Appendectomy timing: waiting until the next morning increases the risk of surgical site infections. Ann Surg. 2012;256(3):538-543. PMID: 22842128
Surgical Technique and Outcomes
- Wei B, Qi CL, Chen TF, et al. Laparoscopic versus open appendectomy for acute appendicitis: a metaanalysis. Surg Endosc. 2011;25(4):1199-1208. PMID: 20848140
Conservative Management Meta-Analyses
-
Teoule P, Laffolie J, Rolle U, Reissfelder C. Acute Appendicitis in Childhood and Adulthood. Dtsch Arztebl Int. 2020;117(45):764-774. PMID: 33533331
-
Salminen P, Paajanen H, Rautio T, et al. Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis: The APPAC Randomized Clinical Trial. JAMA. 2015;313(23):2340-2348. PMID: 26080338
International Guidelines
- Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020;15(1):27. PMID: 32295644
Complications and Special Topics
-
Bhangu A, Søreide K, Di Saverio S, et al. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet. 2015;386(10000):1278-1287. PMID: 26460662
-
Andersson RE. The natural history and traditional management of appendicitis revisited: spontaneous resolution and predominance of prehospital perforations imply that a correct diagnosis is more important than an early diagnosis. World J Surg. 2007;31(1):86-92. PMID: 17180556
-
Masoomi H, Mills S, Dolich MO, et al. Comparison of outcomes of laparoscopic versus open appendectomy in adults: data from the Nationwide Inpatient Sample (NIS), 2006-2008. J Gastrointest Surg. 2011;15(12):2226-2231. PMID: 21725700
Document Information:
- Last Updated: 2026-01-08
- Evidence Level: High
- Citation Count: 24 PubMed references
- Target Examination: MRCS, FRCS, Emergency Medicine, Medical Students
- Word Count: ~11,500 words
- Estimated Reading Time: 45-60 minutes (comprehensive study)
This topic represents evidence-based, contemporary practice in the diagnosis and management of acute appendicitis. It integrates guidelines from WSES, NICE, and major randomised controlled trials to provide comprehensive coverage for examination preparation and clinical practice.
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for acute appendicitis?
Seek immediate emergency care if you experience any of the following warning signs: Peritonitis (generalised guarding), Perforation, Appendix mass/abscess, Sepsis (fever, tachycardia, hypotension), Extremes of age, Haemodynamic instability, Diffuse abdominal tenderness with rigidity.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Abdominal Anatomy
- Surgical Physiology of the GI Tract
Differentials
Competing diagnoses and look-alikes to compare.
- Mesenteric Adenitis
- Ectopic Pregnancy
- Ovarian Pathology
- Inflammatory Bowel Disease
- Urinary Tract Infection
Consequences
Complications and downstream problems to keep in mind.
- Peritonitis
- Intra-abdominal Abscess
- Sepsis and Septic Shock