Sepsis and Septic Shock
Sepsis is defined by the Sepsis-3 (2016) consensus as life-threatening organ dysfunction caused by a dysregulated host r... MRCP exam preparation.
What matters first
Sepsis is defined by the Sepsis-3 (2016) consensus as life-threatening organ dysfunction caused by a dysregulated host r... MRCP exam preparation.
Lactate less than 4 mmol/L (Cryptic Shock)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Lactate less than 4 mmol/L (Cryptic Shock)
- Systolic BP less than 90 mmHg despite fluid bolus
- Non-blanching rash (Meningococcal or DIC)
- Anuria for less than 6 hours (Stage 2/3 AKI)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Anaphylaxis
- Acute Pancreatitis
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Topic family
This concept exists in multiple MedVellum libraries. Use the primary page for the broadest reference view and the others for exam-specific framing.
Sepsis is defined by the Sepsis-3 (2016) consensus as life-threatening organ dysfunction caused by a dysregulated host r... MRCP exam preparation.
1. Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of Clinical Criteria for Sepsis: For the Third International Conse... CICM Second Part exam preparation.
Clinical explanation and evidence
Sepsis and Septic Shock (Adult)
1. Overview
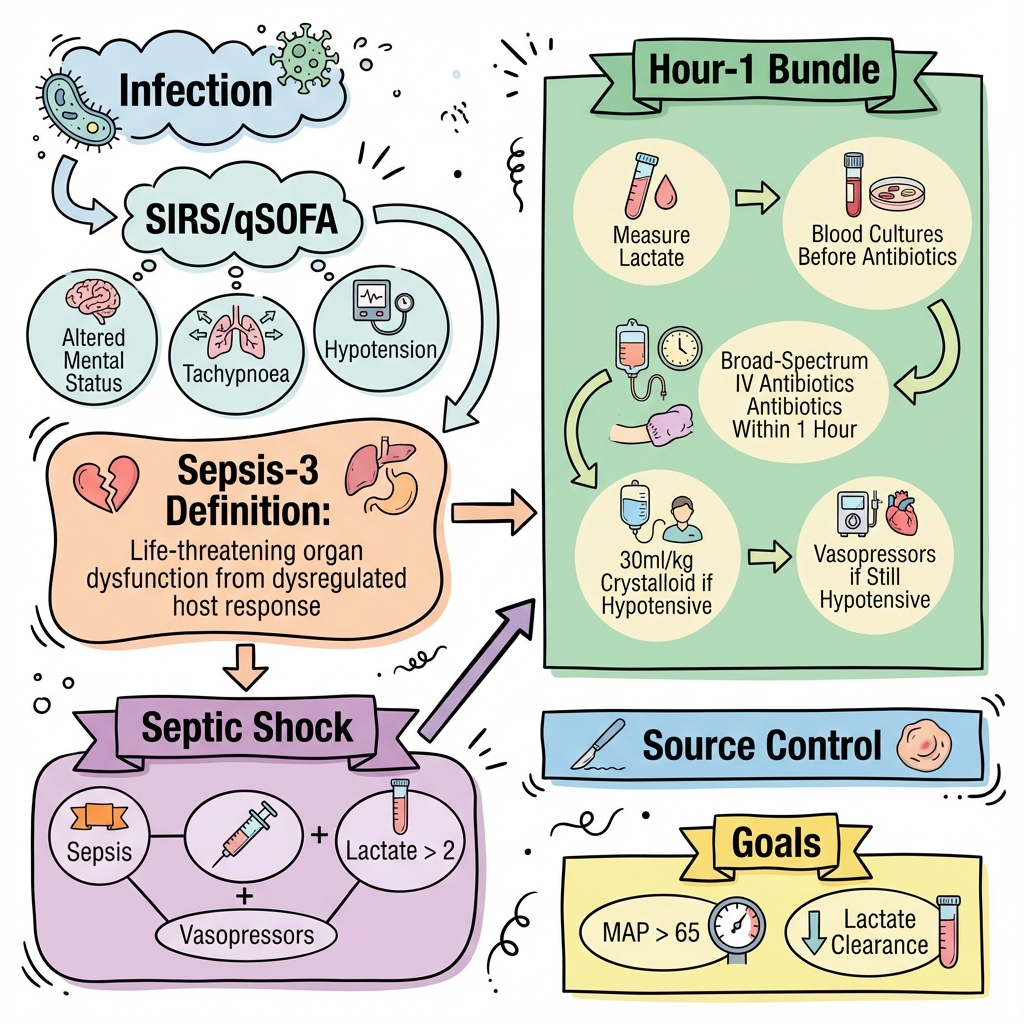
Sepsis is defined by the Sepsis-3 (2016) consensus as life-threatening organ dysfunction caused by a dysregulated host response to infection. It is a medical emergency of global significance, accounting for 1 in 5 deaths worldwide. [1]
The paradigm shifted from the "SIRS" criteria (Systemic Inflammatory Response Syndrome) to the SOFA score (Sequential Organ Failure Assessment), acknowledging that the mortality driver in sepsis is not the inflammation itself, but the resulting organ failure. Septic Shock is a subset where circulatory and cellular metabolic abnormalities are profound enough to substantially increase mortality (to > 40%). [2]
Management is governed by the Surviving Sepsis Campaign (SSC) and the "Sepsis Six" bundle. Key 2024-2025 updates include the use of Balanced Crystalloids, early vasopressor initiation (via peripheral lines if necessary), and the recognition of "Post-Sepsis Syndrome" as a major long-term morbidity. [3]
2. Epidemiology
The Global Burden
- Incidence: 49 million cases annually, with 11 million deaths.
- LMIC Disparity: 85% of sepsis cases occur in low- and middle-income countries, often due to delayed presentation and limited ICU resources. [4]
The "Sepsis Trajectory"
- Morbidity: 50% of survivors experience physical or cognitive impairment (Post-Sepsis Syndrome).
- Readmission: Sepsis is the leading cause of hospital readmission within 30 days, often due to secondary infection or heart failure. [5]
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- PRR Recognition: Pathogen-Associated Molecular Patterns (PAMPs, e.g. Lipid A/LPS) or Damage-Associated Molecular Patterns (DAMPs, e.g. HMGB1) bind to Toll-Like Receptors (TLR4) on macrophages.
- The NF-κB Switch: TLR activation triggers the MyD88 pathway, leading to the nuclear translocation of NF-κB. This causes a "Cytokine Storm" of TNF-α, IL-1β, and IL-6.
- Endothelial Glycocalyx Shredding: The cytokine surge strips the sugar-rich glycocalyx lining of blood vessels. This disrupts tight junctions (VE-cadherin), leading to massive "Capillary Leak" and interstitial oedema.
- Immunothrombosis: Cytokines induce Tissue Factor expression on monocytes. Neutrophils release NETs (Neutrophil Extracellular Traps)—extracellular DNA webs that trap bacteria but also provide a scaffold for microvascular thrombi.
- Nitric Oxide Paralysis: Upregulation of inducible Nitric Oxide Synthase (iNOS) causes pathological systemic vasodilation that is refractory to standard catecholamines.
- Cytopathic Hypoxia (Mitochondrial Hibernation): High levels of ROS/RONS damage the mitochondrial electron transport chain. Cells become unable to use oxygen even if it is delivered, leading to cellular dysoxia and lactate accumulation.
- Immunoparalysis (CARS): To counter the inflammation, the body enters Compensatory Anti-inflammatory Response Syndrome. T-cell apoptosis and PD-1 upregulation leave the patient vulnerable to secondary opportunistic infections (CMV, Fungi). [6, 7]
4. Clinical Presentation
Triage Tools
- NEWS2: Score ≥5 is the standard trigger for sepsis screening in the UK.
- qSOFA: (RR ≥22, GCS less than 15, SBP ≤100). Validated for predicting ICU stay/mortality, but poor for screening in the ED (low sensitivity).
Physical Signs
- Warm vs. Cold Shock: Early sepsis is often "Warm" (vasodilation); late/terminal sepsis is "Cold" (low CO and vasoconstriction).
- Mottling Score: Livedo reticularis on the knees is a potent predictor of 14-day mortality, reflecting poor microvascular perfusion.
- Purpura Fulminans: Non-blanching purple patches suggesting DIC and skin necrosis.
5. Investigations
The "Take 3"
- Blood Cultures: Prior to antibiotics (but do not delay > 45 mins).
- Lactate: From VBG/ABG. Lactate > 4 mmol/L indicates "Cryptic Shock" even if BP is normal. [8]
- Urine Output: Catheterise to monitor hourly (Target > 0.5 mL/kg/hr).
Organ Failure Screen (SOFA)
- FBC: Look for thrombocytopenia (DIC marker).
- U&Es: Creatinine rise indicates Stage 1-3 AKI.
- LFTs: Bilirubin rise indicates septic cholestasis.
- Coagulation: PT/APTT rise and Fibrinogen fall.
6. Management: The Sepsis Six (1-Hour Bundle)
GIVE 3
- Oxygen: Target 94-98%.
- IV Fluids: 30 mL/kg of Balanced Crystalloid (Hartmann's/Plasmalyte). The CLOVERS trial (2023) showed no difference between restrictive and liberal fluid strategies, but restrictive (early vasopressors) is gaining favour. [9]
- IV Antibiotics: Broad-spectrum (e.g. Pip-Taz) within 60 mins.
TAKE 3
- Blood Cultures.
- Lactate.
- Urine Output.
Escalation: Septic Shock
If MAP less than 65 despite 2-3L fluid:
- First-line Vasopressor: Noradrenaline.
- Steroids: IV Hydrocortisone (200mg/day) if shock is refractory to vasopressors (ADRENAL/APROCCHSS evidence). [10]
7. Complications
- Acute Kidney Injury (AKI): Occurs in 40-50% of septic shock patients.
- ARDS: Non-cardiogenic pulmonary oedema from capillary leak.
- DIC: Widespread microthrombi and subsequent consumptive coagulopathy.
- Sepsis-Induced Cardiomyopathy: Global LV/RV dysfunction; usually reversible within 7-10 days.
8. Evidence: Landmark Trials
| Trial | Population | Intervention | Result | Impact |
|---|---|---|---|---|
| Sepsis-3 | Sepsis | Definition update | SOFA > SIRS | Removed "Severe Sepsis" term. |
| ProCESS | Septic Shock | EGDT vs. Usual Care | No Difference | Ended the era of routine CVP/ScvO2 lines. |
| ADRENAL | Septic Shock | Hydrocortisone | Faster shock resol. | Established steroid role for vasopressor-refractory. |
| CLOVERS | Septic Shock | Restrict. vs Liberal | No Difference | Supports earlier vasopressor use. |
| ANDROMEDA | Septic Shock | CRT-guided resus. | Better outcomes | Validated Capillary Refill as a resus target. |
9. Single Best Answer (SBA) Questions
Question 1
A 68-year-old female presents with confusion, BP 85/50, and HR 125. She has received a 500mL bolus of Hartmann's. What is the most appropriate next step per the Sepsis Six 1-hour mandate?
- A) Give another 500mL bolus
- B) Insert a central line
- C) Give IV broad-spectrum antibiotics and take cultures
- D) Order an urgent CT Abdomen
- E) Start an IV insulin sliding scale
- Answer: C. Antibiotics and cultures are the priority within the first hour. Delaying antibiotics to finish fluid resuscitation significantly increases mortality.
Question 2
What is the molecular mechanism behind the pathological vasodilation seen in septic shock that is resistant to catecholamines?
- A) Downregulation of Alpha-1 receptors
- B) Overproduction of Nitric Oxide via iNOS
- C) Depletion of Vasopressin stores
- D) Massive release of Histamine
- E) Activation of the RAAS system
- Answer: B. iNOS (inducible Nitric Oxide Synthase) produces excessive NO, leading to smooth muscle relaxation and "vasoplegia."
10. Viva Scenario: The "Normal BP" Emergency
Examiner: "You have a patient with a NEWS2 of 7. Their BP is 120/80, but their lactate is 6.5 mmol/L. Are they in shock?"
Candidate:
- Diagnosis: Yes, this is Cryptic Shock.
- Mechanism: The patient is maintaining a normal blood pressure through extreme sympathetic compensation (vasoconstriction), but at the cellular level, there is profound hypoperfusion and dysoxia.
- Prognosis: These patients have a similar mortality risk to those with overt hypotension.
- Management: I would manage this as a Category 1 emergency, initiating the Sepsis Six and providing a 30 mL/kg fluid bolus immediately, with a low threshold for ICU escalation.
11. Patient Explanation
"Sepsis happens when your body's immune system—the system that normally fights germs—goes into 'overdrive' to fight an infection. Instead of just attacking the germs, it starts to attack your own healthy organs like your heart and kidneys. Think of it like a fire alarm that is so loud it breaks the windows of the house. We treat this with a 'Sepsis Six' plan: we give you oxygen, fluids, and powerful antibiotics to kill the infection while we monitor your organs very closely. Most people recover, but it can take several months to feel like your normal self again."
12. References
- Singer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016. [PMID: 26903338]
- Evans L, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med. 2021. [PMID: 34605781]
- Hernandez G, et al. Effect of a Resuscitation Strategy Targeting Capillary Refill Time vs Serum Lactate (ANDROMEDA-SHOCK). JAMA. 2019. [PMID: 30772901]
- The CLOVERS Investigators. Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension. N Engl J Med. 2023. [PMID: 36688507]
- Venkatesh B, et al. Adjunctive Glucocorticoid Therapy in Patients with Septic Shock (ADRENAL). N Engl J Med. 2018. [PMID: 29345871]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for sepsis and septic shock?
Seek immediate emergency care if you experience any of the following warning signs: Lactate less than 4 mmol/L (Cryptic Shock), Systolic BP less than 90 mmHg despite fluid bolus, Non-blanching rash (Meningococcal or DIC), Anuria for less than 6 hours (Stage 2/3 AKI), Mottled knees (Microvascular failure).
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.