Cerebral Venous Sinus Thrombosis
Cerebral venous sinus thrombosis (CVST) is thrombosis of the dural venous sinuses and/or cerebral veins, causing impaire... MRCP exam preparation.
What matters first
Cerebral venous sinus thrombosis (CVST) is thrombosis of the dural venous sinuses and/or cerebral veins, causing impaire... MRCP exam preparation.
Thunderclap headache
9 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Thunderclap headache
- Seizures with headache
- Focal neurological deficit in young adult
- Reduced GCS
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Subarachnoid Haemorrhage
- Ischaemic Stroke
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Cerebral Venous Sinus Thrombosis
1. Clinical Overview
Summary
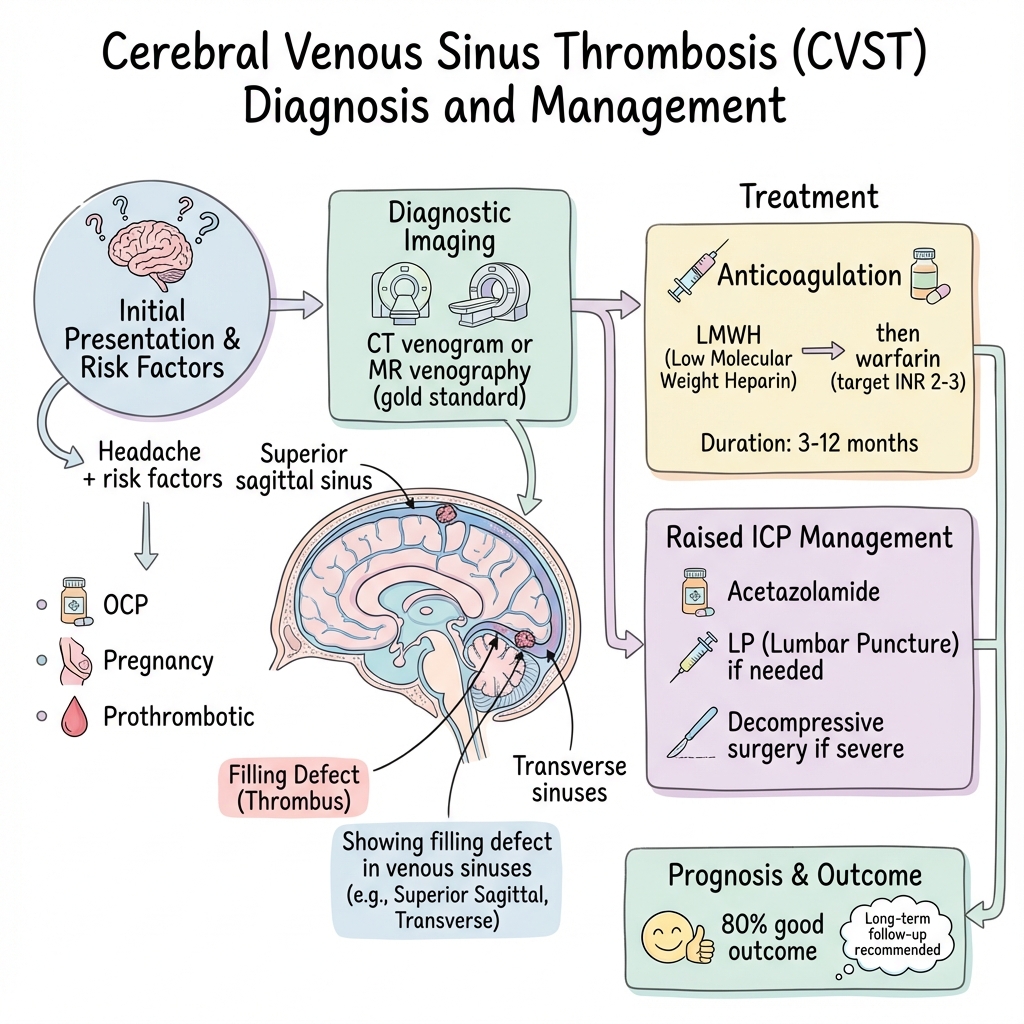
Cerebral venous sinus thrombosis (CVST) is thrombosis of the dural venous sinuses and/or cerebral veins, causing impaired venous drainage, raised intracranial pressure, and potential venous infarction with characteristic haemorrhagic transformation. [1] It represents approximately 0.5-1% of all strokes but is disproportionately important as a treatable cause of stroke in young adults, particularly women due to hormonal risk factors. [2]
Presentation is highly variable and often non-specific: isolated intracranial hypertension (headache with papilloedema), focal neurological deficits, seizures, or encephalopathy. The classic triad of headache, seizures, and focal neurological signs occurs in less than 30% of cases. [3] This diagnostic challenge, combined with potentially catastrophic consequences of missed diagnosis, makes CVST a critical "must-not-miss" condition in acute neurology and emergency medicine.
Diagnosis requires CT or MR venography—conventional CT brain is normal in up to 30% of cases. [4] Counterintuitively, anticoagulation remains the mainstay of treatment even in the presence of haemorrhagic infarction, as haemorrhage is secondary to venous congestion rather than arterial rupture. [5] With prompt diagnosis and anticoagulation, 80-90% of patients achieve good functional outcome, but mortality remains 5-10% and recurrence occurs in 5-15%. [6]
Key Facts
- Definition: Thrombosis of cerebral venous sinuses and/or cortical veins with impaired venous drainage
- Incidence: 1.3-1.6 per 100,000 adults per year; higher in pregnancy/postpartum (6-12 per 100,000 deliveries) [7]
- Peak Demographics: Young adults (median age 35-37 years); female predominance 3:1 due to hormonal factors [1,2]
- Common Locations: Superior sagittal sinus (60-70%), transverse sinus (40-50%), sigmoid sinus (30%), multiple sinuses involved in 50% [8]
- Pathognomonic Signs: Empty delta sign on contrast CT; cord sign on non-contrast CT; absent flow void on MR venography
- Gold Standard Investigation: MR venography (MRV) or CT venography (CTV)—both highly sensitive and specific [9]
- First-line Treatment: Therapeutic anticoagulation with LMWH transitioning to warfarin or DOAC [10]
- Prognosis: 80-90% good outcome (mRS 0-2); 5-10% mortality; 5-15% recurrence over 5 years [6]
Clinical Pearls
Diagnostic Pearl: Consider CVST in any young patient with headache PLUS one of: seizures, focal deficit, papilloedema, or risk factors (OCP, pregnancy/puerperium, thrombophilia, dehydration).
Treatment Pearl: Anticoagulation is safe and recommended even with haemorrhagic venous infarction—haemorrhage results from venous backpressure and capillary rupture, not arterial bleeding. Anticoagulation prevents thrombus propagation and improves venous drainage. [5]
Pitfall Warning: Normal CT brain does NOT exclude CVST. Up to 30% have normal initial CT. Always perform CT or MR venography if clinical suspicion exists. [4]
Imaging Pearl: Hyperdense cortical vein or sinus on non-contrast CT ("cord sign") may be the only clue. Contrast CT shows "empty delta sign"—central hypodensity in superior sagittal sinus surrounded by enhancing dura.
Mnemonic: CVST - Combined oral Contraceptive, Venogram needed, Safe to anticoagulate (even with haemorrhage), Thrombophilia workup
Why This Matters Clinically
CVST is a rare but treatable cause of stroke and raised intracranial pressure in young adults. Delayed diagnosis leads to preventable morbidity and mortality. The condition mimics many other disorders (migraine, idiopathic intracranial hypertension, arterial stroke, encephalitis), making clinical suspicion and appropriate imaging essential. Awareness of risk factors—particularly OCP use, pregnancy/postpartum state, and prothrombotic conditions—is critical for timely diagnosis. The counterintuitive safety of anticoagulation despite haemorrhage must be understood to avoid treatment delays that worsen outcomes.
2. Epidemiology
Incidence and Prevalence
- Overall incidence: 1.3-1.6 per 100,000 adults per year [7]
- All ages including children: 3-4 per 100,000 per year
- Neonatal period: Higher incidence (10-12 per 100,000 live births) [11]
- Pregnancy-associated: 6-12 per 100,000 deliveries [12]
- Postpartum period: 10-fold increased risk in first 6 weeks after delivery
- Accounts for: 0.5-1% of all strokes, but up to 10% of strokes in young adults [2]
Demographics
| Parameter | Value | Source |
|---|---|---|
| Median age | 35-37 years | [1,2] |
| Sex ratio (F:M) | 3:1 overall; 1:1 in absence of sex-specific risk factors | [1] |
| Geographic variation | Higher reported incidence in Middle East and Asia (may reflect diagnostic awareness) | [7] |
| Seasonal variation | Possible winter peak (dehydration, infection) | [13] |
Risk Factors
Hormonal and Reproductive (Account for Female Predominance)
| Factor | Relative Risk | Notes |
|---|---|---|
| Oral contraceptive pill | 5-20x | Most common acquired risk factor; dose-dependent [14] |
| Pregnancy | 3-7x | Risk highest in third trimester and puerperium |
| Postpartum period | 10-15x | Risk peaks in first 2-4 weeks, elevated up to 12 weeks [12] |
| Hormone replacement therapy | 2-4x | Lower risk than OCP |
| Ovarian hyperstimulation | Variable | Case reports; prothrombotic state |
Inherited Thrombophilia (Present in 20-35% of CVST Patients) [15]
| Condition | Frequency | Risk Increase |
|---|---|---|
| Factor V Leiden heterozygote | 10-15% | 3-5x |
| Prothrombin G20210A mutation | 5-10% | 5-10x |
| Protein C deficiency | 2-5% | 10-15x |
| Protein S deficiency | 2-5% | 5-10x |
| Antithrombin deficiency | 1-2% | 10-20x |
| MTHFR homozygosity | 5-10% | Unclear significance |
Acquired Thrombophilia
- Antiphospholipid syndrome: Present in 5-10% of CVST cases [16]
- Paroxysmal nocturnal haemoglobinuria: Rare but important cause
- Hyperhomocysteinaemia: Associated but causality unclear
Infection (10-15% of Cases, Higher in Developing Countries) [13]
| Site | Examples | Mechanism |
|---|---|---|
| Ear-sinus-mastoid | Otitis media, mastoiditis, sinusitis | Direct extension to adjacent sinuses (transverse, sigmoid) |
| CNS | Meningitis, brain abscess, subdural empyema | Inflammatory thrombosis |
| Systemic | Sepsis, endocarditis | Prothrombotic state, DIC |
Septic CVST: Results from direct extension of infection. Associated with worse prognosis. Requires prolonged antibiotics in addition to anticoagulation.
Inflammatory and Autoimmune Disorders
- Inflammatory bowel disease (Crohn's, ulcerative colitis): 1-2% of CVST cases [17]
- Systemic lupus erythematosus
- Behçet's disease: CVST is the most common neurological manifestation
- Sarcoidosis
- Granulomatosis with polyangiitis (Wegener's)
Malignancy (5-10% of Cases)
- Haematological: Polycythaemia vera, essential thrombocytosis, acute leukaemia
- Solid tumours: Direct invasion (meningioma, nasopharyngeal cancer) or hypercoagulability
- Paraneoplastic: Trousseau's syndrome
Mechanical and Iatrogenic
- Head trauma: Skull fracture involving venous sinuses
- Neurosurgery: Manipulation near venous sinuses
- Central venous catheterization: Internal jugular vein catheter
- Lumbar puncture: Rare; low CSF pressure may promote venous stasis
Haematological Disorders
- Polycythaemia vera: Hyperviscosity
- Essential thrombocytosis: Platelet-mediated thrombosis
- Sickle cell disease: Particularly sickle cell-beta thalassaemia
- Thrombotic thrombocytopenic purpura (TTP)
Medications and Substances
- L-asparaginase: Chemotherapy for ALL; depletes antithrombin
- Tamoxifen: Oestrogen receptor modulator
- Androgens and anabolic steroids
- Immunoglobulin therapy: High-dose IVIG
- Ecstasy (MDMA): Dehydration and prothrombotic effects
Other Risk Factors
- Dehydration: Particularly in hot climates or with diarrhoeal illness
- Hyperviscosity syndromes: Waldenstrom's macroglobulinaemia, multiple myeloma
- Nephrotic syndrome: Loss of anticoagulant proteins in urine
- Thyrotoxicosis: Prothrombotic state
Idiopathic CVST
- No identifiable cause: Found in 15-25% of cases after thorough investigation [1]
- May represent unidentified genetic or transient risk factors
- Management and outcomes similar to provoked CVST
3. Anatomy and Pathophysiology
Anatomy of the Cerebral Venous System
Dural Venous Sinuses
Superior Sagittal Sinus (SSS):
- Runs in superior border of falx cerebri from crista galli to internal occipital protuberance
- Drains parasagittal cerebral cortex via superior cortical veins
- Most commonly thrombosed sinus (60-70% of cases) [8]
- Thrombosis typically causes bilateral parasagittal infarction
Transverse Sinuses (Right and Left):
- Extend from confluence of sinuses (torcular Herophili) along posterior attachment of tentorium cerebelli
- Right often larger and dominant
- Second most common site (40-50%) [8]
- May thrombose secondary to mastoiditis or otitis media
Sigmoid Sinuses:
- Continuation of transverse sinuses, forming S-shaped curve
- Exit skull via jugular foramen to become internal jugular vein
- Thrombosis in 30% of cases, often with adjacent transverse sinus
Straight Sinus:
- Runs along junction of falx cerebri and tentorium cerebelli
- Drains deep cerebral veins
- Isolated thrombosis rare but devastating (deep venous system involvement)
Cavernous Sinuses (Bilateral):
- Lateral to pituitary fossa
- Contain internal carotid artery and cranial nerves III, IV, V1, V2, VI
- Thrombosis causes cavernous sinus syndrome: orbital pain, chemosis, proptosis, ophthalmoplegia
Deep Cerebral Veins:
- Internal cerebral veins, basal veins of Rosenthal, vein of Galen
- Drain deep white matter, basal ganglia, thalamus
- Thrombosis (10% of cases) causes bilateral thalamic infarction with poor prognosis [18]
Cortical Veins
Superficial cortical veins drain cerebral cortex into dural sinuses. Isolated cortical vein thrombosis causes localized cortical infarction, often haemorrhagic, with high seizure risk.
Pathophysiology
CVST pathophysiology differs fundamentally from arterial stroke, explaining unique clinical features and management.
Step 1: Thrombus Formation
Virchow's Triad applies:
- Endothelial injury: Infection, trauma, inflammation
- Venous stasis: Immobility, dehydration, pregnancy (mechanical compression)
- Hypercoagulability: OCP, thrombophilia, malignancy, pregnancy
Unlike arterial thrombosis (platelet-rich white clot), venous thrombosis produces fibrin-rich red clot. Thrombus begins in a sinus (commonly superior sagittal) and may propagate.
Step 2: Impaired Venous Drainage—Two Consequences
A. Raised Intracranial Pressure (ICP):
- Cerebral venous drainage is impaired
- CSF absorption at arachnoid granulations (which drain into venous sinuses) is reduced
- ICP rises progressively
- Clinical manifestation: Headache (90% of cases), papilloedema (30-80%), 6th nerve palsy (false localizing), visual obscurations
B. Venous Congestion in Affected Territory:
- Blood cannot drain from brain regions served by thrombosed sinus
- Capillary and venule backpressure increases
- Progresses to capillary leakage and rupture
Step 3: Venous Infarction
Cytotoxic Oedema:
- Impaired venous drainage causes tissue hypoxia
- Cellular energy failure
- Cytotoxic oedema develops
Vasogenic Oedema:
- Increased venous pressure disrupts blood-brain barrier
- Protein-rich fluid leaks into interstitium
- Vasogenic oedema develops
Haemorrhagic Transformation (Characteristic Feature of CVST):
- Elevated venous pressure causes capillary rupture
- Petechial haemorrhage within oedematous brain
- May coalesce into larger parenchymal haematoma
- Haemorrhagic infarction occurs in 30-40% of CVST cases [19]
- Distribution: Often bilateral, parasagittal (SSS), lobar (cortical veins), thalamic (deep veins)
Key concept: Haemorrhage is consequence of venous hypertension, NOT arterial rupture. This is why anticoagulation is safe—it reduces venous pressure by preventing thrombus propagation, improving drainage and reducing further haemorrhage risk. [5]
Step 4: Clinical Manifestations—Three Syndromes
Isolated Intracranial Hypertension (20-30%):
- Pure raised ICP without focal signs
- Headache, papilloedema, visual symptoms
- Mimics idiopathic intracranial hypertension
- Typically SSS thrombosis without infarction
Focal Syndrome (40-50%):
- Venous infarction causes focal deficits
- Hemiparesis, aphasia, visual field defects
- Seizures (40% of all CVST cases): Caused by cortical irritation from oedema/haemorrhage [20]
- May progress over hours-days (unlike sudden-onset arterial stroke)
Encephalopathy/Coma (15-20%):
- Diffuse cerebral dysfunction
- Bilateral large infarcts (SSS, deep veins)
- Massive cerebral oedema
- Coma, GCS less than 8
- Associated with worst prognosis [6]
Step 5: With Treatment—Recanalization
Anticoagulation Effects:
- Prevents thrombus propagation
- Allows endogenous fibrinolysis
- Promotes recanalization (occurs in 80-90% over weeks-months) [21]
- Development of venous collaterals
Natural history without treatment:
- Progressive thrombosis
- Worsening infarction
- Increased haemorrhage
- Cerebral herniation
- Death in 10-30% [1]
4. Clinical Presentation
Symptoms
Headache (85-95% of Cases) [3]
Characteristics:
- Most common presenting symptom
- Onset: Usually progressive over days-weeks (70%); acute/thunderclap in 15-20%; chronic (> 30 days) in 10%
- Quality: Non-specific—throbbing, constant, or pressure-like
- Location: Diffuse or focal (no reliable pattern)
- Severity: Often severe and unresponsive to analgesia
- Timing: Progressive worsening is characteristic
- Associated features: Worse with cough, Valsalva, lying flat (raised ICP features)
Red flags in headache assessment:
- Progressive despite analgesia
- Associated seizure, focal deficit, or papilloedema
- Postural component (worse lying down)
- Pregnancy or postpartum state
- Recent infection (ear, sinus, systemic)
- OCP use, especially with smoking
Visual Symptoms (20-30%)
- Transient visual obscurations (raised ICP affecting optic nerve perfusion)
- Blurred vision (papilloedema)
- Diplopia (6th nerve palsy from raised ICP—false localizing sign)
- Visual field defects (occipital lobe infarction)
- Permanent visual loss if papilloedema untreated (5-10%) [22]
Seizures (40% of Cases) [20]
- Incidence: 40% overall; higher with cortical involvement
- Type: Focal (60%), generalized (25%), status epilepticus (15%)
- Timing: At presentation (70%), during acute phase (20%), late (10%)
- Mechanism: Cortical irritation from oedema, haemorrhage, or ischaemia
- Prognostic significance: Seizures at presentation indicate cortical involvement but do not independently worsen prognosis
Focal Neurological Deficits (30-50%)
- Hemiparesis or hemiplegia (most common)
- Aphasia (dominant hemisphere involvement)
- Visual field defects (homonymous hemianopia)
- Hemisensory loss
- Ataxia (cerebellar involvement)
- Progression: Often stuttering/progressive over hours-days (unlike sudden arterial stroke)
Altered Consciousness (15-20%)
- Confusion and disorientation
- Drowsiness
- Coma (GCS less than 8)—poor prognostic indicator [6]
Other Symptoms
- Nausea and vomiting (associated with raised ICP)
- Photophobia (meningeal irritation)
- Tinnitus (pulsatile with raised ICP)
- Neck stiffness (meningeal irritation or SAH mimic)
Signs
Fundoscopy: Papilloedema (30-80% of Cases) [22]
Findings:
- Optic disc swelling and blurring of margins
- Engorged retinal veins
- Loss of venous pulsation
- Haemorrhages and cotton-wool spots (severe)
- May be absent in acute presentation (takes time to develop)
Focal Neurological Signs
- Hemiparesis (UMN pattern)
- Cranial nerve palsies (III, IV, VI if cavernous sinus; VI alone if raised ICP)
- Aphasia
- Neglect
- Visual field defects
- Cerebellar signs
Reduced Consciousness
- GCS less than 15: Indicates diffuse or severe involvement
- GCS less than 8: Associated with deep venous thrombosis or massive oedema—poor prognosis
Meningism
- Neck stiffness (15-20%)
- May occur with haemorrhagic infarction or infectious aetiology
- Can mimic meningitis or SAH
Signs Related to Aetiology
- Mastoid tenderness: Lateral sinus thrombosis from mastoiditis
- Orbital signs: Cavernous sinus syndrome (chemosis, proptosis, ophthalmoplegia)
- Fever: Septic CVST
- Skin/joint findings: Underlying systemic disease (SLE, Behçet's)
Presentation Patterns (Clinical Syndromes)
| Syndrome | Frequency | Features | Typical Sinus Involved |
|---|---|---|---|
| Isolated intracranial hypertension | 20-30% | Headache, papilloedema, visual symptoms; no focal signs or seizures | Superior sagittal sinus (without infarction) |
| Focal syndrome | 40-50% | Focal deficits, seizures, +/- headache | Any sinus with parenchymal involvement |
| Encephalopathy | 15-20% | Confusion, reduced GCS, coma; diffuse cerebral dysfunction | Deep venous system, extensive SSS, or multifocal |
| Cavernous sinus syndrome | less than 5% | Orbital pain, chemosis, proptosis, CN III/IV/VI palsies, Horner's | Cavernous sinus |
| Subacute/chronic | 10-15% | Progressive headache over weeks-months, mimics IIH | SSS (partial occlusion) |
Atypical Presentations
- Thunderclap headache: 10-15% present with sudden-onset severe headache mimicking SAH [3]
- Isolated psychiatric symptoms: Confusion, psychosis without clear focal signs
- Stroke mimic: Transient neurological deficit (venous TIA concept emerging)
- Pseudotumour cerebri mimic: Chronic headache with papilloedema, normal imaging (only visible on venography)
Red Flags Warranting Urgent Imaging
[!CAUTION] CVST Red Flags
- Thunderclap headache in any patient
- Headache + seizure (consider CVST before labelling as primary seizure disorder)
- Headache + focal neurological deficit in young adult (especially if OCP, pregnancy)
- Headache in pregnancy/postpartum (especially first 6 weeks postpartum)
- Progressive headache despite analgesia
- Papilloedema with headache
- Headache + altered consciousness
- Bilateral deficits or deficits that cross vascular territories
5. Clinical Examination
Neurological Assessment
General Inspection and Vital Signs
Consciousness Level:
- GCS assessment mandatory
- Alert (GCS 15): Good prognosis
- Drowsy (GCS 9-14): Concerning, indicates raised ICP or encephalopathy
- Coma (GCS less than 8): Poor prognosis, ICU required [6]
Vital Signs:
- Blood pressure: Often elevated (Cushing's response to raised ICP)
- Fever: Suggests septic CVST
- Respiratory pattern: Cheyne-Stokes or irregular breathing (severe raised ICP)
Meningism:
- Neck stiffness: Present in 15-20%, especially with haemorrhagic infarction
- Kernig's and Brudzinski's signs
Cranial Nerve Examination
Eyes (Critical in CVST Assessment):
Fundoscopy (essential examination):
- Papilloedema: Swollen optic disc, blurred margins, loss of central cup
- Retinal haemorrhages
- Engorged veins
- Absence of papilloedema does not exclude CVST: May not develop acutely
Pupils:
- Equal and reactive: Normal
- Unilateral dilated fixed pupil: Uncal herniation (medical emergency)
Eye movements:
- 6th nerve palsy (failure of abduction): False localizing sign of raised ICP
- III, IV, VI palsies with proptosis: Cavernous sinus thrombosis
Visual fields:
- Homonymous hemianopia: Occipital infarction
- Enlarged blind spot: Papilloedema
Visual acuity:
- Reduced: Papilloedema or occipital involvement
Other Cranial Nerves:
- VII palsy: Cortical or pontine involvement
- Lower cranial nerves rarely affected unless jugular foramen thrombosis
Motor Examination
- Hemiparesis: UMN pattern (increased tone, hyperreflexia, extensor plantar)
- Distribution: May be bilateral if parasagittal infarction (SSS involvement)
- Progression: May worsen over examination period (unlike arterial stroke)
Sensory Examination
- Hemisensory loss (cortical or thalamic)
- Bilateral sensory loss suggests deep venous thrombosis
Coordination and Gait
- Ataxia: Cerebellar involvement
- Gait assessment if safe: Often impaired by weakness or ataxia
Cognitive Assessment
- Orientation to time, place, person
- Memory: Bilateral thalamic infarction causes severe amnesia
- Language: Aphasia if dominant hemisphere cortical involvement
- Attention and executive function: Impaired with frontal involvement
Examination for Underlying Cause
Local Causes
Ear, Nose, Throat:
- Mastoid tenderness: Mastoiditis with lateral sinus thrombosis
- Ear discharge: Otitis media
- Sinus tenderness: Sinusitis
Orbital Examination:
- Chemosis (conjunctival oedema): Cavernous sinus thrombosis
- Proptosis: Cavernous sinus thrombosis
- Periorbital oedema
Systemic Examination
Skin:
- Livedo reticularis: Antiphospholipid syndrome
- Oral/genital ulcers: Behçet's disease
- Photosensitive rash: SLE
- Erythema nodosum: Behçet's, IBD, sarcoidosis
Cardiovascular:
- Murmurs: Endocarditis (septic emboli)
- Atrial fibrillation: Embolic stroke (arterial) differential
Abdomen:
- Hepatosplenomegaly: Myeloproliferative disorder, malignancy
Musculoskeletal:
- Arthritis: SLE, Behçet's
Evidence of Dehydration:
- Dry mucous membranes, reduced skin turgor
- Particularly important in hot climates or after diarrhoeal illness
6. Differential Diagnosis
CVST is a "great mimic" due to variable presentation. Differential diagnosis depends on presentation pattern.
For Headache-Predominant Presentation
| Differential | Key Distinguishing Features | Definitive Test |
|---|---|---|
| Migraine | Episodic, family history, typical aura, response to triptans; no papilloedema | Clinical; MRV if red flags |
| Idiopathic intracranial hypertension | Young obese women, chronic headache, papilloedema, normal MRI brain; can be identical to CVST | MRV to exclude CVST (IIH is diagnosis of exclusion) |
| Subarachnoid haemorrhage | Thunderclap onset, neck stiffness, no papilloedema | CT brain, LP if CT negative |
| Meningitis/encephalitis | Fever, meningism, rapid progression, CSF pleocytosis | CSF analysis |
| Posterior reversible encephalopathy syndrome (PRES) | Hypertension, posterior headache, visual symptoms, reversible posterior white matter oedema | MRI brain (venography normal) |
| Giant cell arteritis | Age greater than 50, jaw claudication, temporal artery tenderness, raised ESR/CRP | ESR, CRP, temporal artery biopsy |
For Stroke-Like Presentation (Focal Deficit)
| Differential | Key Distinguishing Features | Definitive Test |
|---|---|---|
| Arterial ischaemic stroke | Sudden onset, arterial territory, no haemorrhage typically, older age | CT/MRI brain, CT/MR angiography (arterial) |
| Intracerebral haemorrhage | Sudden onset, hypertension, no venous pattern | CT brain |
| Brain tumour | Subacute progression, mass lesion with surrounding oedema, midline shift | MRI brain with contrast |
| Brain abscess | Fever, ring-enhancing lesion, history of infection/immunosuppression | MRI with contrast, blood cultures |
| Demyelination (MS, ADEM) | Younger age, relapsing-remitting, white matter lesions, CSF oligoclonal bands | MRI brain, CSF analysis |
| Hemiplegic migraine | Family history, recurrent episodes with full recovery, aura | Clinical diagnosis of exclusion |
For Seizure-Predominant Presentation
| Differential | Key Distinguishing Features |
|---|---|
| Primary epilepsy | Recurrent seizures, normal imaging, no headache/papilloedema |
| Arterial stroke | Sudden onset, arterial territory, seizures less common (10%) |
| CNS infection | Fever, meningism, CSF abnormalities |
| Autoimmune encephalitis | Psychiatric features, movement disorders, antibody-positive |
Key point: New-onset seizure in adult with headache or risk factors (OCP, pregnancy) warrants MR venography.
For Encephalopathy Presentation
| Differential | Key Distinguishing Features |
|---|---|
| Meningoencephalitis | Fever, CSF pleocytosis, PCR positive |
| Metabolic encephalopathy | Systemic illness, laboratory abnormalities, diffuse slowing on EEG |
| Toxic encephalopathy | Drug/toxin exposure history |
| Autoimmune encephalitis | Antibodies (NMDA-R, LGI1, etc.), inflammatory CSF |
Cavernous Sinus Syndrome Differentials
| Condition | Features |
|---|---|
| Cavernous sinus thrombosis | Acute, orbital pain, chemosis, proptosis, CN III/IV/VI palsies, may be septic |
| Carotid-cavernous fistula | Pulsatile proptosis, bruit, conjunctival injection |
| Tolosa-Hunt syndrome | Painful ophthalmoplegia, steroid-responsive, granulomatous inflammation |
| Orbital cellulitis | Infection, fever, reduced vision, may progress to cavernous thrombosis |
7. Investigations
Imaging—Essential for Diagnosis
CT Brain (Non-Contrast)
Role: First-line emergency investigation; normal in up to 30% of CVST cases. [4]
Direct Signs of Thrombosis:
- Cord sign: Hyperdense cortical vein or sinus (thrombosed vein appears bright due to acute clot)
- "Sensitivity: 20-30%"
- Highly specific when present
- Dense triangle sign: Hyperdense superior sagittal sinus on axial view
- May be normal variant (high haematocrit) so low specificity alone
Indirect Signs of Venous Infarction:
- Haemorrhagic infarction: Most characteristic finding (30-40%)
- Multiple bilateral lesions not conforming to arterial territories
- Parasagittal (SSS), temporal (transverse sinus), thalamic (deep veins)
- Cerebral oedema: Diffuse or lobar, may have mass effect
- Subarachnoid haemorrhage: Cortical SAH can occur
Pitfall: Normal CT brain does NOT exclude CVST. Always proceed to venography if suspicion exists.
CT Venography (CTV)
Gold standard for acute diagnosis. [9]
Technique:
- IV contrast administration with venous phase imaging (delayed 60-80 seconds)
- 3D reconstruction helpful for visualizing sinus anatomy
Findings:
- Filling defect in dural sinus (thrombus appears as dark area within contrast-enhanced sinus)
- Empty delta sign: Triangular filling defect in SSS on axial imaging (central thrombus with peripheral enhancement of collateral veins and dural margin)
- Absence of normal flow in affected sinus
Advantages:
- Rapid (minutes), widely available in emergency setting
- High sensitivity (95%) and specificity (95%) [9]
- Good for acute presentation
Disadvantages:
- Ionizing radiation
- Iodinated contrast (contraindicated in renal impairment, contrast allergy)
- Less sensitive for cortical vein thrombosis alone
MR Venography (MRV)
Gold standard overall; slightly more sensitive than CTV, especially for cortical veins. [9]
Techniques:
- 2D time-of-flight (TOF) MRV: No contrast, detects flow void loss
- Contrast-enhanced MRV: Gadolinium contrast, better delineation
- SWI (susceptibility-weighted imaging): Detects haemorrhage and deoxyhemoglobin in thrombus
Findings:
- Absence of flow void in affected sinus
- Filling defect on contrast-enhanced sequences
- Thrombus signal characteristics: Variable depending on age (T1/T2 changes)
Advantages:
- No ionizing radiation
- Better for cortical vein thrombosis
- Can assess chronicity based on signal characteristics
- Concurrent MRI brain provides detailed parenchymal assessment
Disadvantages:
- Slower (30-60 minutes), less available in emergency
- Contraindicated with some implants (pacemakers, some aneurysm clips)
- Motion artifact in agitated patients
- Flow artifacts can mimic thrombosis (hypoplastic sinus, slow flow)
MRI Brain (Parenchymal Imaging)
Performed alongside MRV to assess consequences of thrombosis.
Findings:
- Venous infarction: Non-arterial distribution, often haemorrhagic
- Bilateral parasagittal (SSS)
- Temporal lobe (transverse sinus)
- Thalamic (deep veins)
- Haemorrhage: Petechial or confluent
- Oedema: Cytotoxic (restricted diffusion on DWI) and vasogenic
- Mass effect: Midline shift, herniation risk
Sequences:
- T1: Thrombus may be hyperintense (subacute)
- T2/FLAIR: Oedema, infarction
- DWI: Variable restriction (venous infarcts less restricted than arterial)
- GRE/SWI: Haemorrhage highly visible
- T1 post-contrast: Empty delta sign
CT Brain with Contrast
Not routinely performed if CTV available, but can show:
- Empty delta sign: Classic finding on contrast-enhanced axial CT
- Triangular filling defect in SSS
- Central thrombus surrounded by enhancing dura and collateral veins
Catheter Angiography (Digital Subtraction Angiography)
Rarely performed for diagnosis (CTV/MRV sufficient).
Indications:
- Pre-procedural planning for endovascular intervention
- Unclear diagnosis on non-invasive imaging
Findings:
- Absence of sinus opacification
- Delayed venous drainage
- Collateral venous pathways
Laboratory Investigations
Urgent (Emergency Department)
| Test | Purpose | Expected Findings |
|---|---|---|
| Full blood count | Polycythaemia, thrombocytosis, thrombocytopenia | Hb, platelets may be abnormal |
| Coagulation screen | Baseline for anticoagulation; DIC screen | PT, APTT usually normal unless DIC |
| D-dimer | Non-specific but very high levels supportive | Elevated in 90%, but low specificity [4] |
| Renal function | Baseline for contrast studies and medications | Urea, creatinine |
| Liver function | Baseline for anticoagulation monitoring | ALT, AST, bilirubin |
| Inflammatory markers | Infection, vasculitis | ESR, CRP elevated in septic CVST or inflammatory causes |
| Pregnancy test | Exclude pregnancy | Essential in women of childbearing age |
| Blood cultures | If septic CVST suspected | Positive in bacterial infection |
| Glucose | Exclude hypoglycaemia as mimic | Normal or elevated |
D-dimer: Elevated in 90% of CVST cases, but normal D-dimer does not exclude CVST (10% have normal levels). [4] Low specificity (elevated in many conditions). Useful if low clinical suspicion to support decision NOT to image, but high suspicion warrants imaging regardless of D-dimer.
Thrombophilia Workup (After Acute Phase)
Timing: Should be performed at least 2 weeks after acute event and ideally 3-6 months after stopping anticoagulation to avoid false results. [15]
| Test | Purpose |
|---|---|
| Factor V Leiden mutation | Most common hereditary thrombophilia (10-15% of CVST) |
| Prothrombin G20210A mutation | Second most common (5-10%) |
| Protein C activity/level | Hereditary deficiency (anticoagulation reduces levels) |
| Protein S activity/level | Hereditary deficiency (anticoagulation reduces levels) |
| Antithrombin activity | Hereditary deficiency |
| Antiphospholipid antibodies | Lupus anticoagulant, anticardiolipin IgG/IgM, anti-β2-glycoprotein I IgG/IgM |
| Homocysteine level | Hyperhomocysteinaemia (controversial significance) |
| MTHFR mutation | Common but unclear clinical significance |
Repeat testing: Antiphospholipid antibodies must be positive on two occasions 12 weeks apart for diagnosis of APS. [16]
Caveat: Acute thrombosis and anticoagulation alter protein C, protein S, and antithrombin levels. Genetic testing (Factor V Leiden, prothrombin mutation) is unaffected and can be done acutely.
Other Investigations Based on Clinical Context
| Clinical Scenario | Additional Tests |
|---|---|
| Suspected malignancy | Myeloproliferative workup: JAK2 mutation, bone marrow biopsy |
| Suspected inflammatory disease | ANA, ENA, ANCA, complement, ACE level |
| Suspected PNH | Flow cytometry for CD55/CD59 |
| Suspected infection | Specific cultures, serologies based on site |
| Suspected hyperviscosity | Serum protein electrophoresis, immunoglobulins |
Lumbar Puncture
Not routinely indicated for CVST diagnosis.
Indications:
- Exclude meningitis/encephalitis when differential diagnosis unclear
- Document opening pressure if IIH-like presentation
- Therapeutic LP for vision-threatening raised ICP (after imaging excludes mass effect)
Contraindications:
- Mass effect on imaging (herniation risk)
- Large haemorrhage
- Coagulopathy
Findings in CVST (if performed):
- Opening pressure: Often elevated (greater than 25 cmH2O)
- CSF analysis: Usually normal or non-specific
- Mildly elevated protein (50-100 mg/dL) in 50%
- Mild lymphocytic pleocytosis (less than 50 cells) in 10-15%
- RBCs if haemorrhagic infarction
- Normal glucose (helps distinguish from meningitis)
Caveat: LP can precipitate herniation if significant mass effect present. Always image first.
Electroencephalography (EEG)
Not diagnostic for CVST but may be performed for:
- Evaluation of seizures
- Monitoring in ICU if sedated
- Detecting non-convulsive status epilepticus
Findings: Non-specific focal or generalized slowing; epileptiform activity if seizures occurred.
8. Classification and Severity Assessment
Anatomical Classification
CVST is classified by site of thrombosis:
| Site | Frequency | Clinical Features | Prognosis |
|---|---|---|---|
| Superior sagittal sinus | 60-70% | Bilateral parasagittal deficits, seizures, raised ICP | Good if no infarction; moderate if infarction |
| Transverse sinus | 40-50% | Headache, lateral signs, mastoiditis association | Good |
| Sigmoid sinus | 30% | Often with transverse; similar features | Good |
| Straight sinus | 10-20% | Deep venous involvement, impaired consciousness | Poor |
| Deep venous system | 10% | Bilateral thalamic infarction, severe encephalopathy, coma | Poor [18] |
| Cortical veins only | 10-15% | Focal seizures, localized deficit/oedema | Good with treatment |
| Cavernous sinus | less than 5% | Orbital pain, chemosis, CN III/IV/VI palsy | Variable; worse if septic |
| Multiple sinuses | 50% | Variable; more extensive often worse | Depends on extent |
Prognostic Scores
CVST Prognostic Score (Dutch Study) [6]
Predicts poor outcome (mRS 3-6 at 6 months or death).
Risk Factors for Poor Prognosis:
- Coma (GCS less than 9): Strongest predictor
- Mental status disorder (confusion, encephalopathy)
- Deep cerebral venous system thrombosis
- Intracranial haemorrhage on admission CT
- Posterior fossa lesion
- Malignancy
- CNS infection (septic CVST)
- Age greater than 37 years
Outcome by number of risk factors:
- 0-1 risk factors: 5-10% poor outcome
- 2 risk factors: 25% poor outcome
- 3 or more risk factors: Greater than 40% poor outcome
Severity Classification
| Severity | Features | Management Level |
|---|---|---|
| Mild | Headache, no focal signs, no impaired consciousness, isolated raised ICP | Ward, neurology |
| Moderate | Focal deficits, seizures (controlled), alert | Ward/HDU, neurology |
| Severe | GCS less than 8, status epilepticus, massive oedema, deep venous thrombosis | ICU, neurocritical care |
9. Management
Initial Management—Emergency Department/Acute Neurology
Resuscitation and Stabilization
Airway, Breathing, Circulation:
- Airway protection if GCS less than 8 (intubation)
- Oxygen to maintain SpO2 greater than 94%
- IV access: Two large-bore cannulas
Immediate Interventions:
- Seizure management: If actively seizing—lorazepam 4 mg IV, then levetiracetam 1500 mg IV load or phenytoin 20 mg/kg IV
- Raised ICP management (if signs of herniation): Head elevation 30°, IV mannitol 20% 0.5-1 g/kg or hypertonic saline 3% bolus
- Glucose: Check and correct if low
Diagnostic Imaging (Urgent)
- CT brain non-contrast: Immediate (rule out haemorrhage, mass lesion; may show CVST signs)
- CT or MR venography: Urgent (within hours)—diagnostic test
Initiation of Anticoagulation
Start as soon as diagnosis confirmed on venography. [5,10]
First-line: Low Molecular Weight Heparin (LMWH):
- Enoxaparin 1 mg/kg subcutaneous twice daily (therapeutic dose)
- Dalteparin 200 units/kg subcutaneous once daily (alternative)
Alternative: Unfractionated Heparin (UFH):
- Indicated if:
- High bleeding risk (need for rapid reversal)
- Renal impairment (CrCl less than 30 mL/min)
- Anticipated procedure (neurosurgery)
- Dosing: IV bolus 80 units/kg, then infusion 18 units/kg/hr, titrate to APTT 1.5-2.5x control
Critical point: Anticoagulation is safe and recommended even with haemorrhagic infarction. [5]
- Haemorrhage is consequence of venous hypertension, not arterial rupture
- Anticoagulation prevents thrombus propagation, reduces venous pressure, and decreases further haemorrhage risk
- Meta-analyses confirm safety [5]
- Contraindication: Massive intracerebral haematoma with mass effect requiring evacuation (rare)
Medical Management—Ward/ICU
Anticoagulation Continuation and Transition
Acute phase (first 7-14 days):
- Continue LMWH or UFH
- Monitor platelet count (HIT risk with UFH)
- No APTT monitoring needed with LMWH
Transition to oral anticoagulation:
- Start warfarin after 5-7 days of LMWH, overlap until INR 2-3 for 2 consecutive days
- Direct oral anticoagulants (DOACs): Emerging evidence supports use (dabigatran, rivaroxaban, apixaban). [10]
- May be preferred for long-term compliance (no INR monitoring)
- Less evidence than warfarin in CVST but growing data
- Avoid if severe renal impairment
Target INR on warfarin: 2-3
Duration of anticoagulation: [10]
| Scenario | Duration | Rationale |
|---|---|---|
| Provoked by reversible risk factor (e.g., OCP, infection, dehydration, transient risk) | 3-6 months | Risk factor removed; low recurrence |
| Unprovoked or mild thrombophilia (heterozygous Factor V Leiden, prothrombin mutation) | 6-12 months | Moderate recurrence risk |
| Severe thrombophilia (homozygous Factor V, protein C/S/antithrombin deficiency, APS) | Lifelong | High recurrence risk [15] |
| Recurrent CVST | Lifelong | Very high recurrence risk |
| Active malignancy | LMWH for duration of active malignancy, then reassess | LMWH superior to warfarin in cancer |
Management of Raised Intracranial Pressure
Non-invasive measures:
- Head elevation: 30-45° (optimizes venous drainage)
- Avoid neck compression: Collar, tight tube ties
- Maintain normocapnia: PaCO2 4.5-5.0 kPa (hyperventilation only for acute herniation)
- Maintain euvolaemia: Avoid dehydration (worsens thrombosis) and fluid overload
Pharmacological:
- Acetazolamide: 500 mg-1 g twice daily if IIH-like picture (isolated raised ICP without mass effect)
- Reduces CSF production
- Monitor for metabolic acidosis, electrolyte disturbance
Therapeutic lumbar puncture:
- If vision-threatening papilloedema despite medical therapy
- Remove 20-30 mL CSF to reduce opening pressure to less than 20 cmH2O
- May need repeated LPs or LP shunt
- Only if no mass effect on imaging
Osmotic therapy (acute raised ICP/herniation):
- Mannitol 20%: 0.5-1 g/kg IV over 15 minutes, repeat every 6 hours as needed
- Hypertonic saline 3%: 150 mL bolus or continuous infusion
- Monitor serum osmolality (target less than 320 mOsm/kg)
Neurosurgical intervention (severe refractory raised ICP):
- Decompressive craniectomy: Life-saving in malignant cerebral oedema with herniation risk
- Remove bone flap to allow brain swelling
- Indicated if GCS declining despite maximal medical therapy
- Improved survival but variable neurological outcome [22]
Seizure Management
Acute seizures:
- Lorazepam: 4 mg IV (repeat once after 10 minutes if needed)
- Levetiracetam: 1500-3000 mg IV load, then 500-1500 mg twice daily
- Phenytoin: 20 mg/kg IV load if levetiracetam unavailable (slower, more side effects)
- Status epilepticus protocol if seizures persist greater than 5 minutes
Prophylactic anticonvulsants:
- Not routinely recommended in absence of seizures [20]
- Consider if high seizure risk: Large cortical involvement, haemorrhagic infarction
- If used, levetiracetam preferred (no drug interactions with anticoagulation)
Duration if seizures occurred:
- Treat for 6-12 months after last seizure
- Taper if seizure-free and imaging improved
- Recurrence risk moderate; individualize decision
Supportive Care
Analgesia:
- Severe headache common: Paracetamol, codeine, opiates as needed
- NSAIDs: Use cautiously (bleeding risk on anticoagulation, but not contraindicated for short courses)
Antiemetics:
- Ondansetron, metoclopramide for nausea/vomiting
Thromboprophylaxis for arterial events:
- Not routinely given (venous, not arterial, thrombotic disorder)
- LMWH for CVST provides venous and arterial protection
Nutrition and hydration:
- IV fluids if unable to take orally; avoid dehydration (worsens thrombosis)
- NG feeding if swallow unsafe
Physiotherapy:
- Early mobilization when safe (reduces DVT risk)
- Stroke rehabilitation if deficits present
Endovascular Treatment
Indications (limited evidence; consider in severe cases): [21]
- Clinical deterioration despite anticoagulation
- Coma or progressive neurological decline
- Extensive thrombosis with impending herniation
Techniques:
- Mechanical thrombectomy: Catheter-directed aspiration or retrieval of thrombus
- Local thrombolysis: Catheter-directed urokinase or tPA into thrombosed sinus
- Combination: Mechanical + pharmacological
Evidence:
- TO-ACT trial (2020): Randomized trial stopped early for futility; no benefit of endovascular treatment over anticoagulation alone in most patients. [21]
- Endovascular may still be considered in catastrophic cases, but not standard
Risks:
- Bleeding (ICH, systemic)
- Sinus perforation
- Rebleeding into infarct
Current practice: Reserved for exceptional cases; anticoagulation is standard.
Treatment of Underlying Cause
| Cause | Specific Management |
|---|---|
| Oral contraceptive pill | Stop immediately and permanently; switch to non-hormonal contraception |
| Pregnancy/postpartum | LMWH throughout pregnancy and 6 weeks postpartum minimum; warfarin contraindicated in pregnancy |
| Infection (septic CVST) | IV antibiotics (4-6 weeks), source control (mastoidectomy if mastoiditis), continue anticoagulation despite infection |
| Inflammatory disease | Immunosuppression as per underlying condition (steroids, DMARDs) |
| Malignancy | Treat malignancy; LMWH preferred over warfarin |
| Polycythaemia/thrombocytosis | Cytoreductive therapy, aspirin |
Special Populations
Pregnancy
- LMWH is safe in pregnancy (does not cross placenta)
- Warfarin is teratogenic: Contraindicated in pregnancy (especially first trimester)
- DOACs: Insufficient safety data; avoid
- Delivery planning: Discontinue LMWH 24 hours before planned delivery; may use UFH (short half-life) near term
- Postpartum anticoagulation: Resume LMWH or start warfarin (warfarin safe in breastfeeding)
Children and Neonates
- CVST accounts for greater incidence in neonates (perinatal complications)
- Anticoagulation often used but evidence limited
- Specialist paediatric neurology input essential
Elderly
- Higher bleeding risk on anticoagulation
- Consider falls risk assessment
- Adjust doses for renal impairment
Disposition
| Severity | Disposition |
|---|---|
| Mild (headache, no focal signs, alert) | Neurology ward, telemetry if seizure risk |
| Moderate (focal signs, controlled seizures) | Neurology ward or high-dependency unit |
| Severe (coma, status, massive oedema) | Neurocritical care ICU, ICP monitoring if indicated |
Follow-Up
Acute phase (first 2 weeks):
- Daily neurological assessment
- Repeat imaging at 5-7 days to assess infarct evolution, rebleeding
- Platelet monitoring if on UFH (HIT risk)
Subacute (2-12 weeks):
- Neurology clinic at 4-6 weeks
- Repeat MRV at 3-6 months to assess recanalization
- Thrombophilia workup (ideally 2 weeks post-event, off anticoagulation if possible)
Long-term (greater than 3 months):
- Consider stopping anticoagulation at appropriate duration (3-12 months depending on cause)
- Counsel regarding recurrence risk and warning signs
- Women: Avoid combined hormonal contraception lifelong; counsel regarding pregnancy risk
- Seizure risk: Driving restrictions as per local guidelines (UK: cannot drive until seizure-free for 12 months)
10. Complications
Acute Complications (During Admission)
| Complication | Incidence | Mechanism | Management |
|---|---|---|---|
| Haemorrhagic transformation | 30-40% [19] | Venous hypertension causing capillary rupture | Continue anticoagulation (counterintuitive but correct) [5] |
| Seizures | 40% [20] | Cortical irritation from oedema/haemorrhage | Lorazepam, levetiracetam; treat acutely, consider short-term prophylaxis |
| Status epilepticus | 5-10% | Severe cortical involvement | Benzodiazepines, phenytoin/levetiracetam, anaesthesia if refractory |
| Cerebral oedema and herniation | 5-10% | Mass effect from infarction/haemorrhage | Osmotic therapy, decompressive craniectomy if severe [22] |
| Visual loss (permanent) | 5-10% [22] | Papilloedema causing optic atrophy | Acetazolamide, therapeutic LP, optic nerve sheath fenestration |
| Hydrocephalus | less than 5% | Impaired CSF absorption or obstruction | VP shunt if symptomatic |
| Recurrent thrombosis (during acute phase) | less than 5% | Inadequate anticoagulation or prothrombotic state | Ensure therapeutic anticoagulation, consider thrombophilia |
| Venous infarct extension | 10-15% | Thrombus propagation | Ensure anticoagulation; consider endovascular if deteriorating |
| Death | 5-10% [6] | Massive oedema, herniation, underlying malignancy | Intensive care, decompressive surgery, treat cause |
Anticoagulation-Related Complications
| Complication | Incidence | Management |
|---|---|---|
| Major haemorrhage (ICH expansion, systemic) | less than 5% | Stop anticoagulation temporarily; reverse if life-threatening (protamine for heparin, vitamin K/PCC for warfarin); resume when safe |
| Minor bleeding (epistaxis, bruising) | 10-20% | Reassurance; local measures; continue anticoagulation |
| Heparin-induced thrombocytopenia (HIT) | 1-3% with UFH | Stop heparin; switch to alternative anticoagulant (argatroban, fondaparinux) |
Long-Term Complications (Post-Discharge)
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Recurrent CVST | 5-15% over 5 years [6] | Appropriate anticoagulation duration; lifelong if severe thrombophilia [15] |
| Epilepsy (recurrent seizures) | 10-15% | Anticonvulsants if seizures occurred; titrate based on seizure control |
| Persistent headache | 10-20% | Exclude recurrent thrombosis; treat as chronic headache (amitriptyline, topiramate) |
| Cognitive impairment | 10-20% | Rehabilitation, cognitive therapy |
| Motor deficits (hemiparesis) | 5-10% persist | Physiotherapy, occupational therapy, stroke rehabilitation |
| Venous hypertension (from non-recanalized sinus) | Variable | Usually asymptomatic; collaterals develop |
| Post-thrombotic syndrome (venous) | Rare in cerebral veins | Not well-defined for CVST |
Prognostic Indicators for Complications
Risk factors for poor outcome (death or severe disability): [6]
- Coma (GCS less than 9) at presentation
- Deep venous system thrombosis
- Large ICH with mass effect
- Malignancy
- CNS infection
- Age greater than 37 years
Good prognostic features:
- Alert at presentation
- Isolated raised ICP syndrome
- Lateral sinus thrombosis
- Young age
- Provoked by reversible risk factor (OCP, infection)
11. Prognosis
Short-Term Outcomes (At Discharge)
- Complete recovery or minor deficit (mRS 0-2): 60-70%
- Moderate disability (mRS 3-4): 15-20%
- Severe disability or death (mRS 5-6): 10-15%
- Mortality: 5-10% (higher in coma, deep venous thrombosis, malignancy) [6]
Long-Term Outcomes (6-12 Months)
- Complete recovery or minor deficit (mRS 0-2): 80-90% [6]
- Moderate-severe disability (mRS 3-5): 10-15%
- Death: 5-10%
Key point: Most patients (80-90%) achieve good functional outcome with treatment. Prognosis is better than arterial stroke of equivalent severity.
Recurrence Risk
- Overall recurrence rate: 5-15% over 5 years [6]
- Time to recurrence: Highest in first year (50% of recurrences), then plateaus
- Risk factors for recurrence:
- "Severe hereditary thrombophilia (protein C/S deficiency, antithrombin deficiency, homozygous Factor V Leiden): 10-25% [15]"
- "Antiphospholipid syndrome: 15-20% [16]"
- "Unprovoked CVST: 10%"
- "Provoked by reversible risk (OCP, infection): Less than 5%"
Prevention: Appropriate anticoagulation duration based on risk factors. Lifelong anticoagulation if severe thrombophilia or APS.
Recanalization
- Complete or partial recanalization: 80-90% by 6-12 months [21]
- Timing: Progressive over weeks-months
- Collateral development: Venous collaterals develop, often allowing normal function despite persistent occlusion
- Correlation with outcome: Recanalization associated with better outcome, but many patients do well even without complete recanalization due to collaterals
Functional Recovery
Timeline:
- First 2 weeks: Acute phase; may worsen initially then stabilize with anticoagulation
- 1-3 months: Most rapid recovery; deficits improve
- 3-12 months: Continued gradual improvement; neuroplasticity
- After 12 months: Residual deficits usually permanent but adaptive strategies improve function
Rehabilitation: Stroke rehabilitation principles apply—physiotherapy, occupational therapy, speech therapy as needed.
Pregnancy Outcomes in Future Pregnancies
- Women with history of CVST can have future pregnancies
- Risk of recurrence in pregnancy: Approximately 2-7% [12]
- Management in pregnancy:
- Prophylactic LMWH throughout pregnancy and 6 weeks postpartum
- Some advocate surveillance only if CVST was provoked by OCP (not pregnancy)
- Individualize based on thrombophilia status
- Obstetric risks: Slightly increased risk of pregnancy complications (pre-eclampsia, IUGR) if thrombophilia present, but most pregnancies successful
Quality of Life
- Most patients return to baseline activities
- Persistent headache in 10-20% (may be chronic daily headache)
- Fatigue and subtle cognitive deficits reported in some patients despite mRS 0-1
- Anxiety regarding recurrence common; reassurance important
Mortality Predictors
Independent predictors of death: [6]
- Coma at presentation (GCS less than 9)
- Deep venous system thrombosis
- Posterior fossa lesion
- Malignancy
- CNS infection (septic CVST)
- Age greater than 37 years
Causes of death:
- Transtentorial herniation (most common acute cause)
- Brainstem infarction (deep venous thrombosis)
- Underlying malignancy
- Sepsis (if septic CVST)
- Complications of treatment (rare: major haemorrhage)
12. Prevention and Screening
Primary Prevention
Avoidance of modifiable risk factors:
- Hormonal contraception: Avoid combined OCP in high-risk women (known thrombophilia, prior VTE, family history of VTE)
- Use progesterone-only contraception or non-hormonal methods
- Hydration: Adequate fluid intake, particularly in hot climates or during illness
- Infection treatment: Prompt treatment of ear, sinus infections to prevent septic CVST
Secondary Prevention (Preventing Recurrence)
Anticoagulation:
- Appropriate duration based on risk factors (see Management section)
- Lifelong if severe thrombophilia, APS, or recurrent CVST [15]
Risk factor modification:
- Stop OCP permanently after CVST
- Treat underlying inflammatory/autoimmune disease
- Control myeloproliferative disorders (hydroxyurea, aspirin)
- Address modifiable cardiovascular risk factors (smoking, hypertension, diabetes)
Thrombophilia counselling:
- If hereditary thrombophilia identified, family screening may be indicated
- Genetic counselling regarding recurrence risk
Pregnancy planning:
- Women with prior CVST: Prophylactic LMWH in future pregnancies [12]
- Pre-pregnancy counselling with haematology/high-risk obstetrics
Screening
No population screening for CVST (too rare).
Screening for thrombophilia:
- Indicated in all CVST patients to guide anticoagulation duration
- Family screening if severe hereditary thrombophilia identified (protein C/S/antithrombin deficiency, homozygous Factor V)
Monitoring on anticoagulation:
- Warfarin: INR every 4-12 weeks (target 2-3)
- DOACs: Renal function annually; no routine monitoring
- Annual review in anticoagulation clinic
13. Key Guidelines and Evidence
International Guidelines
1. American Heart Association/American Stroke Association Scientific Statement (2011) [1]
- Comprehensive CVST diagnosis and management guideline
- Class I recommendations:
- CT or MR venography for diagnosis (not conventional CT alone)
- Acute anticoagulation with LMWH or dose-adjusted UFH (even with haemorrhagic infarction)
- Transition to warfarin for 3-12 months depending on risk factors
- PMID: 21293023
2. European Stroke Organisation (ESO) Guidelines (2017) [10]
- Updated recommendations incorporating DOAC data
- Endorses anticoagulation as mainstay
- Addresses endovascular treatment (limited role)
- PMID: 28059573
3. European Academy of Neurology (EAN) Consensus (2017)
- Similar to ESO; emphasizes early diagnosis and anticoagulation
4. British Committee for Standards in Haematology (BCSH) VTE Guidelines
- Include CVST in venous thromboembolism management
- Thrombophilia workup recommendations
Landmark Studies and Trials
International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT, 2004) [6]
- Largest prospective cohort: 624 patients from 89 centers
- Established prognostic factors and outcome data
- 80% good outcome (mRS 0-2) at follow-up
- Mortality 8.3%
- Recurrence 6.5% over median 16 months
- PMID: 14976332
Meta-Analysis of Anticoagulation in CVST (Coutinho et al., 2011) [5]
- Systematic review and meta-analysis of anticoagulation safety
- Confirmed safety even with haemorrhagic infarction
- Reduced death and disability (absolute risk reduction 13%, NNT 8)
- PMID: 21903658
TO-ACT Trial (Endovascular Treatment, 2020) [21]
- Randomized controlled trial: Endovascular treatment vs anticoagulation
- Stopped early for futility
- No benefit of endovascular therapy in most patients
- Anticoagulation remains standard
- PMID: 32364579
RE-SPECT CVT (Dabigatran in CVST, 2022)
- Prospective study of dabigatran vs warfarin for CVST
- Non-inferiority of dabigatran demonstrated
- Supports DOAC use as alternative to warfarin [10]
- PMID: 35636321
ACTION-CVT (Apixaban, ongoing)
- Trial comparing apixaban to warfarin
- Results pending; further evidence for DOAC use
Key Systematic Reviews
Dentali et al. (2006) - Risk factors for CVST [14]
- Meta-analysis: OCP increases risk 5-20x
- Thrombophilia present in 20-35%
- PMID: 16864717
Ferro et al. (2017) - Prognosis of CVST [6]
- Long-term follow-up of ISCVT cohort
- 80-90% good outcome at 6 months
- Recurrence 5-15% over 5 years
Bousser and Ferro (2007) - Comprehensive review [2]
- Classic review article covering all aspects
- PMID: 17239803
Evidence Summary
| Question | Evidence Level | Recommendation |
|---|---|---|
| Diagnosis: MRV or CTV? | High (diagnostic studies) | Both highly accurate; MRV slightly more sensitive for cortical veins; CTV faster for acute setting [9] |
| Anticoagulation vs no treatment? | High (RCTs, meta-analysis) | Anticoagulation reduces death/disability; NNT 8 [5] |
| Anticoagulation safe with haemorrhage? | High (meta-analysis) | Safe and recommended even with haemorrhagic infarction [5] |
| LMWH vs UFH? | Moderate (small RCTs) | Both effective; LMWH more convenient (subcutaneous, no monitoring) |
| Warfarin vs DOAC long-term? | Moderate (non-inferiority trials) | DOACs (dabigatran, rivaroxaban) appear non-inferior; warfarin has more long-term data [10] |
| Endovascular treatment? | High (RCT) | No benefit over anticoagulation in most patients; reserve for exceptional cases [21] |
| Duration of anticoagulation? | Moderate (cohort studies) | 3-6 months if provoked; 6-12 months if unprovoked; lifelong if severe thrombophilia [10,15] |
| Thrombophilia screening? | High (cohort studies) | Recommended in all CVST patients to guide anticoagulation duration [15] |
14. Patient Education and Communication
Explaining CVST to Patients
Simple explanation: "You have a blood clot in one of the veins that drains blood from your brain. This vein became blocked, causing pressure to build up and damaging some brain tissue. We treat this with blood-thinning medication to stop the clot from getting bigger and help your body dissolve it over time."
Why it happened: "In your case, the likely cause is [OCP/pregnancy/infection/thrombophilia]. We will do tests to understand why this happened to you, which helps us decide how long you need blood thinners."
Is it serious?: "Yes, this is a serious condition that needs urgent treatment. However, with the blood-thinning treatment we've started, most people make a very good recovery—about 80-90% of patients return to normal or near-normal function."
Addressing Common Patient Concerns
"I have bleeding in my brain—why are you giving blood thinners?"
- "This is different from a usual brain bleed. The bleeding happened because the vein was blocked, causing pressure to build up and small blood vessels to burst. The blood thinner helps unblock the vein, which actually reduces the pressure and prevents more bleeding. Research shows this is safe and effective."
"How long will I need blood thinners?"
- "Usually 3-12 months, depending on what caused the clot. If it was caused by something temporary like the contraceptive pill or an infection, we can often stop after 3-6 months. If you have a blood clotting disorder, you may need longer treatment."
"Can this happen again?"
- "The risk of this happening again is low—about 5-15% over 5 years. Taking blood thinners for the right amount of time reduces this risk. If you have a clotting disorder, we may recommend longer or lifelong treatment to prevent recurrence."
"Can I have children in the future?" (Women of childbearing age)
- "Yes, most women who've had CVST can have successful pregnancies. However, you should not use combined hormonal contraceptives (the pill, patch, or ring) again. In a future pregnancy, you would need blood-thinning injections to reduce the small risk of recurrence. We'll refer you to a specialist to plan this."
Warning Signs to Return to Hospital
Provide written and verbal instructions:
Seek immediate medical attention if you experience:
- Sudden severe headache (thunderclap)
- Worsening headache despite medication
- New weakness or numbness
- Difficulty speaking or understanding
- Seizures or fits
- Vision changes (blurred vision, double vision, loss of vision)
- Unusual bleeding (blood in urine/stool, heavy nosebleeds, coughing blood)
- Confusion or drowsiness
- Severe dizziness or loss of balance
Lifestyle Advice
Hydration:
- Drink adequate fluids (1.5-2 liters daily)
- Especially important in hot weather or during illness
Medications:
- Stop OCP permanently; use alternative contraception (progesterone-only pill, IUD, barrier methods)
- Avoid oestrogen-containing HRT
- Take anticoagulant as prescribed; do not miss doses
- Inform all healthcare providers you are on blood thinners
Activity:
- Gradually return to normal activities as strength improves
- Avoid contact sports while on anticoagulation (bleeding risk)
- Driving: Cannot drive until cleared by neurology and DVLA (UK) if seizures occurred
Alcohol:
- Moderate alcohol intake if on warfarin (affects INR)
Diet:
- If on warfarin, maintain consistent vitamin K intake (green vegetables)—no need to avoid, just be consistent
Follow-Up Plan
First follow-up (4-6 weeks):
- Neurology clinic
- Review symptoms, neurological examination
- Discuss thrombophilia results
- Plan anticoagulation duration
Imaging follow-up (3-6 months):
- Repeat MR venography to assess recanalization
- Usually asymptomatic; done for prognostic information
Long-term:
- Annual review if on long-term anticoagulation
- Anticoagulation monitoring (INR if warfarin)
15. Examination Focus—Viva and OSCE Preparation
Opening Statement (Viva Voce)
"Cerebral venous sinus thrombosis is thrombosis of the dural venous sinuses or cerebral veins, causing impaired venous drainage, raised intracranial pressure, and potentially hemorrhagic venous infarction. It accounts for less than 1% of all strokes but is an important treatable cause in young adults, particularly women due to hormonal risk factors such as oral contraceptives and pregnancy."
Structured Approach to CVST Case
If given a clinical scenario:
-
Recognize the presentation: "This young woman presenting with headache, seizure, and OCP use raises concern for CVST."
-
Immediate management: "I would ensure airway, breathing, circulation. Assess GCS, control seizures with benzodiazepines and levetiracetam, and arrange urgent CT brain followed by CT or MR venography."
-
Diagnosis: "CT brain may show hemorrhagic infarction in a non-arterial distribution or the cord sign. Venography is essential and would show filling defect in the affected sinus."
-
Treatment: "Once confirmed, I would start therapeutic anticoagulation with LMWH, even if hemorrhagic infarction is present, as the hemorrhage is due to venous congestion and anticoagulation is safe and prevents further thrombosis."
-
Investigations: "I would investigate for underlying causes: thrombophilia screen (Factor V Leiden, prothrombin mutation, protein C/S, antithrombin, antiphospholipid antibodies), FBC for polycythemia, and exclude pregnancy and malignancy."
-
Long-term management: "Transition to warfarin or DOAC for 3-12 months depending on etiology. Stop OCP permanently. If severe thrombophilia, consider lifelong anticoagulation."
High-Yield Viva Facts to Memorize
| Topic | Fact |
|---|---|
| Incidence | 1.3-1.6 per 100,000; 3:1 female predominance [7] |
| Most common sinus | Superior sagittal sinus (60-70%) [8] |
| Most common symptom | Headache (85-95%) [3] |
| Seizure incidence | 40% [20] |
| Imaging gold standard | CT or MR venography (not CT brain alone) [9] |
| Pathognomonic sign | Empty delta sign on contrast CT; absent flow void on MRV |
| Hemorrhagic infarction rate | 30-40% [19] |
| Anticoagulation in hemorrhage | Safe and recommended [5] |
| First-line treatment | Therapeutic LMWH (e.g., enoxaparin 1 mg/kg BD) |
| Anticoagulation duration | 3-6 months (provoked), 6-12 months (unprovoked), lifelong (severe thrombophilia) [10] |
| Good outcome rate | 80-90% (mRS 0-2) [6] |
| Mortality | 5-10% [6] |
| Recurrence risk | 5-15% over 5 years [6] |
| Worst prognosis | Coma, deep venous thrombosis, malignancy [6] |
Common Viva Questions and Model Answers
Q1: What are the risk factors for CVST?
A: "I would categorize these into hormonal, thrombophilic, infectious, inflammatory, and malignant causes. Hormonal factors include oral contraceptive pill use (5-20x increased risk), pregnancy, and the postpartum period (highest risk first 2-4 weeks). Thrombophilias include Factor V Leiden and prothrombin G20210A mutations, protein C, S, and antithrombin deficiency, and antiphospholipid syndrome. Infections such as mastoiditis, sinusitis, and meningitis can cause septic CVST. Inflammatory conditions include IBD, Behçet's disease, and SLE. Malignancy and myeloproliferative disorders also increase risk."
Q2: How do you diagnose CVST?
A: "The gold standard is CT or MR venography, which demonstrates filling defects in the affected sinuses. CT brain alone is insufficient as it is normal in up to 30% of cases. Direct signs on CT include the cord sign (hyperdense vein) and dense triangle sign. Indirect signs include hemorrhagic infarction in a non-arterial distribution and cerebral edema. On contrast-enhanced CT, the empty delta sign—a triangular filling defect in the superior sagittal sinus—is pathognomonic. MRV shows absence of the normal flow void in affected sinuses."
Q3: Why is anticoagulation safe despite hemorrhagic infarction?
A: "The hemorrhage in CVST results from venous hypertension causing capillary rupture, not arterial bleeding. Anticoagulation prevents thrombus propagation, which reduces venous pressure and actually decreases further hemorrhage risk. Meta-analyses have confirmed that anticoagulation is safe and reduces death and disability with a number needed to treat of 8. The only contraindication would be a massive hematoma requiring surgical evacuation, which is rare."
Q4: What is the prognosis of CVST?
A: "With treatment, prognosis is generally good. 80-90% of patients achieve good functional outcome (mRS 0-2) at 6-12 months. Mortality is 5-10%. Poor prognostic factors include coma at presentation, deep venous system thrombosis, large intracerebral hemorrhage, malignancy, and CNS infection. Recurrence risk is 5-15% over 5 years, higher in those with severe thrombophilia or antiphospholipid syndrome."
Q5: How long should anticoagulation continue?
A: "Duration depends on the underlying etiology. For provoked CVST with a reversible risk factor like OCP or infection, 3-6 months is appropriate. For unprovoked CVST or mild thrombophilia, 6-12 months. For severe thrombophilia such as protein C, S, or antithrombin deficiency, homozygous Factor V Leiden, or antiphospholipid syndrome, lifelong anticoagulation is recommended due to high recurrence risk."
Common Mistakes That Fail Candidates
❌ Stating CT brain is sufficient for diagnosis (must request venography)
❌ Withholding anticoagulation due to hemorrhagic infarction (anticoagulation is safe and indicated)
❌ Failing to stop OCP (must stop permanently)
❌ Not performing thrombophilia screen (essential to guide anticoagulation duration)
❌ Recommending endovascular treatment as first-line (anticoagulation is standard; TO-ACT trial showed no benefit)
❌ Forgetting pregnancy counseling in women (can have future pregnancies with LMWH prophylaxis)
❌ Driving advice: Must inform DVLA; cannot drive for 12 months if seizure occurred (UK rules)
OSCE Station Tips
History taking:
- Ask about OCP use, pregnancy/recent delivery, family history of clots
- Recent infections (ear, sinus)
- Smoking (increases OCP risk)
- Headache characteristics and progression
- Seizure description
Examination:
- Fundoscopy (papilloedema) is critical—practice this
- Assess GCS and consciousness level
- Full neurological exam for focal signs
Investigations:
- Always request venography, not just CT brain
- Thrombophilia screen
Management:
- Immediate anticoagulation
- Seizure control
- Stop OCP
Communication:
- Explain safety of anticoagulation despite hemorrhage
- Counsel regarding OCP cessation and future contraception
- Pregnancy planning advice
16. References
-
Saposnik G, Barinagarrementeria F, Brown RD Jr, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42(4):1158-1192. doi:10.1161/STR.0b013e31820a8364
-
Bousser MG, Ferro JM. Cerebral venous thrombosis: an update. Lancet Neurol. 2007;6(2):162-170. doi:10.1016/S1474-4422(07)70029-7
-
Cumurciuc R, Crassard I, Sarov M, Valade D, Bousser MG. Headache as the only neurological sign of cerebral venous thrombosis: a series of 17 cases. J Neurol Neurosurg Psychiatry. 2005;76(8):1084-1087. doi:10.1136/jnnp.2004.056275
-
Dentali F, Gianni M, Crowther MA, Ageno W. Natural history of cerebral vein thrombosis: a systematic review. Blood. 2006;108(4):1129-1134. doi:10.1182/blood-2005-12-4795
-
Coutinho JM, de Bruijn SF, Deveber G, Stam J. Anticoagulation for cerebral venous sinus thrombosis. Cochrane Database Syst Rev. 2011;(8):CD002005. doi:10.1002/14651858.CD002005.pub2
-
Ferro JM, Canhão P, Stam J, Bousser MG, Barinagarrementeria F; ISCVT Investigators. Prognosis of cerebral vein and dural sinus thrombosis: results of the International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT). Stroke. 2004;35(3):664-670. doi:10.1161/01.STR.0000117571.76197.26
-
Coutinho JM, Zuurbier SM, Aramideh M, Stam J. The incidence of cerebral venous thrombosis: a cross-sectional study. Stroke. 2012;43(12):3375-3377. doi:10.1161/STROKEAHA.112.671453
-
Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med. 2005;352(17):1791-1798. doi:10.1056/NEJMra042354
-
Leach JL, Fortuna RB, Jones BV, Gaskill-Shipley MF. Imaging of cerebral venous thrombosis: current techniques, spectrum of findings, and diagnostic pitfalls. Radiographics. 2006;26 Suppl 1:S19-S41. doi:10.1148/rg.26si055174
-
Ferro JM, Bousser MG, Canhão P, et al; European Stroke Organization. European Stroke Organization guideline for the diagnosis and treatment of cerebral venous thrombosis - endorsed by the European Academy of Neurology. Eur J Neurol. 2017;24(10):1203-1213. doi:10.1111/ene.13381
-
deVeber G, Andrew M, Adams C, et al. Cerebral sinovenous thrombosis in children. N Engl J Med. 2001;345(6):417-423. doi:10.1056/NEJM200108093450604
-
Lanska DJ, Kryscio RJ. Risk factors for peripartum and postpartum stroke and intracranial venous thrombosis. Stroke. 2000;31(6):1274-1282. doi:10.1161/01.str.31.6.1274
-
Mahale R, Mehta A, John AA, et al. Acute infections as a risk factor for cerebral venous thrombosis. J Neurol Sci. 2016;368:239-243. doi:10.1016/j.jns.2016.07.025
-
Dentali F, Crowther M, Ageno W. Thrombophilic abnormalities, oral contraceptives, and risk of cerebral vein thrombosis: a meta-analysis. Blood. 2006;107(7):2766-2773. doi:10.1182/blood-2005-09-3578
-
Martinelli I, Bucciarelli P, Passamonti SM, Battaglioli T, Previtali E, Mannucci PM. Long-term evaluation of the risk of recurrence after cerebral sinus-venous thrombosis. Circulation. 2010;121(25):2740-2746. doi:10.1161/CIRCULATIONAHA.109.927046
-
Martinelli I, Sacchi E, Landi G, Taioli E, Duca F, Mannucci PM. High risk of cerebral-vein thrombosis in carriers of a prothrombin-gene mutation and in users of oral contraceptives. N Engl J Med. 1998;338(25):1793-1797. doi:10.1056/NEJM199806183382502
-
Grainge MJ, West J, Card TR. Venous thromboembolism during active disease and remission in inflammatory bowel disease: a cohort study. Lancet. 2010;375(9715):657-663. doi:10.1016/S0140-6736(09)61963-2
-
Ferro JM, Correia M, Pontes C, Baptista MV, Pita F. Seizures in cerebral vein and dural sinus thrombosis. Cerebrovasc Dis. 2003;15(1-2):78-83. doi:10.1159/000067133
-
Girot M, Ferro JM, Canhão P, et al. Predictors of outcome in patients with cerebral venous thrombosis and intracerebral hemorrhage. Stroke. 2007;38(2):337-342. doi:10.1161/01.STR.0000254579.16319.35
-
Ferro JM, Canhão P, Bousser MG, Stam J, Barinagarrementeria F. Early seizures in cerebral vein and dural sinus thrombosis: risk factors and role of antiepileptics. Stroke. 2008;39(4):1152-1158. doi:10.1161/STROKEAHA.107.487363
-
Coutinho JM, Zuurbier SM, Bousser MG, et al; TO-ACT Investigators. Effect of endovascular treatment with medical management vs standard care on severe cerebral venous thrombosis: the TO-ACT randomized clinical trial. JAMA Neurol. 2020;77(8):966-973. doi:10.1001/jamaneurol.2020.1022
-
Canhão P, Ferro JM, Lindgren AG, Bousser MG, Stam J, Barinagarrementeria F; ISCVT Investigators. Causes and predictors of death in cerebral venous thrombosis. Stroke. 2005;36(8):1720-1725. doi:10.1161/01.STR.0000173152.84438.1c
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for cerebral venous sinus thrombosis?
Seek immediate emergency care if you experience any of the following warning signs: Thunderclap headache, Seizures with headache, Focal neurological deficit in young adult, Reduced GCS, Papilloedema, Headache in pregnancy/postpartum, Headache with OCP use, Progressive headache despite analgesia.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Venous Anatomy of the Brain
Differentials
Competing diagnoses and look-alikes to compare.
- Subarachnoid Haemorrhage
- Ischaemic Stroke
- Primary Headache Disorders
Consequences
Complications and downstream problems to keep in mind.
- Venous Infarction
- Idiopathic Intracranial Hypertension