Diabetic Ketoacidosis (DKA)
Diabetic Ketoacidosis (DKA) is a profound metabolic emergency defined by the biochemical triad of Hyperglycaemia, Ketona... MRCP exam preparation.
What matters first
Diabetic Ketoacidosis (DKA) is a profound metabolic emergency defined by the biochemical triad of Hyperglycaemia, Ketona... MRCP exam preparation.
GCS less than 12 or altered mental status (Cerebral Oedema risk)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- GCS less than 12 or altered mental status (Cerebral Oedema risk)
- Severe Acidosis (pH less than 7.0 or Bicarbonate less than 5 mmol/L)
- Initial Hypokalaemia (K+ less than 3.5 mmol/L at presentation)
- SBP less than 90 mmHg (Refractory Shock)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Hyperglycaemic Hyperosmolar State (HHS)
- Alcoholic Ketoacidosis (AKA)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Topic family
This concept exists in multiple MedVellum libraries. Use the primary page for the broadest reference view and the others for exam-specific framing.
Diabetic Ketoacidosis (DKA) is a profound metabolic emergency defined by the biochemical triad of Hyperglycaemia, Ketona... MRCP exam preparation.
Diabetic Ketoacidosis represents absolute or relative insulin deficiency combined with counter-regulatory hormone excess... ACEM Fellowship Written, ACEM Fellow
Clinical explanation and evidence
Diabetic Ketoacidosis (Adult)
1. Overview
Diabetic Ketoacidosis (DKA) is a profound metabolic emergency defined by the biochemical triad of Hyperglycaemia, Ketonaemia, and Metabolic Acidosis. It represents the critical failure of glucose homeostasis due to an absolute or relative insulin deficiency combined with a massive surge in counter-regulatory hormones. [1]
The clinical significance of DKA is historical and evolving. It remains the leading cause of mortality in children and young adults with Type 1 Diabetes, primarily due to cerebral oedema. In the 2020s, the rise of Euglycaemic DKA (associated with SGLT2 inhibitors) has redefined the diagnostic threshold, necessitating the measurement of blood ketones even in patients with "normal" glucose levels. [2]
Management is strictly governed by the JBDS (2023) and ADA (2024) protocols, focusing on volume restoration, fixed-rate insulin delivery, and precise electrolyte replacement. Resolution is defined by the clearance of ketones and the restoration of pH, allowing for the critical transition back to subcutaneous insulin. [3]
2. Epidemiology
The T1DM Predominance
- Incidence: 5–8 episodes per 1,000 person-years among patients with Type 1 Diabetes.
- Ketosis-Prone Type 2 (KPD): Increasingly recognized in West African and African American populations (Flatbush Diabetes), where patients present with DKA but can later transition to oral agents. [4]
Mortality Drivers
- Ages less than 20: Cerebral Oedema (0.5–1.0% incidence; 20–25% mortality).
- Ages > 65: Precipitants (MI, Sepsis) and fluid overload/electrolyte failure.
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- Insulin Deficiency & Alarmin Surge: Lack of insulin combined with high Glucagon and Catecholamines triggers a profound catabolic switch.
- Unrestrained Lipolysis: Insulin failure activates Hormone-Sensitive Lipase (HSL) in adipose tissue. Triglycerides are broken down into Free Fatty Acids (FFAs).
- Carnitine Shuttle Disinhibition: In the liver, the fall in insulin reduces Malonyl-CoA levels. This removes the inhibition of CPT-1 (Carnitine Palmitoyltransferase-1), the "gatekeeper" of the mitochondria.
- HMG-CoA Pathway Activation: FFAs enter the mitochondria and undergo β-oxidation to Acetyl-CoA. Excess Acetyl-CoA is diverted into the HMG-CoA cycle by HMG-CoA Synthase (the rate-limiting enzyme).
- Ketogenesis: Two primary ketone bodies are produced: Acetoacetate (AcAc) and 3-β-hydroxybutyrate (3HB). 3HB is the dominant ketone in DKA (ratio often 10:1 vs AcAc).
- Anion Gap Acidosis: 3HB and AcAc are strong acids (pKa ~4.8). They dissociate, releasing protons (H+) that consume bicarbonate (HCO3-). This creates a High Anion Gap Metabolic Acidosis (HAGMA).
- Osmotic Diuresis & Collapse: Severe hyperglycaemia exceeds the renal threshold (10 mmol/L), causing an osmotic pull that strips the body of water, sodium, and potassium (Total water deficit: 100 mL/kg). [5, 6, 7]
4. Clinical Presentation
Symptoms
- GI Distress: Diffuse abdominal pain, nausea, and persistent vomiting. (Pain can mimic a "Surgical Abdomen").
- Respiratory: "Air hunger" (Kussmaul breathing).
- Neurological: Drowsiness and confusion (correlation with hyperosmolality).
Physical Signs
- Kussmaul Respirations: Deep, rapid, sighing breaths to blow off CO2 (compensatory respiratory alkalosis).
- Ketotic Breath: "Pear drops" or "Fruity" smell (due to Acetone, a breakdown product of AcAc).
- Severe Dehydration: Sunken eyes, reduced skin turgor, and dry mucous membranes.
- Hypothermia: Common due to peripheral vasodilation; fever suggests sepsis as a precipitant. [8]
5. Investigations
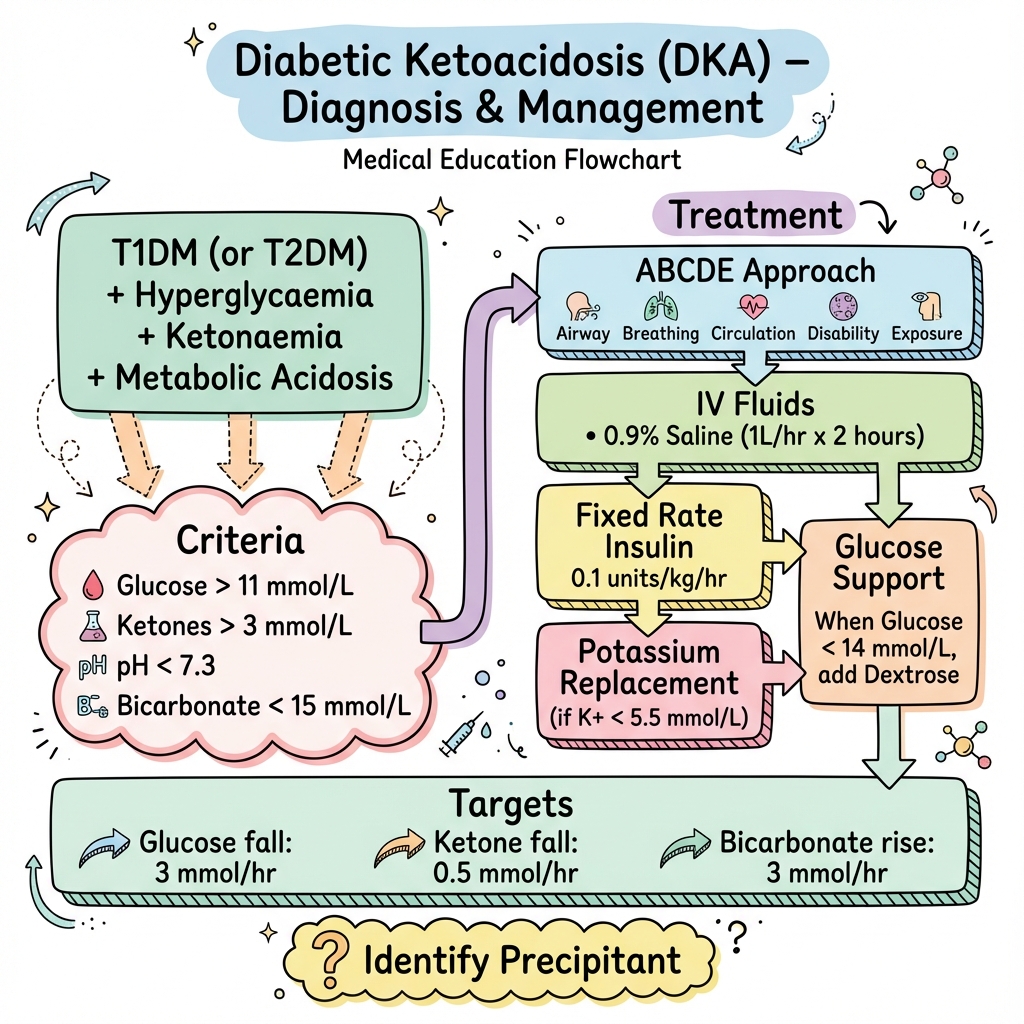
The Diagnostic Triad (JBDS)
- Hyperglycaemia: Glucose > 11.0 mmol/L (or known Diabetes).
- Ketonaemia: Blood Ketones ≥3.0 mmol/L. (Urine ketones are less reliable).
- Acidosis: Venous pH less than 7.30 or Bicarbonate less than 15.0 mmol/L.
The SGLT2i Trap: Euglycaemic DKA
Patients on Gliflozins (SGLT2i) may present with a pH of 7.1 and ketones of 5.0, but a blood glucose of only 6.5 mmol/L. This occurs because SGLT2i promote renal glucose excretion, masking the hyperglycaemia. Always check ketones in a sick SGLT2i user. [9]
6. Management: The 2024 Protocol
1. Fluid Resuscitation (Volume First)
- Immediate: 1L 0.9% NaCl over 1 hour.
- Subsequent: 1L over 2h, then 2h, then 4h, then 4h.
- Switch to 10% Dextrose: When CBG falls below 14 mmol/L. Do not stop the insulin!
2. Fixed-Rate Insulin (FRII)
- Dose: 0.1 units/kg/hr. (e.g. 7 units/hr for a 70kg patient).
- Action: Suppresses hepatic ketogenesis. Continue until ketones less than 0.6 and pH > 7.3.
3. Potassium Replacement (The Killer)
- Rule: Initial serum K+ is falsely high due to acidosis. Once insulin starts, K+ will plummet.
- Protocol: Add 40 mmol/L KCl to every bag if K+ is 3.5–5.5 mmol/L.
- Red Alert: If K+ less than 3.5, hold insulin and replace K+ urgently. [10]
7. Evidence: Landmark Trials
| Trial | Population | Intervention | Result | Impact |
|---|---|---|---|---|
| Pecock et al. | DKA | FRII vs. Bolus | Bolus no benefit | Standardised 0.1 u/kg FRII without bolus. |
| VANISH | DKA | VBG vs. ABG | Equivalence | Replaced painful ABGs with VBGs for monitoring. |
| STITCH | DKA | SGLT2i awareness | ↑ Recognition | Defined Euglycaemic DKA management. |
| 3-Bag System | DKA | Fluid titration | ↓ Errors | Promoted early glucose substrate addition. |
8. Single Best Answer (SBA) Questions
Question 1
A 22-year-old female with T1DM is admitted with DKA. pH 7.15, Ketones 5.2, Glucose 22. K+ is 3.1 mmol/L. What is the most appropriate immediate action?
- A) Start IV Insulin at 0.1 u/kg/hr
- B) Give 1L 0.9% NaCl with 40 mmol KCl over 1 hour
- C) Give 1L 0.9% NaCl and HOLD insulin until K+ > 3.5
- D) Give IV Bicarbonate 8.4%
- E) Loading dose of 10 units SC insulin
- Answer: C. Starting insulin when K+ is low (less than 3.5) will drive potassium into cells, potentially causing fatal cardiac arrest. Volume resuscitation and K+ replacement are the priority until K+ is at a safe level to start insulin.
Question 2
Which molecule acts as the "gatekeeper" to the mitochondria, and whose depletion in DKA allows for the massive entry of free fatty acids for ketogenesis?
- A) HMG-CoA
- B) Malonyl-CoA
- C) Acetoacetate
- D) Pyruvate
- E) Citrate
- Answer: B. Insulin promotes Malonyl-CoA, which inhibits CPT-1. In DKA, the lack of insulin causes Malonyl-CoA to fall, "opening the gates" for FFAs into the mitochondria.
9. Viva Scenario: The "Normal Sugar" DKA
Examiner: "A patient with Type 2 Diabetes on Dapagliflozin presents with nausea and a pH of 7.2. Their blood sugar is 8.0 mmol/L. Is this DKA?"
Candidate:
- Suspicion: Yes, I highly suspect Euglycaemic DKA.
- Mechanism: SGLT2 inhibitors cause the kidneys to dump glucose into the urine, which can keep blood sugar low even during a profound ketoacidotic state.
- Diagnosis: I would immediately check blood ketones. If they are ≥3.0 mmol/L, the diagnosis is confirmed regardless of the "normal" sugar.
- Management: I would treat with the full DKA protocol, but I would need to start 10% Dextrose immediately to allow for the insulin infusion required to clear the ketones.
10. Patient Explanation
"DKA is a serious complication where your body runs out of its main fuel (sugar) and starts to burn fat too quickly for energy. This creates 'acid waste' called ketones that poison the blood. It feels like you are gasping for air because your body is trying to breathe out the acid. We are giving you a constant 'drip' of insulin to stop the fat burning, and lots of fluids to flush out the acid. We will be checking your finger-prick tests every hour until the acid is gone."
11. References
- Joint British Diabetes Societies (JBDS-IP). Management of Diabetic Ketoacidosis in Adults. 2023. Online
- American Diabetes Association (ADA). Standards of Care in Diabetes—2024. Diabetes Care. 2024. [DOI: 10.2337/dc24-S016]
- Dhatariya KK, et al. Diabetic Ketoacidosis in Adults. BMJ. 2020. [PMID: 33115745]
- Dhatariya KK. Euglycaemic diabetic ketoacidosis: a review. Curr Opin Endocrinol Diabetes Obes. 2024.
- Kitabchi AE, et al. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009. [PMID: 19564476]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for diabetic ketoacidosis (dka)?
Seek immediate emergency care if you experience any of the following warning signs: GCS less than 12 or altered mental status (Cerebral Oedema risk), Severe Acidosis (pH less than 7.0 or Bicarbonate less than 5 mmol/L), Initial Hypokalaemia (K+ less than 3.5 mmol/L at presentation), SBP less than 90 mmHg (Refractory Shock), Persistent vomiting (Inability to maintain hydration).
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Hyperglycaemic Hyperosmolar State (HHS)
- Alcoholic Ketoacidosis (AKA)