Giant Cell Arteritis (GCA)
Giant Cell Arteritis (GCA) is a chronic, systemic, granulomatous vasculitis of large and medium-sized arteries, preferen... MRCP exam preparation.
What matters first
Giant Cell Arteritis (GCA) is a chronic, systemic, granulomatous vasculitis of large and medium-sized arteries, preferen... MRCP exam preparation.
Sudden, painless vision loss (A-AION)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
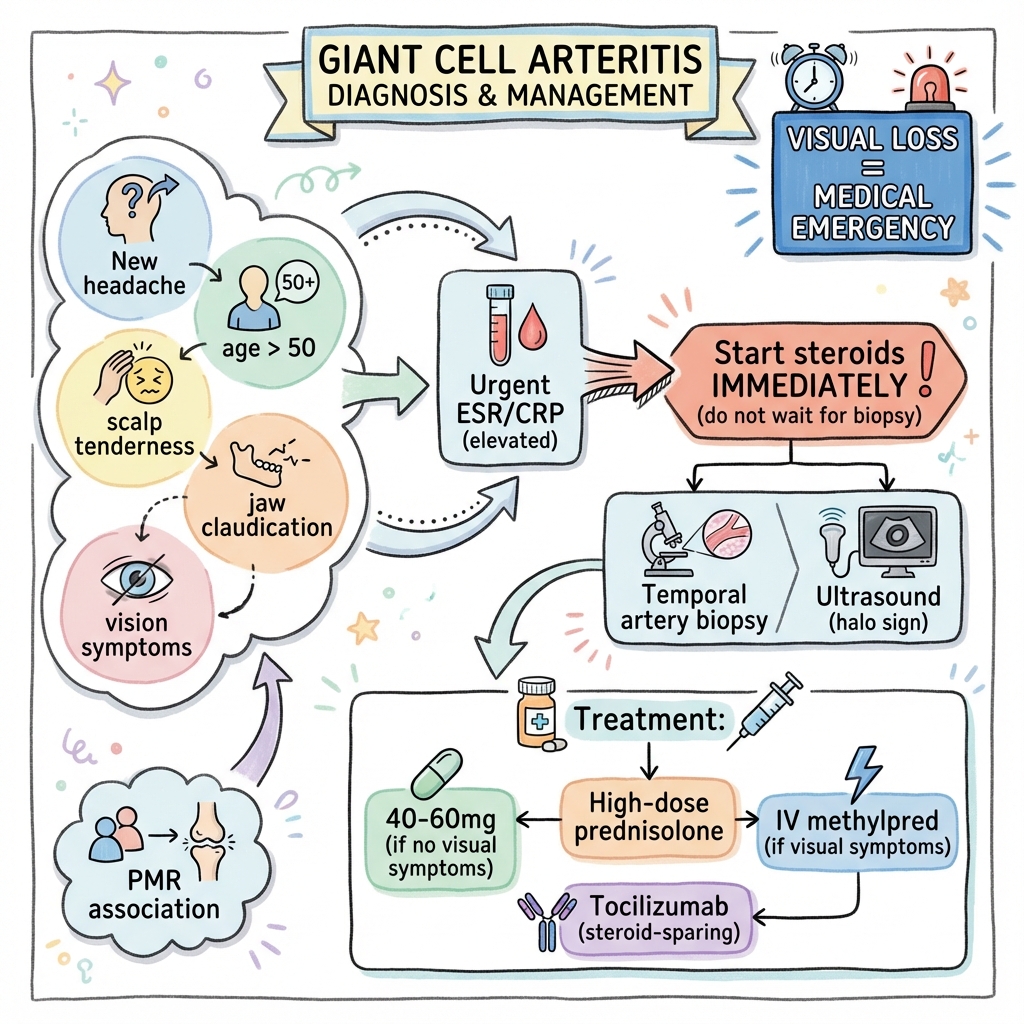
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Sudden, painless vision loss (A-AION)
- Amaurosis fugax (The 'shade' coming down over the eye)
- Jaw claudication (High specificity for ischaemia)
- Diplopia or ptosis (Cranial nerve ischaemia)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Polymyalgia Rheumatica
- Takayasu Arteritis
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Giant Cell Arteritis (Adult)
1. Overview
Giant Cell Arteritis (GCA) is a chronic, systemic, granulomatous vasculitis of large and medium-sized arteries, preferentially involving the extracranial branches of the carotid artery. It is the most common form of primary vasculitis in individuals over 50 and represents a medical and surgical emergency due to the risk of irreversible blindness. [1]
The clinical significance of GCA is defined by the "Time to Sight" mantra. In the 2020s, the management paradigm has shifted from chronic high-dose steroid monotherapy to the early initiation of IL-6 blockade (Tocilizumab), which allows for rapid steroid tapering and a reduction in the catastrophic iatrogenic side-effects (Diabetes, Osteoporosis). [2]
Diagnosis is now anchored in Urgent Ultrasound (The Halo Sign), which has high sensitivity and is replacing biopsy in many European centres. However, the Temporal Artery Biopsy (TAB) remains the definitive gold standard, especially in centers without expert ultrasonographers. [3]
2. Epidemiology
The "Northern Latitude" Disease
- Incidence: 15-30 per 100,000 person-years in Scandinavia and the UK. It is significantly rarer in Asian and Mediterranean populations (less than 2 per 100,000).
- The Age Gate: GCA is almost never seen in patients less than 50 years. The median age at diagnosis is 72.
- Gender: Women are affected 3x more often than men. [4]
The PMR Overlap
40-50% of GCA patients will have concurrent features of Polymyalgia Rheumatica (PMR) at diagnosis, characterized by proximal shoulder and hip girdle stiffness. Conversely, 15-20% of patients with isolated PMR will eventually develop GCA.
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- Adventitial Sentinel Activation: Resident Dendritic Cells (DCs) in the arterial adventitia are activated by unknown triggers (possibly TLR2/4 ligands). They release chemokines (CCL19/21).
- Vasa Vasorum Infiltration: DCs recruit CCR7+ CD4 T-cells and monocytes from the small vasa vasorum vessels into the arterial wall.
- Granulomatous Formation: In the media, T-cells release Interferon-gamma (IFN-γ). This cytokine is essential for the transformation of macrophages into Multi-nucleated Giant Cells.
- Elastic Lamina Destruction: Giant cells and macrophages release Matrix Metalloproteinases (MMP-2 and MMP-9). These "molecular scissors" digest the Internal Elastic Lamina (IEL).
- IL-6 Mediated Systemic Surge: The inflamed wall releases massive amounts of IL-6 into the circulation, driving the liver to produce CRP and causing fever, anaemia of chronic disease, and thrombocytosis.
- Intimal Hyperplasia: Macrophages release VEGF and PDGF, stimulating smooth muscle cells to migrate from the media to the intima, where they hyper-proliferate.
- Luminal Occlusion: The thickening "neointima" causes progressive narrowing and eventual total occlusion of the artery, resulting in distal ischaemia (e.g. the optic nerve head in A-AION). [5, 6, 7]
4. Clinical Presentation
Cranial Symptoms
- New Headache: Usually temporal, but can be diffuse. Often worse at night.
- Jaw Claudication: Pain when chewing that resolves with rest. High Specificity (> 90%) for GCA.
- Scalp Tenderness: Pain when brushing hair or resting the head on a pillow.
Ophthalmic Emergency
- Amaurosis Fugax: Transient "shade" or blurred vision; a critical warning of impending permanent loss.
- A-AION: Sudden, painless, profound vision loss. Fundoscopy shows a pale, swollen optic disc ("Chalky white edema").
- Relative Afferent Pupillary Defect (RAPD): A crucial sign in unilateral or asymmetric optic nerve disease. [8]
5. Investigations
Laboratory Synthesis
- ESR & CRP: Typically > 50 mm/hr and > 10 mg/L. (Note: 10% of biopsy-proven cases have normal ESR).
- FBC: Thrombocytosis and normocytic anaemia are common markers of severe IL-6 activity.
The Halo Sign (Ultrasound)
- The Halo: A hypoechoic, non-compressible "ring" around the temporal artery lumen, representing vessel wall oedema.
- Specificity: > 95% if bilateral halo signs are present.
- The "Biopsy-First" Rule: Ultrasound should be done within 7 days of steroids; TAB remains positive for up to 2 weeks. [9]
6. Management: The "Time is Sight" Protocol
1. Immediate Induction (The Fire Extinguisher)
- No Vision Loss: 60mg Prednisolone PO daily.
- Vision Loss / Amaurosis: IV Methylprednisolone (500mg-1g) daily for 3 days before switching to oral. [10]
2. Steroid-Sparing: Tocilizumab
The GiACTA trial (2017) changed the world:
- Weekly SC Tocilizumab plus a 26-week steroid taper is superior to steroids alone (56% vs 14% remission).
- Mandatory for relapsing disease or high risk of steroid toxicity (Diabetes/Osteoporosis).
3. Adjunctive Care
- Bone Protection: Mandatory Bisphosphonate (e.g. Alendronate) + Calcium/Vit D.
- Gastric Protection: PPI cover.
- Aspirin: Only if there is a secondary CV indication (e.g. Stroke/TIA). [11]
7. Evidence: Landmark Trials
| Trial | Population | Intervention | Result | Impact |
|---|---|---|---|---|
| GiACTA | New/Relapse GCA | Tocilizumab vs Plab | 56% Remission | Established IL-6 blockade as standard. |
| TABUL | Suspected GCA | US vs. Biopsy | US Sensitive | Promoted US as the first-line test. |
| GUSTO | New-onset GCA | IV vs. Oral Steroids | Faster markers ↓ | Validated IV induction for high-risk. |
| SELECT-GCA | New GCA | Upadacitinib (JAKi) | High Efficacy | Emerging oral biologic option. |
8. Single Best Answer (SBA) Questions
Question 1
A 72-year-old female presents with 3 days of right-sided headache and sudden blurring of vision in the right eye. Her ESR is 115. What is the single most appropriate immediate action?
- A) Arrange an urgent Temporal Artery Biopsy
- B) Start Prednisolone 60mg PO
- C) Give IV Methylprednisolone 1g
- D) Perform a Temporal Artery Ultrasound
- E) Wait for a CT Head to exclude stroke
- Answer: C. In the presence of visual symptoms, the patient requires pulse IV methylprednisolone to stabilize the optic nerve and prevent bilateralization. Oral steroids are insufficient in a visual emergency.
Question 2
What is the molecular mechanism behind the permanent vascular narrowing seen in late-stage Giant Cell Arteritis?
- A) Thrombus formation due to Vitamin K deficiency
- B) Intimal hyperplasia driven by PDGF and VEGF
- C) Destruction of the Adventitia by neutrophils
- D) Calcification of the tunica media
- E) Loss of Alpha-1 adrenergic receptors
- Answer: B. Macrophages in the vessel wall release growth factors (PDGF/VEGF) that drive smooth muscle cell migration and proliferation in the intima, leading to luminal stenosis.
9. Viva Scenario: The "Normal Marker" GCA
Examiner: "A 75-year-old has classic jaw claudication and a tender temporal artery, but her ESR and CRP are completely normal. Is GCA excluded?"
Candidate:
- Response: No, GCA is not excluded.
- Evidence: Approximately 5-10% of patients with biopsy-proven GCA have normal inflammatory markers at presentation.
- Next Step: I would still treat this patient as a Clinical GCA and proceed to a Temporal Artery Ultrasound.
- Secondary Search: I would also consider Large-Vessel GCA, which can sometimes have a more indolent inflammatory profile, and potentially order an FDG-PET/CT to look for aortitis. [12]
10. Patient Explanation
"Giant Cell Arteritis is a condition where the blood vessels in your head become inflamed and swollen. Think of it like a pipe that is starting to rust from the inside out, making it hard for blood to reach your eyes. It is an emergency because if the blood is cut off entirely, it can cause permanent blindness. We use high-dose steroids (like Prednisolone) to act like a 'fire extinguisher' for that inflammation. You will need to be on this medication for at least a year, but we will use a new 'steroid-sparing' injection to help us get the dose down quickly."
11. References
- Mackie SL, et al. British Society for Rheumatology guideline on diagnosis and treatment of GCA. Rheumatology. 2020. [PMID: 32090286]
- Stone JH, et al. Trial of Tocilizumab in Giant-Cell Arteritis (GiACTA). N Engl J Med. 2017. [PMID: 28745999]
- Ponte C, et al. 2022 ACR/EULAR classification criteria for giant cell arteritis. Ann Rheum Dis. 2022. [PMID: 36351706]
- Luqmani R, et al. The role of ultrasound in the diagnosis of GCA (TABUL study). Health Technol Assess. 2016.
- Weyand CM, Goronzy JJ. Giant-Cell Arteritis and Polymyalgia Rheumatica. N Engl J Med. 2014. [PMID: 24988477]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for giant cell arteritis (gca)?
Seek immediate emergency care if you experience any of the following warning signs: Sudden, painless vision loss (A-AION), Amaurosis fugax (The 'shade' coming down over the eye), Jaw claudication (High specificity for ischaemia), Diplopia or ptosis (Cranial nerve ischaemia), Scalp necrosis (Terminal sign of multi-vessel occlusion).
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Polymyalgia Rheumatica
- Takayasu Arteritis
Consequences
Complications and downstream problems to keep in mind.
- Permanent Blindness
- Ischaemic Stroke