Head Injury (Adult Traumatic Brain Injury)
Evidence-based emergency diagnosis and management of head injury and traumatic brain injury in adults
What matters first
Evidence-based emergency diagnosis and management of head injury and traumatic brain injury in adults
Check the red flags, emergency triggers, and escalation points before using the deep-dive material.
10 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
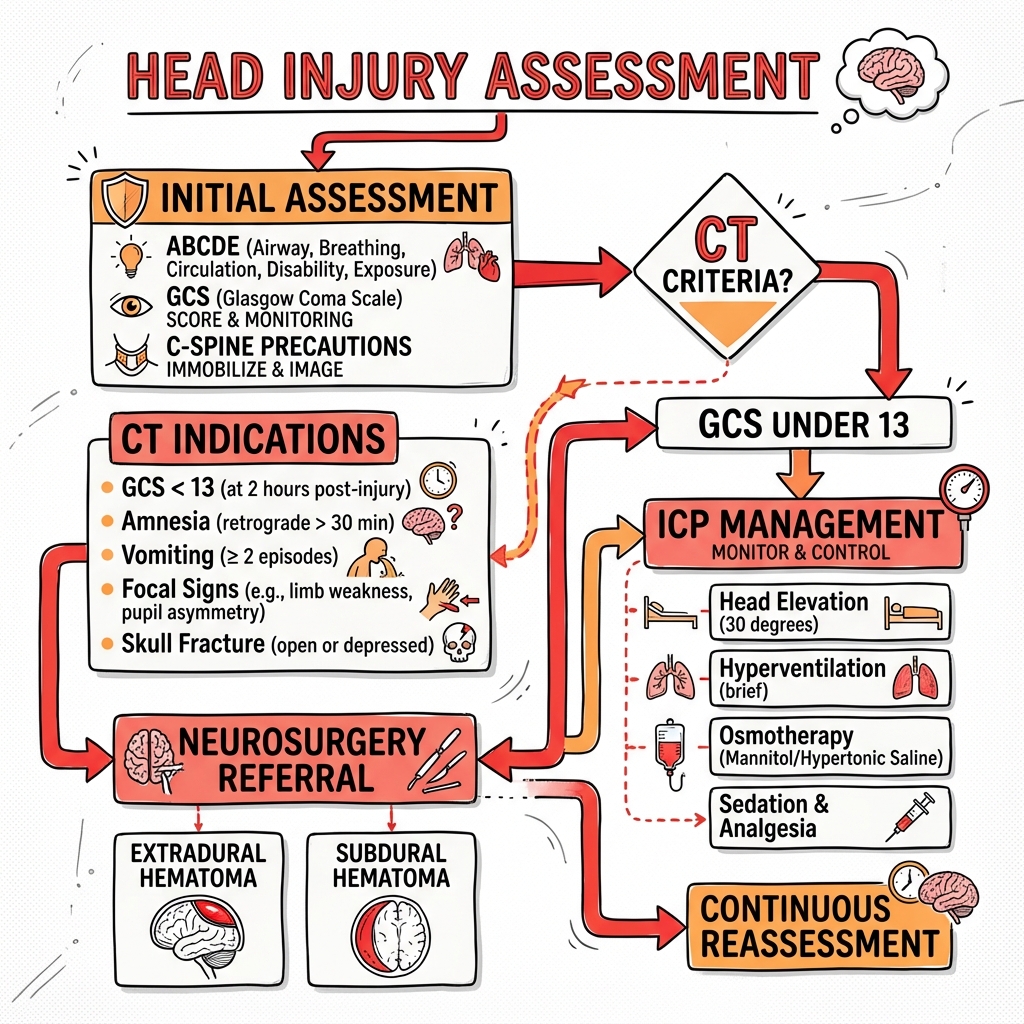
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Exam focus
Current exam surfaces linked to this topic.
- MRCEM, FRCEM, MRCS
Linked comparisons
Differentials and adjacent topics worth opening next.
- Stroke (Ischaemic and Haemorrhagic)
- Syncope
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Head Injury (Adult Traumatic Brain Injury)
Quick Reference
Critical Alerts
Life-Threatening Red Flags:
- GCS ≤8: Severe TBI - intubate immediately for airway protection [1]
- Cushing's triad: Hypertension + bradycardia + irregular respirations = impending herniation [2]
- Unilateral dilated pupil: Uncal herniation (CN III compression) - neurosurgical emergency [3]
- Anticoagulated patients: 3-5× higher risk of intracranial haemorrhage - low threshold for CT [4]
- Hypotension (SBP less than 90 mmHg): Doubles mortality in TBI - aggressive resuscitation mandatory [5]
- Hypoxia (SpO₂ less than 90%): Independent predictor of poor outcome - prevent secondary injury [5]
Emergency Assessment Framework
Primary Survey (ATLS Protocol):
| Component | Assessment | Critical Action |
|---|---|---|
| Airway | C-spine immobilisation, airway patency | Intubate if GCS ≤8 |
| Breathing | RR, SpO₂, breath sounds, pattern | Target SpO₂ > 94% |
| Circulation | BP, HR, capillary refill | SBP > 110 mmHg (age 50-69), > 120 mmHg if less than 50 [1] |
| Disability | GCS (E+V+M), pupils, blood glucose | Repeat GCS every 15 min initially |
| Exposure | Full body exam, temperature | Identify other injuries |
Key Diagnostics
| Test | Indication | Interpretation |
|---|---|---|
| GCS | All head injuries | 13-15 mild, 9-12 moderate, 3-8 severe [1] |
| CT Head (non-contrast) | Per Canadian CT Head Rule | Immediate for GCS less than 13, skull fracture, focal deficit [6] |
| Pupils | All patients | Size, reactivity, asymmetry |
| Blood glucose | All patients | Exclude hypoglycaemia as cause |
| Coagulation (PT/INR, aPTT) | Anticoagulated patients | Guide reversal strategy |
Emergency Treatments
| Condition | First-Line Treatment | Dose/Protocol | Evidence |
|---|---|---|---|
| Elevated ICP (herniation) | Hypertonic saline 23.4% | 30 mL IV push via central line | Faster onset than mannitol [7] |
| Alternative ICP therapy | Mannitol | 1-1.5 g/kg IV over 15 min | Traditional osmotherapy [1] |
| Severe herniation (bridge) | Hyperventilation | Target PaCO₂ 30-35 mmHg (temporary only) | Transient effect, causes cerebral vasoconstriction [1] |
| Warfarin reversal | 4-Factor PCC + Vitamin K | 25-50 units/kg IV + 10 mg IV | Superior to FFP for rapid reversal [8] |
| Dabigatran reversal | Idarucizumab | 5 g IV (2 × 2.5g boluses) | Specific reversal agent [9] |
| Seizure (active) | Levetiracetam | 20 mg/kg IV (max 3 g) over 10 min | First-line for post-traumatic seizures [10] |
| Hypotension in TBI | Crystalloid bolus → vasopressors | 20 mL/kg then norepinephrine to MAP > 80 | CPP = MAP - ICP [1,5] |
Overview
Definition
Head injury encompasses any trauma to the scalp, skull, or brain. Traumatic Brain Injury (TBI) specifically refers to alteration in brain function caused by external mechanical force, manifesting as decreased consciousness, amnesia, neurological deficit, or intracranial lesion. [1]
TBI is a leading cause of death and disability worldwide, with outcomes critically dependent on prevention of secondary brain injury through maintenance of adequate cerebral perfusion and oxygenation. [1,5]
Classification Systems
By Severity (Glasgow Coma Scale): [1]
| Category | GCS Score | Characteristics | Mortality |
|---|---|---|---|
| Mild TBI | 13-15 | 80% of all TBI; brief LOC; may have normal CT | less than 1% |
| Moderate TBI | 9-12 | 10% of TBI; requires monitoring; 10% deteriorate | 5-10% |
| Severe TBI | 3-8 | 10% of TBI; comatose; requires ICU ± surgery | 30-40% |
By Pathoanatomy:
| Type | Mechanism | CT Appearance | Management Priority |
|---|---|---|---|
| Epidural Haematoma (EDH) | Arterial (middle meningeal) | Biconvex (lens-shaped), doesn't cross sutures | Surgical evacuation if > 30 mL [11] |
| Subdural Haematoma (SDH) | Venous (bridging veins) | Crescent-shaped, crosses sutures | Surgery if > 10 mm or midline shift > 5 mm [11] |
| Subarachnoid Haemorrhage (SAH) | Cortical vessel rupture | Blood in sulci/cisterns | Secondary vasospasm risk |
| Intraparenchymal Contusion | Direct brain tissue injury | Mixed density, frontal/temporal poles | Monitor for expansion |
| Diffuse Axonal Injury (DAI) | Rotational shear forces | Petechiae at grey-white junction | Poor prognosis; no surgery |
| Skull Fracture | Direct impact | Linear, depressed, basilar | Open/depressed > 1 table → surgery |
By Mechanism: [1]
- Primary injury: Immediate mechanical damage (not reversible)
- Secondary injury: Subsequent damage from hypoxia, hypotension, oedema, inflammation (preventable and treatable)
Epidemiology
Incidence and Burden
- Global incidence: 200-300 per 100,000 population annually [2]
- US statistics: 2.87 million ED visits, 288,000 hospitalisations, 61,000 deaths annually [2]
- Leading causes: Falls (48%), motor vehicle collisions (20%), struck by/against object (17%), assault (10%) [2]
- Economic burden: US$76.5 billion annually in direct and indirect costs [2]
Demographics
- Age distribution: Bimodal peaks at 15-24 years (high-risk behaviours, MVCs) and > 75 years (falls) [2]
- Sex: Male-to-female ratio 3:1 for severe TBI [2]
- Mortality: 30-40% for severe TBI despite advances in care [1,5]
Risk Factors
Patient Factors:
- Age > 65 years (brain atrophy increases SDH risk, often on anticoagulation) [4]
- Age less than 4 years (non-accidental injury, falls)
- Anticoagulation (warfarin, DOACs) or antiplatelet therapy [4]
- Previous TBI (cumulative effects, especially in contact sports)
- Substance use (alcohol, drugs - impaired judgment)
- Seizure disorder
Mechanism Factors:
- High-energy trauma (MVC > 40 mph, fall > 3 metres)
- Pedestrian struck by vehicle
- Ejection from vehicle
- Unhelmeted motorcycle/bicycle crash
Pathophysiology
Primary vs Secondary Brain Injury
Primary Injury (occurs at moment of impact): [1]
- Direct mechanical disruption of neurons, axons, blood vessels
- Includes contusions, lacerations, diffuse axonal injury
- Not reversible - prevention is only strategy (helmets, seatbelts)
Secondary Injury (evolves over hours to days): [1,5]
| Insult | Mechanism | Prevention Target | Evidence |
|---|---|---|---|
| Hypotension | ↓ CPP → cerebral ischaemia | SBP > 110 mmHg | Single episode doubles mortality [5] |
| Hypoxia | ↓ O₂ delivery → neuronal death | SpO₂ > 94% | Independent predictor of poor outcome [5] |
| Intracranial hypertension | ↑ ICP → ↓ CPP → herniation | ICP less than 22 mmHg | Graded relationship with mortality [1] |
| Hyperthermia | ↑ Metabolic demand, excitotoxicity | Normothermia (36-37°C) | Each 1°C ↑ worsens outcome [1] |
| Hypoglycaemia | Energy failure | Glucose 6-10 mmol/L | Tight control harmful (NICE-SUGAR) [1] |
| Hyperglycaemia | Osmotic stress, inflammation | Avoid > 10 mmol/L | U-shaped curve |
| Hyponatraemia | Cerebral oedema | Na+ > 135 mmol/L | Monitor closely |
| Seizures | ↑ Metabolic demand, ↑ ICP | Prophylaxis if high risk | Prevents early (not late) seizures [10] |
Intracranial Pressure Dynamics
Monroe-Kellie Doctrine: [1,2]
- Skull is fixed volume (~1500 mL): Brain 80% + Blood 10% + CSF 10%
- Increase in one component must be compensated by decrease in others
- Once compensation exhausted → exponential rise in ICP
Cerebral Perfusion Pressure (CPP): [1]
CPP = MAP - ICP
- Normal ICP: 5-15 mmHg
- Treatment threshold: ICP > 22 mmHg [1]
- Target CPP: 60-70 mmHg (some centres 50-70) [1]
- CPP less than 50 mmHg → cerebral ischaemia
Autoregulation: [1,2]
- Normally maintains constant cerebral blood flow (CBF) at MAP 50-150 mmHg
- Lost or impaired in TBI → CBF becomes pressure-passive
- Makes brain vulnerable to both hypotension (ischaemia) and hypertension (hyperaemia, oedema)
Herniation Syndromes
Life-Threatening Complication of Raised ICP: [3]
| Type | Anatomy | Clinical Features | Management |
|---|---|---|---|
| Uncal | Medial temporal lobe → tentorial notch | Ipsilateral dilated pupil (CN III compression), contralateral hemiparesis, drowsiness | Hyperventilation + osmotherapy + urgent surgery |
| Central transtentorial | Bilateral downward displacement | Progressive deterioration: small reactive pupils → mid-position fixed → bilateral dilation; decerebrate posturing | Hyperventilation + osmotherapy + decompressive craniectomy |
| Tonsillar | Cerebellar tonsils → foramen magnum | Cardiorespiratory arrest (medullary compression) | Rapidly fatal - emergency posterior fossa decompression |
| Subfalcine | Cingulate gyrus under falx cerebri | Contralateral leg weakness (ACA compression); often asymptomatic | Treat underlying ICP |
Clinical Presentation
History
AMPLE + Mechanism: [1]
- Allergies
- Medications: Anticoagulants (warfarin, DOACs, aspirin, clopidogrel), antiplatelets
- Past history: Previous TBI, neurosurgery, VP shunt, seizures, coagulopathy
- Last oral intake (for potential surgery)
- Events/Environment
Mechanism Details (critical for risk stratification): [6]
- What happened? (Fall, MVC, assault, sports injury)
- Height of fall (> 1 metre high risk in elderly; > 1.5 metres in adults)
- Speed of vehicle (> 40 mph)
- Helmet worn? Seatbelt?
- Ejection from vehicle, pedestrian struck = very high risk
Loss of Consciousness: [6]
- Did patient lose consciousness?
- Duration of LOC (> 5 minutes → higher risk)
- Post-traumatic amnesia: Duration? (> 24 hours = severe TBI)
- Retrograde amnesia: How far back? (> 30 minutes → CT indicated by Canadian CT Head Rule [6])
Symptoms: [1]
- Headache (severity, progression - worsening headache is red flag)
- Vomiting (≥2 episodes → CT indicated [6])
- Confusion, disorientation
- Visual disturbances, diplopia
- Dizziness, imbalance
- Seizure activity witnessed
Physical Examination
Glasgow Coma Scale (Must document individual components): [1]
| Component | Response | Score |
|---|---|---|
| Eye Opening (E) | Spontaneous | 4 |
| To voice/command | 3 | |
| To pain | 2 | |
| None | 1 | |
| Verbal Response (V) | Oriented (person, place, time) | 5 |
| Confused conversation | 4 | |
| Inappropriate words | 3 | |
| Incomprehensible sounds | 2 | |
| None | 1 | |
| Motor Response (M) | Obeys commands | 6 |
| Localises to pain | 5 | |
| Withdraws from pain | 4 | |
| Abnormal flexion (decorticate) | 3 | |
| Abnormal extension (decerebrate) | 2 | |
| None (flaccid) | 1 |
GCS Interpretation:
- GCS 15: May still have intracranial injury if high-risk mechanism
- GCS 13-14: "Mild TBI" but 5-10% have significant CT findings [6]
- GCS 9-12: High risk of deterioration - close monitoring essential
- GCS ≤8: "Does not maintain airway"
- intubate [1]
Pupillary Examination (critical for herniation detection): [3]
| Finding | Likely Cause | Significance |
|---|---|---|
| Unilateral dilated, fixed | Ipsilateral uncal herniation (CN III) | Neurosurgical emergency |
| Bilateral dilated, fixed | Bilateral herniation, severe hypoxia, death imminent | Consider organ donation if no cardiac output |
| Bilateral pinpoint | Pontine lesion or opioid intoxication | Distinguish by naloxone response |
| Unilateral small (Horner's) | Carotid dissection, brainstem lesion | Consider CT angiography |
Cushing's Triad (impending herniation): [2,3]
- Hypertension (widened pulse pressure)
- Bradycardia
- Irregular respirations (Cheyne-Stokes, apneustic)
Signs of Basilar Skull Fracture: [1]
- Battle's sign: Mastoid ecchymosis (appears 12-24 hours post-injury)
- Raccoon eyes: Periorbital ecchymosis (bilateral)
- CSF rhinorrhoea or otorrhoea ("halo sign" on filter paper)
- Haemotympanum
- CN VII palsy (facial nerve injury)
Focal Neurological Deficits: [1]
- Hemiparesis, hemisensory loss
- Cranial nerve palsies
- Aphasia
- Visual field defects
- Ataxia, dysmetria
Signs of Raised ICP: [2,3]
- Headache (severe, progressive)
- Vomiting (especially projectile)
- Papilloedema (takes 6-24 hours to develop)
- Altered consciousness (progressive drowsiness)
- Posturing: Decorticate (flexor) or Decerebrate (extensor)
Red Flags
Immediate Life Threats (activate trauma team): [1]
| Finding | Significance | Immediate Action |
|---|---|---|
| GCS ≤8 | Severe TBI, airway at risk | RSI, CT, neurosurgery consult |
| Rapidly declining GCS (≥2 points) | Expanding haematoma | Repeat CT, urgent surgery |
| Unilateral dilated pupil | Uncal herniation | Osmotherapy, hyperventilation, emergency surgery |
| Cushing's triad | Imminent herniation | Osmotherapy, neurosurgery immediately |
| Open/depressed skull fracture | Brain exposure, infection risk | Antibiotics, surgery |
| Penetrating injury | Active bleeding | Do not remove object, surgery |
| SBP less than 90 mmHg | Doubles mortality | Aggressive fluid resuscitation |
High-Risk Features for Intracranial Injury (per Canadian CT Head Rule): [6]
- GCS less than 15 at 2 hours post-injury
- Suspected open or depressed skull fracture (palpable step, boggy swelling)
- Any sign of basilar skull fracture
- ≥2 episodes of vomiting
- Age ≥65 years
- Retrograde amnesia > 30 minutes
- Dangerous mechanism (pedestrian struck, ejection from vehicle, fall from > 1 metre or 5 stairs)
Differential Diagnosis
Consider Non-Traumatic Causes
Many "falls with head injury" are actually medical events causing the fall:
| Diagnosis | Distinguishing Features | Key Investigation |
|---|---|---|
| Spontaneous ICH (caused fall) | Hypertension, anticoagulation, sudden severe headache before fall | CT brain + CTA if ICH found |
| Ischaemic stroke | Focal deficit out of proportion to trauma, atrial fibrillation | CT perfusion, diffusion-weighted MRI |
| Subarachnoid haemorrhage | Thunderclap headache, neck stiffness, no clear trauma | CTA for aneurysm |
| Syncope/arrhythmia | Prodrome (lightheadedness, palpitations), rapid recovery, cardiac history | ECG, telemetry, echocardiogram |
| Hypoglycaemia | Diabetes, confusion before fall, responds to glucose | Bedside glucose |
| Seizure | Witnessed tonic-clonic activity, post-ictal confusion, tongue biting | EEG, medication levels |
| Alcohol/drug intoxication | Smell of alcohol, toxidrome, history | Ethanol level, urine drug screen |
| Vertebrobasilar insufficiency | Vertigo, diplopia, ataxia | MRI posterior fossa, vertebral Doppler |
Mimics of Decreased Consciousness
- Hepatic encephalopathy: Asterixis, jaundice
- Hypercapnia: COPD, high PaCO₂
- Medication overdose: Benzodiazepines, opioids
- Hypothermia: Core temperature less than 35°C
- Non-convulsive status epilepticus: Subtle twitching, EEG diagnostic
Diagnostic Approach
Clinical Decision Rules for CT Imaging
Canadian CT Head Rule (GCS 13-15 only, age ≥16): [6]
High-Risk Criteria (for neurosurgical intervention - sensitivity 100%):
- GCS less than 15 at 2 hours post-injury
- Suspected open or depressed skull fracture
- Any sign of basilar skull fracture (haemotympanum, raccoon eyes, Battle's sign, CSF leak)
- ≥2 episodes of vomiting
- Age ≥65 years
Medium-Risk Criteria (for brain injury on CT):
- Retrograde amnesia ≥30 minutes to impact
- Dangerous mechanism:
- Pedestrian struck by motor vehicle
- Occupant ejected from motor vehicle
- Fall from elevation ≥1 metre or 5 stairs
CT Head if ANY criterion present.
Not applicable if: GCS less than 13, penetrating injury, obvious depressed fracture, anticoagulation/coagulopathy.
Performance: Sensitivity 98.4% for neurosurgical intervention, specificity 49.6% [6]
NICE Head Injury Guidelines (CG176, 2014): [12]
CT within 1 hour if ANY of:
- GCS less than 13 on initial assessment
- GCS less than 15 at 2 hours post-injury
- Suspected open or depressed skull fracture
- Sign of skull base fracture
- Post-traumatic seizure
- Focal neurological deficit
-
1 episode of vomiting
- Amnesia > 30 minutes of events before impact (if age ≥65 or dangerous mechanism or > 30 min retrograde amnesia)
Observe for ≥8 hours if anticoagulated (even if CT negative initially).
Imaging Studies
CT Head Non-Contrast (gold standard for acute TBI): [1]
Indications:
- All moderate-severe TBI (GCS less than 13)
- Mild TBI with risk factors per Canadian CT Head Rule or NICE guidelines [6,12]
- All anticoagulated patients (even low-energy mechanism) [4]
- Penetrating injury
- Unable to assess clinically (intoxication, sedation)
Key Findings to Identify:
| Finding | CT Appearance | Surgical Significance |
|---|---|---|
| Epidural haematoma | Biconvex (lens), does not cross sutures, often associated skull fracture | Surgery if > 30 mL volume or thickness > 15 mm or midline shift > 5 mm [11] |
| Subdural haematoma (acute) | Crescent-shaped, crosses sutures, hyperdense (white) | Surgery if thickness > 10 mm or midline shift > 5 mm or GCS decline ≥2 [11] |
| Subdural haematoma (chronic) | Crescent, hypodense (dark) or mixed density | Burr hole drainage if symptomatic |
| Subarachnoid blood | Hyperdensity in sulci, basal cisterns | Monitor for vasospasm, hydrocephalus |
| Intraparenchymal contusion | Mixed density (blood + oedema), often frontal/temporal poles | Surgery if > 50 mL or progressive deterioration [1] |
| Diffuse axonal injury | Normal or petechial haemorrhages at grey-white junction, corpus callosum, brainstem | No surgery - supportive care, poor prognosis |
| Skull fracture | Linear lucency (often missed!), depressed (bone below inner table) | Surgery if open, depressed > 1 table thickness, cosmetic [1] |
| Midline shift | > 5 mm associated with worse outcomes | Consider decompressive craniectomy if refractory ICP [13] |
| Effacement | Loss of sulci, compressed basal cisterns (especially perimesencephalic) | Raised ICP - aggressive management |
Marshall CT Classification (prognostic): [2]
- Diffuse Injury I: No visible pathology
- Diffuse Injury II: Cisterns present, midline shift 0-5 mm, lesions less than 25 mL
- Diffuse Injury III (swelling): Cisterns compressed/absent, midline shift 0-5 mm
- Diffuse Injury IV (shift): Midline shift > 5 mm
- Evacuated mass lesion V
- Non-evacuated mass lesion VI: Lesion > 25 mL
CT Angiography (CTA):
- Suspected vascular injury (carotid/vertebral dissection)
- Penetrating trauma
- Basilar skull fracture (may injure carotid in cavernous sinus)
- SAH to identify aneurysm
MRI Brain (not acute):
- Better sensitivity for diffuse axonal injury (FLAIR, SWI sequences)
- Subacute/chronic bleeds (after days-weeks)
- Prognostication in severe TBI
- Follow-up imaging
Repeat CT Head Indications: [1]
- Clinical deterioration (GCS decline ≥2 points)
- New focal deficit
- Anticoagulated patients: 6-24 hours after initial CT (delayed haematoma expansion) [4]
- Routine at 12-24 hours for moderate-severe TBI on conservative management
- After reversal of anticoagulation if high-risk mechanism
Laboratory Studies
| Test | Indication | Action Based on Result |
|---|---|---|
| Blood glucose | All patients | Treat if less than 4 mmol/L; target 6-10 mmol/L [1] |
| Full blood count | Baseline, assess for anaemia | Transfuse if Hb less than 70 g/L (restrictive strategy) [1] |
| PT/INR, aPTT | Anticoagulated, coagulopathic, pre-op | INR > 1.4 → reverse urgently [8] |
| Fibrinogen, thromboelastography | Massive haemorrhage protocol | Guide blood product replacement |
| Urea, creatinine, electrolytes | Baseline, monitor for SIADH, DI | Na+ critical (hypo/hypernatraemia worsens outcome) |
| Type and screen | All moderate-severe TBI | In case of emergency surgery |
| Ethanol level, urine drug screen | Altered consciousness | Contributes to GCS; medicolegal |
| Pregnancy test (β-hCG) | Women of childbearing age | Affects imaging/management decisions |
Neuromonitoring (in ICU)
ICP Monitoring (EVD or intraparenchymal bolt): [1]
- Indications: Severe TBI (GCS ≤8) with abnormal CT, or normal CT but ≥2 of: age > 40, motor posturing, SBP less than 90 mmHg
- Target: ICP less than 22 mmHg
- Treat if: ICP > 22 mmHg sustained (not brief spikes during suctioning)
Cerebral Perfusion Pressure:
- Target CPP: 60-70 mmHg [1]
- Requires arterial line + ICP monitor
Brain Tissue Oxygenation (PbtO₂): [1]
- Goal > 20 mmHg
- Guides oxygen/ventilation/CPP management
Jugular Venous Oximetry (SjvO₂):
- Monitors global cerebral O₂ extraction
- less than 50% suggests ischaemia
Management
Principles of TBI Management
"Brain Trauma Foundation Guidelines" (4th Edition, 2016): [1]
- Prevent secondary injury: Avoid hypoxia, hypotension, hyper/hypocapnia, hyper/hypoglycaemia
- Maintain cerebral perfusion: CPP 60-70 mmHg
- Control ICP: Tiered approach (basic → osmotherapy → surgery)
- Early neurosurgical consultation: For all significant findings
- Reverse coagulopathy: Immediately in ICH
- Multimodal monitoring: ICP, CPP, PbtO₂
- Early rehabilitation: Improves functional outcomes [14]
Airway Management
Indications for Intubation: [1]
- GCS ≤8 ("does not maintain airway")
- Inability to protect airway (reduced gag/cough)
- Hypoxia despite supplemental O₂
- Hypercarbia requiring controlled ventilation
- Combativeness requiring sedation
- Transport of severe TBI (helicopter, long distance)
- Pre-operative
Rapid Sequence Intubation (RSI) in TBI: [1]
| Agent | Dose | Advantages | Disadvantages |
|---|---|---|---|
| Pre-treatment: | |||
| Lidocaine | 1.5 mg/kg IV | May blunt ICP rise with laryngoscopy (controversial) | Evidence weak |
| Fentanyl | 2-3 mcg/kg IV | Blunts sympathetic response, analgesia | Hypotension if large dose |
| Induction: | |||
| Ketamine | 1-2 mg/kg IV | Safe in TBI (old dogma incorrect), maintains BP, bronchodilator | Hypersalivation (give glycopyrrolate) |
| Etomidate | 0.3 mg/kg IV | Haemodynamically neutral, ↓ ICP | Adrenal suppression (single dose likely safe) |
| Propofol | 1-2 mg/kg IV | ↓ ICP, anti-seizure | Hypotension (avoid if haemodynamically unstable) |
| Thiopental | 3-5 mg/kg IV | ↓ ICP, cerebral protection | Significant hypotension |
| Paralysis: | |||
| Rocuronium | 1-1.2 mg/kg IV | Fast onset, predictable | Requires reversal (sugammadex) if failed intubation |
| Succinylcholine | 1-1.5 mg/kg IV | Faster onset, short duration | ↑ ICP (insignificant), contraindications (burns, crush) |
Post-Intubation Ventilation: [1]
- Mode: Volume control or pressure control
- Tidal volume: 6-8 mL/kg ideal body weight (lung-protective)
- Target PaCO₂: 35-40 mmHg (normocapnia)
- Hypocapnia (PaCO₂ less than 35) → vasoconstriction → cerebral ischaemia
- Hypercapnia (PaCO₂ > 45) → vasodilation → ↑ ICP
- Target PaO₂: > 80 mmHg (SpO₂ > 94%)
- PEEP: 5-10 cmH₂O (balance oxygenation vs venous return; excessive PEEP may ↑ ICP)
Haemodynamic Management
Blood Pressure Goals (BTF Guidelines 2016): [1,5]
| Age Group | Target SBP | Rationale |
|---|---|---|
| 50-69 years | > 110 mmHg | Optimises CPP [1] |
| 15-49 years or > 70 years | > 120 mmHg | Higher targets may improve outcomes [5] |
- Single episode of SBP less than 90 mmHg doubles mortality [5]
- Hypotension = strongest predictor of poor outcome (after age and GCS) [5]
Resuscitation Strategy:
- Fluid bolus: 20 mL/kg crystalloid (0.9% saline or Hartmann's)
- Vasopressors if persistent hypotension: Norepinephrine (0.05-0.5 mcg/kg/min) to maintain MAP > 80 mmHg
- Avoid hypotonic fluids (Dextrose 5%, 0.45% saline → cerebral oedema)
- Avoid Dextrose unless hypoglycaemic
- Blood products: If haemorrhagic shock (1:1:1 ratio RBC:FFP:platelets)
Cerebral Perfusion Pressure (CPP): [1]
- Target: 60-70 mmHg
- Formula: CPP = MAP - ICP
- Lower threshold (50-60 mmHg) may be acceptable if PbtO₂ adequate
- Higher CPP (> 70) → risk of ARDS (excessive fluid/pressors)
ICP Management
Tiered Approach (escalate sequentially): [1]
Tier 0 - Basic Measures (all severe TBI patients):
- Head of bed 30° (improves venous drainage; ensure head midline)
- Avoid jugular venous compression (loosen hard collar, no neck ties)
- Sedation and analgesia: Propofol 3-5 mg/kg/h or midazolam + fentanyl/remifentanil
- Normothermia: Target 36-37°C (paracetamol, cooling blanket if febrile)
- Normoglycaemia: 6-10 mmol/L (insulin infusion if needed)
- Normonatraemia: Na+ 135-145 mmol/L initially
- Prevent hypoxia: SpO₂ > 94%, PaO₂ > 80 mmHg
- Prevent hypotension: SBP > 110-120 mmHg
- Maintain normocapnia: PaCO₂ 35-40 mmHg
- Seizure control: Treat clinically evident seizures (consider EEG monitoring for subclinical)
- Evacuate mass lesions if surgical criteria met
Tier 1 - Osmotherapy (if ICP > 22 mmHg despite Tier 0): [1,7]
| Agent | Dose | Mechanism | Onset | Duration | Monitoring | Contraindications |
|---|---|---|---|---|---|---|
| Hypertonic saline 3% | 250-500 mL IV over 15 min | Osmotic gradient → draws fluid intravascularly | 15-30 min | 4-6 hours | Na+ every 4-6h (target 145-155) | Hypernatraemia > 160 |
| Hypertonic saline 23.4% | 30 mL IV push (via central line preferred) | Rapid osmotic effect | 5-15 min | 2-4 hours | Continuous infusion pump, Na+ monitoring | Requires central access |
| Mannitol | 1-1.5 g/kg IV (20% solution) over 15 min | Osmotic diuresis + ↓ blood viscosity | 15-30 min | 4-6 hours | Serum osmolality less than 320 mOsm/kg; urine output | Hypotension, renal failure, osmolality > 320 |
Hypertonic saline vs Mannitol: [7]
- HTS may have faster onset and sustained effect
- Mannitol has diuretic effect (risk of hypotension/hypovolaemia)
- No clear superiority in meta-analyses; institutional preference
Tier 2 - Advanced Therapies (if ICP refractory to Tier 1): [1]
Hyperventilation (rescue only, temporary): [1]
- Target PaCO₂: 30-35 mmHg (NOT less than 30 mmHg)
- Mechanism: Vasoconstriction → ↓ cerebral blood volume → ↓ ICP
- Problem: ↓ Cerebral blood flow → ischaemia
- Use: Bridge to definitive surgery only (30-60 minutes maximum)
- Monitor: SjvO₂ or PbtO₂ to detect ischaemia
Barbiturate Coma (Pentobarbital): [1]
- Indication: Refractory intracranial hypertension despite maximal medical therapy and surgery
- Mechanism: ↓ Cerebral metabolic rate → ↓ CBF → ↓ ICP
- Dose: Loading 10 mg/kg over 30 min, then 5 mg/kg/h × 3 doses, then 1-2 mg/kg/h
- Monitoring: EEG (target burst suppression), haemodynamics (causes profound hypotension → requires vasopressors)
- Complications: Hypotension, immunosuppression (infection), ileus
Hypothermia (Targeted Temperature Management): [1]
- Controversial: Eurotherm 3235 trial showed harm with hypothermia 32-35°C [1]
- Not routinely recommended outside clinical trials
- Avoid fever (target normothermia 36-37°C)
Decompressive Craniectomy (surgical ICP control): [13]
- Indication: Refractory ICP > 25 mmHg despite maximal medical therapy; large hemispheric stroke; malignant MCA syndrome
- Procedure: Large (12-15 cm diameter) frontotemporal-parietal bone flap removed; dura opened (duroplasty); allows brain to herniate outwards (relieving pressure on brainstem)
- Evidence: DECRA trial showed ↓ ICP and ICU stay but ↑ unfavourable outcomes (vegetative state) [13]; RESCUEicp showed ↓ mortality but ↑ severe disability [13]
- Conclusion: Reduces death but increases severe disability; discuss with family
- Timing: Earlier may be better (before irreversible brainstem injury)
Coagulopathy Reversal
Critical in Traumatic ICH - every minute counts: [8,9]
| Anticoagulant | Reversal Agent | Dose | Adjuncts | Time to Reversal |
|---|---|---|---|---|
| Warfarin | 4-Factor PCC (Beriplex, Octaplex) | 25-50 units/kg IV (based on INR) | Vitamin K 10 mg IV (takes 6-12 hours but sustains reversal) | less than 15 minutes |
| Alternative: FFP (if PCC unavailable) | 15-30 mL/kg | Slower, requires large volume, risk of fluid overload | 2-4 hours | |
| Dabigatran (Pradaxa) | Idarucizumab (Praxbind) | 5 g IV (2 × 2.5 g boluses 15 min apart) | None | less than 15 minutes |
| Alternative: haemodialysis | 4 hours | Removes 60% | Hours | |
| Rivaroxaban, Apixaban (Factor Xa inhibitors) | Andexanet alfa (Ondexxxa) | 400-800 mg IV bolus then infusion | Consider 4F-PCC if andexanet unavailable (off-label) | 2-5 minutes |
| Alternative: 4F-PCC (off-label) | 50 units/kg | Weaker evidence | 30 min | |
| Heparin (UFH) | Protamine sulphate | 1 mg per 100 units heparin (max 50 mg) | Give slowly (risk anaphylaxis) | 5 min |
| LMWH (enoxaparin) | Protamine (partial reversal) | 1 mg per 1 mg enoxaparin (if less than 8h since dose) | Only 60% reversal | 15 min |
| Aspirin, Clopidogrel | Platelet transfusion (if emergency surgery) | 1-2 units | Desmopressin (DDAVP) 0.3 mcg/kg (weak evidence) | 30 min |
Tranexamic Acid (TXA) in TBI: [15]
- CRASH-3 Trial (2019): TXA 1 g IV over 10 min, then 1 g over 8 hours
- Benefit: ↓ Head injury-related death if given less than 3 hours from injury AND mild-moderate TBI (GCS 9-15)
- No benefit in severe TBI (GCS 3-8)
- Harm if given > 3 hours post-injury
- Current recommendation: Consider in mild-moderate TBI if within 3 hours [15]
Seizure Management
Prophylaxis: [10]
| Indication | Agent | Dose | Duration | Evidence |
|---|---|---|---|---|
| High-risk TBI (GCS ≤10, cortical contusion, depressed skull fracture, SDH, EDH, penetrating injury, seizure within 24h) | Levetiracetam (first-line) | 20 mg/kg IV load (max 3 g), then 500-1000 mg IV BID | 7 days | Prevents early seizures (less than 7 days); NO effect on late seizures [10] |
| Alternative: Phenytoin | 20 mg/kg IV load (max 50 mg/min), then 100 mg IV TDS | 7 days | Equivalent efficacy; more side effects |
Does NOT reduce long-term epilepsy risk - only prevents early post-traumatic seizures. [10]
Treatment of Active Seizures:
- Benzodiazepines: Lorazepam 4 mg IV or Midazolam 10 mg IM
- Loading dose antiepileptic: Levetiracetam 20 mg/kg IV or Phenytoin 20 mg/kg IV
- If status epilepticus: Intubate, midazolam/propofol infusion, EEG monitoring
Surgical Management
Neurosurgical Consultation - Immediate for: [11]
- GCS ≤8 (severe TBI)
- Deteriorating GCS (≥2 point drop)
- Mass lesion on CT (EDH, SDH, IPH)
- Depressed or open skull fracture
- Penetrating injury
- Signs of herniation
Surgical Indications (BTF Guidelines): [1,11]
| Lesion | Surgical Criteria | Procedure | Evidence |
|---|---|---|---|
| Epidural haematoma | Volume > 30 mL OR thickness > 15 mm OR midline shift > 5 mm OR GCS ≤8 with pupillary abnormality | Craniotomy, evacuation, MMA ligation | Class III (observational) |
| Can observe if: less than 30 mL, less than 15 mm thick, less than 5 mm shift, GCS > 8, no focal deficit | Serial CT (initially 6h), close monitoring | ||
| Subdural haematoma (acute) | Thickness > 10 mm OR midline shift > 5 mm OR GCS decline ≥2 OR pupil asymmetry | Craniotomy, evacuation ± duroplasty | Saves lives (Class III) |
| Subdural haematoma (chronic) | Symptomatic (headache, confusion, focal deficit) | Burr hole drainage (vs craniotomy) | High recurrence rate (~30%) |
| Intraparenchymal haematoma | Volume > 50 mL OR progressive neurological deterioration OR refractory ICP | Craniotomy, evacuation | Selected cases only |
| Posterior fossa haematoma | Any mass effect, hydrocephalus, clinical deterioration | Suboccipital craniectomy ± EVD | Rapidly fatal if not decompressed |
| Depressed skull fracture | Open (compound) OR depression > 1 table thickness OR cosmetically significant | Elevation, debridement | Prevent infection (open) |
| Penetrating injury | Most cases | Debridement, haemostasis, dural repair | Do NOT remove impaled object in field |
External Ventricular Drain (EVD):
- Treat hydrocephalus (blood in ventricles)
- ICP monitoring + therapeutic CSF drainage
- Infection risk (~10% if > 5 days)
Decompressive Craniectomy: [13]
- Large bone flap (12-15 cm) removed; dura opened
- Allows brain to swell outwards
- Cranioplasty (replace bone or titanium plate) at 3-6 months
- Patient needs helmet until cranioplasty
Post-Operative Care
- ICU monitoring: ICP, CPP, pupils, GCS
- Repeat CT: Immediately post-op, then 12-24 hours, or if deterioration
- Seizure prophylaxis: Levetiracetam × 7 days
- VTE prophylaxis: Mechanical (TED stockings, sequential compression) immediately; chemical (LMWH) when safe (typically 24-48h post-op if no expansion on repeat CT)
- Nutrition: Early enteral feeding (NG/NJ tube) within 72 hours
- Glycaemic control: Target 6-10 mmol/L (avoid hypoglycaemia)
- Stress ulcer prophylaxis: PPI or H2-blocker
- Mobilisation: Physiotherapy as soon as safe
Disposition and Follow-Up
Admission Criteria
ICU Admission: [1]
- GCS ≤8 (severe TBI)
- Intubated
- ICP monitoring required
- Haemodynamic instability
- Post-operative neurosurgical care
- Large intracranial haematoma (even if conservative management)
- Rapidly evolving neurological status
Ward Admission (neurosurgical or trauma ward):
- GCS 9-14 (mild-moderate TBI)
- Intracranial injury on CT not requiring surgery
- Persistent symptoms (headache, vomiting, confusion)
- Age > 65 with any head injury (even normal CT)
- Anticoagulated with positive CT
- No reliable observer at home
- Suspected non-accidental injury (safeguarding)
Observation Unit (6-24 hours):
- GCS 15, low-risk mechanism, no high-risk features BUT: intoxication, live alone, social concerns
Discharge Criteria (Mild TBI, GCS 15)
Safe to discharge if ALL of: [12]
- GCS 15 AND neurologically intact
- Normal CT (if performed) OR low-risk by Canadian CT Head Rule (no CT needed)
- Symptoms resolving (mild headache acceptable)
- Reliable adult to observe × 24 hours
- Written head injury advice understood
- Transport home available
- Access to ED if deteriorates
Do NOT discharge if:
- Anticoagulated (even if normal CT - observe 8-24 hours, repeat CT) [4,12]
- Intoxicated (cannot assess GCS accurately)
- Homeless (no observer)
- Suspected abuse (safeguard)
Head Injury Discharge Instructions
Provide written instructions (patient + observer): [12]
What to expect:
- Mild headache, fatigue, difficulty concentrating normal for 7-14 days
- Most symptoms resolve within 2-4 weeks
Activity restrictions:
- Rest for 24-48 hours (physical and cognitive)
- No alcohol × 48 hours minimum
- No driving until symptom-free
- No contact sports until cleared by doctor (minimum 7 days)
- Gradual return to work/school as tolerated
Return to ED immediately if: [12]
- Worsening or severe headache
- Repeated vomiting (> 2 episodes)
- Increasing drowsiness or confusion
- Difficulty waking up from sleep
- Seizure or fit
- Weakness or numbness in arms/legs
- Slurred speech
- One pupil larger than the other
- Clear fluid from nose or ear
- Loss of consciousness
Observer instructions:
- Check patient every 2-4 hours (including overnight - can wake for brief check)
- Ensure patient can wake, talk, walk
- Call 999 if concerned
Follow-Up
| Scenario | Follow-Up | Purpose |
|---|---|---|
| Mild TBI, normal CT, discharged | GP in 7-14 days | Assess symptom resolution; return-to-work/sport clearance |
| Mild TBI, positive CT, conservative | Neurosurgery outpatient 1-2 weeks | Repeat imaging; assess for delayed surgery |
| Moderate TBI | Neurosurgery + rehabilitation | Cognitive assessment, physio, OT |
| Severe TBI | MDT: Neurosurgery, rehabilitation, neuropsychology | Long-term cognitive/physical rehab |
| Anticoagulated, ICH | Haematology + neurosurgery | Restart anticoagulation decision (typically 4-8 weeks if needed) |
| Athletes (concussion) | Sports medicine | Graduated return-to-play protocol (minimum 7 days) |
Rehabilitation
Early rehabilitation improves outcomes: [14]
Domains:
- Physical: Mobility, balance, strength
- Cognitive: Memory, attention, executive function
- Speech and language: Aphasia, dysarthria
- Psychological: Depression, PTSD, anxiety (common post-TBI)
- Vocational: Return to work support
Services:
- Acute: Physiotherapy, OT, SALT on ward
- Post-acute: Neurorehabilitation unit (if severe disability)
- Outpatient: Community neurorehabilitation team
- Specialist: Headway (UK charity), brain injury case managers
Prognosis factors: [2]
- Best predictors: Age, GCS, pupil reactivity, CT findings (Marshall classification)
- Severe TBI (GCS 3-8): 30-40% mortality; 50% survivors have significant disability
- Moderate TBI (GCS 9-12): 10% mortality; 60% good recovery
- Mild TBI (GCS 13-15): less than 1% mortality; 80-90% good recovery
- Post-concussion syndrome: 10-15% have persistent symptoms > 3 months (headache, fatigue, concentration problems)
Special Populations
Anticoagulated Patients
Highest Risk Group: [4]
| Risk Factor | Relative Risk of ICH |
|---|---|
| Warfarin | 3-5× increased risk |
| DOACs | 2-3× increased risk |
| Antiplatelet (aspirin, clopidogrel) | 1.5-2× increased risk |
Management Principles:
- Low threshold for CT (even minor mechanism)
- Immediate reversal if ICH present (see Coagulopathy Reversal table)
- Repeat CT at 6-24 hours (delayed haemorrhage common) [4,12]
- Observe minimum 8-24 hours even if initial CT normal [12]
- Do NOT restart anticoagulation for 4-8 weeks if ICH (haematology/neurosurgery decision)
NICE Guidance: Admit for observation ≥8 hours if on anticoagulant/antiplatelet AND head injury, even if GCS 15. [12]
Elderly (Age > 65 Years)
High-Risk Features: [2,4]
- Brain atrophy → bridging veins stretched → ↑ SDH risk
- Often on anticoagulation (AF, VTE, mechanical valve)
- Falls are leading mechanism
- Comorbidities worsen outcomes
- Higher mortality at same GCS
Management:
- Age ≥65 is Canadian CT Head Rule high-risk criterion (CT mandatory) [6]
- Low threshold for admission (even GCS 15)
- Consider causes of fall (syncope, arrhythmia, medication)
- Safeguarding assessment (elder abuse, neglect, unsafe home environment)
Paediatric (Age less than 16 Years)
Use PECARN Rules (not Canadian CT Head Rule): [16]
Age less than 2 years - CT if:
- GCS ≤14
- Palpable skull fracture
- Altered mental status
- Scalp haematoma (non-frontal)
- LOC ≥5 seconds
- Severe mechanism
- Not acting normally per parent
Age ≥2 years - CT if:
- GCS ≤14
- Signs of basilar skull fracture
- Altered mental status
- LOC
- Severe mechanism
- Severe headache/vomiting
Non-Accidental Injury (NAI) - suspect if: [16]
- History inconsistent with injuries
- Delay in presentation
- Multiple injuries of different ages
- Retinal haemorrhages (shaken baby syndrome)
- Subdural haematoma in infant
- Rib/metaphyseal fractures
Athletes (Sports-Related Concussion)
Concussion = Mild TBI (GCS 13-15): [17]
Acute Management:
- Remove from play immediately (same-day return contraindicated)
- Assess with SCAT5 (Sport Concussion Assessment Tool)
- CT if high-risk features
Return-to-Play Protocol (minimum 7 days): [17]
- Complete rest (24-48 hours)
- Light aerobic exercise (walking, stationary bike)
- Sport-specific exercise (no contact)
- Non-contact training drills
- Full-contact practice (medical clearance)
- Return to game
Each stage minimum 24 hours; if symptoms recur, return to previous stage.
Second Impact Syndrome: Rare but catastrophic - second concussion before first has healed → malignant cerebral oedema → death. [17]
Chronic Traumatic Encephalopathy (CTE): Long-term sequela of repetitive head impacts (boxing, rugby, American football) → dementia, parkinsonism. [17]
Penetrating Trauma
Gunshot/Stab Wounds to Head: [1]
Pre-Hospital:
- Do NOT remove impaled object (tamponading bleeding)
- Immobilise object with bulky dressings
Hospital Management:
- High-dose antibiotics (ceftriaxone 2 g + metronidazole 500 mg IV)
- Tetanus prophylaxis
- CT head + CTA (trajectory, vascular injury)
- Urgent neurosurgical debridement
- High mortality (especially if transventricular trajectory)
Quality Metrics and Clinical Pearls
Performance Indicators
| Metric | Target | Rationale | Evidence |
|---|---|---|---|
| CT head within 1 hour (severe TBI) | 100% | Rapid diagnosis enables treatment | NICE CG176 [12] |
| Hypoxia avoided (SpO₂ > 94%) | 100% | Prevents secondary injury | BTF Guidelines [1] |
| Hypotension avoided (SBP > 110) | 100% | Strongest modifiable predictor of outcome | Manley et al [5] |
| Neurosurgery consult (surgical lesion) | Within 1 hour | Time to surgery affects outcome | SBNS Guidelines |
| Coagulopathy reversal (INR less than 1.4) | Within 4 hours | Prevents haematoma expansion | PATCH Trial [8] |
| ICP monitoring (severe TBI) | > 90% | Guides therapy | BTF Guidelines [1] |
Key Clinical Pearls
Diagnostic Pearls:
- GCS 15 ≠ No intracranial injury: 5% with high-risk mechanism have CT findings [6]
- Lucid interval (classic EDH): Only 20-50% have true lucid interval; don't rely on it
- "Talk and die": 10-15% of fatal TBI patients were initially GCS 13-15 [2]
- Elderly fall + warfarin = CT mandatory: Even if "feels fine" [4]
- Look for cause of fall: Medical event (MI, PE, arrhythmia, stroke) often precipitates fall
- Basilar skull fracture signs delayed: Battle's sign and raccoon eyes appear 12-24 hours post-injury
- Small EDH can be lethal: Temporal location + arterial bleeding → rapid expansion
Treatment Pearls:
- "First, do no harm": Hypotension and hypoxia are preventable causes of death [5]
- Intubate at GCS ≤8: Don't wait for aspiration
- Ketamine is safe in TBI: Old teaching (↑ ICP) debunked [1]
- Hyperventilate ONLY as bridge to surgery: Causes ischaemia; temporary rescue only [1]
- Mannitol vs HTS: Both work; HTS may be faster and more sustained [7]
- Reverse anticoagulation immediately: Every 30 min delay → worse outcome [8]
- Osmotherapy requires functioning BBB: Won't work in DAI/massive oedema
- Barbiturate coma = last resort: Requires vasopressors, EEG; for refractory ICP only [1]
- TXA only if less than 3 hours: Benefit in mild-moderate TBI (GCS 9-15); harm if late or severe TBI [15]
- Normal ICP does NOT exclude brain injury: DAI, contusions can occur without raised ICP
Disposition Pearls:
- Anticoagulated patients need observation: Minimum 8-24 hours; repeat CT [4,12]
- Concussion: No same-day return to play: Minimum 7-day graduated protocol [17]
- Reliable observer is mandatory for discharge: Document name and phone number
- Post-concussion syndrome (10-15%): Persistent headache, fatigue, poor concentration > 3 months
- Early rehabilitation improves outcomes: Physio, OT, cognitive therapy [14]
Pitfalls to Avoid:
- ❌ Discharging intoxicated patient (cannot assess GCS)
- ❌ Discharging anticoagulated patient without observation
- ❌ Prolonged hyperventilation (causes ischaemia)
- ❌ Aggressive fluid restriction ("dry is good for brain") - causes hypotension
- ❌ Steroids in TBI (CRASH trial showed harm) [18]
- ❌ Prophylactic hypothermia (Eurotherm trial showed harm) [1]
- ❌ Missing non-accidental injury in children
- ❌ Removing impaled object from skull (pre-hospital)
Common Viva Questions
Opening Statement
"Describe your approach to an adult patient with head injury in the Emergency Department."
Model Answer:
"Head injury is a common presentation with a spectrum from minor scalp laceration to life-threatening traumatic brain injury. My approach follows ATLS principles, focusing on identifying those requiring neurosurgical intervention and preventing secondary brain injury.
I would perform a primary survey ensuring airway protection with c-spine immobilisation, adequate oxygenation, and haemodynamic stability. Hypotension and hypoxia are the strongest modifiable predictors of poor outcome and must be corrected immediately.
For disability, I would assess GCS (documenting individual E, V, M components) and pupillary response. GCS ≤8 requires intubation for airway protection. A unilateral dilated pupil suggests uncal herniation and is a neurosurgical emergency.
CT head is indicated based on the Canadian CT Head Rule or NICE guidelines - essentially any patient with GCS less than 15, high-risk mechanism, age ≥65, anticoagulation, focal deficit, or ≥2 episodes of vomiting.
Management priorities are: (1) Prevent secondary injury through maintaining CPP 60-70 mmHg, normoxia, normocapnia, normothermia; (2) Control ICP with head elevation, sedation, osmotherapy (hypertonic saline or mannitol) if indicated; (3) Reverse coagulopathy immediately if intracranial haemorrhage; (4) Early neurosurgical consultation for surgical lesions.
Disposition depends on severity: severe TBI (GCS ≤8) requires ICU with ICP monitoring; moderate TBI and CT-positive mild TBI require admission; carefully selected low-risk mild TBI can be discharged with a reliable observer and clear return precautions. This approach is based on the Brain Trauma Foundation Guidelines 2016."
Anticipated Follow-Up Questions
Q1: "What are the indications for intubation in head injury?"
A: GCS ≤8 (unable to maintain airway), hypoxia despite supplemental oxygen, need for controlled ventilation (hypercarbia), combativeness requiring sedation, and transport of severe TBI. I would use rapid sequence intubation with ketamine (safe in TBI contrary to old teaching) or etomidate for induction, and rocuronium for paralysis. Post-intubation, I target normocapnia (PaCO₂ 35-40 mmHg) as hypocapnia causes vasoconstriction and ischaemia.
Q2: "How do you manage raised intracranial pressure?"
A: I use a tiered approach. Tier 0 includes basic measures: head of bed 30°, head midline, adequate sedation and analgesia, normothermia, normoglycaemia, and avoiding hypotension/hypoxia. Tier 1 is osmotherapy - either hypertonic saline (3% or 23.4%) or mannitol 1-1.5 g/kg, monitoring serum sodium or osmolality. Tier 2 includes hyperventilation (only as temporary bridge to surgery, targeting PaCO₂ 30-35 mmHg), barbiturate coma (pentobarbital with EEG monitoring), or decompressive craniectomy for refractory ICP. The target is ICP less than 22 mmHg and CPP 60-70 mmHg based on Brain Trauma Foundation Guidelines.
Q3: "When would you consider surgery for a subdural haematoma?"
A: According to the Brain Trauma Foundation Guidelines, surgical evacuation is indicated if the acute subdural haematoma is > 10 mm thickness or causes > 5 mm midline shift, or if there is a GCS decline of ≥2 points attributable to the SDH, or if there is pupillary abnormality. Even if these criteria are not met, surgery may be needed for progressive neurological deterioration or refractory intracranial hypertension. I would involve neurosurgery immediately for any significant SDH.
Q4: "How do you reverse warfarin in a patient with traumatic intracranial haemorrhage?"
A: Immediate reversal is critical as every delay worsens outcome. First-line is 4-factor prothrombin complex concentrate (PCC) 25-50 units/kg IV based on the INR, which reverses warfarin within 15 minutes. I would also give vitamin K 10 mg IV which takes 6-12 hours but sustains the reversal. FFP is second-line (slower, requires large volume). Target is INR less than 1.4 within 4 hours. I would check INR at 30 minutes and repeat dose if needed.
Q5: "What is the role of tranexamic acid in traumatic brain injury?"
A: The CRASH-3 trial (2019) showed that tranexamic acid (1 g IV over 10 min, then 1 g over 8 hours) reduced head injury-related death when given within 3 hours of injury in patients with mild-to-moderate TBI (GCS 9-15). There was no benefit in severe TBI (GCS 3-8) and potential harm if given > 3 hours post-injury. Current recommendation is to consider it in mild-moderate TBI if presenting within 3 hours, but it's not standard practice in all centres.
Q6: "Describe the Canadian CT Head Rule."
A: The Canadian CT Head Rule applies to adults (≥16 years) with minor head injury (GCS 13-15) to determine who needs CT. There are high-risk criteria (100% sensitivity for neurosurgical intervention): GCS less than 15 at 2 hours, suspected open/depressed skull fracture, any sign of basilar skull fracture, ≥2 episodes of vomiting, or age ≥65. Medium-risk criteria (for brain injury on CT): retrograde amnesia ≥30 minutes or dangerous mechanism (pedestrian struck, ejection, fall > 1 metre/5 stairs). CT is indicated if ANY criterion present. It's not applicable if GCS less than 13, penetrating injury, or anticoagulation.
Q7: "What are the signs of brain herniation?"
A: Uncal herniation: ipsilateral dilated fixed pupil (CN III compression), contralateral hemiparesis, drowsiness progressing to coma - this is the classic emergency neurosurgical scenario. Central herniation: progressive bilateral midbrain dysfunction - small reactive pupils → mid-position fixed pupils → bilateral dilation, with Cheyne-Stokes breathing and posturing. Cushing's triad (hypertension, bradycardia, irregular respirations) indicates imminent herniation. Tonsillar herniation (cerebellar tonsils through foramen magnum) causes cardiorespiratory arrest. Immediate management is hyperventilation (temporary), osmotherapy (hypertonic saline or mannitol), and emergency neurosurgical decompression.
Q8: "What is the prognosis for severe traumatic brain injury?"
A: Severe TBI (GCS 3-8) has approximately 30-40% mortality despite optimal care. Of survivors, about 50% have significant long-term disability. The strongest predictors of poor outcome are: increasing age, low GCS (especially motor score), absent pupillary responses, hypotension, hypoxia, and CT findings (Marshall classification - worse with compressed cisterns, midline shift > 5 mm, large lesions). Diffuse axonal injury has particularly poor prognosis. However, outcomes have improved with adherence to evidence-based guidelines - prevention of secondary injury and early neurosurgical intervention are key.
References
-
Carney N, Totten AM, O'Reilly C, et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery. 2017;80(1):6-15. doi:10.1227/NEU.0000000000001432
-
Maas AIR, Stocchetti N, Bullock R. Moderate and severe traumatic brain injury in adults. Lancet Neurol. 2008;7(8):728-741. doi:10.1016/S1474-4422(08)70164-9
-
Godoy DA, Lubillo S, Rabinstein AA. Pathophysiology and management of intracranial hypertension and tissular brain hypoxia after severe traumatic brain injury: an integrative approach. Neurosurg Clin N Am. 2018;29(2):195-212. doi:10.1016/j.nec.2017.11.004
-
Riccardi A, Frumento F, Guiddo G, et al. Traumatic intracranial hemorrhage in patients on antithrombotic agents. J Emerg Trauma Shock. 2013;6(3):238-245. doi:10.4103/0974-2700.115323
-
Manley G, Knudson MM, Morabito D, et al. Hypotension, hypoxia, and head injury: frequency, duration, and consequences. Arch Surg. 2001;136(10):1118-1123. doi:10.1001/archsurg.136.10.1118
-
Stiell IG, Wells GA, Vandemheen K, et al. The Canadian CT Head Rule for patients with minor head injury. Lancet. 2001;357(9266):1391-1396. doi:10.1016/S0140-6736(00)04561-X
-
Kamel H, Navi BB, Nakagawa K, et al. Hypertonic saline versus mannitol for the treatment of elevated intracranial pressure: a meta-analysis of randomized clinical trials. Crit Care Med. 2011;39(3):554-559. doi:10.1097/CCM.0b013e318206b9be
-
Steiner T, Poli S, Griebe M, et al. Fresh frozen plasma versus prothrombin complex concentrate in patients with intracranial haemorrhage related to vitamin K antagonists (PATCH): a randomised trial. Lancet Neurol. 2016;15(6):566-573. doi:10.1016/S1474-4422(16)00110-1
-
Pollack CV Jr, Reilly PA, van Ryn J, et al. Idarucizumab for dabigatran reversal - full cohort analysis. N Engl J Med. 2017;377(5):431-441. doi:10.1056/NEJMoa1607278
-
Temkin NR, Dikmen SS, Wilensky AJ, et al. A randomized, double-blind study of phenytoin for the prevention of post-traumatic seizures. N Engl J Med. 1990;323(8):497-502. doi:10.1056/NEJM199008233230801
-
Bullock MR, Chesnut R, Ghajar J, et al. Surgical management of acute epidural hematomas. Neurosurgery. 2006;58(3 Suppl):S7-15. doi:10.1227/01.NEU.0000210363.91172.A8
-
National Institute for Health and Care Excellence. Head injury: assessment and early management. Clinical guideline [CG176]. Published January 2014. Updated May 2023. https://www.nice.org.uk/guidance/cg176
-
Cooper DJ, Rosenfeld JV, Murray L, et al. Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med. 2011;364(16):1493-1502. doi:10.1056/NEJMoa1102077
-
Turner-Stokes L, Pick A, Nair A, et al. Multi-disciplinary rehabilitation for acquired brain injury in adults of working age. Cochrane Database Syst Rev. 2015;(12):CD004170. doi:10.1002/14651858.CD004170.pub3
-
CRASH-3 trial collaborators. Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): a randomised, placebo-controlled trial. Lancet. 2019;394(10210):1713-1723. doi:10.1016/S0140-6736(19)32233-0
-
Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160-1170. doi:10.1016/S0140-6736(09)61558-0
-
McCrory P, Meeuwisse W, Dvorak J, et al. Consensus statement on concussion in sport-the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. 2017;51(11):838-847. doi:10.1136/bjsports-2017-097699
-
CRASH trial collaborators. Effect of intravenous corticosteroids on death within 14 days in 10008 adults with clinically significant head injury (MRC CRASH trial): randomised placebo-controlled trial. Lancet. 2004;364(9442):1321-1328. doi:10.1016/S0140-6736(04)17188-2
-
Chesnut RM, Temkin N, Carney N, et al. A trial of intracranial-pressure monitoring in traumatic brain injury. N Engl J Med. 2012;367(26):2471-2481. doi:10.1056/NEJMoa1207363
-
Hutchinson PJ, Kolias AG, Timofeev IS, et al. Trial of decompressive craniectomy for traumatic intracranial hypertension. N Engl J Med. 2016;375(12):1119-1130. doi:10.1056/NEJMoa1605215
High-Yield Facts for Spaced Repetition:
- GCS ≤8 requires intubation for airway protection
- Canadian CT Head Rule high-risk criteria: GCS less than 15 at 2 hours, suspected skull fracture, basilar skull fracture signs, ≥2 vomiting episodes, age ≥65
- Uncal herniation classic sign: Ipsilateral dilated pupil (CN III compression)
- CPP = MAP - ICP; target CPP 60-70 mmHg
- Osmotherapy for raised ICP: Mannitol 1-1.5 g/kg or Hypertonic saline 23.4% 30 mL
- Warfarin reversal: 4-Factor PCC 25-50 units/kg + Vitamin K 10 mg IV
- Dabigatran reversal: Idarucizumab 5 g IV
- Subdural haematoma surgical indications: thickness > 10 mm or midline shift > 5 mm
- Epidural haematoma surgical indications: volume > 30 mL or thickness > 15 mm
- Seizure prophylaxis duration post-TBI: 7 days (prevents early, NOT late seizures)
- Single episode SBP less than 90 mmHg doubles mortality in TBI
- Target PaCO₂ in ventilated TBI patient: 35-40 mmHg (normocapnia)
- Hyperventilation target PaCO₂: 30-35 mmHg (temporary bridge to surgery only)
- ICP treatment threshold: > 22 mmHg
- TXA in TBI: benefit if given less than 3 hours in mild-moderate TBI (GCS 9-15)
- Cushing's triad: Hypertension, bradycardia, irregular respirations
- Marshall CT Classification Diffuse Injury III: cisterns compressed/absent, midline shift 0-5 mm
- Return-to-play after concussion: minimum 7 days graduated protocol
- Severe TBI mortality: 30-40%
- Battle's sign appears 12-24 hours post-injury
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Neurological Examination
Differentials
Competing diagnoses and look-alikes to compare.
- Stroke (Ischaemic and Haemorrhagic)
- Syncope
Consequences
Complications and downstream problems to keep in mind.
- Intracranial Haemorrhage
- Status Epilepticus