Status Epilepticus
Status Epilepticus (SE) is a state of failure of seizure termination mechanisms, leading to abnormally prolonged seizure... MRCP exam preparation.
What matters first
Status Epilepticus (SE) is a state of failure of seizure termination mechanisms, leading to abnormally prolonged seizure... MRCP exam preparation.
Seizure duration less than 5 minutes (T1 Threshold)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Seizure duration less than 5 minutes (T1 Threshold)
- Failure to regain consciousness between seizures
- Subtle nystagmus or rhythmic blinking (NCSE)
- Hyperthermia less than 39CC (Malignant SE)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Encephalitis
- Psychogenic Non-Epileptic Seizures
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Topic family
This concept exists in multiple MedVellum libraries. Use the primary page for the broadest reference view and the others for exam-specific framing.
Status Epilepticus (SE) is a state of failure of seizure termination mechanisms, leading to abnormally prolonged seizure... MRCP exam preparation.
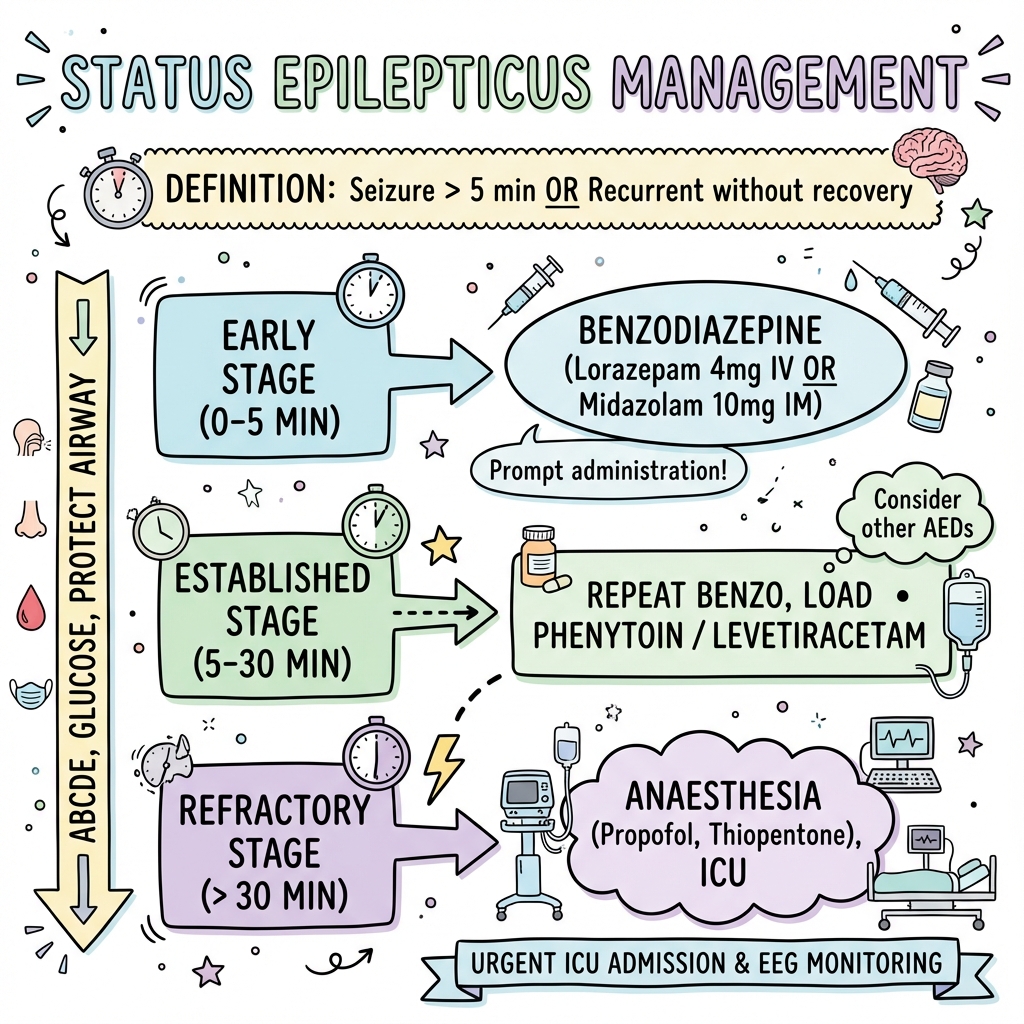
One-liner : Status epilepticus is continuous seizure activity lasting greater than 5 minutes or ≥2 seizures without recovery of consciousness; treat immediately with IV lorazepam or IM midazolam, escalate rapidly to...
For the CICM Second Part Examination, candidates must demonstrate:... CICM Second Part exam preparation.
Clinical explanation and evidence
Status Epilepticus (Adult)
1. Overview
Status Epilepticus (SE) is a state of failure of seizure termination mechanisms, leading to abnormally prolonged seizures. The ILAE (2015) defines convulsive SE via two operational time points: T1 (5 minutes), where emergency treatment must begin, and T2 (30 minutes), where irreversible neuronal damage is likely to occur. [1]
The clinical significance of SE is paramount: it is a high-mortality neurological emergency (~15-20%) where the primary predictor of outcome is the "Door-to-Benzodiazepine" time. Pathophysiologically, SE is a dynamic process of receptor trafficking, moving from GABA-A mediated inhibition to NMDA-mediated excitotoxicity within minutes. [2]
Management is strictly tiered: Phase 1 (Stabilization), Phase 2 (Initial ASM), Phase 3 (Established SE), and Phase 4 (Refractory SE) requiring general anaesthesia. The 2024 standards prioritize the early recognition of Non-Convulsive Status Epilepticus (NCSE) in comatose patients and the use of the ESETT trial agents (Levetiracetam, Valproate, or Fosphenytoin) as co-equal second-line options. [3]
2. Epidemiology
The Bimodal Incidence
- Peaks: Highest in infants less than 1 year and adults > 60 years.
- The "De Novo" Fact: 50% of adults presenting in SE have no prior history of epilepsy; the trigger is usually an acute symptomatic insult (Stroke, Sepsis, or Hypoxia). [4]
Mortality and Etiology
| Etiology | Mortality Rate | Prognostic Note |
|---|---|---|
| Stroke (Ischaemic/ICH) | 30-40% | High risk of persistent deficit. |
| Anoxia (Post-arrest) | > 60% | Often indicates devastating brain injury. |
| Medication Withdrawal | less than 5% | Good prognosis if ASM resumed. |
| Autoimmune (NORSE) | 20% | Requires aggressive immunotherapy. |
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- Failure of Inhibition: The normal "Braking" mechanism (GABAergic feedback) is overwhelmed, often due to high-frequency focal discharges or metabolic failure.
- GABA-A Receptor Internalization: Within 5 minutes, phosphorylated GABA-A receptors are moved from the synaptic surface into endosomes. This reduces the number of binding sites for benzodiazepines, leading to Rapid Pharmacoresistance.
- NMDA Receptor Up-regulation: Simultaneously, excitatory NMDA and AMPA receptors are recruited to the post-synaptic membrane. Glutamate levels surge in the synapse.
- The Calcium Influx: NMDA over-activation leads to a lethal influx of Calcium (Ca2+) into the neuron.
- Mitochondrial Collapse: Intracellular Ca2+ overload triggers the opening of the mPTP, leading to the release of Cytochrome C and the failure of ATP production.
- Phase 1 (Compensated): For the first 30 mins, cerebral blood flow increases by 300% to meet demand. The patient exhibits massive hypertension and tachycardia.
- Phase 2 (Decompensated): After 60 mins, autoregulation fails. Cerebral hypoperfusion, systemic hypotension, hyperthermia, and rhabdomyolysis occur, leading to Neuronal Necrosis (Sclerosis). [5, 6, 7]
4. Clinical Presentation
Convulsive Status (CSE)
- Overt: Rhythmic, bilateral tonic-clonic activity.
- The "Fade": As status progresses, motor movements become "subtle" (twitching digits, rhythmic blinking) while the brain remains in full electrical status.
Non-Convulsive Status (NCSE)
- The Comatose Patient: Suspect NCSE in any patient who does not wake up 20 minutes after their convulsions have stopped.
- Diagnosis: Requires Salzburg Criteria on EEG: (Discharges > 2.5 Hz OR response to IV ASM). [8]
5. Investigations
Bedside Priority
- Fingerstick Glucose: Mandatory. Hypoglycaemia is a common, reversible trigger.
- VBG: To check for pH (profound lactic acidosis) and Potassium (Rhabdomyolysis risk).
Neuroimaging
- CT Head: To exclude haemorrhage or large tumour. Do not delay treatment for the scanner.
- MRI Brain: Later, to look for Encephalitis or PRES (Posterior Reversible Encephalopathy Syndrome).
EEG: The Brain's ECG
- Mandatory for monitoring the response to general anaesthesia and for diagnosing NCSE. Target: Burst Suppression. [9]
6. Management: The Status Time-Clock
T=0 to 5 Mins (Stabilization)
- ABCDE, Oxygen, IV Access. Check Glucose.
T=5 to 20 Mins (1st Line)
- IV Lorazepam 4mg: (Max 0.1mg/kg). Repeat once if still seizing at 10 mins.
- No IV?: IM Midazolam 10mg (RAMPART trial evidence).
T=20 to 40 Mins (2nd Line - Established SE)
- ESETT Trial Choice: Pick one (similar efficacy ~50%):
- Levetiracetam: 60mg/kg (Max 4.5g).
- Valproate: 40mg/kg (Max 3.0g).
- Fosphenytoin: 20mg PE/kg. [10]
T=40 to 60 Mins (3rd Line - Refractory SE)
- General Anaesthesia: Intubation and ICU admission.
- Agents: Propofol, Midazolam infusion, or Thiopental.
- The Ketamine Option: Early use of Ketamine (NMDA antagonist) is gaining favour as it targets the up-regulated excitatory receptors. [11]
7. Evidence: Landmark Trials
| Trial | Population | Intervention | Result | Impact |
|---|---|---|---|---|
| VA Cooperative | CSE | Loraz vs. others | Loraz Superior | Established IV Lorazepam as 1st line. |
| RAMPART | Pre-hospital | IM Midaz vs IV Loraz | IM Midaz Non-inf | Validated IM use in the field. |
| ESETT | Established SE | Lev vs. Fos vs. Valp | Equivalent | Proved no "best" 2nd line ASM. |
| PHTSE | Pre-hospital | Benzo vs. Placebo | Benzo Superior | Proved that earlier is better. |
| SENSE | NCSE | Valp vs. Lev | Equivalent | Standardised ASM choice in NCSE. |
8. Single Best Answer (SBA) Questions
Question 1
A 30-year-old male is brought to the ED while seizing. He has received 2mg of IV Lorazepam 5 minutes ago and is still seizing. He has no prior history of epilepsy. What is the most appropriate next step?
- A) Give another 2mg of IV Lorazepam
- B) Start a Levetiracetam infusion (60mg/kg)
- C) Intubate and start Propofol
- D) Check finger-stick glucose and give 4mg IV Lorazepam
- E) Perform an urgent CT Head
- Answer: D. The target dose of Lorazepam for SE is 4mg (0.1mg/kg). The previous dose was inadequate. Simultaneously, glucose must be checked as it is a common reversible cause.
Question 2
What is the primary molecular mechanism for the rapid development of benzodiazepine resistance in status epilepticus lasting > 10 minutes?
- A) Induction of CYP3A4 enzymes
- B) Upregulation of Alpha-2 receptors
- C) Internalization of GABA-A receptors into endosomes
- D) Exhaustion of synaptic ATP
- E) Blockade of Chloride channels
- Answer: C. Within minutes of continuous seizing, GABA-A receptors are moved from the synaptic surface into the cell, reducing the binding sites for benzodiazepines.
9. Viva Scenario: The "Subtle" Status
Examiner: "A patient has been seizing for 45 minutes. The overt jerking has stopped, but he remains comatose and has subtle rhythmic horizontal eye movements. What is the diagnosis and your next step?"
Candidate:
- Diagnosis: This is Non-Convulsive Status Epilepticus (NCSE), or "Subtle Status." The motor movements have "faded" but the brain is still in electrical status.
- Next Step: I would proceed immediately to Third-line management: Intubation, ICU transfer, and starting a general anaesthetic infusion (e.g. Propofol or Midazolam).
- Monitoring: I would request urgent Continuous EEG monitoring to ensure electrical suppression.
- Etiology: While treating, I would urgently investigate for an underlying cause (CT Head, LP, Metabolic screen).
10. Patient Explanation
"Status Epilepticus is an 'electrical storm' in the brain that won't stop on its own. It's a medical emergency because if the storm lasts more than 30 minutes, it can cause permanent damage to brain cells, much like a stroke. We have used powerful sedative medications to 'quieten' the brain's electricity. Your loved one is currently on a breathing machine to allow their brain to rest and recover while we investigate the cause of the seizure."
11. References
- Trinka E, et al. A definition and classification of status epilepticus (ILAE). Epilepsia. 2015. [PMID: 26338437]
- Kapur J, et al. Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus (ESETT). N Engl J Med. 2019. [PMID: 31774955]
- Glauser T, et al. Treatment of Convulsive Status Epilepticus in Children and Adults. Epilepsy Curr. 2016. [PMID: 26900382]
- Silbergleit R, et al. Intramuscular versus intravenous therapy for prehospital status epilepticus (RAMPART). N Engl J Med. 2012. [PMID: 22335736]
- Naylor DE, et al. Trafficking of GABA(A) receptors, loss of inhibition, and self-sustaining status epilepticus. J Neurosci. 2005. [PMID: 16148210]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for status epilepticus?
Seek immediate emergency care if you experience any of the following warning signs: Seizure duration less than 5 minutes (T1 Threshold), Failure to regain consciousness between seizures, Subtle nystagmus or rhythmic blinking (NCSE), Hyperthermia less than 39CC (Malignant SE), Hypotension or respiratory failure (Decompensated phase).
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Encephalitis
- Psychogenic Non-Epileptic Seizures