Heart Failure
Heart Failure (HF) is a complex clinical syndrome characterised by the heart's inability to maintain sufficient cardiac ... MRCP exam preparation.
What matters first
Heart Failure (HF) is a complex clinical syndrome characterised by the heart's inability to maintain sufficient cardiac ... MRCP exam preparation.
Acute respiratory distress (pulmonary oedema)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Acute respiratory distress (pulmonary oedema)
- Cardiogenic shock (SBP less than 90 mmHg, cold peripheries)
- New-onset AF with rapid ventricular response
- Acute Coronary Syndrome (ACS) as precipitant
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- COPD Exacerbation
- Pulmonary Embolism
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Heart Failure (Adult)
1. Overview
Heart Failure (HF) is a complex clinical syndrome characterised by the heart's inability to maintain sufficient cardiac output to meet metabolic demands, or doing so only at elevated filling pressures. It is the final common pathway for most cardiac diseases and remains the leading cause of hospitalisation in adults over 65. Historically a "death sentence," the 21st-century management of HF has been transformed by neurohormonal blockade and targeted metabolic therapies. [1]
The syndrome is defined by a constellation of symptoms (dyspnoea, fatigue) and signs (oedema, raised JVP) resulting from structural or functional cardiac abnormalities. Modern classification is anchored in the Left Ventricular Ejection Fraction (LVEF): HFrEF (Reduced, ≤40%), HFmrEF (Mildly Reduced, 41-49%), and HFpEF (Preserved, ≥50%). [2]
Management has shifted from a sequential "step-up" approach to a rapid initiation of the "Four Pillars" of guideline-directed medical therapy (GDMT) within weeks of diagnosis, a strategy proven to significantly reduce 90-day readmissions and mortality. [3]
2. Epidemiology
Global Distribution
HF affects over 64 million people worldwide. While incidence is stabilising in high-income countries due to better management of IHD and hypertension, prevalence is rising due to an ageing population and improved survival after myocardial infarction. [4]
| Demographic Factor | Impact on Prevalence | Mechanism |
|---|---|---|
| Age > 70 | > 10% prevalence | Age-related fibrosis, hypertension, stiffening. |
| Male Sex | Higher in HFrEF | Increased incidence of Coronary Artery Disease. |
| Female Sex | Higher in HFpEF | Links to obesity, hypertension, and stiffness. |
| Ethnicity | 1.5x higher in Black populations | Higher rates of HTN and specific genetic variants. |
Mortality Risk
The "Cancer Comparison": Advanced HF carries a 5-year mortality rate (~50%) that is worse than many common malignancies, including breast and prostate cancer. [5]
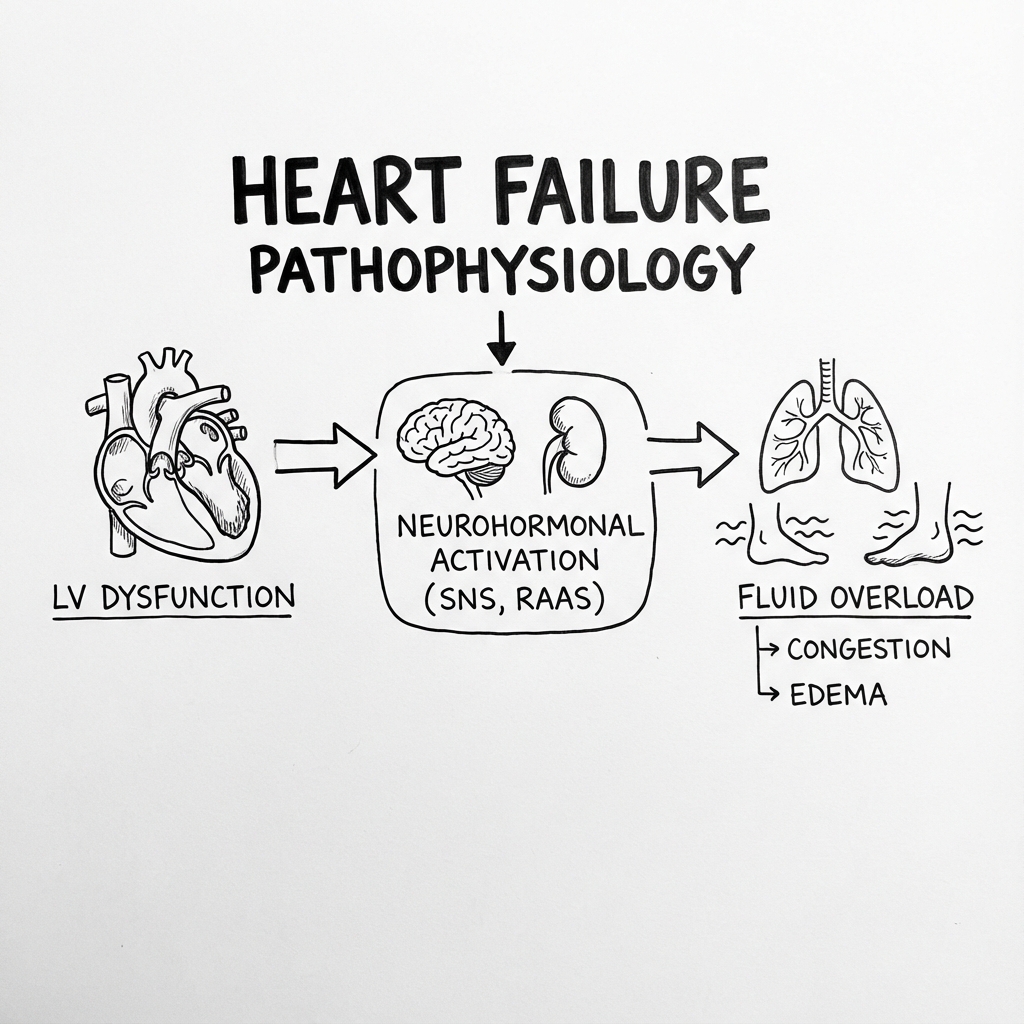
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- The Index Insult: A primary event (MI, pressure/volume overload, or toxin) causes the loss of functional myocytes or impairs their contractility.
- Neurohormonal Trigger: Falling cardiac output triggers the arterial baroreceptors to unload, activating the Sympathetic Nervous System (SNS) and the Renin-Angiotensin-Aldosterone System (RAAS).
- Adrenergic Toxicity: Chronic SNS activation leads to chronic exposure to high norepinephrine levels. This causes β1-receptor downregulation and direct cardiomyocyte toxicity (Ca2+ overload and apoptosis).
- RAAS-Mediated Fibrosis: Angiotensin II acts on AT1 receptors, stimulating TGF-β. This promotes the transition of fibroblasts to myofibroblasts, leading to collagen deposition and stiffening of the myocardium (remodelling).
- Neprilysin Counter-Regulation: The body attempts to compensate via Natriuretic Peptides (ANP, BNP). However, these are rapidly degraded by the enzyme neprilysin. The imbalance between the "destructive" RAAS/SNS and the "protective" Natriuretic system drives progression.
- SGLT2 & Metabolic Derangement: Failing hearts shift from fatty acid oxidation to inefficient glucose metabolism. The loss of metabolic flexibility and myocardial "starvation" precipitates pump failure.
- Decompensation & Vicious Cycle: Elevated filling pressures lead to pulmonary and systemic congestion, which impairs renal function (Cardiorenal Syndrome Type 1), further activating RAAS and creating a lethal positive feedback loop. [6]
4. Clinical Presentation
Symptoms
- Dyspnoea on Exertion (DOE): Most sensitive (95%).
- Orthopnoea: Need for multiple pillows (highly specific).
- Paroxysmal Nocturnal Dyspnoea (PND): Sudden waking with gasping (highly specific).
- Fatigue: Reduced cardiac output and skeletal muscle hypoperfusion.
Physical Signs
- Elevated JVP: Most specific sign of fluid overload (> 4 cm above sternal angle).
- S3 Gallop: Low-frequency sound in early diastole; indicates a dilated LV with high filling pressures.
- Displaced Apex Beat: Evidence of cardiomegaly (displaced laterally and inferiorly).
- Bibasal Crackles: Pulmonary oedema (often absent in chronic HF due to lymphatic compensation).
- Peripheral Oedema: Pitting oedema (ankles, legs, sacrum).
5. Investigations
First-Line
- NT-proBNP/BNP: The "Rule Out" test.
- Acute: NT-proBNP less than 300 pg/mL excludes HF (NPV > 98%).
- Chronic: NT-proBNP less than 125 pg/mL excludes HF.
- 12-Lead ECG: Look for LBBB (CRT candidate), prior Q-waves (IHD), or AF.
- Chest X-Ray: Cardiomegaly, Kerley B lines, pleural effusions.
The Gold Standard
- Transthoracic Echocardiogram (TTE): Essential for categorisation (HFrEF/HFpEF), valvular assessment, and measuring wall stress.
Advanced Imaging
- Cardiac MRI (CMR): The "gold standard" for tissue characterisation (ischaemic scar vs. non-ischaemic fibrosis) and viability assessment.
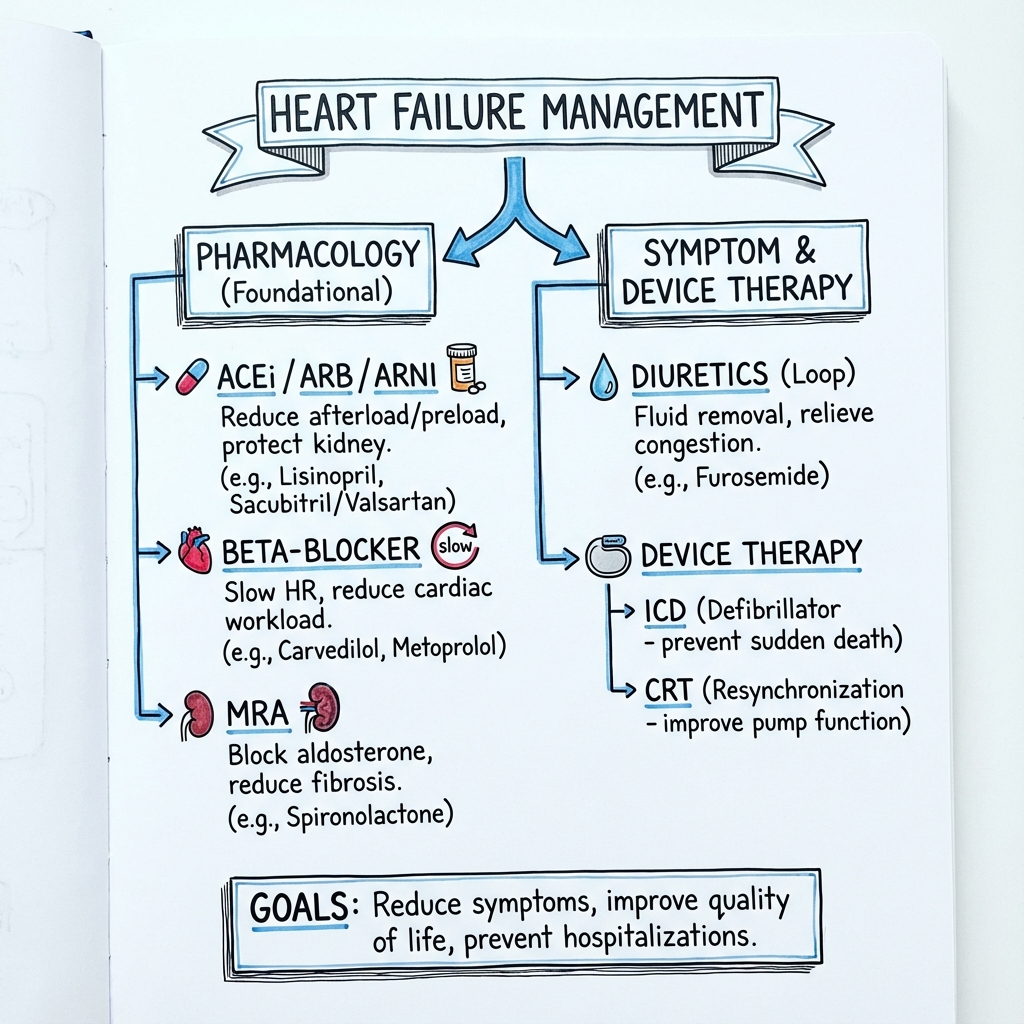
6. Management: The "Four Pillars" Revolution
Management has moved away from the sequential approach to Triple/Quadruple therapy within 4 weeks of diagnosis. [7]
Pillar 1: ARNI (Sacubitril/Valsartan)
- Mechanism: Neprilysin inhibition (increases BNP) + AT1 blockade.
- Trial: PARADIGM-HF showed 20% reduction in CV death vs. Enalapril.
- Pearl: Must have a 36-hour washout if switching from an ACE inhibitor to avoid angioedema.
Pillar 2: Beta-Blocker (Bisoprolol/Carvedilol)
- Mechanism: Blocks adrenergic toxicity and reduces heart rate (prolonging diastole).
- Trial: CIBIS-II / MERIT-HF.
- Pearl: Do NOT stop in acute decompensation unless the patient is in cardiogenic shock.
Pillar 3: MRA (Spironolactone/Eplerenone)
- Mechanism: Antagonises aldosterone-mediated fibrosis.
- Trial: RALES.
- Pearl: Gynaecomastia is common with spironolactone; switch to Eplerenone if this occurs.
Pillar 4: SGLT2 Inhibitor (Dapagliflozin/Empagliflozin)
- Mechanism: Osmotic diuresis + myocardial metabolic switch + reduced preload/afterload.
- Trial: DAPA-HF / EMPEROR-Reduced.
- Pearl: Effective even in non-diabetic patients.
7. HFpEF Management (The Preserved Challenge)
HFpEF (EF ≥50%) was once untreatable.
- First-line: SGLT2 inhibitors (EMPEROR-Preserved / DELIVER).
- Weight Loss: STEP-HFpEF trial showed Semaglutide (GLP-1) significantly improves symptoms and exercise capacity in obese HFpEF patients. [8]
8. Device Therapy (When Drugs Are Not Enough)
- ICD (Defibrillator): Primary prevention of Sudden Cardiac Death (SCD) if EF ≤35% despite 3 months of GDMT.
- CRT (Biventricular Pacing): Indicated if EF ≤35% and LBBB (QRS > 130-150ms). Resynchronises the septum and lateral wall.
- LBBP (Left Bundle Branch Pacing): Emerging "physiological" pacing technique superior to traditional CRT in some cohorts.
9. Complications
- Cardiorenal Syndrome: Reciprocal injury to kidneys.
- Cardiac Cachexia: Loss of > 5% body weight; poor prognostic marker.
- Tachycardiomyopathy: AF with rapid ventricular response causing EF drop.
- Sudden Cardiac Death: 50% of HFrEF deaths are arrhythmic.
10. Evidence: Landmark Trials
| Trial | Population | Intervention | Result (HR) | Impact |
|---|---|---|---|---|
| PARADIGM-HF | HFrEF | ARNI vs. ACEi | 0.80 | ARNI became 1st line over ACEi. |
| DAPA-HF | HFrEF | Dapa vs. Placebo | 0.74 | Added SGLT2i to the 4 pillars. |
| STRONG-HF | Acute HF | Rapid Titration | 0.66 | Mandated 4-week goal for target doses. |
| STEP-HFpEF | HFpEF + Obese | Semaglutide | Symptom + | GLP-1 as key for obese HFpEF. |
11. Single Best Answer (SBA) Questions
Question 1
A 70-year-old male with HFrEF (EF 30%) is on Ramipril 10mg and Bisoprolol 10mg. He remains symptomatic (NYHA III). BP is 115/75, K+ 4.2. What is the most appropriate medication to add next?
- A) Digoxin
- B) Ivabradine
- C) Spironolactone
- D) Furosemide
- E) Amlodipine
- Answer: C. MRAs (Spironolactone) are one of the "Four Pillars" and have a proven mortality benefit. They should be added before symptoms-only drugs like Digoxin.
Question 2
A patient is being switched from Enalapril to Sacubitril/Valsartan. How long must you wait between the last dose of Enalapril and the first dose of the new drug?
- A) 12 hours
- B) 24 hours
- C) 36 hours
- D) 48 hours
- E) No wait required
- Answer: C. A 36-hour washout period is mandatory to prevent bradykinin accumulation and the risk of life-threatening angioedema.
12. Viva Scenario: The "Cold and Wet" Patient
Examiner: "A patient with HFrEF is admitted with worsening breathlessness. On examination, they have basal crackles, but their peripheries are cold to the touch and their SBP is 85 mmHg. What is the haemodynamic profile and management?"
Candidate:
- Haemodynamic Profile: This is a "Cold and Wet" profile, indicating Cardiogenic Shock (congestion + hypoperfusion).
- Management:
- Stabilisation: High-flow O2, sit upright, escalate to CCU/ICU.
- Inotropes: Dobutamine or Milrinone to increase CO.
- Diuresis: Careful IV loop diuretics once perfusion is supported.
- Mechanical Support: Consider IABP or Impella if refractory.
- Avoid: Do NOT give beta-blockers in this acute shocked state.
13. References
- McDonagh TA, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021. [PMID: 34447992]
- Heidenreich PA, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. Circulation. 2022. [PMID: 35363499]
- Mebazaa A, et al. Safety, tolerability and efficacy of up-titration of guideline-directed medical therapies for acute heart failure (STRONG-HF). Lancet. 2022. [PMID: 36356616]
- Kosiborod MN, et al. Semaglutide in Patients with Heart Failure with Preserved Ejection Fraction and Obesity (STEP-HFpEF). N Engl J Med. 2023. [PMID: 37622681]
- McMurray JJ, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure (PARADIGM-HF). N Engl J Med. 2014. [PMID: 25176015]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for heart failure?
Seek immediate emergency care if you experience any of the following warning signs: Acute respiratory distress (pulmonary oedema), Cardiogenic shock (SBP less than 90 mmHg, cold peripheries), New-onset AF with rapid ventricular response, Acute Coronary Syndrome (ACS) as precipitant, Refractory ventricular arrhythmias.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Consequences
Complications and downstream problems to keep in mind.
- Cardiorenal Syndrome
- Cardiac Cachexia