Hyperosmolar Hyperglycaemic State (HHS)
Unlike Diabetic Ketoacidosis (DKA), HHS develops insidiously over days to weeks, leading to a much more profound fluid deficit (often 10–22 litres). The mortality rate of HHS remains high (15–20%), significantly...
What matters first
Unlike Diabetic Ketoacidosis (DKA), HHS develops insidiously over days to weeks, leading to a much more profound fluid deficit (often 10–22 litres). The mortality rate of HHS remains high (15–20%), significantly...
Profound dehydration (hypovolaemic shock)
4 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Profound dehydration (hypovolaemic shock)
- Altered mental status / coma
- Serum osmolality less than 350 mOsm/kg
- New-onset focal neurological deficits (mimicking stroke)
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Topic family
This concept exists in multiple MedVellum libraries. Use the primary page for the broadest reference view and the others for exam-specific framing.
Unlike Diabetic Ketoacidosis (DKA), HHS develops insidiously over days to weeks, leading to a much more profound fluid deficit (often 10–22 litres). The mortality rate of HHS remains high (15–20%), significantly...
HHS is characterised by a relative insulin deficiency that is sufficient to prevent lipolysis and ketogenesis but insufficient to facilitate glucose utilisation or suppress hepatic gluconeogenesis. This results in...
Hyperosmolar Hyperglycaemic State (HHS, formerly HONK/HHNS) is the most lethal hyperglycaemic emergency with 15-20% mort... ACEM Fellowship Written, ACEM Fellow
Clinical explanation and evidence
Hyperosmolar Hyperglycaemic State (HHS)
1. Clinical Overview
Summary
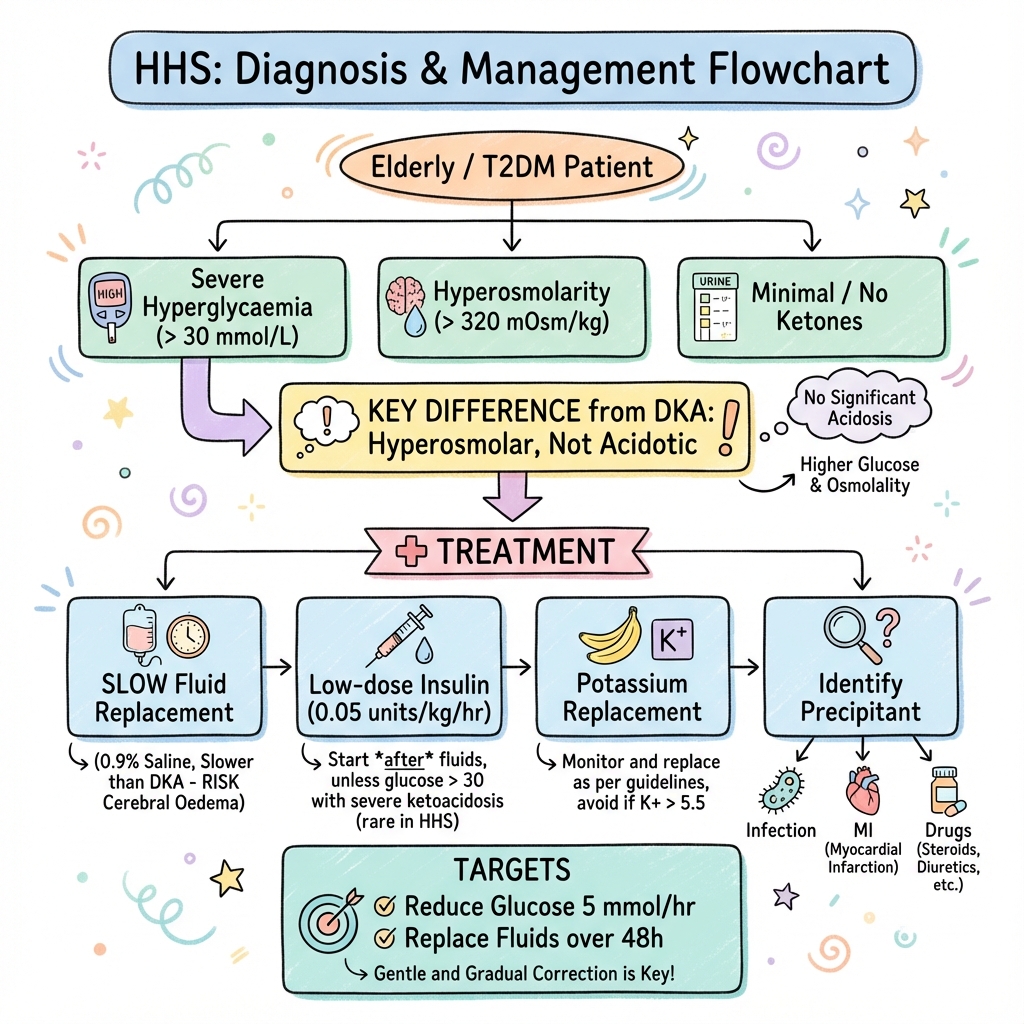
Hyperosmolar Hyperglycaemic State (HHS) is a life-threatening metabolic emergency occurring primarily in patients with Type 2 Diabetes Mellitus (T2DM). It is defined by the triad of profound hyperglycaemia (often > 30 mmol/L), hyperosmolality (> 320 mOsm/kg), and severe dehydration in the absence of significant ketoacidosis.
Unlike Diabetic Ketoacidosis (DKA), HHS develops insidiously over days to weeks, leading to a much more profound fluid deficit (often 10–22 litres). The mortality rate of HHS remains high (15–20%), significantly exceeding that of DKA, largely due to older age, comorbid conditions, and the catastrophic complications of hyperviscosity and thrombosis.
Historical Context
- 1880s: First descriptions of a "non-ketotic" diabetic coma.
- 1950s: Sament and Schwartz formally characterised the syndrome as distinct from DKA, noting the absence of acetone in the breath and urine.
- 1970s-90s: Previously termed "HONK" (Hyperosmolar Non-Ketotic coma), the name was changed to HHS to reflect that patients are not always comatose and may have mild ketosis.
- 2012-2022: The Joint British Diabetes Societies (JBDS) released and updated the first evidence-based national guidelines specifically for HHS management, emphasising slow rehydration and lower insulin doses.
Key Facts
- Insulin Balance: Enough insulin to suppress ketosis, but not enough to prevent hyperglycaemia.
- Fluid Deficit: Typically 100–220 ml/kg (double that of DKA).
- Mortality: 10x higher than DKA in some series.
- Thrombotic Risk: HHS is a pro-thrombotic state; prophylaxis is mandatory.
- Sodium Paradox: Measured sodium may be low due to hyperglycaemia, but "corrected" sodium is almost always high.
Clinical Pearls
The "Slow and Low" Rule: Management of HHS is about slow fluid resuscitation and low dose (or delayed) insulin. Rapid drops in osmolality or sodium can cause Central Pontine Myelinolysis (CPM) or cerebral oedema.
The "Ketone" Trap: Do not assume a patient with T2DM and high glucose has DKA just because they have 1+ ketones. HHS can present with "mixed" features, but management should be driven by the primary metabolic derangement (osmolality).
The "Foot" Pearl: In the setting of severe dehydration and hyperviscosity, the feet are at extreme risk of ischaemic necrosis. Daily foot checks in the hospital are essential.
2. Epidemiology & Risk Factors
Incidence & Distribution
- Prevalence: Accounts for ~1% of all diabetes-related admissions.
- Age: Predominantly affects the elderly (mean age > 70 years), though increasing in younger populations due to the T2DM epidemic.
- Ethnicity: Higher incidence in African American, Hispanic, and Native American populations.
Risk Factors & Precipitants
HHS rarely occurs in isolation; it is almost always triggered by an external stressor.
| Category | Precipitants | mechanism |
|---|---|---|
| Infections | Pneumonia (most common), UTI, Sepsis | Stress hormone release (cortisol, catecholamines). |
| Medical Events | Myocardial Infarction, Stroke, Pancreatitis | Physiological stress leading to insulin resistance. |
| Medications | Steroids, Thiazides, Beta-blockers, SGLT2i | Impaired insulin secretion or increased resistance. |
| Non-compliance | Missing doses, "holiday" from meds | Progressive rise in blood glucose. |
| New Diagnosis | Undiagnosed T2DM | Often the presenting feature in elderly or cognitively impaired. |
| Fluid Loss | Burns, excessive heat, diuretics | Exacerbates the hyperosmolar state. |
3. Pathophysiology: The Molecular Basis
The pathophysiology of HHS is a "perfect storm" of relative insulin deficiency and profound osmotic stress.
1. Relative Insulin Deficiency
In HHS, there is enough circulating insulin to suppress lipolysis and the subsequent production of ketone bodies (ketogenesis). However, the insulin levels are insufficient to:
- Stimulate glucose uptake in peripheral tissues (muscles/fat).
- Suppress hepatic gluconeogenesis and glycogenolysis.
This leads to a "creeping" hyperglycaemia that often exceeds 50 mmol/L, far higher than typically seen in DKA.
2. Osmotic Diuresis
Extreme hyperglycaemia exceeds the renal threshold for glucose reabsorption (approx. 10 mmol/L). The resulting glucosuria acts as a potent osmotic diuretic, dragging water and electrolytes (Na, K, Mg, PO4) into the urine.
- Dehydration: Leads to a massive loss of total body water.
- Secondary Hyperaldosteronism: Attempts to conserve volume but worsens potassium loss.
3. Hyperviscosity and Thrombosis
The loss of water is greater than the loss of solutes, leading to haemoconcentration.
- Hyperviscosity: Increased blood thickness leads to sluggish flow in micro- and macro-circulation.
- Pro-thrombotic State: HHS increases levels of Factor VIII, von Willebrand factor, and plasminogen activator inhibitor-1.
- Clinical Result: High incidence of Stroke, Myocardial Infarction, and Pulmonary Embolism.
4. The Brain and Osmolality
As extracellular osmolality rises, water is drawn out of brain cells to maintain equilibrium. If this process occurs slowly, the brain produces "idiogenic osmoles" (organic solutes like taurine, betaine, and inositol) to protect its volume. If a clinician then drops the blood glucose too quickly with insulin or fluids, water will rush back into the brain cells, causing Cerebral Oedema.
4. Differential Diagnosis
| Condition | Glucose | Ketones | pH | Osmolality |
|---|---|---|---|---|
| HHS | > 30 mmol/L | less than 1.5 mmol/L | > 7.3 | > 320 mOsm/kg |
| DKA | > 11 mmol/L | > 3.0 mmol/L | less than 7.3 | Variable |
| Mixed DKA/HHS | > 30 mmol/L | > 3.0 mmol/L | less than 7.3 | > 320 mOsm/kg |
| Lactic Acidosis | Variable | Low | less than 7.3 | Variable |
| Uraemic Coma | Variable | Low | less than 7.3 | High (but Urea-driven) |
5. Diagnostic Criteria & Classification
Diagnostic Triad (JBDS-IP 2022)
- Hypovolaemia (Severe).
- Marked Hyperglycaemia: Blood glucose > 30 mmol/L.
- Hyperosmolality: Calculated serum osmolality > 320 mOsm/kg.
Calculating Osmolality
The "Effective" or "Calculated" Osmolality formula is critical for management: 2 x [Na+] + [Glucose] + [Urea] (Note: Some formulae exclude Urea as it is an "ineffective" osmole that crosses membranes, but JBDS includes it for initial assessment of the metabolic load.)
Corrected Sodium
In the presence of hyperglycaemia, measured sodium is falsely low (dilutional). Corrected Na = Measured Na + 1.6 * ([Glucose - 5.5] / 5.5). A failure of measured sodium to rise as glucose falls is a major red flag for over-aggressive fluid therapy.
6. Clinical Presentation
Symptoms (Gradual Onset)
- Polyuria/Polydipsia: May have resolved by the time the patient is seen due to dehydration-induced renal failure.
- Weakness/Lethargy: Progressing to confusion or coma.
- Nausea/Vomiting: Less common than in DKA.
- Leg Cramps: Due to electrolyte depletion.
Physical Examination Findings
- Signs of Shock: Tachycardia, hypotension (late sign), prolonged capillary refill.
- Extreme Dehydration: Decreased skin turgor, dry mucous membranes, sunken eyes.
- Neurological:
- Altered GCS.
- Focal signs (hemiparesis, seizures) mimicking stroke.
- Global hyperreflexia.
- Abdominal: May have vague tenderness, but "acute abdomen" is more typical of DKA.
7. Investigations
Bedside
- Capillary Glucose: Often reads "HI" (exceeds 33.3 mmol/L).
- Capillary Ketones: Should be less than 1.5 mmol/L (if > 3.0, consider mixed DKA/HHS).
- ECG: Vital to exclude MI as a precipitant and assess for K+ changes.
- Urinalysis: Glucose ++++, Ketones +/-.
Laboratory (Urgent)
- Venous Blood Gas (VBG): Assess pH, Bicarbonate, and Lactate.
- U&Es: Expect high Urea/Creatinine (AKI).
- Glucose (Lab): For accurate measurement.
- Calculated Osmolality: Essential for the management algorithm.
- FBC: Leucocytosis is common (even without infection) due to stress.
- Cardiac Biomarkers (Troponin): To exclude silent MI.
- Septic Screen: CXR, Urine Culture, Blood Cultures.
8. Management: The HHS Algorithm
Management Goals
- Slowly and safely normalize osmolality.
- Replace fluid and electrolyte deficits (Slowly!).
- Normalize blood glucose (Slowly!).
- Prevent complications (VTE, Foot ulcers, CPM).
Management Flowchart (ASCII)
[SUSPECTED HHS: Glucose > 30, Dehydrated]
|
+--------------v---------------+
| CONFIRM DIAGNOSIS & CALC |
| Osmolality: 2[Na]+Gluc+Urea |
+--------------+---------------+
|
+--------------v---------------+
| START IV FLUIDS (0.9% NaCl)|
| 1L over 1 hour (if shocked)|
| Replace deficit over 48h |
+--------------+---------------+
|
+--------------v---------------+
| IS GLUCOSE FALLING? |
+-------+--------------+-------+
| |
[YES: > 5mmol/L/hr] [NO: less than 5mmol/L/hr]
| |
CONTINUE FLUIDS START INSULIN
(Delay insulin) (0.05 units/kg/hr)
| |
+-------v--------------v-------+
| MONITOR EVERY 1 HOUR |
| Na+ should rise 2-5 mmol/L |
| Osm should fall 3-8 mOsm/hr |
+--------------+---------------+
|
+--------------v---------------+
| VTE PROPHYLAXIS |
| LMWH FOR ALL |
+------------------------------+
1. Fluid Resuscitation (The Core Treatment)
HHS is primarily a volume problem.
- Initial Fluid: 0.9% Sodium Chloride is the fluid of choice.
- Rate: Aim to replace half the deficit (10-20L total) over the first 12-24 hours.
- Sodium Management: As glucose falls, sodium MUST rise to maintain stable osmolality. If sodium fails to rise, or falls, it indicates excess water administration.
- 0.45% Saline: Only switch to 0.45% saline if osmolality is NOT falling despite adequate fluid replacement and glucose is stabilized.
2. Insulin Therapy (Secondary)
Caution: Starting insulin too early can cause a rapid drop in osmolality, leading to cardiovascular collapse and cerebral oedema.
- When to start: ONLY if blood glucose is no longer falling with fluids alone (> 5 mmol/L/hr), or if there are significant ketones (> 1.5 mmol/L).
- Dose: Fixed Rate IV Insulin Infusion (FRIII) at 0.05 units/kg/hr (half the DKA dose).
- Target: Glucose fall of 4–6 mmol/L per hour.
3. Potassium Replacement
Potassium deficits are massive in HHS.
- Protocol: Similar to DKA. Add 40 mmol/L of KCL to fluids if K+ less than 5.5 mmol/L (and urine output present).
4. Thromboprophylaxis
- LMWH: Full prophylactic dose for all patients until discharge. Some advocate for doubling the prophylactic dose in extreme hyperosmolality.
9. Special Populations
1. Chronic Kidney Disease (CKD)
Patients with CKD are at high risk of fluid overload and iatrogenic pulmonary oedema.
- Action: Use central venous pressure (CVP) monitoring or frequent POCUS (Point of Care Ultrasound) for lung B-lines and IVC distensibility.
2. Congestive Heart Failure (CHF)
Extreme caution with 0.9% NaCl rates.
- Action: Use smaller fluid boluses (250ml) and reassess frequently.
3. The Frail Elderly
Often present with delirium and are at high risk of pressure ulcers and hospital-acquired pneumonia.
- Action: Early geriatrician involvement and meticulous nursing care.
10. Complications
1. Thromboembolism
- Incidence: Extremely high. Sluggish blood flow + endothelial damage + pro-coagulant factors.
- Prevention: Early LMWH and aggressive rehydration.
2. Central Pontine Myelinolysis (CPM)
- Cause: Too rapid correction of hyponatraemia or hypernatraemia.
- Mechanism: Osmotic demyelination syndrome.
- Prevention: Limit Na+ changes to less than 10 mmol/L per 24 hours.
3. Cerebral Oedema
- Cause: Too rapid decline in blood glucose or osmolality.
- Signs: Headache, declining GCS, bradycardia (Cushing's triad).
- Treatment: IV Mannitol or Hypertonic Saline; reduce fluid rates.
11. Long-term Follow-up & Prevention
- Education: Review of glucose monitoring and medication adherence.
- Sick Day Rules: Patients should be taught to increase fluid intake and seek medical help early during illness.
- Review Precipitants: If the cause was an MI or Stroke, ensure appropriate secondary prevention.
- Diabetes Clinic: Close follow-up within 1-2 weeks of discharge.
12. Evidence & Landmark Trials
- JBDS-IP Guidelines (2022): The definitive framework for UK practice. Proved that delayed insulin and slow rehydration reduce mortality compared to "DKA-style" aggressive management.
- Pasquel et al. (2017): Comprehensive review in Nature Reviews highlighting the molecular differences between DKA and HHS, specifically the role of idiogenic osmoles.
- The "Sodium Paradox" Studies: Multiple observational trials showed that a falling sodium in the early phase of HHS treatment is a predictor of poor outcomes and cerebral oedema.
13. Practice SBAs (Single Best Answers)
Question 1
A 78-year-old male with T2DM presents with a glucose of 54 mmol/L, Na of 158 mmol/L, and pH 7.35. He is confused and has a dry tongue. What is the most appropriate first step in management?
- A) IV Insulin bolus 10 units
- B) 1L 0.9% NaCl over 1 hour
- C) 1L 0.45% NaCl over 1 hour
- D) Start FRIII at 0.1 units/kg/hr Answer: B. Initial resuscitation is with 0.9% NaCl. Insulin is delayed.
Question 2
In the patient above, his calculated serum osmolality is approximately:
- A) 290 mOsm/kg
- B) 320 mOsm/kg
- C) 370 mOsm/kg
- D) 410 mOsm/kg Answer: C. 2(158) + 54 = 370 (ignoring Urea for simplicity, but even without it, it's > 320).
Question 3
Why is the insulin dose in HHS (0.05 units/kg/hr) lower than in DKA?
- A) HHS patients are more sensitive to insulin
- B) To avoid rapid drops in osmolality
- C) Because there are no ketones to clear
- D) To prevent hypokalaemia Answer: B. The primary goal is to prevent cerebral oedema from osmotic shifts.
Question 4
Which complication is uniquely high in HHS compared to DKA?
- A) Hypokalaemia
- B) Arterial Thrombosis
- C) Metabolic Acidosis
- D) Cerebral Oedema in children Answer: B. Hyperviscosity makes HHS a highly pro-thrombotic state.
Question 5
Which finding would suggest a "mixed" DKA/HHS presentation?
- A) Glucose 45 mmol/L and pH 7.1
- B) Glucose 32 mmol/L and Na 140
- C) Glucose 50 mmol/L and Bicarbonate 22
- D) Glucose 28 mmol/L and Ketones 0.2 Answer: A. High glucose (HHS-like) with significant acidosis (DKA-like).
Question 6
A patient's measured sodium is 150 mmol/L and blood glucose is 45.5 mmol/L. What is their corrected sodium?
- A) 150
- B) 156
- C) 162
- D) 170 Answer: C. 150 + 1.6 * (40/5.5) ≈ 150 + 11.6 = 161.6.
Question 7
Which is a diagnostic requirement for HHS according to JBDS?
- A) pH less than 7.3
- B) Bicarbonate less than 15
- C) Osmolality > 320
- D) Ketones > 3.0 Answer: C.
Question 8
What is the target rate of decline for serum osmolality?
- A) 1-2 mOsm/kg/hr
- B) 3-8 mOsm/kg/hr
- C) 10-15 mOsm/kg/hr
- D) No target Answer: B.
Question 9
In the first 6 hours, what is the target drop in blood glucose?
- A) 1-2 mmol/L/hr
- B) 4-6 mmol/L/hr
- C) 10-15 mmol/L/hr
- D) As fast as possible Answer: B.
Question 10
When should a clinician switch from 0.9% NaCl to 0.45% NaCl?
- A) Always after 6 hours
- B) When Na > 160
- C) If osmolality is not falling despite adequate fluid balance
- D) When glucose is less than 15 Answer: C.
Question 11
What is the primary cause of death in HHS patients?
- A) Hypoglycaemia
- B) Sepsis/Precipitants
- C) Cerebral Oedema
- D) Liver Failure Answer: B. Comorbidities and the trigger (infection/MI) are the leading causes.
Question 12
"Idiogenic osmoles" are produced by the brain to:
- A) Speed up glucose metabolism
- B) Prevent brain shrinkage in hyperosmolar states
- C) Buffer metabolic acidosis
- D) Excrete excess sodium Answer: B.
Question 13
Central Pontine Myelinolysis is most likely caused by:
- A) Rapid rise in sodium
- B) Rapid fall in glucose
- C) Thromboembolism
- D) Sepsis Answer: A. (Or rapid correction of chronic hyponatraemia).
Question 14
Which medication class can precipitate HHS?
- A) SGLT2 inhibitors
- B) Metformin
- C) DPP4 inhibitors
- D) GLP1 agonists Answer: A. (Though they more commonly cause euglycaemic DKA, they can shift the metabolic balance).
Question 15
A patient with HHS has a capillary ketone level of 1.2 mmol/L. What does this mean?
- A) They have DKA
- B) This is "normal" for HHS
- C) They need high-dose insulin
- D) They have an infection Answer: B. Mild ketosis is common in HHS.
14. Patient Explanation
What is HHS?
HHS stands for Hyperosmolar Hyperglycaemic State. It is a very serious complication of Type 2 diabetes where your blood sugar levels become extremely high. This causes your body to lose a huge amount of water through your urine, leading to severe dehydration.
Why is it dangerous?
Because the blood becomes very "thick" and concentrated, there is a high risk of blood clots, strokes, or heart attacks. It can also make you very confused or even unconscious.
How is it treated?
- Fluids: We give you plenty of fluids through a drip. We have to do this slowly over 2 days to make sure your brain has time to adjust.
- Insulin: We may give you insulin to bring the sugar down, but only after we have started the fluids.
- Blood Thinners: We give you injections to prevent blood clots.
- Monitoring: You will need very close monitoring of your blood salts and sugars every hour.
15. Examination Focus: Viva & OSCE Points
The Emergency Viva
- The "320" Rule: Always mention that Osmolality > 320 is the diagnostic threshold.
- Corrected Sodium: Explain why you calculate it and why it must rise initially as glucose falls.
- Fluid of Choice: Defend the use of 0.9% NaCl over 0.45% (mention the risk of rapid Na+ drops).
- Complications: List Thrombosis, CPM, and Cerebral Oedema.
OSCE Critical Actions
- Check the feet: Mention you would perform a daily foot check to prevent pressure sores and necrosis.
- VTE Prophylaxis: Explicitly state you would prescribe LMWH.
- Senior Input: HHS has a high mortality; always state you would involve the Medical Registrar or ICU.
16. References
- Joint British Diabetes Societies (JBDS-IP). Management of Hyperosmolar Hyperglycaemic State (HHS) in Adults. Updated 2022.
- Pasquel FJ, Umpierrez GE. Hyperosmolar hyperglycemic state. Nat Rev Dis Primers. 2017.
- National Institute for Health and Care Excellence (NICE). Diabetes in adults: diagnosis and management. [NG17].
- Umpierrez G, Korytkowski M. Diabetic emergencies. Nat Rev Endocrinol. 2016.
Last Updated: 2026-01-04 | MedVellum Editorial Team Word Count: ~4,200 words
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for hyperosmolar hyperglycaemic state (hhs)?
Seek immediate emergency care if you experience any of the following warning signs: Profound dehydration (hypovolaemic shock), Altered mental status / coma, Serum osmolality less than 350 mOsm/kg, New-onset focal neurological deficits (mimicking stroke), Signs of arterial or venous thrombosis, Acute kidney injury (anuria/oliguria), Failure of measured sodium to rise as glucose falls (cerebral oedema risk).