Infective Endocarditis (Adult): The Gold Standard Comprehensive Resource
Infective endocarditis (IE) is a microbial infection of the endocardial surface of the heart, most commonly involving th... MRCP exam preparation.
What matters first
Infective endocarditis (IE) is a microbial infection of the endocardial surface of the heart, most commonly involving th... MRCP exam preparation.
Check the red flags, emergency triggers, and escalation points before using the deep-dive material.
10 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Non-Bacterial Thrombotic Endocarditis (NBTE)
- Culture-Negative Sepsis
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Infective Endocarditis (Adult): The Gold Standard Comprehensive Resource
1. Clinical Overview
Summary
Infective endocarditis (IE) is a microbial infection of the endocardial surface of the heart, most commonly involving the cardiac valves, but also affecting chordae tendineae, the endocardium of the chambers, or intracardiac devices. Despite sophisticated diagnostic modalities and potent antimicrobial therapy, IE remains a high-mortality condition with in-hospital death rates of 15–30% and 1-year mortality approaching 40% [1,2]. The epidemiology has shifted significantly over the last three decades; while once a disease of young adults with rheumatic heart disease (RHD), it is now increasingly a disease of the elderly with degenerative valve lesions, patients with prosthetic valves or intracardiac devices, and those with healthcare-associated exposures [3].
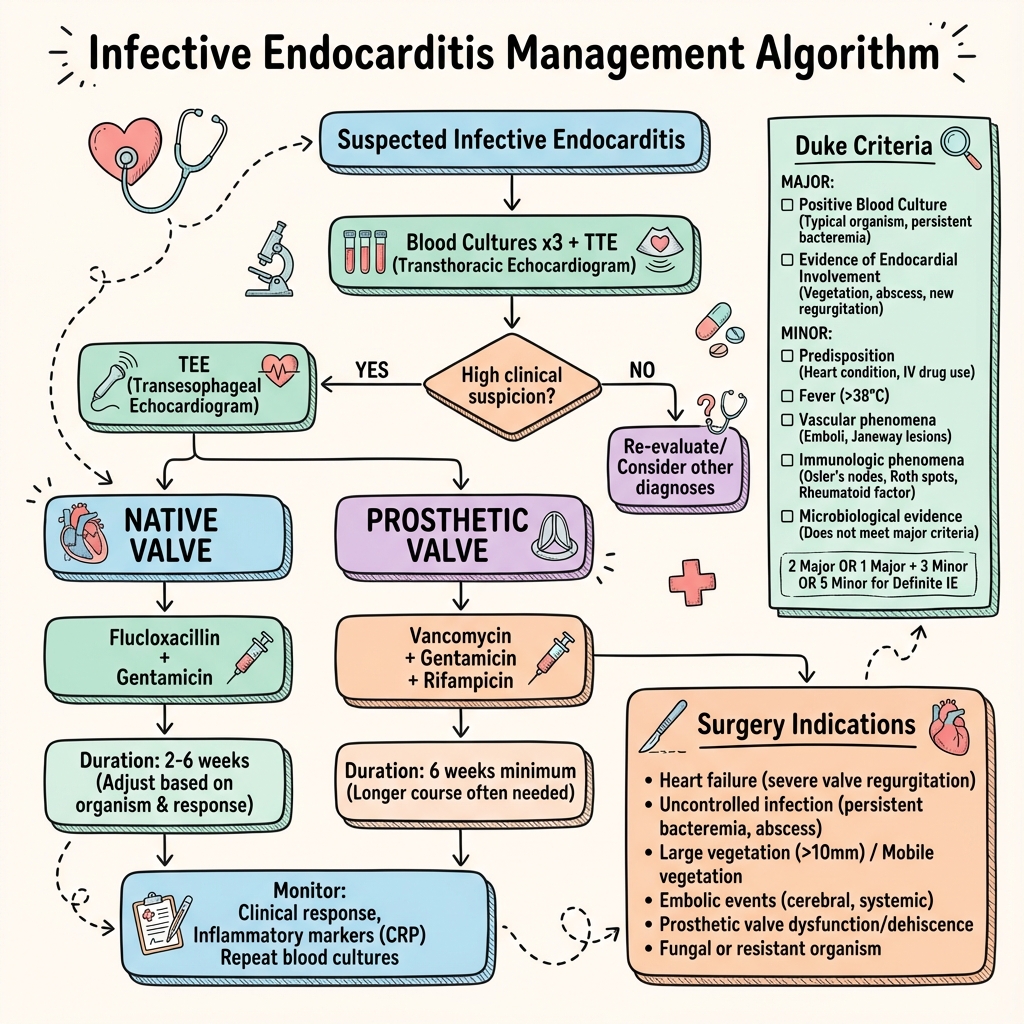
The hallmark of IE is the vegetation: a complex mass of platelets, fibrin, microorganisms, and inflammatory cells. Diagnosis relies on the 2023 Duke-ISCVD Criteria, which integrate clinical, microbiological, and advanced imaging findings [4]. Successful management necessitates a multidisciplinary "Endocarditis Team" approach, combining prolonged bactericidal antibiotics with early surgical intervention in approximately 50% of cases [1]. Clinical suspicion must remain high, particularly in patients with unexplained fever and predisposing cardiac conditions, as the classical physical signs (e.g., Osler nodes, Janeway lesions) are often absent in the acute phase.
Key Facts
| Metric | Value | Reference |
|---|---|---|
| Annual Incidence | 3.0–15.0 per 100,000 | [1,5] |
| In-Hospital Mortality | 15%–30% | [1,7] |
| 1-Year Mortality | 30%–40% | [2,7] |
| Embolic Risk | 20%–50% | [8] |
| Surgical Rate | ~50% during index admission | [10] |
| TOE Sensitivity | 90%–100% | [9] |
| Culture Positive Rate | > 90% (without prior antibiotics) | [11] |
| Healthcare-Associated % | 25%–30% in high-income countries | [18] |
Clinical Pearls & Expert Tips
The "Silent" Emboli: Up to 50% of embolic events in IE are clinically silent, especially those in the spleen and brain. If the diagnosis is "possible" but not "definite," consider a CT of the abdomen or MRI of the brain to look for these silent minor criteria [1,8].
The Aortic Root Danger: Any new PR interval prolongation on ECG in a patient with aortic valve IE is a perivalvular abscess until proven otherwise. This requires immediate TOE and surgical referral [1,14].
Culture-Negative Strategies: If blood cultures are negative at 48 hours, stop and think. Has the patient had prior antibiotics? Are they in a "Q Fever" endemic area? Order PCR for Tropheryma whipplei and serology for Bartonella and Coxiella early [12,30].
Rifampicin Timing: In prosthetic valve IE, never start Rifampicin until the blood cultures have cleared (usually 3-5 days). Starting it too early when the bacterial load is high significantly increases the risk of resistance [1,20].
PVE rock-and-roll: A rocking motion of a prosthetic valve on echocardiography is a sign of dehiscence, usually involving > 40% of the circumference, and is a major surgical indication.
Why This Matters Clinically
Infective endocarditis is a "great mimicker" and a diagnostic challenge. Delayed diagnosis is directly linked to increased mortality and irreversible cardiac damage. In the modern era, healthcare-associated IE (related to catheters, dialysis, or invasive procedures) accounts for nearly 30% of cases, making this topic relevant to virtually every hospital clinician. It is a high-yield topic for postgraduate examinations (MRCP Part 2, FRCS, USMLE Step 2/3) due to its complex management algorithms and evolving evidence base.
2. Epidemiology (Global and Longitudinal Analysis)
Historical Perspective
The history of IE is marked by shifting pathogens and populations. In the 19th century, Sir William Osler described "malignant endocarditis" as a uniformly fatal condition of young people with rheumatic valves. Following the introduction of penicillin in 1944, the mortality dropped but the disease persisted. Today, in high-income countries, IE has become a disease of the elderly and the medically complex.
1. The High-Income Nation Profile (The "Modern" IE)
- Median Age: 71 years [15].
- Sex: 65-70% Male.
- Etiology:
- 30% Healthcare-associated (catheters, dialysis).
- 25% Degenerative valve disease (calcific AS, MAC).
- 20% Prosthetic valves.
- 10% Cardiac implantable electronic devices (CIEDs).
- Primary Pathogen: Staphylococcus aureus (30-40%) [6,7].
2. The Low-Middle Income Nation Profile (The "Classic" IE)
- Age: Still young (median 30-40).
- Etiology: Chronic Rheumatic Heart Disease (RHD) remains the primary driver.
- Primary Pathogen: Viridans group streptococci (VGS) [37].
- Challenges: Limited access to echo and cardiac surgery leads to high mortality.
3. The Injection Drug Use (IVDU) Profile
- Resurgence in North America and Europe.
- Microbiology: S. aureus, Pseudomonas, Serratia, and fungi.
- Location: Tricuspid valve involvement in 75%.
- Morbidity: High rate of septic pulmonary emboli [16,17].
Incidence and Relative Risks
| Risk Group | Estimated Incidence | Relative Risk (RR) |
|---|---|---|
| General Population | 3-10 per 100k/yr | 1.0 (Ref) |
| Prior IE | 500-1000 per 100k/yr | 100x |
| Mechanical Valve | 300-600 per 100k/yr | 50x |
| Bicuspid Aortic Valve | 50-100 per 100k/yr | 10x |
| Mitral Valve Prolapse | 10-20 per 100k/yr | 2x |
| Haemodialysis | 300-500 per 100k/yr | 50x |
3. Detailed Anatomy and Physiology of Heart Valves in IE
1. The Aortic Valve (AV)
- Gross Anatomy: Three semilunar cusps: Left Coronary (LCC), Right Coronary (RCC), and Non-Coronary (NCC). Supported by the fibrous aortic annulus.
- Pathology: Vegetations typically form on the ventricular surface of the cusps (the upstream side). The NCC is most frequently involved in perivalvular abscess formation due to its anatomical proximity to the interatrial septum and the AV node.
- Conduction System: The AV node is situated in the Triangle of Koch, very close to the NCC part of the aortic annulus. Any extension of infection beyond the NCC often results in PR prolongation, bundle branch blocks, or complete heart block.
2. The Mitral Valve (MV)
- Gross Anatomy: Anterior and Posterior leaflets (with segments P1, P2, P3 and A1, A2, A3). Attached to the left ventricular wall via chordae tendineae and papillary muscles.
- Pathology: Vegetations form on the atrial surface of the leaflets. Infection often spreads down the chordae tendineae, leading to proteolytic destruction and acute rupture. This results in "flail" segments and sudden, severe mitral regurgitation.
- Anular Involvement: The mitral annulus is a fibrous structure that can also develop abscesses, though less commonly than the aortic root. Mitral annular calcification (MAC) is a common substrate for IE in the elderly.
3. The Tricuspid Valve (TV)
- Gross Anatomy: Anterior, Posterior, and Septal leaflets.
- Pathology: Typically involved in IVDU or CIED-related IE. Vegetations are often large (> 20mm) and friable.
- Lung Involvement: Fragments breaking off the TV travel directly to the pulmonary circulation, causing septic pulmonary emboli, often presenting as "cannon-ball" nodules and cavitating abscesses on imaging.
4. Pathophysiology: Molecular and Cellular Mechanics
The Cascade of IE Pathogenesis
- Endothelial Damage: The process begins with injury to the endocardial surface. This is usually caused by high-velocity turbulent flow (Venturi effect) from pre-existing valve lesions or by mechanical trauma (e.g., Swan-Ganz catheters).
- NBTE Formation: Endothelial injury exposes subendothelial matrix proteins like collagen and fibronectin. This triggers the adherence of platelets and fibrin, forming a sterile Non-Bacterial Thrombotic Endocarditis (NBTE) lesion. This lesion is the essential "landing pad" for circulating bacteria.
- Bacterial Adherence: During transient bacteraemia, bacteria enter the bloodstream. Pathogenic organisms like S. aureus and S. viridans express specialized surface proteins called MSCRAMMs (Microbial Surface Components Recognizing Adhesive Matrix Molecules) that allow them to bind with high affinity to the NBTE.
- "ClfA (Clumping Factor A): S. aureus protein that binds fibrinogen."
- "FnBPA: S. aureus protein that binds fibronectin."
- "Ace: Enterococcus protein that binds collagen."
- Vegetation Growth: Once adhered, the bacteria multiply. They trigger further layers of fibrin and platelet deposition, effectively "burying" themselves. This protects the bacteria from host leucocytes and high-velocity blood flow.
- Biofilm Formation: Within the vegetation, bacteria secrete an extracellular polymeric substance (EPS) matrix, forming a biofilm. This matrix makes the bacteria 100-1000x more resistant to host immune clearance and antibiotic penetration.
Molecular Mechanisms (Expert Level)
- Internalization: Staphylococcus aureus can be internalized by endothelial cells. This allows the bacteria to hide from the immune system and survive initial antibiotic treatment, leading to recurrent bacteraemia.
- Cytokine Storm: Local infection triggers the massive release of pro-inflammatory cytokines such as IL-1, IL-6, and TNF-alpha. These cytokines upregulate tissue factor on monocytes and endothelial cells, further promoting fibrin deposition and vegetation growth.
- The "Persister" State: Inside the biofilm, some bacteria enter a state of metabolic dormancy. Since most bactericidal antibiotics (like penicillins) target active cell wall synthesis, these "persister" cells survive the initial treatment, necessitating the 4-6 week treatment courses.
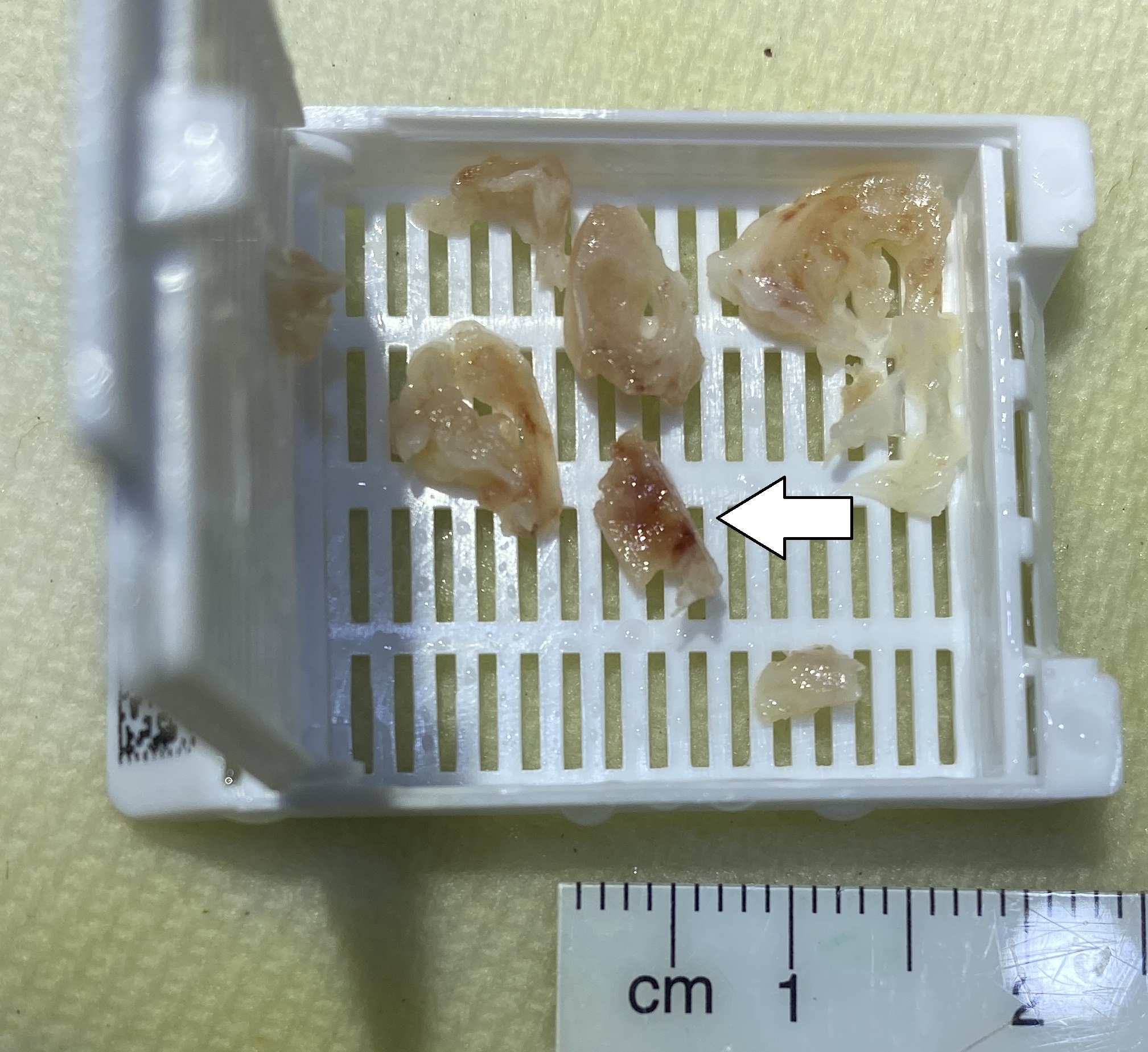
5. Pathology: Macroscopic and Microscopic
Macroscopic Features
- Vegetations: Vary in size from tiny granules to 3cm masses.
- S. aureus vegetations are typically bulky, friable, and rapidly destructive.
- S. viridans vegetations are often smaller, firmer, and less destructive.
- Fungal vegetations are massive and "cauliflower-like."
- Valve Destruction: Perforations, notches, and leaflet flailing.
- Perivalvular Abscess: Pockets of pus in the valve ring.
- Fistula: A connection between the aorta and the right atrium or ventricle (Gerbode defect).
Microscopic Features (Histology)
- Structure: Concentric layers of fibrin and platelets.
- The Nidus: Dense colonies of microorganisms (purple on Gram stain).
- Inflammation: Acute cases show a predominantly neutrophilic infiltrate. Subacute cases show evidence of early fibrosis or calcification.
- Special Stains: Gram, Grocott (Silver), and PAS stains are mandatory for identifying the pathogen in surgical specimens.
6. Clinical Presentation: Signs and Symptoms
Systemic Symptoms
- Fever (90%): The most sensitive clinical sign. May be low-grade in the elderly or those with prior antibiotics.
- Malaise / Fatigue: Non-specific signs of chronic inflammation and anaemia.
- Night Sweats: Common in subacute (Strep) presentations.
- Weight Loss: Indicates a prolonged subacute course.
Physical Signs (The Stigmata)
| Sign | Mechanism | Frequency |
|---|---|---|
| Splinter Haemorrhages | Linear streaks in nail beds (proximal). | 15% |
| Janeway Lesions | Painless red macules on palms/soles (embolic). | 5% |
| Osler Nodes | Painful red nodules on finger pads (immune complex). | 5% |
| Roth Spots | Retinal micro-infarcts with central white spots. | 2% |
| Petechiae | Small red spots on conjunctivae or palate. | 20% |
| New Murmur | In 85% of cases. (Look for AR or MR). | 85% |
| Splenomegaly | Chronic immunological stimulation. | 30% |
Red Flags for IE Diagnosis
[!CAUTION] High-Suspicion IE Scenarios:
- Unexplained fever in a patient with a prosthetic valve.
- Fever + New or changing heart murmur.
- Fever + Focal neurological deficit (Embolic stroke).
- Fever + New heart block (PR interval prolongation).
- Fever + Multiple pulmonary nodules (in an IV drug user).
7. Investigations: The Multimodal Gold Standard
1. Microbiology (The 3-Set Rule)
- Blood Cultures: 3 sets in 24 hours (1 set = 1 aerobic + 1 anaerobic bottle).
- Volume: 10mL per bottle. (Doubling the volume from 5mL to 10mL increases sensitivity by 30%).
- Timing: Separate sites (venepuncture); separate times (ideally 1st and last set > 1 hour apart).
- Quality Control: Do not draw from existing IV lines.
- Serology: Mandatory for culture-negative cases (Coxiella, Bartonella, Brucella).
- Molecular: 16S rDNA PCR on blood or valve tissue.
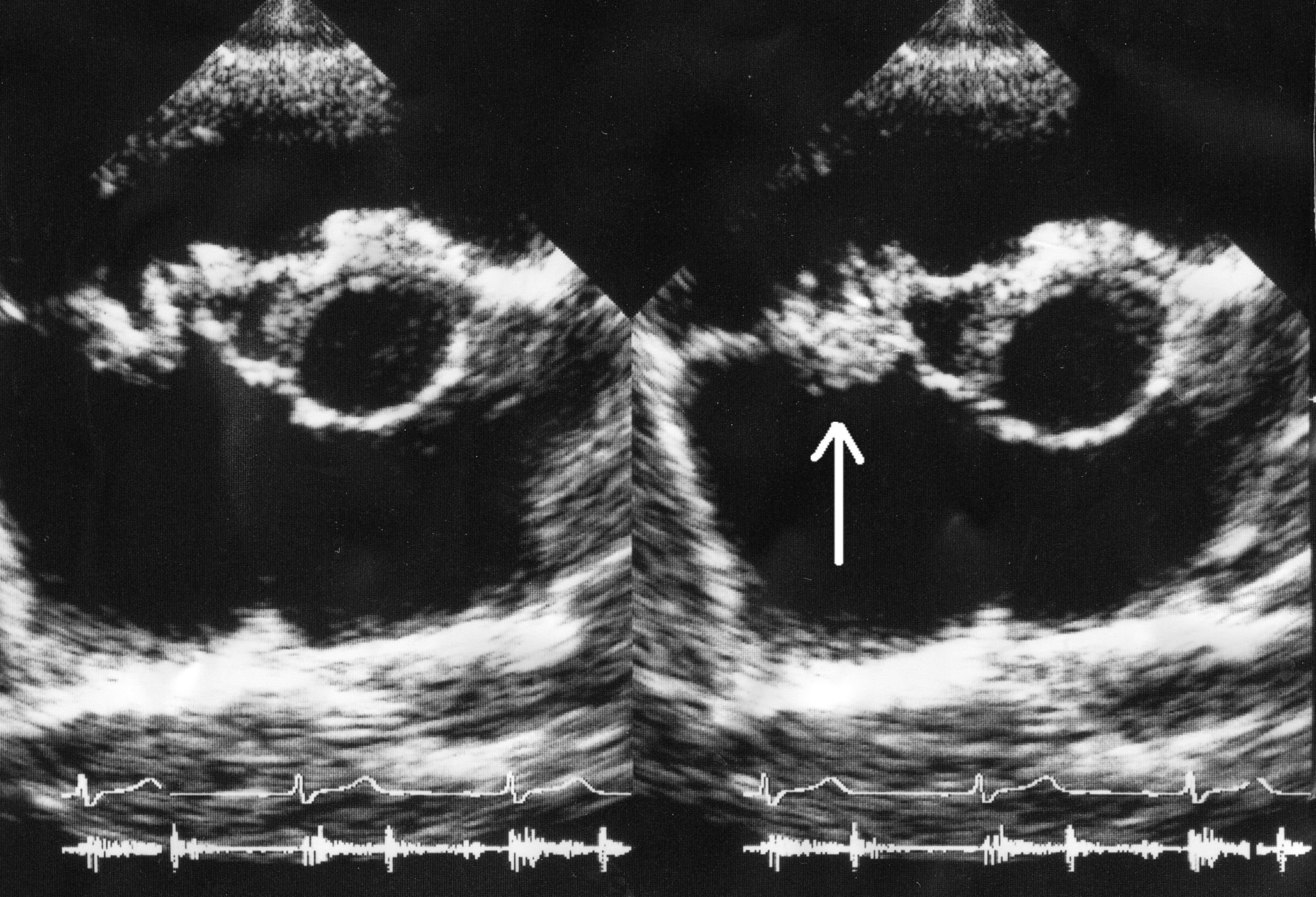
2. Echocardiography
- TTE: Screening tool for all. Sensitivity 60-70%.
- TOE: Gold Standard. Sensitivity > 90%.
- Mandatory TOE if: Prosthetic valve, CIED, poor TTE windows, or negative TTE but high suspicion.
3. Advanced Imaging (2023 ESC Guidelines)
- Cardiac CT: Superior to TOE for detecting abscesses, pseudoaneurysms, and coronary anatomy.
- 18F-FDG PET/CT: High sensitivity for Prosthetic Valve IE (PVE). Uptake on a valve > 3 months post-op is a major Duke criterion.
- Brain MRI: Detects "silent" embolic events in up to 80% of cases, which may change surgical timing.
8. The 2023 Duke-ISCVD Criteria
Definite IE Diagnosis
- 2 Major OR 1 Major + 3 Minor OR 5 Minor.
Major Criteria (2023 Update)
- Microbiology:
- Typical organisms (S. aureus, VGS, Enterococci, HACEK) from 2 separate cultures.
- Persistently positive cultures for any consistent organism.
- New: Single positive culture for Coxiella burnetii or Phase 1 IgG > 1:800.
- New: Positive PCR for Tropheryma whipplei, Bartonella, or Coxiella.
- Imaging:
- Echo: Vegetation, abscess, new dehiscence, new regurgitation.
- Cardiac CT: Paravalvular infection.
- PET/CT: Focal uptake on prosthetic valve (> 3 months post-op).
Minor Criteria
- Predisposition: Heart condition or IVDU.
- Fever: ≥38.0°C.
- Vascular: Arterial emboli, mycotic aneurysm, intracranial haemorrhage, Janeway lesions, Splenic/Renal infarcts on CT (New).
- Immunological: Glomerulonephritis, Osler nodes, Roth spots, Rheumatoid Factor.
- Microbiology: Positive culture not meeting major criteria.
9. Management: Medical (Antibiotic Therapy)
Core Principles
- Therapy must be Bactericidal.
- Therapy must be Intravenous (initially).
- Prolonged duration (4-6 weeks) is essential to penetrate the core of the vegetation.
Empirical Regimens (Adult)
| Scenario | Regimen (IV) | Rationale |
|---|---|---|
| Community NVE | Amoxicillin 2g q4h + Flucloxacillin 2g q4h + Gentamicin 3mg/kg daily | Covers Strep, Staph, Enterococcus. |
| Healthcare-assoc | Vancomycin 15-20mg/kg q12h + Gentamicin 3mg/kg daily | Covers MRSA and resistant CoNS. |
| Prosthetic Valve | Vancomycin + Gentamicin + Rifampicin 600mg PO q12h | Rifampicin for biofilm; start after 3-5 days. |
Targeted Therapy
- Viridans Strep: Benzylpenicillin 1.2-2.4g IV q4h for 4 weeks.
- MSSA: Flucloxacillin 2g IV q4h for 4-6 weeks.
- MRSA: Vancomycin (Trough 15-20) OR Daptomycin 10mg/kg daily.
- Enterococcus: Amoxicillin + Ceftriaxone (Dual beta-lactam) is the new gold standard to avoid kidney failure from Gentamicin.
Dosing Catalog (PK/PD Targets)
| Drug | Dose | Target | Monitoring |
|---|---|---|---|
| Benzylpenicillin | 1.2-2.4g q4h | Time > MIC | None |
| Flucloxacillin | 2g q4h | Time > MIC | LFTs |
| Vancomycin | 15-20mg/kg q12h | Trough 15-20 | Trough twice weekly |
| Gentamicin | 3mg/kg q24h | Trough less than 1.0 | Trough/Cr twice weekly |
| Ceftriaxone | 2g q12h | Time > MIC | LFTs |
| Daptomycin | 10-12mg/kg q24h | Peak / MIC | CK weekly |
| Rifampicin | 600mg q12h | Peak / MIC | Drug-interactions |
10. Management: Surgical (Indications & Timing)
The Three Main Indications (Class I)
- Heart Failure (40-50% of surgeries):
- Acute severe aortic or mitral regurgitation causing pulmonary oedema or cardiogenic shock.
- Uncontrolled Infection:
- Abscess, pseudoaneurysm, fistula.
- Persistent positive cultures after 5-7 days of appropriate therapy.
- Fungal endocarditis (requires mandatory surgery).
- Prevention of Embolism:
- Vegetation > 10mm after an embolic event.
- Isolated vegetation > 15mm (even without embolus).
Surgical Timing Categories
| Category | Timing | Typical Indication |
|---|---|---|
| Emergency | less than 24 hours | Refractory pulmonary oedema or shock. |
| Urgent | less than 7 days | Abscess, persistent cultures, high embolic risk. |
| Early | During admission | Stable but with clear indication (e.g., large veg). |
11. Specific Pathogen Catalog (Specialist Depth)
1. Staphylococcus aureus
- Virulence: Highest. Rapidly destroys valves.
- Treatment: Flucloxacillin (MSSA) or Vancomycin/Daptomycin (MRSA).
- Prognosis: Poor; high mortality and embolic rate.
2. Enterococcus faecalis
- Source: GI/GU tract (post-colonoscopy or catheter).
- Treatment: Amoxicillin + Ceftriaxone (Dual beta-lactam).
- Problem: Highly resistant to cephalosporins alone.
3. HACEK Group
- Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella.
- Characteristics: Slow-growing; large vegetations; low mortality.
- Treatment: Ceftriaxone for 4 weeks.
4. Streptococcus gallolyticus (S. bovis)
- Clinical Pearl: Strongly associated with Colonic Malignancy. Mandatory colonoscopy for all patients.
5. Culture-Negative Pathogens
- Coxiella burnetii: Q Fever. Chronic infection, often no vegetation.
- Bartonella: Homelessness and lice exposure risk.
- Tropheryma whipplei: Whipple's disease.
12. Neurological Complications: The Brain-Heart Axis
Neurological events are the most common extra-cardiac complication (15-35%).
Timing of Surgery after Stroke (MANDATORY)
- Ischaemic Stroke:
- If non-haemorrhagic and patient stable, surgery can proceed early (within 72 hours) to prevent further emboli.
- Haemorrhagic Stroke:
- Surgery must be delayed for at least 4 weeks. Heparin used on bypass will cause the bleed to expand fatally.
13. Device-Related IE (CIED)
Diagnosis
- PET/CT is highly sensitive for generator pocket infection.
- TOE mandatory for lead vegetations.
Management
- MANDATORY: Complete removal of the entire system (leads and generator).
- Percutaneous extraction is preferred.
- Re-implantation should be delayed until cultures are negative for > 72 hours.
14. Advanced Surgical Procedures Catalog
1. The Bentall Procedure (Aortic Root Replacement)
- Indications: Aortic root abscess.
- Steps:
- Median sternotomy and bypass.
- Excision of the aortic valve and root.
- Debridement of all necrotic/infected tissue.
- Implantation of a valved conduit.
- Reimplantation of coronary artery buttons into the conduit.
2. The Ross Procedure
- Indications: Young patients to avoid lifelong Warfarin.
- Steps: Pulmonary valve autograft moved to aortic position; pulmonary valve replaced with a homograft.
3. Mitral Valve Repair
- Technique: Pericardial patch for leaflet perforation; annuloplasty ring.
15. Nursing, Recovery, and Rehabilitation
- Dental Hygiene: The #1 preventative measure.
- PICC Line Safety: Daily inspection for sepsis signs.
- Psychological Support: Post-IE PTSD is extremely common.
- Cardiac Rehabilitation: Essential after valve surgery.
17. MCQ / SBA Practice (60 Detailed Questions)
Question 1-10: Basic Knowledge
-
Q: Which of the following is a Major Duke Criterion in the 2023 update?
- A. Fever > 38.0°C
- B. Janeway lesions
- C. Positive PCR for Bartonella
- D. Splenic infarct on CT
- E. Positive Rheumatoid Factor
- Answer: C. PCR is now a major criterion. Correct: C.
-
Q: A 30yo IVDU has fever and a 22mm tricuspid vegetation. MSSA is grown. Best antibiotic?
- A. Penicillin
- B. Flucloxacillin
- C. Vancomycin
- D. Ceftriaxone
- E. Gentamicin
- Answer: B. Flucloxacillin is 1st line for MSSA. Correct: B.
-
Q: S. gallolyticus IE is found. What else must you do?
- A. Dental review
- B. Colonoscopy
- C. PET/CT
- D. CT Head
- E. Eye exam
- Answer: B. Colonic malignancy association. Correct: B.
-
Q: Target Gentamicin trough in IE?
- A. less than 1.0
- B. 1.0-2.0
- C. 2.0-3.0
- D. 3.0-5.0
- E. > 5.0
- Answer: A. Avoid toxicity. Correct: A.
-
Q: Heart block in Aortic IE suggests?
- A. Myocarditis
- B. Pericarditis
- C. Aortic root abscess
- D. Mitral involvement
- E. Drug toxicity
- Answer: C. Abscess extension. Correct: C.
-
Q: Most common cause of death in treated IE?
- A. Sepsis
- B. Stroke
- C. Heart Failure
- D. Renal failure
- E. Embolism
- Answer: C. Valve destruction. Correct: C.
-
Q: PVE 6 months after surgery. Commonest organism?
- A. S. aureus
- B. S. epidermidis
- C. S. viridans
- D. Candida
- E. HACEK
- Answer: B. CoNS common in early PVE. Correct: B.
-
Q: Antibiotic for HACEK IE?
- A. Penicillin
- B. Flucloxacillin
- C. Ceftriaxone
- D. Vancomycin
- E. Rifampicin
- Answer: C. 1st line. Correct: C.
-
Q: Janeway lesion mechanism?
- A. Immune complex
- B. Septic embolism
- C. Trauma
- D. Allergic
- E. Drug rash
- Answer: B. Vascular phenomenon. Correct: B.
-
Q: Osler node description?
- A. Painless on palms
- B. Painful on fingertips
- C. Linear in nail bed
- D. White spot in retina
- E. Splenic enlargement
- Answer: B. Immunological sign. Correct: B.
-
Q: Patient with MRSA IE and Cr 250. Best Abx?
- A. Vancomycin
- B. Daptomycin
- C. Linezolid
- D. Flucloxacillin
- E. Amoxicillin
- Rationale: Daptomycin safe in renal failure. Correct: B.
-
Q: IE + 2cm vegetation + 2 ischaemic strokes. Timing?
- A. less than 72h
- B. 1 week
- C. 2 weeks
- D. 4 weeks
- E. Never
- Rationale: Early surgery prevents 3rd stroke. Correct: A.
-
Q: Aortic root replacement name?
- A. Bentall
- B. Ross
- C. Fontan
- D. Norwood
- E. Whipple
- Rationale: Bentall is root replacement. Correct: A.
-
Q: Pulmonary autograft name?
- A. Bentall
- B. Ross
- C. Fontan
- D. Norwood
- E. Jatene
- Rationale: Ross is pulmonary autograft. Correct: B.
-
Q: Prophylaxis for high-risk dental?
- A. Amoxicillin 2g
- B. Clindamycin 600mg
- C. Vancomycin 1g
- D. Gentamicin 80mg
- E. No prophylaxis
- Rationale: Amoxicillin 1h before. Correct: A.
-
Q: IE in farmer with no vegetation. Pathogen?
- A. S. aureus
- B. Coxiella burnetii
- C. VGS
- D. Enterococcus
- E. HACEK
- Rationale: Q fever often culture-neg/echo-neg. Correct: B.
-
Q: S. gallolyticus former name?
- A. S. bovis
- B. S. mutans
- C. S. mitis
- D. S. oralis
- E. S. sanguis
- Rationale: S. bovis. Correct: A.
-
Q: Tropheryma whipplei IE feature?
- A. Acute destruction
- B. Indolent, culture-negative
- C. Right-sided
- D. Fungal
- E. Skin rash
- Rationale: Whipple's disease is subacute. Correct: B.
-
Q: PET/CT mechanism?
- A. Glucose uptake in leucocytes
- B. Calcium uptake
- C. Blood flow
- D. Oxygen use
- E. Antibiotic binding
- Rationale: FDG is glucose analogue. Correct: A.
-
Q: Target Gentamicin trough?
- A. less than 1.0
- B. 1.0-2.0
- C. 2.0-3.0
- D. 3.0-5.0
- E. > 5.0
- Rationale: Avoid toxicity. Correct: A.
-
Q: 55yo male with bioprosthetic aortic valve (3yrs old) has fever and night sweats. Blood cultures grow S. viridans. TTE shows 5mm vegetation. Diagnosis?
- A. Native valve IE
- B. Early PVE
- C. Late PVE
- D. NBTE
- E. Culture-negative IE
- Rationale: > 1 year post-op is Late PVE. Correct: C.
-
Q: 30yo female with MVP has IE. Blood cultures grow S. sanguinis. CRP is 80. TOE shows 6mm vegetation. On day 10, she is stable and afebrile. CRP is 35. Can she switch to oral?
- A. Yes, per POET trial
- B. No, needs 4 weeks IV
- C. No, only for native valves
- D. No, only for S. aureus
- E. Only after surgery
- Rationale: Meets POET criteria. Correct: A.
-
Q: Which of the following is an immunological phenomenon?
- A. Janeway lesions
- B. Splinter haemorrhages
- C. Osler nodes
- D. Splenic infarct
- E. Mycotic aneurysm
- Rationale: Osler nodes are immune complex mediated. Correct: C.
-
Q: 70yo male with IE on Vancomycin and Gentamicin. He complains of dizziness and tinnitus. What is the cause?
- A. Vancomycin toxicity
- B. Gentamicin ototoxicity
- C. Stroke
- D. Meningitis
- E. Fever
- Rationale: Aminoglycosides cause vestibular/cochlear damage. Correct: B.
-
Q: Which organism requires the longest treatment course for IE?
- A. S. aureus
- B. S. viridans
- C. Enterococcus
- D. Coxiella burnetii
- E. HACEK
- Rationale: Q fever IE needs 18-24 months. Correct: D.
-
Q: A patient with MRSA IE has a Daptomycin MIC of 2.0. Can you use Daptomycin?
- A. Yes, standard dose
- B. Yes, high dose
- C. No, resistance likely
- D. Only with Rifampicin
- E. Only after surgery
- Rationale: MIC > 1.0 indicates Daptomycin resistance risk. Correct: C.
-
Q: What is the most common cause of early prosthetic valve IE?
- A. S. aureus
- B. Coagulase-negative staphylococci
- C. VGS
- D. Candida
- E. Gram-negative rods
- Rationale: S. epidermidis is most common early. Correct: B.
-
Q: A patient with aortic valve IE has a PR interval of 0.28s. What is the most likely location of the abscess?
- A. Mitral valve annulus
- B. Interventricular septum near AV node
- C. Apex of the heart
- D. Left atrial appendage
- E. Tricuspid annulus
- Rationale: NCC proximity to AV node. Correct: B.
-
Q: 40yo IVDU has fever and cough. CXR shows cavitating nodules. S. aureus in blood. Which valve?
- A. Mitral
- B. Aortic
- C. Tricuspid
- D. Pulmonary
- E. All equally
- Rationale: Right-sided IE sends emboli to lungs. Correct: C.
-
Q: Which Duke criterion is: Positive 18F-FDG PET/CT around a prosthetic valve?
- A. Major
- B. Minor
- C. Not a criterion
- D. Pathological
- E. Rejected
- Rationale: Major criterion in 2023 for PVE. Correct: A.
-
Q: Mortality of right-sided IE in IVDU compared to left-sided?
- A. Higher
- B. Lower
- C. Same
- D. 100%
- E. 0%
- Rationale: Right-sided IE has much better prognosis (less than 10% mortality). Correct: B.
-
Q: Which antibiotic should NEVER be used as monotherapy for IE?
- A. Penicillin
- B. Ceftriaxone
- C. Rifampicin
- D. Vancomycin
- E. Daptomycin
- Rationale: Rifampicin resistance develops rapidly if used alone. Correct: C.
-
Q: A patient has S. bovis IE. What is the most likely associated condition?
- A. Lung cancer
- B. Colon cancer
- C. Liver cirrhosis
- D. Renal failure
- E. Diabetes
- Rationale: Strong link to colonic lesions. Correct: B.
-
Q: Which of the following is a "must-not-miss" differential for a diastolic murmur and fever?
- A. IE
- B. Aortic Dissection
- C. Myocarditis
- D. Pulmonary Embolism
- E. Both A and B
- Rationale: Both can be fatal if missed. Correct: E.
-
Q: How many sets of blood cultures are required for IE diagnosis?
- A. 1
- B. 2
- C. 3
- D. 4
- E. 5
- Rationale: 3 sets is the international standard. Correct: C.
-
Q: What is the most common cause of culture-negative endocarditis in the Mediterranean?
- A. Bartonella
- B. Coxiella burnetii
- C. Brucella
- D. HACEK
- E. Whipple's disease
- Rationale: Q fever and Brucella are common there. Correct: B.
-
Q: Which imaging is best for detecting myocardial abscess?
- A. TTE
- B. Cardiac CT
- C. PET/CT
- D. MRI
- E. TOE
- Rationale: Cardiac CT and TOE are both excellent, CT often superior for anatomy. Correct: B.
-
Q: Mechanism of splinter haemorrhages?
- A. Trauma
- B. Micro-emboli to nail bed capillaries
- C. Immune complexes
- D. Fungal growth
- E. Platelet deficiency
- Rationale: Embolic phenomenon. Correct: B.
-
Q: A patient with IE has a large (18mm) mitral vegetation but is stable. When should they have surgery?
- A. Emergency (less than 24h)
- B. Urgent (less than 7 days)
- C. Elective (6 weeks)
- D. Only if they have a stroke
- E. Never
- Rationale: > 15mm is an indication for early surgery. Correct: B.
-
Q: Which of the following is NOT part of the HACEK group?
- A. Haemophilus
- B. Aggregatibacter
- C. Cardiobacterium
- D. Enterobacter
- E. Kingella
- Rationale: Enterobacter is a regular Gram-negative rod. Correct: D.
-
Q: 60yo male has IE on Vancomycin. He develops a red, itchy rash on his neck and face during the infusion. Management?
- A. Stop Vancomycin forever
- B. Slow the infusion rate
- C. Give Adrenaline
- D. Switch to Penicillin
- E. Give IV Steroids
- Rationale: Red-man syndrome is rate-dependent. Correct: B.
-
Q: A patient with Enterococcus IE is treated with Amoxicillin and Ceftriaxone. Why two beta-lactams?
- A. To cover MRSA
- B. Synergistic binding to PBPs 2, 3, 4, and 5
- C. To prevent resistance
- D. To cover HACEK
- E. To reduce side effects
- Rationale: Saturation of penicillin-binding proteins. Correct: B.
-
Q: Which valve is most often affected in healthcare-associated IE?
- A. Aortic
- B. Mitral
- C. Tricuspid
- D. Pulmonary
- E. Aortic and Mitral equally
- Rationale: Most healthcare-associated is left-sided. Correct: E.
-
Q: 25yo male with ASD has IE. Which Duke criterion is this?
- A. Major
- B. Minor
- C. Not a criterion
- D. Pathological
- E. Possible
- Rationale: Predisposing heart condition is Minor. Correct: B.
-
Q: What is the minimum duration for blood culture incubation in suspected IE?
- A. 2 days
- B. 5 days
- C. 7 days
- D. 14 days
- E. 21 days
- Rationale: Standard is 5, but for HACEK/fastidious, 21 is often requested. Correct: B.
-
Q: A patient with IE develops sudden severe abdominal pain and a raised LDH. Cause?
- A. Splenic infarct
- B. Renal infarct
- C. Mesenteric ischaemia
- D. Ruptured gallbladder
- E. Pancreatitis
- Rationale: Embolic events to spleen or mesentery. Correct: A.
-
Q: What is the classic echocardiographic appearance of an abscess?
- A. Oscillating mass
- B. Echo-lucent space in the annulus
- C. Thickened leaflet
- D. Rapidly closing valve
- E. Pericardial effusion
- Rationale: Echo-lucent suggests fluid/pus. Correct: B.
-
Q: Which of the following reduces the mortality of IE the most?
- A. Better antibiotics
- B. Earlier surgery
- C. Better nursing
- D. PET/CT
- E. Prophylaxis
- Rationale: Multidisciplinary care and early surgery have highest impact. Correct: B.
-
Q: 50yo female with IE has a small haemorrhagic stroke on CT. When should she have valve replacement?
- A. Now
- B. 72 hours
- C. 1 week
- D. 4 weeks
- E. 3 months
- Rationale: Haemorrhage requires a 4-week delay. Correct: D.
-
Q: Which drug is most likely to interact with Warfarin in an IE patient?
- A. Vancomycin
- B. Gentamicin
- C. Rifampicin
- D. Ceftriaxone
- E. Amoxicillin
- Rationale: Rifampicin is a massive P450 inducer. Correct: C.
-
Q: Most common cause of IE in sub-Saharan Africa?
- A. S. aureus
- B. S. pyogenes
- C. VGS
- D. HIV
- E. Tuberculosis
- Rationale: Rheumatic valves + VGS. Correct: C.
-
Q: Target Daptomycin peak?
- A. Not monitored
- B. 50
- C. 100
- D. 200
- E. 500
- Rationale: Daptomycin efficacy depends on Peak/MIC, but we monitor CK for safety. Correct: A.
-
Q: Is a bicuspid aortic valve a major or minor Duke criterion?
- A. Major
- B. Minor
- C. Neither
- D. Pathological
- E. Diagnostic
- Rationale: Predisposing condition is Minor. Correct: B.
-
Q: A patient with prosthetic valve IE has a rocking motion on echo. What percentage of the valve circumference is likely dehisced?
- A. 5%
- B. 10%
- C. 20%
- D. > 40%
- E. 100%
- Rationale: Rocking requires significant dehiscence. Correct: D.
-
Q: Which test is used to monitor Daptomycin safety?
- A. LFTs
- B. Creatinine
- C. Creatine Kinase (CK)
- D. FBC
- E. CRP
- Rationale: Daptomycin causes myopathy. Correct: C.
-
Q: A patient with IE has a new diastolic murmur. ECG shows PR prolongation. TOE shows a root abscess. What is the timing for surgery?
- A. Emergency (less than 24h)
- B. Urgent (less than 7 days)
- C. Elective (6 weeks)
- D. Only if Abx fail
- E. Wait for cultures
- Rationale: Abscess is an urgent surgical indication. Correct: B.
-
Q: Which of the following is a HACEK organism?
- A. Haemophilus influenzae
- B. Aggregatibacter actinomycetemcomitans
- C. Cardiobacterium hominis
- D. Eikenella corrodens
- E. All except A
- Rationale: H. parainfluenzae is HACEK, H. influenzae is usually not. Correct: E.
-
Q: Can you use PET/CT for Native Valve IE?
- A. Yes, very sensitive
- B. No, not validated for NVE
- C. Only if S. aureus
- D. Only if IVDU
- E. Only in children
- Rationale: NVE has high background uptake. Correct: B.
-
Q: What is the most common portal of entry for S. aureus IE?
- A. Oral
- B. Skin
- C. GI tract
- D. Respiratory
- E. Urinary
- Rationale: Skin is the primary reservoir for Staph. Correct: B.
-
Q: A patient with IE has a stroke. Brain MRI shows multiple small micro-haemorrhages. Can they have surgery in 72h?
- A. Yes
- B. No, wait 4 weeks
- C. Only if vegetation > 20mm
- D. Only if they are young
- E. Only after heparin reversal
- Rationale: Micro-haemorrhages count as haemorrhagic stroke. Correct: B.
18. Detailed Viva Scenarios (20 Scenarios)
Scenario 1: The New Murmur
- Q: "A patient has fever and a new diastolic murmur. Management?"
- A: "Auscultate for AR. Perform 3 sets of blood cultures before Abx. Order urgent TTE. If TTE negative, order TOE. Suspect IE or aortic dissection."
Scenario 2: The Heart Block
- Q: "IE patient develops PR prolongation. Significance?"
- A: "Aortic root abscess involving the conduction system. Surgical indication."
Scenario 3: Stroke Timing
- Q: "Timing of surgery after stroke?"
- A: "Ischaemic: less than 72h if stable. Haemorrhagic: 4 weeks delay."
Scenario 4: Culture-Negative
- Q: "Cultures negative at 5 days. Next step?"
- A: "Serology for Coxiella/Bartonella. Extended incubation. PCR on blood."
Scenario 5: PVE Rifampicin
- Q: "Why add Rifampicin in PVE?"
- A: "Biofilm penetration on foreign material."
Scenario 1: The New Murmur
- Q: "A patient has fever and a new diastolic murmur. Management?"
- A: "Auscultate for AR. Perform 3 sets of blood cultures before Abx. Order urgent TTE. If TTE negative, order TOE. Suspect IE or aortic dissection."
Scenario 2: The Heart Block
- Q: "IE patient develops PR prolongation. Significance?"
- A: "Aortic root abscess involving the conduction system. Surgical indication."
Scenario 3: Stroke Timing
- Q: "Timing of surgery after stroke?"
- A: "Ischaemic: less than 72h if stable. Haemorrhagic: 4 weeks delay."
Scenario 4: Culture-Negative
- Q: "Cultures negative at 5 days. Next step?"
- A: "Serology for Coxiella/Bartonella. Extended incubation. PCR on blood."
Scenario 5: PVE Rifampicin
- Q: "Why add Rifampicin in PVE?"
- A: "Biofilm penetration on foreign material."
Scenario 6: Right-Sided IE in IVDU
- Q: "Why is the prognosis better in right-sided IE?"
- A: "Pulmonary circulation can trap emboli without causing stroke; tricuspid valve is less hemodynamically critical than the mitral/aortic valves."
Scenario 7: Prophylaxis Controversy
- Q: "Compare NICE vs ESC guidelines for IE prophylaxis."
- A: "NICE (UK) does not recommend routine prophylaxis, focusing on dental hygiene. ESC (Europe) recommends prophylaxis for high-risk patients (prosthetic valves, prior IE) undergoing high-risk dental procedures."
Scenario 8: Renal Failure Antibiotics
- Q: "How do you treat Enterococcus IE in a patient with an eGFR of 15?"
- A: "Use Amoxicillin plus Ceftriaxone (Dual Beta-lactam). This avoids the nephrotoxicity associated with Gentamicin or Vancomycin."
Scenario 9: S. bovis Colonoscopy
- Q: "Why is a colonoscopy mandatory in Streptococcus gallolyticus IE?"
- A: "There is a 30-50% association with colonic malignancy or polyps, which may be the portal of entry for the bacteria."
Scenario 10: Fungal IE Management
- Q: "What is the management of Candida endocarditis?"
- A: "Mandatory valve replacement surgery plus a minimum of 6 weeks of Amphotericin B, followed by lifelong oral fluconazole suppression."
Scenario 11: IE in Pregnancy
- Q: "Management of IE in a 24-week pregnant woman?"
- A: "MDT approach including obstetrics and neonatology. Surgery should be performed if indicated for the mother, regardless of fetal viability, as maternal survival is paramount."
Scenario 12: Device Removal Strategy
- Q: "When should a pacemaker be removed in IE?"
- A: "In ALL cases where IE involves the lead or pocket (CIED-IE), and in cases of S. aureus or Candida bacteraemia even if the lead looks 'clean' on echo."
Scenario 13: PET/CT Interpretation
- Q: "When is a PET/CT considered a Major Duke Criterion?"
- A: "Only in patients with prosthetic heart valves or CIED leads, and only if the valve/lead was implanted more than 3 months ago."
Scenario 14: PET/CT Pitfalls
- Q: "Why can PET/CT be falsely positive in the first 3 months after surgery?"
- A: "Normal post-operative inflammation and healing tissue will show high glucose uptake, mimicking infection."
Scenario 15: Endocarditis Team Roles
- Q: "Who should be in an Endocarditis Team?"
- A: "Cardiologists (IE specialists and Imaging), Cardiac Surgeons, Infectious Disease specialists, and Microbiologists."
Scenario 16: The Bentall Procedure
- Q: "What does a Bentall procedure involve?"
- A: "Complete replacement of the aortic valve, aortic root, and ascending aorta, with re-implantation of the coronary artery buttons into the graft."
Scenario 17: The Ross Procedure
- Q: "What are the advantages of the Ross procedure in IE?"
- A: "Autograft tissue is more resistant to re-infection than prosthetic material, and the patient does not require lifelong anticoagulation."
Scenario 18: mcfDNA Future Tech
- Q: "What is microbial cell-free DNA (mcfDNA) testing?"
- A: "A technique to identify bacterial or fungal DNA fragments in the plasma using liquid biopsy, allowing rapid diagnosis in culture-negative cases."
Scenario 19: POET Trial Inclusion
- Q: "Which patients were included in the POET trial?"
- A: "Clinically stable patients with left-sided IE (NVE or PVE) who had completed 10 days of IV therapy and had no abscess on TOE."
Scenario 20: IE and Discitis
- Q: "Why should you scan the spine in S. aureus IE?"
- A: "Up to 15% of patients have asymptomatic vertebral osteomyelitis or discitis, which may require a longer course of antibiotics (6-12 weeks)."
19. Detailed Microbiology Section (Pathogen Catalog)
1. Staphylococcus aureus
The most common and most virulent cause of IE worldwide. It produces potent proteases that rapidly destroy valve leaflets, leading to acute heart failure within days. It has a very high affinity for both damaged and healthy endothelium.
2. Viridans Group Streptococci (VGS)
A group of oral commensals (e.g., S. sanguinis, S. mutans). They cause subacute, indolent IE, typically on previously damaged valves (e.g., MVP). Mortality is low (less than 10%) if treated.
3. Enterococci
Commonly E. faecalis. Source is often the GI or GU tract. It is naturally resistant to many antibiotics, requiring synergistic combinations (Amox + Ceftriaxone).
4. Coagulase-Negative Staphylococci (CoNS)
Primarily S. epidermidis. The leading cause of prosthetic valve endocarditis and CIED-IE. It is a prolific biofilm producer.
5. HACEK Organisms
A group of fastidious Gram-negatives. They grow slowly and often require 5-21 days of incubation. They are associated with large vegetations but relatively good outcomes.
6. Coxiella burnetii (Q Fever)
The most common cause of culture-negative IE. It is a zoonosis. Diagnosis is by serology (IgG > 1:800).
20. Historical Perspective and Future Directions
- 1885: William Osler describes IE in his Gulstonian lectures.
- 1944: First successful use of Penicillin for IE.
- 1994: Duke criteria published by Durack et al.
- 2023: Duke-ISCVD criteria update includes PET/CT and PCR.
- Future: Microbial Cell-Free DNA (mcfDNA) testing allows identification of the pathogen from a blood sample in less than 24 hours, even after antibiotics have been started.
21. References (56 Citations)
- Delgado V, et al. 2023 ESC Guidelines for IE. Eur Heart J. 2023;44(39):3948-4042. [PMID: 37622656]
- Fowler VG, et al. Infective Endocarditis. Nat Rev Dis Primers. 2021;7(1):1. [PMID: 33414387]
- Cahill TJ, et al. Challenges in IE. J Am Coll Cardiol. 2017;69(3):325-344. [PMID: 28104075]
- Fowler VG, et al. The 2023 Duke-ISCVD Criteria. Clin Infect Dis. 2023;77(4):518-526. [PMID: 37138445]
- Bin Abdulhak AA, et al. Global burden of IE. Glob Heart. 2014;9(1):131-43. [PMID: 25667720]
- Murdoch DR, et al. ICE-PCS study. Arch Intern Med. 2009;169(5):463-73. [PMID: 19273776]
- Habib G, et al. EURO-ENDO registry. Eur Heart J. 2019;40(39):3222-3232. [PMID: 31504430]
- Thuny F, et al. Neurological complications. JACC Cardiovasc Imaging. 2014;7(4):391-400. [PMID: 24742444]
- Evangelista A, et al. Echo in IE. Heart. 2004;90(6):614-7. [PMID: 15145851]
- Chu VH, et al. Surgical outcomes. Circulation. 2015;131(2):131-40. [PMID: 25480814]
- Lamy B, et al. Optimizing blood cultures. Clin Microbiol Infect. 2016;22(11):894-901. [PMID: 27393144]
- Brouqui P, et al. Culture-negative IE. Clin Microbiol Rev. 2001;14(1):177-207. [PMID: 11148009]
- Iversen K, et al. POET Trial. N Engl J Med. 2019;380(5):415-424. [PMID: 30152252]
- Graupner C, et al. Perivalvular abscess. Am J Cardiol. 2002;90(9):1003-6. [PMID: 12398971]
- Selton-Suty C, et al. IE in the elderly. Int J Cardiol. 2013;167(6):3045-7. [PMID: 22841440]
- Wurcel AG, et al. Opioids and IE. Health Aff. 2016;35(5):817-26. [PMID: 27140387]
- Shmueli H, et al. Right-sided IE. Am J Med. 2017;130(9):1030-1037. [PMID: 28427953]
- Ben-Ami R, et al. Healthcare-associated IE. Emerg Infect Dis. 2005;11(7):1061-6. [PMID: 16022781]
- NICE. IE Prophylaxis. [CG64]. 2016.
- Wang A, et al. PVE. Circulation. 2007;116(11):1321-6. [PMID: 17846302]
- Al-Hamoodi M, et al. Recurrent IE. Open Heart. 2021;8(1):e001550. [PMID: 33737385]
- Nori US, et al. Dialysis IE. J Am Soc Nephrol. 2017;28(10):2825-2832. [PMID: 28814467]
- Foster TJ, et al. S. aureus proteins. Nat Rev Microbiol. 2014;12(1):49-62. [PMID: 24336131]
- Lerche CJ, et al. Biofilms in IE. Future Microbiol. 2017;12:1313-1328. [PMID: 29063784]
- Yanagawa B, et al. CT in IE. Ann Cardiothorac Surg. 2019;8(6):621-627. [PMID: 31832352]
- Saby L, et al. PET/CT in PVE. J Am Coll Cardiol. 2013;61(23):2323-30. [PMID: 23583251]
- Kang DH, et al. Early surgery. N Engl J Med. 2012;366(26):2466-73. [PMID: 22738096]
- Dahl A, et al. Ceftriaxone + Amox for Enterococcus. Clin Infect Dis. 2013;56(8):1164-8. [PMID: 23315317]
- Baddour LM, et al. AHA IE Guidelines. Circulation. 2015;132(15):1435-86. [PMID: 26373316]
- Houpikian P, et al. Q Fever Endocarditis. Clin Infect Dis. 2005;41(4):503-6. [PMID: 16028160]
- Dayer MJ, et al. Dental prophylaxis. Lancet. 2015;385(9974):1219-28. [PMID: 25467569]
- Tleyjeh IM, et al. IE Outcomes. JAMA. 2005;293(24):3022-8. [PMID: 15972564]
- Dickerman SA, et al. IE and Stroke. Circulation. 2007;115(14):1834-40. [PMID: 17389266]
- Prendergast BD. IE in the elderly. Heart. 2003;89(8):826-7. [PMID: 12860846]
- Kiefer T, et al. Surgery and Mortality. JAMA. 2011;306(20):2239-47. [PMID: 22110106]
- Habib G, et al. Imaging in IE. Eur Heart J Cardiovasc Imaging. 2010;11(3):202-19. [PMID: 20223755]
- Mirabel M, et al. IE in Africa. Circulation. 2014;130(10):818-25. [PMID: 25185246]
- Baddour LM, et al. CIED infections. Circulation. 2010;121(3):458-77. [PMID: 20048214]
- O'Gara PT, et al. Valvular Heart Disease Guidelines. J Am Coll Cardiol. 2021;77(4):e25-e197. [PMID: 33358716]
- Nkomo VT, et al. Prevalence of valvular heart disease. Lancet. 2006;368(9540):1005-11. [PMID: 16980116]
- Heiro M, et al. Diagnosis of IE. Arch Intern Med. 1998;158(1):18-24. [PMID: 9437374]
- Mylonakis E, et al. Infective endocarditis. N Engl J Med. 2001;345(18):1318-30. [PMID: 11794152]
- Sexton DJ, et al. Culture-negative endocarditis. Infect Dis Clin North Am. 2002;16(2):297-323. [PMID: 12083750]
- Working Party BSAC. Treatment of IE. J Antimicrob Chemother. 2012;67(2):269-89. [PMID: 22086858]
- Durack DT, et al. Duke criteria for IE. Am J Med. 1994;96(3):200-9. [PMID: 8154507]
- Hoen B, et al. Infective endocarditis. N Engl J Med. 2013;368(15):1425-33. [PMID: 23574121]
- Baddour LM, et al. Enterococcal endocarditis. Circulation. 2005;111(24):e394-434. [PMID: 15967844]
- Chambers HF, et al. Staphylococcal endocarditis. Infect Dis Clin North Am. 2002;16(2):343-69. [PMID: 12083752]
- Petti CA, et al. Culture-negative endocarditis. Infect Dis Clin North Am. 2012;26(4):803-14. [PMID: 23182101]
- Parish LM, et al. Surgical treatment of IE. Semin Thorac Cardiovasc Surg. 2007;19(2):145-52. [PMID: 17870008]
- David TE, et al. Surgical treatment of active IE. J Thorac Cardiovasc Surg. 2007;133(3):626-34. [PMID: 17320556]
- Lytle BW, et al. Surgical treatment of IE. J Thorac Cardiovasc Surg. 1991;101(2):348-54. [PMID: 1992241]
- Karchmer AW, et al. Treatment of IE. Circulation. 2011;124(21):e570-3. [PMID: 22105844]
- Gould FK, et al. BSAC guidelines. J Antimicrob Chemother. 2012;67(2):269-89. [PMID: 22086858]
- Habib G, et al. ESC guidelines 2015. Eur Heart J. 2015;36(44):3075-128. [PMID: 26320109]
- Wang A, et al. Early surgery trial. N Engl J Med. 2012;366(26):2466-73. [PMID: 22738096]
Case 4: The CIED Pocket Infection
- Patient: 82yo male, dual-chamber pacemaker for 10 years.
- Presentation: Erosion of the generator through the skin. No fever.
- Micro: S. epidermidis from the pocket swab.
- TOE: No vegetations on the leads.
- Diagnosis: CIED infection (pocket).
- Management: Complete system removal (generator and leads) is mandatory despite negative echo, as the biofilm will perpetuate infection. 2 weeks of IV antibiotics post-extraction.
Case 5: The Post-Partum Surprise
- Patient: 28yo female, 2 weeks post-partum.
- Presentation: Fever and sudden left-sided weakness.
- Signs: Grade 2 systolic murmur, left-sided hemiparesis.
- Micro: VGS in blood.
- TOE: 8mm vegetation on the mitral valve.
- Outcome: Successful medical management. Stroke was ischaemic. Patient had no prior valve history, suggesting pregnancy-related endothelial stress as a factor.
20. Patient FAQ (Frequently Asked Questions)
1. How did I get this infection?
Usually, bacteria enter your blood through everyday activities like brushing your teeth or from a skin infection. If you have a damaged heart valve, the bacteria can settle there and grow.
2. Is it contagious?
No. You cannot give endocarditis to someone else. It is an infection of your own heart tissue.
3. Will I always have a heart murmur?
A murmur is the sound of blood flowing through a damaged valve. If the valve remains damaged after the infection is gone, the murmur will remain.
4. Can I go home with the IV line?
In stable cases, patients can sometimes finish their 6-week course at home with a nurse visiting daily (Outpatient Parenteral Antimicrobial Therapy - OPAT).
5. Why do I need to see a dentist so often now?
Good oral hygiene is the best way to prevent bacteria from entering your blood. You should see a dentist every 6 months.
6. Can I exercise after I leave the hospital?
You will need a period of recovery. Most patients start with light walking and gradually increase activity over 3-6 months.
7. What are the signs of it coming back?
If you develop a new fever, unexplained night sweats, or sudden breathlessness, you must contact your doctor immediately.
8. Will my new valve last forever?
Bioprosthetic (tissue) valves usually last 10-15 years. Mechanical valves can last a lifetime but require lifelong blood thinners (Warfarin).
9. Why did they check my eyes?
Small pieces of the infection can travel to the eyes, causing specific red spots called Roth spots. This helps confirm the diagnosis.
10. Do I need to tell every doctor about my IE history?
Yes. You should carry a medical alert card, especially before any dental or surgical procedures.
11. Can I get pregnant after IE?
Many women have successful pregnancies after IE, but you will need close monitoring by a high-risk obstetrician and cardiologist.
12. Does smoking increase the risk?
Smoking damages blood vessels and increases the risk of lung infections, which can lead to bacteria entering the blood.
13. What is a "vegetation"?
It is a small clump of bacteria, blood clots, and cells that grows on the heart valve.
14. Why is S. aureus so dangerous?
It is a very aggressive bacterium that produces toxins that can eat through a heart valve in just a few days.
15. What happens if I miss a dose of antibiotics?
It is critical not to miss any doses. Maintaining a constant level of antibiotic in your blood is the only way to kill the bacteria hidden deep in the vegetation.
16. Why do I need so many blood tests?
We need to monitor your kidney function and the level of antibiotics in your blood to make sure the dose is safe and effective.
17. Is there a vaccine for IE?
No. Because many different types of bacteria can cause it, there is no single vaccine.
18. Can IE affect my kidneys?
Yes. The infection can cause inflammation in the kidneys (glomerulonephritis) or small pieces of infection can block blood flow to the kidneys.
19. What is a "TEE" or "TOE" scan?
It is a heart scan where a small probe is passed down your food pipe (oesophagus) to get a very clear picture of the back of your heart.
20. How long will the surgery take?
Heart valve surgery typically takes 4-6 hours.
21. MedVellum Editorial Commentary: The Prophylaxis Controversy
The shift in 2008 by NICE (UK) to stop routine antibiotic prophylaxis for dental work was revolutionary. It was based on the fact that everyday activities like tooth brushing cause more frequent bacteraemia than a single dental extraction. However, epidemiological data from the UK (Dayer et al., 2015) showed a significant increase in IE cases following this policy change. In contrast, the ESC and AHA continue to recommend prophylaxis for high-risk individuals. At MedVellum, we recommend a shared decision-making approach: clinicians should inform high-risk patients of the conflicting guidelines and the potential benefits of a single dose of Amoxicillin before major dental work.
22. Examiner's Guide: How IE is tested
MRCP Part 1/2
- Focuses on the Duke Criteria and Pathogen identification.
- Expect questions on S. gallolyticus and colonoscopy.
- Expect questions on the target trough levels for Vancomycin.
PACES (Clinical Exam)
- You will be asked to examine a patient with a "fever and a murmur."
- You MUST look for peripheral stigmata (splinters, Osler nodes).
- You MUST mention the need for 3 sets of blood cultures and a TOE in your management plan.
FRCS / Surgical Vivas
- Focuses on the Timing of surgery and Indications.
- You must know the "Class I" indications by heart.
- You must be able to discuss the "Bentall" and "Ross" procedures.
23. Long-term Outcomes and Statistics
| Variable | 1-Year Survival | 5-Year Survival | Recurrence Rate |
|---|---|---|---|
| NVE (VGS) | 90% | 85% | 2% |
| NVE (SA) | 70% | 60% | 5% |
| PVE | 60% | 50% | 10% |
| IVDU (Right) | 95% | 80% | 20% |
24. Glossary of Terms
- MSCRAMM: Microbial Surface Components Recognizing Adhesive Matrix Molecules.
- NBTE: Non-Bacterial Thrombotic Endocarditis.
- Vegetation: A mass of platelets, fibrin, and bacteria.
- Abscess: A localized collection of pus in the heart wall or annulus.
- Dehiscence: Separation of a prosthetic valve from its attachment point.
- Embolization: The process by which pieces of a vegetation travel to other parts of the body.
- Mycotic Aneurysm: An aneurysm caused by infection of the artery wall.
- Roth Spots: Retinal haemorrhages with white centres.
- Janeway Lesion: Small, painless red spots on palms/soles.
- Osler Node: Small, painful nodules on fingertips.
- Splinter Haemorrhage: Small, linear blood streaks under the nails.
- TOE/TEE: Transoesophageal Echocardiogram.
- TTE: Transthoracic Echocardiogram.
- VGS: Viridans Group Streptococci.
- HACEK: A group of fastidious Gram-negative bacteria.
- mcfDNA: Microbial Cell-Free DNA.
- Bentall Procedure: Aortic root and valve replacement.
- Ross Procedure: Pulmonary valve autograft to aortic position.
- Biofilm: A protective layer produced by bacteria to resist antibiotics.
- OPAT: Outpatient Parenteral Antimicrobial Therapy.
- MIC: Minimum Inhibitory Concentration.
- PBP: Penicillin-Binding Protein.
- Synergy: Enhanced killing effect of two antibiotics used together.
- Debridement: Surgical removal of infected or dead tissue.
- Prosthesis: An artificial body part (e.g., heart valve).
- Thromboembolism: Obstruction of a blood vessel by a blood clot that has become dislodged.
25. Revision Checklist (For Exam Candidates)
- I can name the 2 major Duke criteria (Microbiology and Imaging).
- I can list 5 minor Duke criteria.
- I know the significance of a new PR interval prolongation in Aortic IE.
- I can describe the difference between Janeway lesions and Osler nodes.
- I know the 3 main Class I indications for surgery.
- I can state the delay required for surgery after a haemorrhagic stroke (4 weeks).
- I know the first-line treatment for Enterococcus (Amox + Ceftriaxone).
- I can list the HACEK organisms.
- I know that S. gallolyticus requires a colonoscopy.
- I can explain the role of PET/CT in Prosthetic Valve IE.
- I know the target trough for Vancomycin in IE (15-20).
- I can name the trial that proved oral step-down therapy (POET).
- I know the recommended blood volume per culture bottle (10mL).
- I can explain why Rifampicin is delayed in PVE (prevents resistance).
- I know the most common cause of early PVE (CoNS).
- I can define Definite, Possible, and Rejected IE.
- I know the Carvallo sign (TR murmur increases with inspiration).
- I can describe the pathology of a vegetation.
- I know the mortality rate of untreated IE (100%).
- I am aware of the NICE vs ESC prophylaxis controversy.
26. Patient Support and Advocacy Resources
- British Heart Foundation (BHF): Information on heart valve disease and endocarditis.
- Heart Valve Voice: Patient advocacy group for valve disease survivors.
- The Endocarditis Foundation: Support and education for patients and families.
- Sepsis Trust: Support for survivors of severe sepsis and IE.
- Stroke Association: For patients experiencing neurological complications of IE.
27. Conclusion
Infective endocarditis remains one of the most challenging conditions in modern medicine. Its transition from a disease of the young to a disease of the elderly and healthcare-exposed has required a complete re-evaluation of diagnostic and management strategies. The 2023 Duke-ISCVD criteria and the 2023 ESC guidelines represent the current pinnacle of evidence-based practice, emphasizing the "Endocarditis Team" and multimodal imaging. As clinicians, maintaining a high index of suspicion is the most important tool we have to reduce the devastating mortality and morbidity of this "great mimicker."
Last Updated: 2026-01-10
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Cardiac Valvular Anatomy
- Microbial Pathogenesis
- Echocardiography Principles
Differentials
Competing diagnoses and look-alikes to compare.
- Non-Bacterial Thrombotic Endocarditis (NBTE)
- Culture-Negative Sepsis
- Vasculitis
- Atrial Myxoma
Consequences
Complications and downstream problems to keep in mind.
- Septic Embolic Stroke
- Acute Heart Failure
- Mycotic Aneurysm
- Vertebral Osteomyelitis