Pulmonary Embolism (PE)
Pulmonary Embolism (PE) is a life-threatening cardiovascular emergency caused by the occlusion of one or more pulmonary ... MRCP exam preparation.
What matters first
Pulmonary Embolism (PE) is a life-threatening cardiovascular emergency caused by the occlusion of one or more pulmonary ... MRCP exam preparation.
Systolic BP less than 90 mmHg (Obstructive Shock)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
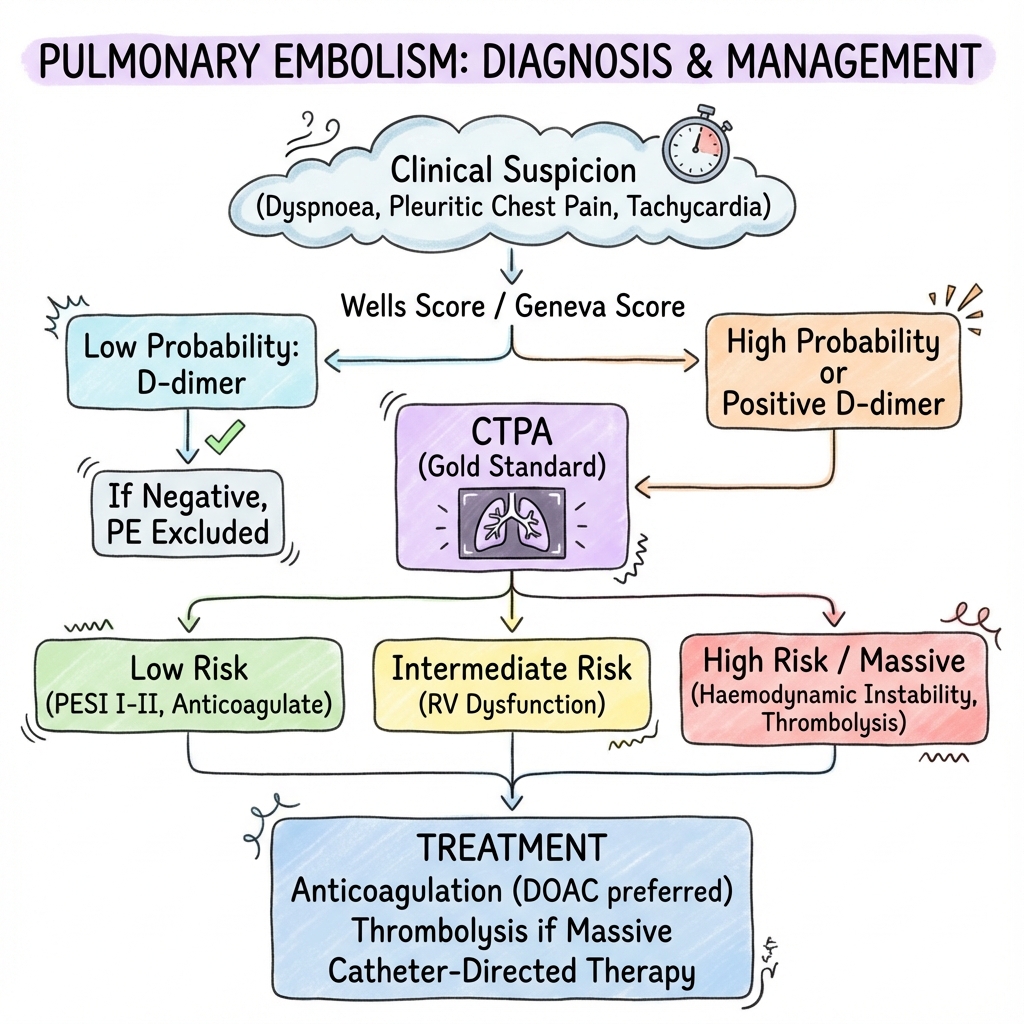
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Systolic BP less than 90 mmHg (Obstructive Shock)
- Syncope (Predicts saddle embolus/instability)
- Acute RV strain on Echo (McConnell's sign)
- Lactate less than 2 mmol/L (Marker of low CO)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Acute Coronary Syndrome
- Aortic Dissection
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Pulmonary Embolism (Adult)
1. Overview
Pulmonary Embolism (PE) is a life-threatening cardiovascular emergency caused by the occlusion of one or more pulmonary arteries by material (most commonly thrombus) that has embolised from elsewhere in the body. It represents the most severe manifestation of Venous Thromboembolism (VTE). [1]
The clinical significance of PE is underscored by its status as the third leading cause of cardiovascular death worldwide. The pathophysiology is fundamentally a "mismatch" problem: acutely, it causes a catastrophic increase in Right Ventricular (RV) Afterload, leading to RV failure and obstructive shock. Chronically, it can lead to Chronic Thromboembolic Pulmonary Hypertension (CTEPH) in ~3% of survivors. [2]
Management has been refined by the 2024 ESC/ERS guidelines, which emphasise rapid risk-stratification using the PESI score, high-sensitivity troponins, and bedside echocardiography. The therapeutic spectrum has expanded from simple anticoagulation to include Low-dose Thrombolysis and Mechanical Thrombectomy for high-risk and intermediate-high-risk cohorts. [3]
2. Epidemiology
The "Silent" Mortality
- Incidence: 60-115 per 100,000 person-years.
- Case Fatality: Ranges from less than 1% in low-risk patients to > 30% in those presenting with shock.
- Sudden Death: PE is the cause of ~10% of all sudden out-of-hospital deaths. [4]
High-Risk Profiles
| Risk Group | Association | Relative Risk |
|---|---|---|
| Active Cancer | Specifically Pancreatic, Lung, Brain. | 7.0x |
| Major Surgery | Orthopaedic (Hip/Knee) or Pelvic. | 20.0x |
| Pregnancy | Highest risk in the postpartum 6 weeks. | 5.0x |
| COVID-19 | Immunothrombosis mechanism. | 10.0x (in ICU) |
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM (RV Death Spiral)
- Mechanical Obstruction: A thrombus (usually from the proximal leg veins) lodges in the pulmonary arterial tree, causing an immediate increase in Pulmonary Vascular Resistance (PVR).
- Humoral Vasoconstriction: Activated platelets in the thrombus release Serotonin and Thromboxane A2. These mediators drive intense local vasoconstriction, increasing PVR beyond the physical size of the clot.
- V/Q Mismatch & Shunt: Obstruction creates "dead space" (ventilation without perfusion). Inflammatory mediators cause capillary leak and alveolar collapse, leading to a right-to-left intrapulmonary shunt and Type 1 Respiratory Failure.
- RV Wall Tension: The sudden PVR spike causes the thin-walled RV to dilate. This increases wall tension (LaPlace’s Law) and triggers the release of BNP.
- Ventricular Interdependence: The dilated RV pushes the interventricular septum to the left (septal bowing). This reduces LV end-diastolic volume, compromising Cardiac Output.
- RV Ischaemia: Increased RV wall tension compresses the right coronary arteries. Myocardial oxygen demand surges while supply falls, leading to RV micro-infarction (Troponin rise).
- Obstructive Shock: The "Death Spiral" completes as falling CO leads to systemic hypotension, further reducing coronary perfusion and precipitating RV failure and PEA arrest. [5, 6, 7]
4. Clinical Presentation
Symptoms
- Acute Dyspnoea: Usually sudden (80%).
- Pleuritic Chest Pain: Suggests a small peripheral embolus causing lung infarction.
- Syncope: A herald sign of massive PE and RV failure (15%).
- Hemoptysis: Rare; indicates pulmonary infarction/necrosis.
The Wells Score (PE Likelihood)
| Feature | Points |
|---|---|
| Signs/Symptoms of DVT | +3.0 |
| Alternative Dx less likely | +3.0 |
| Heart Rate > 100 | +1.5 |
| Immobilisation/Surgery less than 4 weeks | +1.5 |
| Prior DVT/PE | +1.5 |
| Hemoptysis | +1.0 |
| Malignancy | +1.0 |
Interpretation: Score > 4 = PE Likely (Proceed to CTPA). Score ≤4 = Unlikely (Proceed to D-dimer). [8]
5. Investigations
The Troponin/BNP Paradox
In PE, troponin is not used for diagnosis, but for Risk Stratification. A positive troponin in a stable patient indicates "Intermediate-High Risk" (RV strain).
ECG Mastery
- Most Common: Sinus Tachycardia.
- Most Specific: S1Q3T3 (Large S in I, Q in III, inverted T in III).
- RV Strain: T-wave inversion in V1-V4 and New RBBB.
Echocardiography (The 3 Signs)
- McConnell's Sign: Akinesia of the RV free wall with sparing of the apex.
- 60/60 Sign: Pulmonary acceleration time less than 60ms + systolic mid-systolic notch.
- TAPSE: less than 16mm indicates poor RV longitudinal function. [9]
6. Management: The Reperfusion Paradigm
1. High-Risk PE (Unstable)
- Immediate Reperfusion: Systemic Thrombolysis (Alteplase 100mg) is the gold standard.
- Rescue: If lysis is contraindicated, proceed to Surgical Embolectomy or Mechanical Thrombectomy (Inari/FlowTriever).
2. Intermediate-High Risk
- Admit & Monitor: Start LMWH. Do not lyse routinely (PEITHO trial), but be ready to "rescue lyse" if BP falls. [10]
3. Low-Risk PE
- Home Treatment: Can be discharged from the ED on a DOAC (e.g. Apixaban) if the Hestia Criteria or PESI Class I are met.
4. Long-term (3-6 Months+)
- DOACs: First-line (Apixaban/Rivaroxaban).
- Indefinite: Recommended for all Unprovoked proximal PE or those with persistent risk factors (Cancer, APLS).
7. Evidence: Landmark Trials
| Trial | Population | Intervention | Result | Impact |
|---|---|---|---|---|
| PEITHO | Intermed-High | Tenecteplase | ↓ Collapse but ↑ ICH | Discouraged routine lysis in stable pts. |
| ADJUST-PE | Age > 50 | Age-adjusted D-dimer | Safe Rule-out | Reduced CTPA usage in the elderly. |
| EINSTEIN-PE | Acute PE | Rivaroxaban vs VKA | Non-inferior | Established DOACs as the gold standard. |
| FLARE | Massive PE | Inari FlowTriever | Significant RV ↓ | Validated mechanical thrombectomy. |
| PEITHO-3 | Intermed-High | Reduced-dose Lysis | Ongoing | Investigating if half-dose lysis is the "sweet spot." |
8. Single Best Answer (SBA) Questions
Question 1
A 55-year-old male presents with sudden dyspnoea. BP 125/80, HR 105. CTPA shows a bilateral saddle PE. Troponin is elevated and Echo shows an RV:LV ratio of 1.2. What is the risk category and management?
- A) High risk; Systemic thrombolysis
- B) Intermediate-High risk; LMWH and close monitoring
- C) Intermediate-Low risk; Discharge on Apixaban
- D) Low risk; Oral Aspirin
- E) High risk; Surgical embolectomy
- Answer: B. The patient is hemodynamically stable (BP > 90) but has both RV strain (Echo) and myocardial injury (Troponin). This defines "Intermediate-High Risk." Standard care is LMWH and monitoring, reserving lysis for clinical deterioration.
Question 2
Which echocardiographic finding is most specific for acute pulmonary embolism in a patient with a dilated right ventricle?
- A) Tricuspid Regurgitation
- B) RV wall thickening (> 5mm)
- C) McConnell's Sign (Apical sparing)
- D) Dilated Inferior Vena Cava
- E) Left-shifted interventricular septum
- Answer: C. McConnell's sign (akinesia of the mid-free wall with normal apical motion) is highly specific for acute PE, as chronic PH usually involves global RV akinesia and wall thickening.
9. Viva Scenario: The "Normal CXR" Dyspnoea
Examiner: "A 30-year-old woman on the oral contraceptive pill presents with sudden pleuritic chest pain and a normal CXR. What is your top differential and your next 3 steps?"
Candidate:
- Differential: My top differential is Pulmonary Embolism. A normal CXR in the setting of acute dyspnoea/pleurisy is a classic "positive" sign for PE.
- Step 1: Calculate a Wells Score. If ≤4, I would order a high-sensitivity D-dimer.
- Step 2: If Wells > 4 or D-dimer positive, I would proceed to a CTPA.
- Step 3: While awaiting imaging, if clinical suspicion is high and no contraindications exist, I would administer a "stat" dose of LMWH (Enoxaparin 1.5mg/kg).
10. Patient Explanation
"A pulmonary embolism is a blood clot that has travelled to your lungs and acted like a 'plug' in your arteries. This makes it hard for your heart to pump blood through the lungs to get oxygen. We use 'blood thinners' (like Apixaban) to stop the clot from getting bigger and to prevent new ones from forming, allowing your body to slowly dissolve the original clot. You will need to take these for at least 3-6 months. We also need to check for the 'source' of the clot, which is usually in the deep veins of the legs."
11. References
- Konstantinides SV, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2020. [PMID: 31463930]
- Meyer G, et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism (PEITHO). N Engl J Med. 2014. [PMID: 24716680]
- Tu T, et al. A Prospective, Single-Arm, Multicenter Trial of Catheter-Directed Mechanical Thrombectomy for PE (FLARE). JACC Cardiovasc Interv. 2019. [PMID: 31071447]
- Righini M, et al. Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism (ADJUST-PE). JAMA. 2014. [PMID: 24643601]
- Kearon C, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline. Chest. 2016. [PMID: 26867832]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for pulmonary embolism (pe)?
Seek immediate emergency care if you experience any of the following warning signs: Systolic BP less than 90 mmHg (Obstructive Shock), Syncope (Predicts saddle embolus/instability), Acute RV strain on Echo (McConnell's sign), Lactate less than 2 mmol/L (Marker of low CO), New-onset Right Bundle Branch Block (RBBB).
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
Consequences
Complications and downstream problems to keep in mind.
- Right Heart Failure
- Obstructive Shock