Rheumatoid Arthritis
Rheumatoid Arthritis (RA) is a chronic, systemic, inflammatory autoimmune disorder primarily characterised by a symmetri... MRCP exam preparation.
What matters first
Rheumatoid Arthritis (RA) is a chronic, systemic, inflammatory autoimmune disorder primarily characterised by a symmetri... MRCP exam preparation.
Atlanto-axial subluxation (neck pain, neurological signs)
5 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Atlanto-axial subluxation (neck pain, neurological signs)
- Scleritis (deep, boring eye pain, vision-threatening)
- Mononeuritis multiplex (sudden foot/wrist drop)
- Felty's syndrome (RA + Splenomegaly + Neutropenia)
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Psoriatic Arthritis
- Systemic Lupus Erythematosus
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Rheumatoid Arthritis (Adult)
1. Overview
Rheumatoid Arthritis (RA) is a chronic, systemic, inflammatory autoimmune disorder primarily characterised by a symmetrical, erosive polyarthritis of the synovial joints. Beyond the joints, it is a multisystem "Rheumatoid Disease" that drives accelerated atherosclerosis, interstitial lung disease, and systemic vasculitis. [1]
The hallmark of RA is the loss of immune tolerance to self-antigens, specifically citrullinated proteins. The 2010 ACR/EULAR classification shifted the diagnostic focus from late-stage deformities to early inflammatory features, enabling the "Hit Hard, Hit Early" paradigm. A "Window of Opportunity" exists in the first 12 weeks of symptoms where aggressive initiation of Disease-Modifying Anti-Rheumatic Drugs (DMARDs) can fundamentally alter the disease's natural history, potentially inducing drug-free remission. [2]
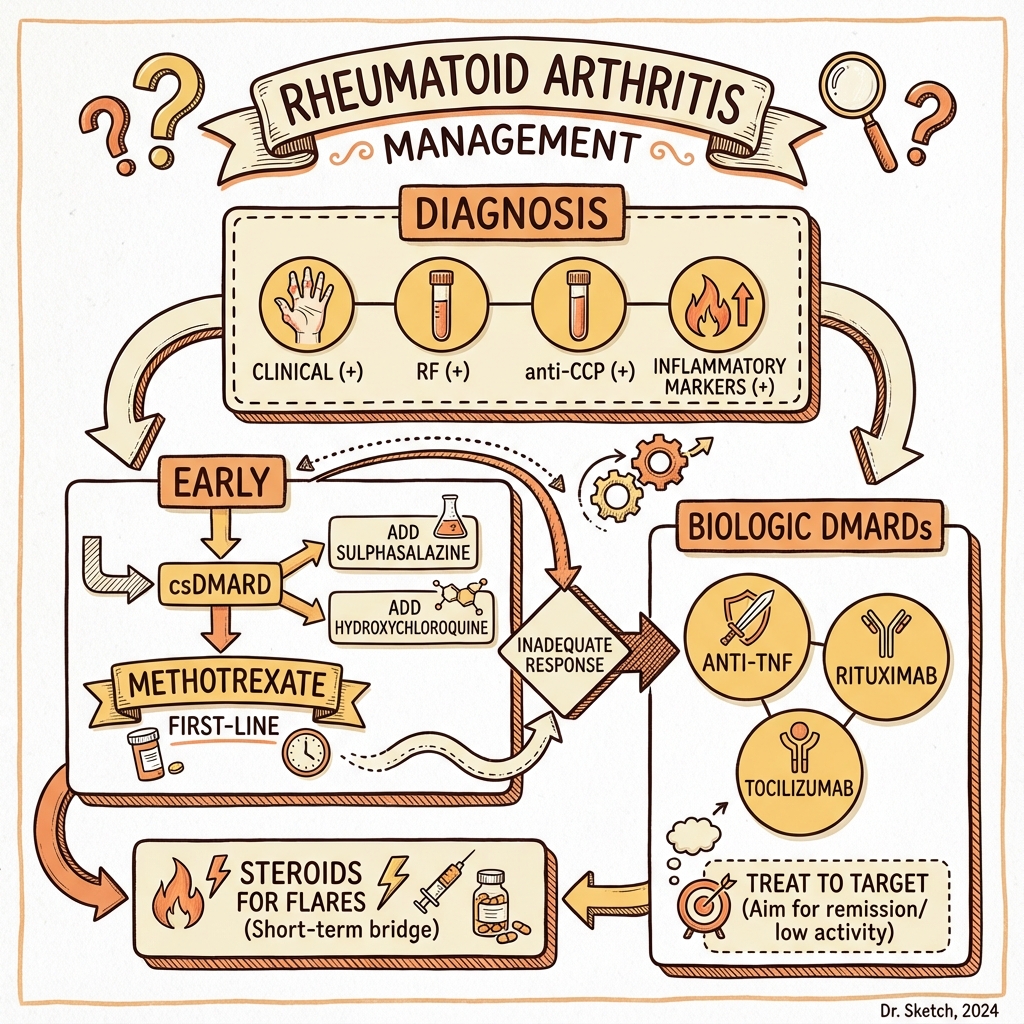
Management is governed by the "Treat-to-Target" principle, aiming for clinical remission (DAS28 less than 2.6). The therapeutic landscape has been transformed by the sequential use of conventional synthetic DMARDs (Methotrexate), biological DMARDs (Anti-TNF, Anti-IL6), and targeted synthetic DMARDs (JAK inhibitors). [3]
2. Epidemiology
Global Prevalence
- Stats: Affects ~1% of the adult population worldwide.
- Gender: Sizable female preponderance (3:1 ratio), though this gap narrows in older age groups.
- Onset: Typically 30-50 years, but "Late-Onset RA" (> 60 years) is increasingly recognised and often follows a more aggressive, large-joint pattern. [4]
The "Shared Epitope"
Genetic susceptibility is strongly linked to the HLA-DRB1 locus. The "Shared Epitope" is a specific 5-amino acid sequence in the peptide-binding groove of the HLA-DRβ chain. It preferentially presents citrullinated peptides to T-cells, explaining the powerful Gene-Environment interaction with smoking. [5]
3. Aetiology & Pathophysiology
⚠️ THE 7-STEP MOLECULAR MECHANISM
- Citrullination (The Neo-antigen): Environmental triggers (Smoking or P. gingivalis periodontitis) activate the enzyme PAD (Peptidyl Arginine Deiminase). Arginine residues on proteins (fibrinogen, vimentin) are converted to Citrulline.
- MHC-II Presentation: In individuals with the "Shared Epitope" (HLA-DR4/DR1), these citrullinated "neo-antigens" fit perfectly into the MHC-II groove of Dendritic cells.
- Germinal Centre Reaction: Dendritic cells migrate to lymph nodes and activate CD4+ T-helper cells. This drives B-cell class-switching to produce ACPA (Anti-Citrullinated Protein Antibodies) and Rheumatoid Factor (RF).
- Synovial Homing: ACPAs enter the joint space. They bind to citrullinated proteins on the synovial membrane, forming immune complexes that activate the Complement System and recruit Macrophages.
- The Pannus Formation: Chronic inflammation causes the normally thin synovium to hyper-proliferate into a thick, invasive tissue called Pannus. This tissue behaves like a "locally invasive tumour."
- Cytokine Storm: Macrophages and T-cells in the pannus release the "Destructive Triad": TNF-α, IL-6, and IL-1. TNF-α upregulates RANK-L on T-cells.
- Erosive Destruction: RANK-L activates Osteoclasts at the pannus-bone interface, leading to marginal bone erosions. Matrix Metalloproteinases (MMPs) simultaneously degrade the cartilage matrix, resulting in joint space narrowing. [6, 7]
4. Clinical Presentation
Articular Features
- Symmetry: Essential for diagnosis. Affects MCPs, PIPs, Wrists, and MTPs. (DIPs are classically spared; involvement suggests OA or Psoriatic).
- Morning Stiffness: Lasts > 1 hour; improves with activity (unlike OA).
- Joint Deformities (Late):
- Ulnar Deviation at the MCPs.
- Swan-neck (PIP hyperextension, DIP flexion).
- Boutonnière (PIP flexion, DIP hyperextension).
- Atlanto-axial Subluxation: Synovitis of the transverse ligament of C1; risk of cord compression.
Extra-Articular Features (The "Seropositive" Body)
- Rheumatoid Nodules: Found on extensor surfaces (elbows, Achilles). Pathognomonic for seropositive RA.
- Lungs: Interstitial Lung Disease (ILD) - usually a UIP pattern. Caplan's Syndrome (RA + Coal worker's pneumoconiosis).
- Eyes: Episcleritis (benign) vs. Scleritis (emergency; can cause Scleromalacia Perforans/globe rupture).
- Heart: Pericarditis and accelerated CAD (RA is an "IHD Risk Equivalent"). [8]
5. Investigations
The Serological Doublet
- Rheumatoid Factor (RF): IgM against the Fc portion of IgG. Sensitive (70%) but poor specificity (found in SBE, TB, SLE).
- Anti-CCP (ACPA): Highly specific (> 95%). Presence predicts aggressive, erosive disease and poor prognosis.
Imaging Strategy
- X-Rays (Hands/Feet): Look for Peri-articular osteopenia (earliest sign) and Marginal Erosions.
- Ultrasound (Power Doppler): Used in early RA to detect "subclinical synovitis" (hypervascularity) when physical exam is equivocal.
- MRI: Most sensitive for detecting Bone Marrow Oedema, which is the strongest predictor of future erosions. [9]
6. Management: The Pyramid of Care
1. The Anchor: Methotrexate (MTX)
- Dose: 15-25mg ONCE WEEKLY (Oral or SC).
- Supplement: Folic acid 5mg weekly (on a different day) to reduce mucosal/liver toxicity.
- Toxicities: Myelosuppression, Liver Fibrosis, and Pneumonitis (acute dry cough - stop MTX immediately).
2. Triple Therapy (csDMARDs)
If MTX monotherapy fails: Methotrexate + Sulfasalazine + Hydroxychloroquine.
3. Biological Revolution (bDMARDs)
Indicated if DAS28 > 5.1 despite two conventional DMARDs.
- Anti-TNF (Adalimumab/Etanercept): Must screen for Latent TB and Hep B/C before starting.
- Rituximab (Anti-CD20): Preferred in seropositive patients failing Anti-TNF.
- Tocilizumab (Anti-IL6): Highly effective; note that it suppresses CRP, rendering it useless as a marker of infection.
4. JAK Inhibitors (tsDMARDs)
- Baricitinib / Upadacitinib: Oral alternative to biologics.
- 2024 Safety Note: Use with caution in those > 65 or smokers due to increased risk of VTE and MACE (ORAL Surveillance trial). [10]
7. Evidence: Landmark Trials
| Trial | Population | Intervention | Result | Impact |
|---|---|---|---|---|
| TICORA | Early RA | Tight Control | SGR 0.42 | Proved that monthly review/target improves outcomes. |
| BeSt | Early RA | Initial Triple/Bio | Better Erosions | Promoted early aggressive combination therapy. |
| ACROSS | ACPA+ | Abatacept | Delayed RA | Investigating "Pre-clinical RA" prevention. |
| ORAL Surv. | RA > 50y | Tofacitinib vs. TNF | ↑ MACE/VTE | Black-box warning for JAKi in high-risk patients. |
8. Single Best Answer (SBA) Questions
Question 1
A 45-year-old female with long-standing RA is scheduled for an elective cholecystectomy. She has occasional neck pain but no neurological symptoms. What is the most important preoperative investigation?
- A) Pulmonary Function Tests
- B) Cervical Spine X-Ray (Flexion/Extension views)
- C) Echocardiogram
- D) Anti-CCP titre
- E) CRP levels
- Answer: B. Atlanto-axial subluxation can be asymptomatic. Neck extension during intubation can cause catastrophic cord compression. Lateral flexion/extension films are mandatory.
Question 2
A patient on Methotrexate for 3 months presents with a dry cough and a fever of 37.5°C. CXR shows diffuse interstitial infiltrates. What is the immediate management?
- A) Start Amoxicillin for community-acquired pneumonia
- B) Increase Folic Acid to 5mg daily
- C) Stop Methotrexate and arrange urgent respiratory review
- D) Start Prednisolone 40mg and continue Methotrexate
- E) Check a procalcitonin level
- Answer: C. This is a classic presentation of Methotrexate Pneumonitis, an idiosyncratic hypersensitivity reaction. The drug must be stopped permanently.
9. Viva Scenario: The "Pre-clinical" Patient
Examiner: "A 30-year-old smoker is found to have a high-titre Anti-CCP while being screened for another condition. They have no joint pains. What is the risk and your advice?"
Candidate:
- Risk: I would explain that ACPA is highly specific and can precede clinical RA by up to 10 years. This patient is in the "Pre-clinical RA" phase.
- Advice: The most critical intervention is Smoking Cessation. Smoking drives citrullination in the lungs and provides the "second hit" needed to transition to clinical disease.
- Monitoring: I would counsel them on the symptoms of early synovitis (morning stiffness, knuckle pain) and review them if symptoms emerge.
- Evidence: I would mention that trials (like ARIAA) are investigating if short courses of Abatacept can prevent the transition to full RA in this cohort.
10. Patient Explanation
"Rheumatoid Arthritis is not just 'wear and tear' arthritis; it's a condition where your immune system is 'confused' and starts attacking the lining of your joints. Think of your joint as a hinges on a door—the inflammation acts like rust that eventually eats into the metal (bone). Our goal is to 'Hit it Hard' early on with medications like Methotrexate to stop that rust before it causes permanent damage. This isn't just about joints—controlling the inflammation also protects your heart and lungs for the future."
11. References
- Smolen JS, et al. EULAR recommendations for the management of rheumatoid arthritis: 2022 update. Ann Rheum Dis. 2023. [PMID: 36526365]
- Aletaha D, et al. 2010 Rheumatoid Arthritis Classification Criteria. Arthritis & Rheumatism. 2010. [PMID: 20872358]
- Ytterberg SR, et al. Cardiovascular and Cancer Risk with Tofacitinib in RA (ORAL Surveillance). N Engl J Med. 2022. [PMID: 35081280]
- McInnes IB, Schett G. The Pathogenesis of Rheumatoid Arthritis. N Engl J Med. 2011. [PMID: 22150039]
- Grigor C, et al. Tight control of rheumatoid arthritis (TICORA). Lancet. 2004. [PMID: 15276390]
Last Updated: 2026-01-05 | MedVellum Editorial Team
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
Consequences
Complications and downstream problems to keep in mind.
- Secondary Amyloidosis
- Accelerated Atherosclerosis