TIA (Transient Ischaemic Attack) - Adult
Comprehensive evidence-based guide to transient ischaemic attack covering tissue-based definitions, ABCD2 risk stratification, urgent investigation protocols, dual antiplatelet therapy, carotid intervention, and...
What matters first
Comprehensive evidence-based guide to transient ischaemic attack covering tissue-based definitions, ABCD2 risk stratification, urgent investigation protocols, dual antiplatelet therapy, carotid intervention, and...
Check the red flags, emergency triggers, and escalation points before using the deep-dive material.
17 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Migraine with Aura
- Seizure Disorders
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
TIA (Transient Ischaemic Attack) - Adult
Quick Reference
Critical Alerts
⚠️ Red Flag: - TIA is a medical emergency - 10-15% risk of stroke within 90 days, with highest risk in first 48-72 hours [1,2]
- Tissue-based definition now standard - absence of infarction on DWI-MRI, not symptom duration [3]
- 30-40% of clinical "TIAs" show DWI lesions - these represent minor strokes with infarction [4]
- Start dual antiplatelet immediately - aspirin + clopidogrel loading reduces stroke by 30% [5,6]
- Urgent carotid imaging essential - CEA within 2 weeks for symptomatic ≥70% stenosis [7]
- EXPRESS study showed 80% risk reduction with urgent treatment vs standard care [8]
Key Diagnostics
| Investigation | Purpose | Timing |
|---|---|---|
| CT head (non-contrast) | Exclude haemorrhage | Immediate |
| MRI brain with DWI | Detect acute infarction | Within 24 hours |
| Carotid duplex ultrasound | Stenosis assessment | Within 24 hours |
| CTA/MRA head and neck | Vessel imaging | If stenosis detected |
| ECG | Atrial fibrillation | Immediate |
| Echocardiography (TTE/TEE) | Cardiac source | Within 7 days |
| Holter/prolonged monitoring | Paroxysmal AF | If cryptogenic |
Emergency Treatments
| Treatment | Dose | Evidence |
|---|---|---|
| Aspirin | 300 mg loading, then 75-100 mg daily | All TIA patients [5] |
| Clopidogrel | 300-600 mg loading, then 75 mg daily (21 days) | High-risk TIA (ABCD2 ≥4) [5,6] |
| High-intensity statin | Atorvastatin 80 mg or Rosuvastatin 20-40 mg | SPARCL trial [9] |
| Blood pressure | Target less than 130/80 mmHg (not acutely) | PROGRESS trial [10] |
| Carotid intervention | CEA/CAS within 2 weeks | Symptomatic ≥70% stenosis [7] |
Definition and Modern Concepts
Evolving Definition of TIA
The understanding of transient ischaemic attack has undergone a paradigm shift from a time-based to a tissue-based definition, fundamentally changing clinical approach and risk stratification. [3]
Classical Time-Based Definition (Historical) Transient episode of neurological dysfunction lasting less than 24 hours, presumed to be caused by focal brain, spinal cord, or retinal ischaemia.
Modern Tissue-Based Definition (Current Standard) Transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischaemia, without acute infarction on neuroimaging. [3]
Exam Detail: Why the Definition Changed
The 2009 AHA/ASA scientific statement redefined TIA based on several key observations: [3]
- Arbitrary 24-hour threshold: The 24-hour cutoff was arbitrary with no biological basis - most TIAs resolve within 60 minutes
- DWI-MRI sensitivity: 30-50% of patients with symptoms lasting less than 24 hours have evidence of infarction on DWI-MRI [4]
- Prognostic implications: Presence of DWI lesion indicates completed infarction regardless of symptom duration
- Treatment implications: Tissue injury defines stroke, not symptom duration
Clinical Implications of Tissue-Based Definition:
- MRI with DWI is the gold standard for distinguishing TIA from minor stroke
- "TIA" with positive DWI = minor ischaemic stroke (tissue injury present)
- "TIA" with negative DWI = true TIA (no tissue injury)
- Both require urgent evaluation and treatment
Terminology Clarification
| Term | Definition | DWI-MRI | Management |
|---|---|---|---|
| True TIA | Transient symptoms, no infarction | Negative | Urgent secondary prevention |
| Minor stroke | Transient/minimal symptoms, infarction present | Positive | Same as stroke (may qualify for thrombolysis) |
| Amaurosis fugax | Monocular vision loss (retinal TIA) | N/A | Urgent carotid imaging |
| Crescendo TIA | Multiple TIAs within 24-72 hours | Variable | Admission, expedited intervention |
Why TIA Matters: The Warning Stroke
TIA represents a critical window of opportunity for stroke prevention. The concept of "brain attack" emphasises the urgency comparable to myocardial infarction. [1,2]
Short-Term Stroke Risk After TIA:
| Time Period | Stroke Risk | With Urgent Treatment |
|---|---|---|
| 48 hours | 3-5% | less than 1% |
| 7 days | 5-10% | 1-2% |
| 30 days | 8-12% | 2-3% |
| 90 days | 10-17% | 3-5% |
The EXPRESS study (2007) demonstrated that urgent TIA clinic evaluation with immediate treatment initiation reduced 90-day stroke risk by 80% compared to standard care (10.3% vs 2.1%, p=0.0001). [8]
Epidemiology
Incidence and Prevalence
TIA incidence varies by population, diagnostic criteria, and healthcare access. The shift to tissue-based definitions has refined epidemiological understanding. [11]
| Parameter | Value | Population | Reference |
|---|---|---|---|
| Annual incidence (time-based) | 200-500 per 100,000 | United States | [11] |
| Annual incidence (tissue-based) | 100-300 per 100,000 | Europe | [11] |
| Estimated annual TIAs (US) | 240,000-500,000 | Population-based | [11] |
| Proportion preceding stroke | 15-30% of strokes | All ischaemic strokes | [2] |
| Age-specific incidence (> 85 years) | 1,000 per 100,000 | Elderly population | [11] |
Demographics
Age Distribution:
- Median age at TIA: 72 years
- Incidence doubles every decade after age 55
- Rare before age 45 (consider alternative diagnoses)
Sex Differences:
- Men: Higher incidence before age 75
- Women: Higher incidence after age 75
- Similar overall lifetime risk
Ethnic Variations:
- African Americans: 38% higher risk than Caucasians
- Hispanic populations: Intermediate risk
- Asian populations: Higher proportion of intracranial disease
Temporal Patterns
- Peak incidence: 8:00-11:00 AM (morning surge)
- Seasonal variation: Higher in winter months
- Circadian rhythm correlates with blood pressure and platelet activation
Pathophysiology
Mechanism of Transient Ischaemia
TIA results from temporary interruption of cerebral blood flow insufficient to cause permanent tissue injury. The pathophysiological mechanisms mirror those of ischaemic stroke. [3]
Transient Vascular Occlusion (embolic or thrombotic)
↓
Focal Cerebral Hypoperfusion
↓
Ischaemic Penumbra Development
↓
Neurological Symptoms Manifest
↓
Spontaneous Reperfusion/Collateral Recruitment
↓
Symptoms Resolve (No Infarction)
Exam Detail: Ischaemic Cascade (Molecular Level)
The transient nature of TIA involves incomplete activation of the ischaemic cascade:
- Energy failure (seconds): ATP depletion, ionic pump failure
- Glutamate excitotoxicity (minutes): NMDA receptor activation
- Calcium influx: Intracellular Ca²⁺ accumulation
- Oxidative stress: Reactive oxygen species generation
- Mitochondrial dysfunction: Cytochrome c release
Why No Permanent Injury?
- Rapid reperfusion (less than 60 minutes typically)
- Collateral circulation activation
- Ischaemic penumbra salvaged
- Incomplete cascade activation
- Ischaemic preconditioning in some patients
Penumbra Concept: The ischaemic penumbra represents tissue at risk surrounding the ischaemic core. In TIA, the entire affected territory functions as salvaged penumbra due to timely reperfusion.
Aetiological Classification (TOAST/Oxford)
Understanding the underlying mechanism guides secondary prevention strategy. [12]
| Mechanism | Proportion | Description | Key Features |
|---|---|---|---|
| Large artery atherosclerosis | 20-30% | Carotid or intracranial stenosis | Amaurosis fugax, stuttering onset |
| Cardioembolism | 20-30% | AF, valvular disease, cardiomyopathy | Sudden onset, maximal at onset |
| Small vessel disease (lacunar) | 15-25% | Lipohyalinosis, microatheroma | Pure motor/sensory syndromes |
| Other determined causes | 5-10% | Dissection, vasculitis, hypercoagulable | Young patients, unusual history |
| Cryptogenic | 20-30% | Unknown despite full workup | May include occult AF |
Exam Detail: Large Artery Atherosclerosis - Mechanism Details
Carotid stenosis causes TIA through three main mechanisms:
-
Artery-to-artery embolism (most common)
- Unstable plaque with thrombus formation
- Platelet-fibrin emboli to distal vessels
- Often ulcerated or irregular plaque
-
Haemodynamic compromise
- Critical stenosis (> 90%) with flow limitation
- Watershed territory symptoms
- Postural symptoms possible
-
In-situ thrombosis
- Acute plaque rupture with thrombotic occlusion
- Transient before spontaneous lysis
Cardioembolic Sources (High-Risk):
- Atrial fibrillation (accounts for 50% of cardioembolic strokes)
- Left ventricular thrombus
- Mechanical heart valves
- Infective endocarditis
- Left atrial appendage thrombus
- Dilated cardiomyopathy (EF less than 35%)
Cardioembolic Sources (Medium-Risk):
- Patent foramen ovale (controversial)
- Atrial septal aneurysm
- Aortic arch atheroma (> 4 mm)
- Mitral valve prolapse
- Mitral annular calcification
Risk Factors
| Non-Modifiable | Modifiable | Lifestyle |
|---|---|---|
| Age (> 55 years) | Hypertension (RR 2-4) | Smoking (RR 2) |
| Male sex | Diabetes mellitus (RR 2-4) | Physical inactivity |
| Race (African descent) | Dyslipidaemia | Obesity |
| Family history of stroke | Atrial fibrillation (RR 5) | Excessive alcohol |
| Prior stroke/TIA | Carotid stenosis | Poor diet |
| Genetic factors | Hyperhomocysteinaemia | Illicit drug use |
Population Attributable Risk (Key Statistics): [13]
- Hypertension: 35% of stroke risk attributable
- Smoking: 19% of stroke risk attributable
- Obesity: 19% of stroke risk attributable
- Physical inactivity: 36% of stroke risk attributable
- Diet: 23% of stroke risk attributable
Clinical Presentation
Symptom Patterns by Vascular Territory
Clinical presentation depends on the arterial territory affected. Recognition of vascular patterns aids diagnosis and guides imaging.
Anterior Circulation (Carotid Territory)
| Syndrome | Arterial Territory | Symptoms |
|---|---|---|
| Amaurosis fugax | Ophthalmic artery (ICA branch) | Monocular vision loss "curtain descending" |
| MCA cortical | Middle cerebral artery | Hemiparesis (face/arm > leg), hemisensory loss, aphasia (left), neglect (right) |
| ACA territory | Anterior cerebral artery | Leg weakness > arm, personality change |
| Watershed | ICA/MCA border zone | Proximal arm/leg weakness, "man-in-barrel" |
Posterior Circulation (Vertebrobasilar Territory)
| Syndrome | Arterial Territory | Symptoms |
|---|---|---|
| Brainstem | Basilar artery/branches | Vertigo + diplopia/dysarthria/dysphagia, crossed deficits |
| Cerebellar | PICA/AICA/SCA | Ataxia, vertigo, nystagmus |
| Occipital | PCA | Homonymous hemianopia, visual disturbance |
| Thalamic | Posterior thalamic | Hemisensory loss, pain, behavioural change |
Clinical Pearl: Isolated Vertigo - Is It TIA?
Isolated vertigo is rarely due to posterior circulation TIA. Suspect TIA only when vertigo is accompanied by other posterior circulation symptoms:
- Diplopia
- Dysarthria
- Dysphagia
- Ataxia
- Crossed sensory/motor findings
Use the HINTS exam to differentiate peripheral from central vertigo:
- Head Impulse test (normal = central)
- Nystagmus type (direction-changing = central)
- Test of Skew (skew deviation = central)
A benign HINTS pattern has higher sensitivity for ruling out stroke than early MRI (98% vs 80%).
Duration and Timing
| Duration | DWI-MRI Positive Rate | Implication |
|---|---|---|
| less than 10 minutes | 15-20% | Lower risk, but still requires workup |
| 10-60 minutes | 25-35% | Typical TIA duration |
| 1-6 hours | 40-50% | High likelihood of tissue injury |
| 6-24 hours | 60-70% | Likely minor stroke |
| > 24 hours | > 80% | Stroke by any definition |
Key Point: Most true TIAs last 10-15 minutes. Symptoms lasting > 1 hour significantly increase probability of DWI lesion (infarction). [4]
TIA Mimics (Differential Diagnosis)
Up to 60% of patients referred with suspected TIA have alternative diagnoses. [14]
| Mimic | Distinguishing Features | Key Differentiator |
|---|---|---|
| Migraine with aura | Positive visual symptoms (scintillations), gradual spread over 5-20 minutes, headache follows | Spreading positive phenomena |
| Focal seizure/postictal paralysis | Motor activity, LOC, gradual resolution over hours | Witnessed convulsion, Todd's paralysis |
| Hypoglycaemia | Confusion, sweating, tremor, responds to glucose | Check blood glucose |
| Peripheral vestibular disorder | Isolated vertigo, positive Dix-Hallpike, benign HINTS | No other brainstem symptoms |
| Syncope/presyncope | Loss of consciousness, no focal deficit, prodrome | Global symptoms, not focal |
| Transient global amnesia | Isolated amnesia, repetitive questioning, no focal signs | Preserved identity, resolves less than 24h |
| Anxiety/hyperventilation | Perioral/bilateral tingling, breathlessness | Non-vascular distribution |
| Functional neurological disorder | Inconsistent examination, distractible | Does not fit vascular territory |
| MS relapse | Age less than 50, prior episodes, progressive | Days not minutes |
| Cerebral amyloid angiopathy | Transient focal neurological episodes, haemorrhage on imaging | Superficial siderosis on MRI |
| Subdural haematoma | Trauma history, elderly, fluctuating | Chronic symptoms, imaging |
Physical Examination
Often Normal by Presentation
The examination is frequently unremarkable as symptoms have resolved. However, examine for:
| Finding | Clinical Significance | Next Step |
|---|---|---|
| Residual focal deficit | May represent minor stroke, not TIA | MRI with DWI urgently |
| Carotid bruit | 25% sensitivity for > 70% stenosis | Carotid imaging regardless |
| Irregular pulse | Atrial fibrillation | ECG, anticoagulation |
| Cardiac murmur | Valvular source | Echocardiography |
| Retinal emboli (Hollenhorst plaques) | Carotid atherosclerosis | Urgent carotid imaging |
| Blood pressure differential | Subclavian steal/dissection | Bilateral BP measurement |
| Xanthelasma, arcus | Dyslipidaemia | Lipid panel |
Red Flags and High-Risk Features
Immediate High-Risk Indicators
⚠️ Red Flag: | Red Flag | Clinical Concern | Immediate Action | |----------|-----------------|------------------| | Ongoing symptoms | Active stroke | Stroke protocol, consider thrombolysis | | Crescendo TIAs (≥2 in 24h) | Unstable plaque, imminent stroke | Admission, expedited carotid imaging | | ABCD2 score ≥4 | 4% 48-hour stroke risk | Consider admission | | Known carotid stenosis ≥50% | Symptomatic stenosis, treatable | Urgent surgery evaluation | | Atrial fibrillation | Cardioembolic source | Anticoagulation | | Recent carotid intervention | Restenosis, hyperperfusion | Urgent imaging | | Amaurosis fugax + carotid bruit | High-grade carotid disease | Urgent CEA evaluation | | DWI lesion on MRI | Minor stroke (not TIA) | Higher recurrence risk | | Large artery stenosis/occlusion | Haemodynamic or embolic | Consider intervention |
Crescendo TIA - A Stroke Emergency
Crescendo TIA describes multiple TIAs occurring over hours to days, indicating:
- Unstable atherosclerotic plaque
- Critical stenosis with flow limitation
- High-risk cardioembolic source
- Imminent stroke
Management:
- Hospital admission mandatory
- Continuous telemetry monitoring
- Expedited carotid imaging (same day)
- Consider dual antiplatelet therapy
- Early surgical consultation if carotid disease
- BP permissive (avoid hypotension)
Risk Stratification
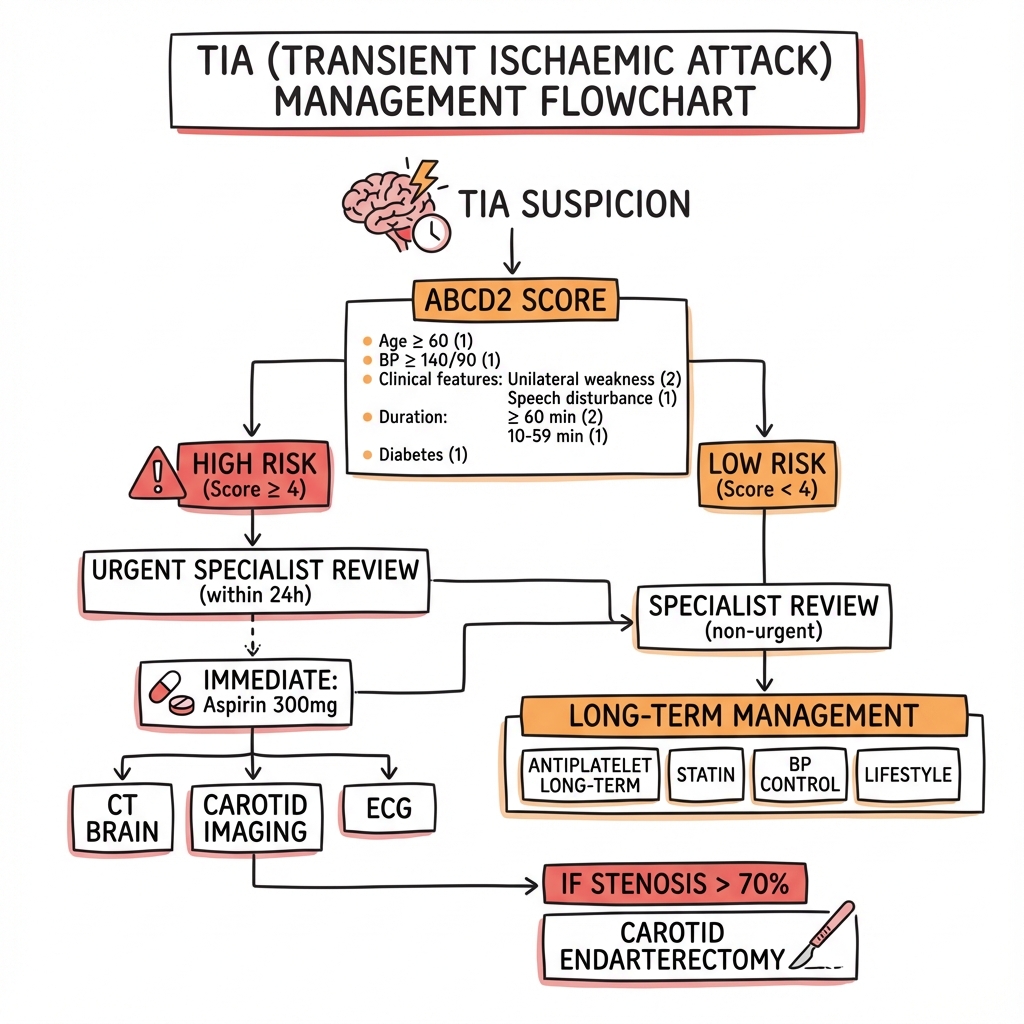
ABCD2 Score
The ABCD2 score stratifies short-term stroke risk after TIA. Despite limitations, it remains widely used for disposition decisions. [15]
| Factor | Finding | Points |
|---|---|---|
| Age | ≥60 years | 1 |
| Blood pressure | SBP ≥140 mmHg OR DBP ≥90 mmHg | 1 |
| Clinical features | Unilateral weakness | 2 |
| Speech disturbance without weakness | 1 | |
| Duration | ≥60 minutes | 2 |
| 10-59 minutes | 1 | |
| Diabetes | Present | 1 |
| Total | 0-7 |
Risk Stratification by ABCD2 Score:
| Score | 2-Day Risk | 7-Day Risk | 90-Day Risk | Risk Category |
|---|---|---|---|---|
| 0-3 | 1.0% | 1.2% | 3.1% | Low |
| 4-5 | 4.1% | 5.9% | 9.8% | Moderate |
| 6-7 | 8.1% | 11.7% | 17.8% | High |
Exam Detail: Limitations of ABCD2 Score
The ABCD2 score has significant limitations that should be recognised: [15]
- Does not include imaging findings - DWI lesion and carotid stenosis independently predict stroke
- Lower scores do not exclude high-risk aetiology - AF or critical stenosis may have ABCD2 = 2
- Variable performance - Validation studies show AUC 0.62-0.72
- Does not differentiate TIA mimics - May "score" non-vascular causes
Enhanced Risk Scores:
ABCD2-I (adds imaging):
- Add 2 points for DWI lesion
- Add 2 points for carotid stenosis ≥50%
ABCD3-I (adds dual TIA):
- Add 2 points for dual TIA (≥2 in 7 days)
- Add 2 points for DWI lesion
- Add 2 points for ≥50% stenosis
These modified scores improve discrimination (AUC 0.74-0.82) but are less widely implemented.
Clinical Decision Rules for Disposition
Consider Admission If:
- ABCD2 score ≥4
- Crescendo TIAs
- Symptomatic carotid stenosis ≥50%
- Known or newly detected atrial fibrillation
- Positive DWI on MRI
- Unable to complete urgent outpatient workup within 24-48 hours
- Residual neurological deficit
- Unreliable patient or poor social circumstances
- Unable to return rapidly if symptoms recur
Outpatient TIA Clinic Appropriate If:
- ABCD2 score 0-3
- No high-risk features above
- Brain imaging and carotid imaging completed or arranged within 24 hours
- Antiplatelet therapy initiated
- Reliable patient with ability to return
- Close follow-up arranged (within 24-48 hours)
Diagnostic Approach
Structured Investigation Algorithm
Phase 1: Immediate (Emergency Department)
| Investigation | Purpose | Target Timing |
|---|---|---|
| Blood glucose | Exclude hypoglycaemia | Immediate |
| 12-lead ECG | Detect atrial fibrillation | Immediate |
| CT head (non-contrast) | Exclude haemorrhage, mass | Immediate |
| FBC, U&E, coagulation | Baseline, pre-treatment | Immediate |
Phase 2: Urgent (Within 24 Hours)
| Investigation | Purpose | Key Findings |
|---|---|---|
| MRI brain with DWI/FLAIR | Detect acute infarction | DWI restriction = infarct |
| Carotid duplex ultrasound | Stenosis assessment | ≥50% stenosis actionable |
| Lipid panel, HbA1c | Risk factor assessment | Guide therapy |
| TTE echocardiography | Cardiac source | LV thrombus, valve disease |
Phase 3: Extended (Within 7-14 Days)
| Investigation | Indication | Purpose |
|---|---|---|
| CTA/MRA head and neck | Stenosis confirmed or suspected | Surgical planning |
| TEE (transoesophageal echo) | Suspected cardioembolic, PFO | LA appendage, aortic arch |
| Holter monitor (24-72 hours) | Cryptogenic, suspected paroxysmal AF | Occult AF detection |
| Extended cardiac monitoring | Cryptogenic TIA | Up to 30% AF detection rate |
| Thrombophilia screen | Young patient, unprovoked | Hypercoagulable states |
| Vasculitis screen | Young, systemic features | ESR, CRP, ANA, ANCA |
Neuroimaging
CT Head
- First-line to exclude haemorrhage
- Low sensitivity for acute ischaemia (10-20%)
- May show old infarcts, tumours, other pathology
- Cannot distinguish TIA from minor stroke
MRI Brain with DWI (Gold Standard) [4]
- Detects acute ischaemia within minutes of onset
- Sensitivity 80-90% for acute infarction
- 30-50% of "clinical TIAs" have DWI lesion (= minor stroke)
- Informs prognosis: DWI+ patients have 3-4x higher recurrence risk
- Should be performed within 24 hours when possible
Clinical Pearl: DWI-MRI Interpretation Pearls
- DWI bright + ADC dark = acute ischaemia (cytotoxic oedema)
- DWI bright + ADC bright = T2 shine-through (not acute)
- Small DWI lesions may not have corresponding ADC change
- Posterior fossa lesions harder to detect (susceptibility artifact)
- False negatives occur in first 6 hours and for very small lesions
- Serial MRI can detect new lesions indicating ongoing embolism
Carotid Imaging
Carotid stenosis is the most treatable cause of TIA. All patients require carotid assessment.
| Modality | Advantages | Limitations |
|---|---|---|
| Carotid duplex ultrasound | Non-invasive, no radiation, first-line | Operator-dependent, calcification artifact |
| CT angiography (CTA) | Rapid, good for calcified plaque, surgical planning | Contrast, radiation |
| MR angiography (MRA) | No radiation, shows plaque composition | Overestimates stenosis, claustrophobia |
| Digital subtraction angiography | Gold standard (historical) | Invasive, 1% stroke risk, rarely needed |
NASCET vs ECST Measurement Methods:
- NASCET: Stenosis relative to normal distal ICA (most commonly used)
- ECST: Stenosis relative to estimated original lumen
- Conversion: ECST 70% ≈ NASCET 50%; ECST 85% ≈ NASCET 70%
Cardiac Evaluation
ECG Findings:
| Finding | Significance | Action |
|---|---|---|
| Atrial fibrillation | Cardioembolic source (5-10% new diagnosis) | Anticoagulation |
| Left ventricular hypertrophy | Hypertensive heart disease | BP optimisation |
| Q waves | Prior MI, LV thrombus risk | Echo for thrombus |
| Prolonged QTc | Electrolyte abnormality | Check K+, Mg2+ |
Echocardiography Indications:
- All TIA patients (TTE as minimum)
- TEE if: suspected cardioembolic, young patient, cryptogenic TIA, PFO evaluation
- Bubble study (agitated saline contrast) for PFO detection
Extended Cardiac Monitoring for Occult AF: [16]
| Duration | AF Detection Rate | Use Case |
|---|---|---|
| 24-hour Holter | 2-5% | Minimum standard |
| 7-day continuous | 10-15% | Cryptogenic TIA |
| 30-day event recorder | 15-25% | Cryptogenic TIA |
| Implantable loop recorder | 25-30% at 3 years | Highly selected cryptogenic |
The CRYSTAL-AF trial demonstrated that implantable cardiac monitors detected AF in 30% of cryptogenic stroke/TIA patients over 3 years, compared to 3% with standard monitoring. [16]
Laboratory Investigations
| Test | Purpose | Target |
|---|---|---|
| Glucose (fasting) | Diabetes screening | less than 7.0 mmol/L |
| HbA1c | Glycaemic control | less than 48 mmol/mol (less than 6.5%) |
| Lipid panel | Dyslipidaemia | LDL less than 1.8 mmol/L |
| FBC | Polycythaemia, thrombocytosis | Normal ranges |
| U&E, creatinine | Renal function for medications | eGFR > 30 for DOACs |
| Coagulation (PT/INR, APTT) | Baseline, anticoagulation planning | Normal |
| TSH | Thyroid dysfunction (AF risk) | Normal |
| ESR, CRP | Vasculitis screen if indicated | Normal |
Extended Investigations (Selected Patients):
- Thrombophilia screen: Young, unprovoked, family history
- Vasculitis screen: Systemic symptoms, young patient
- Lumbar puncture: Suspected CNS vasculitis, infection
- Toxicology: Young patient, cocaine/amphetamine use
Treatment
Immediate Antiplatelet Therapy
Antiplatelet therapy is the cornerstone of TIA management and should be initiated immediately in the emergency department unless contraindicated. [5,6]
Single Antiplatelet Therapy (All TIA Patients)
| Agent | Loading Dose | Maintenance | Evidence |
|---|---|---|---|
| Aspirin | 300 mg stat | 75-100 mg daily | Foundation of therapy |
| Clopidogrel | 300 mg stat | 75 mg daily | Alternative to aspirin |
Dual Antiplatelet Therapy (DAPT) - High-Risk TIA [5,6]
The CHANCE and POINT trials established dual antiplatelet therapy as standard for high-risk TIA:
| Trial | Regimen | Duration | Stroke Reduction | Bleeding Risk |
|---|---|---|---|---|
| CHANCE (2013) | Aspirin + Clopidogrel | 21 days | 32% RRR | No increase |
| POINT (2018) | Aspirin + Clopidogrel | 90 days | 25% RRR | 2.3x major bleeding |
Exam Detail: CHANCE Trial (Clopidogrel in High-Risk Patients with Acute Non-disabling Cerebrovascular Events) [6]
- Population: 5,170 Chinese patients with TIA (ABCD2 ≥4) or minor stroke (NIHSS ≤3)
- Intervention: Aspirin 75 mg + Clopidogrel 75 mg (after 300 mg load) vs Aspirin 75 mg alone
- Duration: 21 days of DAPT
- Primary Outcome: Stroke at 90 days: 8.2% vs 11.7% (HR 0.68, pless than 0.001)
- Bleeding: No significant difference in major haemorrhage
- Conclusion: Short-term DAPT superior to aspirin alone in Chinese population
POINT Trial (Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke) [5]
- Population: 4,881 international patients with TIA (ABCD2 ≥4) or minor stroke (NIHSS ≤3)
- Intervention: Aspirin 50-325 mg + Clopidogrel 600 mg load then 75 mg vs Aspirin alone
- Duration: 90 days of DAPT
- Primary Outcome: Major ischaemic events: 5.0% vs 6.5% (HR 0.75, p=0.02)
- Bleeding: Major haemorrhage: 0.9% vs 0.4% (HR 2.32, p=0.02)
- Conclusion: Benefit primarily in first 21 days; bleeding risk increases with duration
Synthesis - Current Practice:
- DAPT for 21 days is optimal balance of efficacy and safety
- Start within 12-24 hours of symptom onset
- After 21 days, continue single antiplatelet (aspirin or clopidogrel)
- DAPT reduces stroke by ~30% but increases major bleeding modestly
Current DAPT Recommendations:
| Patient Group | Regimen | Duration |
|---|---|---|
| High-risk TIA (ABCD2 ≥4) | Aspirin 75-100 mg + Clopidogrel 75 mg (after loading) | 21 days |
| Minor stroke (NIHSS ≤3) | Aspirin 75-100 mg + Clopidogrel 75 mg (after loading) | 21 days |
| After 21 days | Monotherapy (clopidogrel preferred or aspirin) | Long-term |
Contraindications to Antiplatelet Therapy:
- Active significant bleeding
- Severe thrombocytopenia
- Known hypersensitivity
- Planned urgent surgery
- Anticoagulation indication (AF - switch to anticoagulant)
Statin Therapy
High-intensity statin therapy is recommended for all patients with TIA of presumed atherosclerotic origin. [9]
SPARCL Trial (Stroke Prevention by Aggressive Reduction in Cholesterol Levels) [9]
- Atorvastatin 80 mg vs placebo in stroke/TIA patients
- 16% reduction in recurrent stroke (HR 0.84)
- 35% reduction in major cardiovascular events
- Benefit independent of baseline LDL
| Statin | Dose | LDL Reduction |
|---|---|---|
| Atorvastatin | 80 mg daily | 50-60% |
| Rosuvastatin | 20-40 mg daily | 55-65% |
| Simvastatin | 40 mg daily | 35-45% |
Targets:
- LDL cholesterol: less than 1.8 mmol/L (70 mg/dL) for very high-risk
-
50% reduction from baseline if target not achievable
- Consider PCSK9 inhibitors if target not achieved on maximum statin
Blood Pressure Management
Hypertension is the most important modifiable risk factor for stroke. Management differs in acute versus chronic phases. [10]
Acute Phase (First 24-48 Hours):
- Permissive hypertension (avoid lowering unless extreme)
- Do not treat unless BP > 220/120 mmHg
- Rationale: Maintain cerebral perfusion through collaterals
- Exception: If thrombolysis candidate (different thresholds apply)
Chronic Secondary Prevention:
| Trial | Intervention | Stroke Reduction |
|---|---|---|
| PROGRESS (2001) | Perindopril ± Indapamide | 28% RRR |
| HOPE (2000) | Ramipril | 32% RRR |
| SPS3 (2013) | less than 130 vs less than 150 mmHg target | 19% RRR (non-significant) |
Current Targets: [10]
- General target: less than 130/80 mmHg
- Severe bilateral carotid stenosis: More liberal (individual assessment)
- Elderly (> 80 years): less than 140/90 mmHg may be acceptable
Preferred Agents:
- ACE inhibitors (perindopril has best evidence)
- Thiazide diuretics (indapamide)
- Calcium channel blockers
- Combination therapy usually required
Carotid Revascularisation
Carotid endarterectomy (CEA) is highly effective for preventing stroke in symptomatic carotid stenosis. Timing and patient selection are critical. [7,17]
Indications for Carotid Endarterectomy:
| Stenosis Grade | Recommendation | NNT |
|---|---|---|
| ≥70% (NASCET) | Strong indication - operate within 2 weeks | 6 |
| 50-69% | Moderate indication - weigh risks/benefits | 22 |
| less than 50% | No benefit from surgery | - |
Exam Detail: Landmark Carotid Surgery Trials
NASCET (North American Symptomatic Carotid Endarterectomy Trial) [7]
- 2,226 patients with symptomatic carotid stenosis
- For 70-99% stenosis: 2-year ipsilateral stroke risk 9% vs 26% (CEA vs medical)
- Absolute risk reduction: 17% (NNT = 6)
- For 50-69% stenosis: Modest benefit (ARR 6.5% at 5 years)
ECST (European Carotid Surgery Trial) [17]
- Similar findings to NASCET
- Confirmed benefit for severe stenosis
- Different measurement methodology
Key Surgical Principles:
- Timing: Operate within 2 weeks of TIA (greatest benefit)
- Delay reduces benefit: 14% reduction in benefit per week of delay
- Surgical risk: less than 6% perioperative stroke/death rate required for net benefit
- No benefit for less than 50% stenosis: Medical therapy alone
Carotid Artery Stenting (CAS) vs CEA:
| Factor | CEA Preferred | CAS Preferred |
|---|---|---|
| Age | > 70 years | less than 70 years |
| Anatomy | Standard | High lesion, prior neck surgery/radiation |
| Comorbidities | Low surgical risk | High surgical risk (cardiac, pulmonary) |
| Perioperative risk | Lower stroke risk | Lower MI risk |
The CREST trial showed equivalent long-term outcomes for CEA and CAS, but differing short-term risk profiles:
- CEA: Higher MI risk (2.3% vs 1.1%)
- CAS: Higher stroke risk (4.1% vs 2.3%)
Contraindications to Carotid Surgery:
- Chronic total occlusion
- Severe disability from prior stroke
- Limited life expectancy
- High surgical risk with low-grade stenosis
Anticoagulation for Atrial Fibrillation
If atrial fibrillation is detected, anticoagulation replaces antiplatelet therapy for secondary prevention. [18]
Timing of Anticoagulation After TIA:
- TIA with no infarction on imaging: Start immediately (1-3 days)
- Minor stroke (small infarct): Start at 3-5 days
- Moderate stroke: Start at 5-7 days
- Large stroke: Start at 7-14 days (haemorrhagic transformation risk)
CHA₂DS₂-VASc Score:
| Factor | Points |
|---|---|
| Congestive heart failure | 1 |
| Hypertension | 1 |
| Age ≥75 years | 2 |
| Diabetes mellitus | 1 |
| Stroke/TIA/thromboembolism | 2 |
| Vascular disease | 1 |
| Age 65-74 years | 1 |
| Sex category (female) | 1 |
- Score ≥2 (male) or ≥3 (female): Anticoagulation recommended
- TIA/stroke adds 2 points → virtually all TIA patients with AF require anticoagulation
Anticoagulant Options: [18]
| Agent | Dose (Standard) | Advantages | Considerations |
|---|---|---|---|
| Apixaban | 5 mg BD | Lowest bleeding risk | Preferred in elderly |
| Rivaroxaban | 20 mg OD | Once daily dosing | Take with food |
| Dabigatran | 150 mg BD | Reversible (idarucizumab) | GI side effects |
| Edoxaban | 60 mg OD | Once daily, renal dosing | CrCl 15-95 mL/min |
| Warfarin | Target INR 2-3 | Mechanical valves, severe renal impairment | Requires monitoring |
DOACs vs Warfarin Post-Stroke/TIA:
- DOACs have lower intracranial bleeding risk
- Similar or better efficacy for stroke prevention
- No routine monitoring required
- Preferred for non-valvular AF
Lifestyle Modifications
Comprehensive lifestyle intervention is essential for secondary prevention.
| Intervention | Target | Evidence |
|---|---|---|
| Smoking cessation | Complete cessation | 50% risk reduction |
| Diet | Mediterranean diet | 30% RRR (PREDIMED) |
| Physical activity | 150 min/week moderate | 25-30% risk reduction |
| Alcohol | ≤14 units/week | J-shaped curve |
| Weight | BMI 18.5-25 kg/m² | Reduces multiple risk factors |
| Sodium | less than 2 g/day | BP reduction |
Disposition and Follow-Up
Emergency Department Disposition
Admission Criteria:
- ABCD2 score ≥4 and unable to complete urgent outpatient workup
- Crescendo TIAs
- Symptomatic carotid stenosis ≥50% confirmed
- Newly detected atrial fibrillation requiring anticoagulation initiation
- Positive DWI on MRI (minor stroke)
- Residual neurological deficit
- Unable to obtain timely outpatient imaging
- Unreliable patient or poor social circumstances
- Patient unable to return quickly if symptoms recur
Discharge with Urgent Outpatient Follow-Up:
- Low-risk TIA (ABCD2 0-3) with no high-risk features
- Brain imaging completed or arranged within 24 hours
- Carotid imaging completed or arranged within 24 hours
- Antiplatelet therapy initiated
- Statin therapy initiated
- Reliable patient with ability to return
- Clear return precautions provided
- Follow-up arranged within 24-48 hours
Discharge Checklist
| Item | Completed |
|---|---|
| Antiplatelet therapy prescribed (aspirin ± clopidogrel) | ☐ |
| Statin therapy prescribed | ☐ |
| Brain imaging completed or arranged | ☐ |
| Carotid imaging completed or arranged | ☐ |
| ECG performed | ☐ |
| Cardiac monitoring plan (if cryptogenic) | ☐ |
| Risk factor management discussed | ☐ |
| FAST stroke recognition taught | ☐ |
| Clear return precautions given | ☐ |
| Follow-up appointment scheduled | ☐ |
| Driving restrictions discussed | ☐ |
Follow-Up Schedule
| Timeframe | Purpose | Actions |
|---|---|---|
| 24-72 hours | Complete imaging, neurology review | MRI, carotid imaging, echo |
| 2 weeks | Carotid surgery assessment | CEA/CAS if indicated |
| 1 month | Medication review, risk factor control | BP, lipids, glucose assessment |
| 3 months | Secondary prevention optimisation | Adherence, side effects, targets |
| 6-12 months | Long-term prevention | Ongoing monitoring |
Driving Regulations (UK DVLA)
| Licence Type | Group 1 (Car/Motorcycle) | Group 2 (HGV/Bus) |
|---|---|---|
| TIA (single) | 1 month off driving | 1 year off driving |
| Multiple TIAs | 3 months off driving | 5 years off driving |
| TIA + carotid surgery | 1 month off driving | 1 year off driving |
Special Populations
Young Adults (less than 45 Years)
Unusual causes are more prevalent in young patients:
| Cause | Clinical Features | Investigation |
|---|---|---|
| Arterial dissection | Neck pain, Horner's syndrome, trauma | MRA/CTA neck |
| Patent foramen ovale | Valsalva manoeuvre precipitant | Bubble echo |
| Antiphospholipid syndrome | Recurrent thromboses, pregnancy loss | Lupus anticoagulant, anticardiolipin |
| Inherited thrombophilia | Family history, unprovoked events | Thrombophilia screen |
| Illicit drug use | Cocaine, amphetamines | Toxicology screen |
| Vasculitis | Systemic symptoms | ESR, CRP, ANA, ANCA |
| Mitochondrial disease | MELAS, migrainous features | Genetic testing |
Investigation Approach:
- Standard TIA workup PLUS:
- MRA/CTA including vessel wall imaging
- TEE with bubble study (PFO evaluation)
- Thrombophilia screen
- Vasculitis screen if indicated
- Consider lumbar puncture if CNS vasculitis suspected
Elderly (> 80 Years)
| Consideration | Approach |
|---|---|
| Increased stroke risk | More aggressive treatment beneficial |
| Polypharmacy | Review drug interactions |
| Falls risk | Balance bleeding vs stroke risk |
| Anticoagulation | DOACs generally safer than warfarin |
| Carotid surgery | Benefit maintained if fit for surgery |
| Life expectancy | Consider in intervention decisions |
| Cognitive impairment | May affect adherence |
Pregnancy
TIA in pregnancy requires specialist multidisciplinary management:
| Aspect | Consideration |
|---|---|
| Aetiology | Pre-eclampsia, HELLP, paradoxical embolism, CVST |
| Imaging | MRI preferred (no radiation); avoid gadolinium in first trimester |
| Antiplatelet | Low-dose aspirin safe; clopidogrel limited data |
| Anticoagulation | LMWH for cardioembolic; DOACs contraindicated |
| BP management | Labetalol, nifedipine, methyldopa |
| Delivery | Multidisciplinary planning; timing depends on aetiology |
Cryptogenic TIA
When standard workup is negative, extended evaluation may reveal occult causes:
ESUS (Embolic Stroke of Undetermined Source) Approach:
- Prolonged cardiac monitoring (≥30 days)
- TEE for aortic arch atheroma and PFO
- Consider implantable loop recorder
- PFO closure in selected patients (less than 60 years, high-risk PFO features)
Prognosis
Short-Term Outcomes
| Outcome | Risk (Without Treatment) | Risk (With Urgent Treatment) |
|---|---|---|
| Stroke at 48 hours | 3-5% | less than 1% |
| Stroke at 7 days | 5-10% | 1-2% |
| Stroke at 90 days | 10-17% | 3-5% |
Long-Term Outcomes
| Outcome | 5-Year Risk |
|---|---|
| Recurrent stroke | 15-25% |
| Myocardial infarction | 10-15% |
| Vascular death | 10-20% |
| All-cause mortality | 20-30% |
Prognostic Factors
Poor Prognosis:
- High ABCD2 score
- DWI lesion on MRI
- Carotid stenosis ≥50%
- Atrial fibrillation
- Multiple TIAs
- Diabetes mellitus
- Persistent risk factors
Good Prognosis:
- Single brief TIA
- Prompt treatment initiation
- Negative DWI-MRI
- No carotid disease
- Excellent risk factor control
- High adherence to medications
Patient Education
Understanding TIA
Key messages for patients:
- TIA is a "warning stroke"
- brain ischaemia without permanent damage
- The risk of a complete stroke is highest in the next few days
- Urgent treatment and evaluation significantly reduces stroke risk
- Medication adherence and lifestyle changes are essential
- Know the signs of stroke and call emergency services immediately
FAST Stroke Recognition
| Letter | Meaning | Action |
|---|---|---|
| F | Face drooping | Ask to smile - is one side drooping? |
| A | Arm weakness | Raise both arms - does one drift down? |
| S | Speech difficulty | Repeat a sentence - is speech slurred? |
| T | Time to call emergency services | If any positive - call 999/911 immediately |
Medication Adherence
| Medication | Purpose | Duration | Key Points |
|---|---|---|---|
| Aspirin | Prevents blood clots | Lifelong | Take with food |
| Clopidogrel | Prevents blood clots (DAPT) | 21 days then review | Do not stop suddenly |
| Statin | Lowers cholesterol, stabilises plaque | Lifelong | Take at night (some) |
| BP medication | Reduces blood pressure | Lifelong | Do not miss doses |
Lifestyle Modification Counselling
| Topic | Recommendation | Impact |
|---|---|---|
| Smoking | Stop completely; offer support and pharmacotherapy | Halves risk |
| Diet | Mediterranean diet; reduce salt, processed foods | 30% risk reduction |
| Exercise | 150 minutes moderate activity per week | 25% risk reduction |
| Alcohol | Maximum 14 units per week | Reduces BP and risk |
| Weight | Achieve BMI 18.5-25 kg/m² | Reduces multiple risks |
Return Precautions
Return to Emergency Department Immediately If:
- Any new weakness, numbness, or paralysis
- New speech difficulty (slurred or confused)
- New vision changes
- Severe sudden headache
- Symptoms similar to your TIA that return
- Any symptoms lasting more than a few minutes
Viva Preparation
Common Viva Questions
Viva Point: Q: A 68-year-old man presents with resolved right arm weakness lasting 20 minutes. How would you approach this?
Opening Statement: "This presentation is concerning for a transient ischaemic attack, which represents a medical emergency given the high short-term stroke risk. My approach would be systematic, focusing on confirming the diagnosis, risk stratifying, initiating immediate treatment, and arranging urgent investigation."
Structured Answer:
- Immediate assessment: ABC, glucose, full neurological examination
- Confirm TIA: Symptoms consistent with vascular territory, resolved completely
- Risk stratify: Calculate ABCD2 score (age ≥60 = 1, BP ≥140/90 = 1, unilateral weakness = 2, duration 10-59 min = 1, diabetes = check) = likely 4-5 (moderate-high risk)
- Immediate treatment: Aspirin 300 mg stat, consider dual antiplatelet if ABCD2 ≥4
- Investigations: CT head, ECG, bloods (glucose, lipids, HbA1c), arrange urgent MRI and carotid imaging
- Disposition: Consider admission given high-risk score; alternatively, urgent TIA clinic within 24 hours if imaging arranged
Viva Point: Q: What is the evidence for dual antiplatelet therapy in TIA?
Key Evidence: "Two landmark trials established dual antiplatelet therapy for high-risk TIA:
-
CHANCE trial (2013): Chinese population, aspirin plus clopidogrel for 21 days reduced 90-day stroke from 11.7% to 8.2% (32% relative risk reduction) with no increase in major bleeding.
-
POINT trial (2018): International population, aspirin plus clopidogrel for 90 days reduced major ischaemic events from 6.5% to 5.0% (25% RRR) but with increased major bleeding (0.9% vs 0.4%).
The synthesis is that 21 days of DAPT provides optimal balance - most stroke prevention benefit occurs early, while bleeding risk increases with prolonged therapy. Current guidelines recommend DAPT for 21 days in high-risk TIA (ABCD2 ≥4) or minor stroke, followed by single antiplatelet therapy."
Viva Point: Q: When would you refer for carotid endarterectomy?
Answer: "Carotid endarterectomy is indicated for symptomatic carotid stenosis ≥70% (NASCET criteria) and should be performed within 2 weeks of the index event.
Key points from NASCET:
- 70-99% stenosis: 2-year stroke risk 9% with CEA vs 26% medical therapy (NNT = 6)
- 50-69% stenosis: Modest benefit (NNT = 22), decision individualised
- less than 50% stenosis: No benefit from surgery
Timing is critical: Benefit decreases by 14% for each week of delay. Surgery should be performed within 2 weeks, ideally within first week.
Patient selection: Perioperative stroke/death rate must be less than 6% for net benefit. CAS is alternative for high surgical risk or anatomically unfavourable cases."
Model Answers for Common Scenarios
Scenario 1: TIA with 80% carotid stenosis
"This patient has symptomatic severe carotid stenosis and requires urgent carotid endarterectomy within 2 weeks. Immediate management includes dual antiplatelet therapy, high-intensity statin, and blood pressure optimisation. Surgical referral should occur within 24-48 hours with target intervention within 2 weeks."
Scenario 2: TIA with new atrial fibrillation
"This is a cardioembolic TIA. Anticoagulation is indicated and will replace long-term antiplatelet therapy. Given no infarction on imaging, I would initiate a DOAC within 1-3 days. Apixaban is preferred given its favourable bleeding profile. CHA₂DS₂-VASc score is at least 2 (stroke = 2 points), confirming anticoagulation indication."
Scenario 3: Young patient (35 years) with TIA
"In young patients, I would consider unusual causes including arterial dissection, PFO with paradoxical embolism, vasculitis, and hypercoagulable states. Investigation would include MRA neck with vessel wall imaging, TEE with bubble study, thrombophilia screen, and vasculitis markers. Standard secondary prevention applies pending results."
Common Mistakes (What Fails Candidates)
⚠️ Red Flag: Avoid These Errors:
❌ Failing to recognise TIA as a medical emergency ❌ Not initiating antiplatelet therapy immediately ❌ Using outdated 24-hour time-based definition ❌ Not arranging urgent carotid imaging for all patients ❌ Forgetting to check for atrial fibrillation ❌ Not knowing DAPT duration (21 days, not 90 days) ❌ Wrong NASCET stenosis thresholds for CEA (≥70% = strong, 50-69% = moderate) ❌ Failing to counsel on driving restrictions ❌ Not knowing landmark trials (CHANCE, POINT, NASCET, SPARCL) ❌ Missing the distinction between TIA (no infarct) and minor stroke (DWI+)
Key Guidelines
International Guidelines Summary
| Organisation | Guideline | Year | Key Recommendations |
|---|---|---|---|
| AHA/ASA | Guidelines for Prevention of Stroke | 2021 | DAPT 21 days, CEA less than 2 weeks, DOACs for AF |
| ESC | Guidelines on Cardiovascular Prevention | 2021 | LDL less than 1.4 mmol/L very high risk, BP less than 130/80 |
| NICE | Stroke and TIA (NG128) | 2019 | Urgent assessment less than 24h, carotid imaging all patients |
| Royal College of Physicians | National Clinical Guideline for Stroke | 2023 | DAPT 21 days, CEA within 7 days if possible |
Evidence Strength Summary
| Recommendation | Evidence Level | Strength |
|---|---|---|
| DAPT for 21 days (high-risk TIA) | Level I | Strong |
| High-intensity statin | Level I | Strong |
| CEA for ≥70% symptomatic stenosis | Level I | Strong |
| MRI with DWI for diagnosis | Level II | Strong |
| DOACs over warfarin for AF | Level I | Strong |
| BP target less than 130/80 mmHg | Level II | Moderate |
| Extended cardiac monitoring (cryptogenic) | Level I | Strong |
Clinical Pearls Summary
Clinical Pearl: Diagnostic Pearls:
- TIA is a clinical diagnosis - symptoms resolved, investigations may be negative
- 30-50% of "clinical TIAs" are actually minor strokes (DWI positive)
- ABCD2 score underestimates risk - add imaging and carotid findings
- Amaurosis fugax strongly suggests carotid source
- Isolated vertigo is rarely TIA - require additional posterior circulation symptoms
- AF may be paroxysmal - extended monitoring detects 25-30% occult AF
Treatment Pearls:
- Start aspirin immediately - don't wait for imaging (unless haemorrhage suspected)
- DAPT for 21 days in high-risk TIA - not 90 days (bleeding risk increases)
- Carotid surgery within 2 weeks - benefit decreases by 14% per week delay
- High-intensity statin for all (SPARCL trial)
- BP control chronic phase only - permissive acutely
- DOACs preferred over warfarin for AF-related TIA
Disposition Pearls:
- Low-risk TIA can be managed outpatient IF urgent workup ensured
- High-risk (ABCD2 ≥4, carotid disease, AF) - consider admission
- Crescendo TIAs warrant admission - unstable condition
- Close follow-up essential - highest stroke risk first 48 hours
- Ensure patient understands FAST signs and when to return
References
-
Amarenco P, Lavallée PC, Labreuche J, et al. One-year risk of stroke after transient ischemic attack or minor stroke. N Engl J Med. 2016;374(16):1533-1542. doi:10.1056/NEJMoa1412981
-
Coull AJ, Lovett JK, Rothwell PM; Oxford Vascular Study. Population based study of early risk of stroke after transient ischaemic attack or minor stroke: implications for public education and organisation of services. BMJ. 2004;328(7435):326. doi:10.1136/bmj.37991.635266.44
-
Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2009;40(6):2276-2293. doi:10.1161/STROKEAHA.108.192218
-
Coutts SB, Simon JE, Eliasziw M, et al. Triaging transient ischemic attack and minor stroke patients using acute magnetic resonance imaging. Ann Neurol. 2005;57(6):848-854. doi:10.1002/ana.20497
-
Johnston SC, Easton JD, Farrant M, et al. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA. N Engl J Med. 2018;379(3):215-225. doi:10.1056/NEJMoa1800410
-
Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med. 2013;369(1):11-19. doi:10.1056/NEJMoa1215340
-
Barnett HJM, Taylor DW, Haynes RB, et al. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991;325(7):445-453. doi:10.1056/NEJM199108153250701
-
Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007;370(9596):1432-1442. doi:10.1016/S0140-6736(07)61448-2
-
Amarenco P, Bogousslavsky J, Callahan A III, et al. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355(6):549-559. doi:10.1056/NEJMoa061894
-
PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attack. Lancet. 2001;358(9287):1033-1041. doi:10.1016/S0140-6736(01)06178-5
-
Kleindorfer D, Panagos P, Pancioli A, et al. Incidence and short-term prognosis of transient ischemic attack in a population-based study. Stroke. 2005;36(4):720-723. doi:10.1161/01.STR.0000158917.59233.b7
-
Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24(1):35-41. doi:10.1161/01.STR.24.1.35
-
O'Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761-775. doi:10.1016/S0140-6736(16)30506-2
-
Sheehan OC, Merwick A, Kelly LA, et al. Diagnostic usefulness of the ABCD2 score to distinguish transient ischemic attack and minor ischemic stroke from noncerebrovascular events: the North Dublin TIA Study. Stroke. 2009;40(11):3449-3454. doi:10.1161/STROKEAHA.109.557074
-
Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292. doi:10.1016/S0140-6736(07)60150-0
-
Sanna T, Diener HC, Passman RS, et al. Cryptogenic stroke and underlying atrial fibrillation. N Engl J Med. 2014;370(26):2478-2486. doi:10.1056/NEJMoa1313600
-
European Carotid Surgery Trialists' Collaborative Group. MRC European Carotid Surgery Trial: interim results for symptomatic patients with severe (70-99%) or with mild (0-29%) carotid stenosis. Lancet. 1991;337(8752):1235-1243. doi:10.1016/0140-6736(91)92916-P
-
Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893-2962. doi:10.1093/eurheartj/ehw210
-
Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(7):2160-2236. doi:10.1161/STR.0000000000000024
-
Brott TG, Hobson RW 2nd, Howard G, et al. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med. 2010;363(1):11-23. doi:10.1056/NEJMoa0912321
Version History
| Version | Date | Changes |
|---|---|---|
| 1.0 | 2025-01-15 | Initial comprehensive version |
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Prerequisites
Start here if you need the foundation before this topic.
- Cerebrovascular Anatomy
- Atherosclerosis Pathophysiology
Differentials
Competing diagnoses and look-alikes to compare.
- Migraine with Aura
- Seizure Disorders
- Hypoglycaemia