Ulcerative Colitis
Ulcerative Colitis (UC) is a chronic, relapsing-remitting inflammatory bowel disease (IBD) characterized by continuous m... MRCP exam preparation.
What matters first
Ulcerative Colitis (UC) is a chronic, relapsing-remitting inflammatory bowel disease (IBD) characterized by continuous m... MRCP exam preparation.
Stool frequency less than 6/day + systemic toxicity (Acute Severe Colitis)
6 Jan 2026
Generated educational material; verify before clinical use.
Visible references section
See the concept before reading it
Study the key anatomy, imaging, and decision pathways as full teaching plates.
Clinical board
A visual summary of the highest-yield teaching signals on this page.
Urgent signals
Safety-critical features pulled from the topic metadata.
- Stool frequency less than 6/day + systemic toxicity (Acute Severe Colitis)
- Abdominal distension + SBP less than 120 (Toxic Megacolon)
- Rigidity and guarding (Perforation)
- Massive rectal haemorrhage
Exam focus
Current exam surfaces linked to this topic.
- MRCP
Linked comparisons
Differentials and adjacent topics worth opening next.
- Crohn's Disease
- Infective Colitis
Content status and exam context
This page is AI-generated educational content. It may contain errors or omissions and is not a substitute for current guidelines, local protocols, senior clinical judgement, or professional medical advice.
MedVellum does not claim an individual clinician reviewer, board certification, or professional credential for this page unless a future version names a real, verifiable reviewer.
Clinical explanation and evidence
Ulcerative Colitis (Adult)
1. Overview
Ulcerative Colitis (UC) is a chronic, relapsing-remitting inflammatory bowel disease (IBD) characterized by continuous mucosal inflammation limited to the colon and rectum. Unlike Crohn's disease, UC invariably involves the rectum and extends proximally in a contiguous fashion without skip lesions. [1]
The clinical significance of UC lies in its potential for life-threatening complications—specifically Acute Severe Colitis (ASC) and toxic megacolon—and its strong association with colorectal malignancy. UC represents a disease of mucosal barrier dysfunction and dysregulated immune tolerance to commensal microbiota, driving a destructive inflammatory cascade. [2,7]
The Modern Paradigm Shift
Management has entered the "Treat-to-Target" era, moving beyond symptom control to achievement of deep remission—a composite of clinical remission, endoscopic healing (Mayo endoscopic subscore 0-1), and increasingly, histological remission. [3] This paradigm shift reflects evidence that mucosal healing predicts sustained remission, reduces hospitalization, and decreases colorectal cancer risk.
The therapeutic armamentarium now extends well beyond aminosalicylates and corticosteroids to include multiple biologics (anti-TNF, anti-integrin, anti-IL12/23) and small molecules (JAK inhibitors, S1P modulators). [16] Unlike Crohn's disease, UC can potentially be "cured" surgically via panproctocolectomy with ileal pouch-anal anastomosis (IPAA), though this carries significant morbidity and quality-of-life implications.
Epidemiological Context
UC represents a global health burden with rising incidence in newly industrialized nations. [4] The disease exhibits curious epidemiological paradoxes—protective effects of smoking and early appendicectomy—that provide clues to its immunopathogenesis.
2. Epidemiology
Global Distribution and Incidence
High-incidence regions: Northern Europe, United Kingdom, and North America demonstrate incidence rates of 10-20 per 100,000 person-years with prevalence approaching 250-500 per 100,000. [4,18]
Emerging epidemiology: Rapidly industrializing nations in Asia (China, South Korea, India), South America (Brazil), and the Middle East show accelerating incidence rates, following a pattern 2-3 decades behind Western nations. This suggests environmental triggers associated with Westernization—dietary changes, antibiotic exposure, reduced microbial diversity, and urbanization. [4]
Age and Sex Distribution
Bimodal age distribution:
- Primary peak: 15-30 years (young adulthood)
- Secondary smaller peak: 50-70 years (late-onset UC)
Late-onset UC (diagnosed > 60 years) represents 10-15% of cases and often presents with more extensive disease but potentially less aggressive course. [1]
Sex ratio: Slight male predominance (male:female ratio approximately 1.2:1), though this varies geographically.
Genetic Susceptibility
Familial clustering: First-degree relatives of UC patients have 10-15 fold increased risk. Concordance in monozygotic twins is 10-15% (lower than Crohn's disease at 30-35%), suggesting environmental factors play a larger role. [1]
Genome-wide association studies (GWAS): Over 240 susceptibility loci identified, including genes involved in:
- Epithelial barrier function (ECM1, CDH1, LAMB1)
- Innate immunity (NOD2, IL23R, CARD9)
- Adaptive immunity (IL10, MST1, STAT3)
- Autophagy pathways
However, genetic risk factors explain only 15-20% of disease variance, emphasizing the critical role of gene-environment interactions. [7]
The "Protective" Paradoxes
Smoking: The UC Exception
Active smoking is protective against UC onset (OR 0.58, 95% CI 0.45-0.75) and reduces flare severity—a unique paradox as smoking worsens Crohn's disease. [5] Proposed mechanisms include:
- Altered colonic mucus production and composition
- Reduced intestinal permeability
- Modified cytokine profiles (reduced IL-13)
- Changes in gut microbiome composition
Clinical caveat: The harms of smoking far outweigh any protective benefit, and smoking cessation should always be encouraged. Disease flares following smoking cessation can be managed with appropriate medical therapy.
Appendicectomy Effect
Early appendicectomy for true appendicitis (before age 20) reduces long-term UC risk by approximately 50%. [13] This protective effect is specific to appendicectomy for appendicitis, not incidental appendicectomy during other procedures. Proposed mechanisms involve removal of lymphoid tissue involved in aberrant immune priming or alteration of gut microbiome composition.
Socioeconomic and Environmental Factors
Urban > Rural: Higher incidence in urban areas suggests environmental triggers (pollution, dietary factors, reduced microbial exposure).
Hygiene hypothesis: Reduced early-life microbial exposure may predispose to UC through inadequate immune system education.
Antibiotic exposure: Particularly in early childhood, associated with increased UC risk (dose-dependent relationship).
3. Aetiology & Pathophysiology
The Multifactorial Model
UC arises from complex interactions between:
- Genetic susceptibility (> 240 loci identified)
- Environmental triggers (microbiome perturbation, diet, medications)
- Immune dysregulation (loss of tolerance to commensal bacteria)
- Epithelial barrier dysfunction
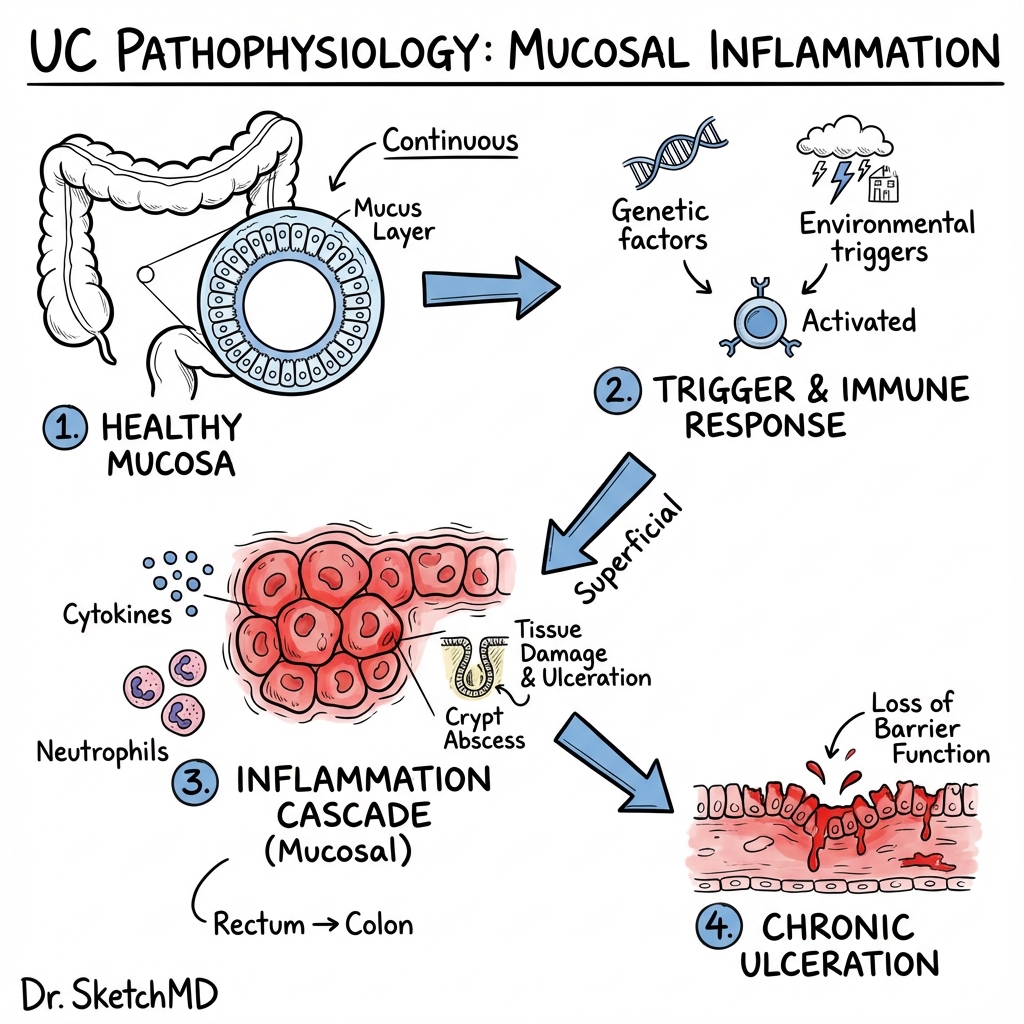
⚠️ THE 7-STEP MOLECULAR CASCADE
This mechanistic framework integrates current understanding of UC immunopathology:
Step 1: Mucus Barrier Failure
The colonic mucus layer comprises an inner firmly adherent layer (sterile) and outer loose layer (colonized). Genetic variants affecting mucin production (MUC2, MUC19) or glycosylation patterns lead to:
- Thinning of inner mucus layer
- Altered mucus composition and viscosity
- Increased bacterial penetration toward epithelium
- Reduced spatial separation between microbiota and host tissue [6]
Step 2: Epithelial Barrier Disruption
Genetic defects in tight junction proteins (CLDN2, CDH1) and increased epithelial apoptosis result in:
- Increased intestinal permeability ("leaky gut")
- Paracellular passage of bacterial antigens
- Direct bacterial contact with basolateral epithelial surface
- Activation of pattern recognition receptors (TLRs, NOD2) [7]
Step 3: Dendritic Cell Activation
Bacterial antigens engage Toll-like receptors (TLR2, TLR4, TLR5) and NOD-like receptors on dendritic cells, triggering:
- NF-κB activation and pro-inflammatory gene transcription
- IL-23 and IL-12 production by activated dendritic cells
- Migration to mesenteric lymph nodes
- Presentation of bacterial antigens to naive T cells [7]
Step 4: Pathogenic T Cell Differentiation
IL-23-driven polarization generates pathogenic T cell subsets:
Th2-like cells:
- Produce IL-5 (eosinophil recruitment) and IL-13 (epithelial toxicity)
- IL-13 is the central effector cytokine in UC pathogenesis
Th17 cells:
- Produce IL-17A/F (neutrophil recruitment)
- Produce IL-22 (epithelial proliferation but also barrier disruption)
Reduced regulatory T cells (Tregs):
- Defective IL-10 production
- Impaired suppression of effector T cells
- Loss of tolerance to commensal antigens [6,7]
Step 5: IL-13 Mediated Epithelial Injury
IL-13 is the master cytokine driving UC tissue damage through multiple mechanisms:
- Direct apoptosis of colonocytes via STAT6 signaling
- Increased epithelial permeability through tight junction disruption
- Impaired epithelial restitution and wound healing
- Reduced mucin production exacerbating barrier dysfunction
- Enhanced antigen presentation by epithelial cells [6]
This contrasts with Crohn's disease, where IL-12/IFN-γ/TNF-α predominate.
Step 6: Neutrophil-Mediated Tissue Destruction
Massive neutrophil recruitment driven by CXCL8 (IL-8) and IL-17:
- Neutrophil migration through lamina propria into intestinal crypts
- Formation of crypt abscesses (pathognomonic histological feature)
- Release of reactive oxygen species (ROS) causing oxidative damage
- Degranulation releasing proteases and matrix metalloproteinases (MMPs)
- Secondary epithelial injury and ulcer formation [1,7]
Step 7: Chronic Inflammation and Architectural Distortion
Repeated injury-repair cycles lead to:
- Goblet cell depletion (reduced mucin production)
- Crypt architectural distortion (branching, atrophy, shortening)
- Basal plasmacytosis (plasma cells in deep lamina propria)
- Pseudopolyp formation (islands of regenerating mucosa)
- Dysplasia-carcinoma sequence (long-term consequence) [13]
The Microbiome in UC
Patients with UC demonstrate:
- Reduced microbial diversity (particularly Firmicutes)
- Expansion of pathobionts (e.g., adherent-invasive E. coli, Fusobacterium)
- Depletion of butyrate-producing bacteria (butyrate is primary colonocyte fuel)
- Reduced Faecalibacterium prausnitzii (anti-inflammatory commensal)
Whether dysbiosis is primary (causative) or secondary (consequence of inflammation) remains debated, but microbiome manipulation represents a therapeutic target. [1]
4. Clinical Presentation
Cardinal Symptom Complex
Bloody Diarrhoea
- Hallmark symptom present in > 95% of patients
- Blood is typically mixed with stool or coating surface
- May be accompanied by mucus ("redcurrant jelly" appearance)
- Distinguishes UC from irritable bowel syndrome (IBS)
Urgency and Tenesmus
- Sudden, compelling need to defecate
- Tenesmus: painful straining with passage of only blood/mucus
- Indicates rectal inflammation (proctitis)
- Severely impacts quality of life and social functioning
Nocturnal Symptoms
- Waking at night to defecate is highly specific for organic IBD
- Distinguishes from functional bowel disorders (IBS rarely causes nocturnal symptoms)
- Number of nocturnal stools correlates with disease severity
Abdominal Pain
- Typically cramping lower abdominal pain
- May be relieved temporarily by defecation
- Severe pain suggests complications (toxic megacolon, perforation)
- Usually less prominent than in Crohn's disease
Disease Extent Classification
Disease extent determines prognosis, cancer risk, and treatment approach:
E1: Proctitis (30-40% at presentation)
- Limited to rectum (distal to rectosigmoid junction)
- Rectal bleeding, urgency, tenesmus predominate
- Constipation may occur paradoxically (rectal inflammation impairs filling)
- Topical therapy often sufficient
- Lowest cancer risk
E2: Left-sided colitis (30-40% at presentation)
- Extends to splenic flexure
- Bloody diarrhoea and cramping left lower quadrant pain
- Responds to topical + oral therapy
- Intermediate cancer risk
E3: Extensive colitis/pancolitis (20-30% at presentation)
- Extends proximal to splenic flexure or involves entire colon
- Most severe symptoms
- Higher risk of acute severe colitis
- Highest cancer risk
- Often requires systemic therapy
Progression: Approximately 30% of patients with limited disease will develop more extensive disease over time, though regression of extent is uncommon. [1,13]
Clinical Phenotypes
Acute Severe Colitis (ASC)
Life-threatening presentation requiring hospitalization:
- Truelove and Witts criteria (1955, still current):
- ≥6 bloody stools per day AND
- "One or more systemic features:"
- Fever > 37.8°C
- Tachycardia > 90 bpm
- Haemoglobin less than 10.5 g/dL
- ESR > 30 mm/hr (or CRP > 30 mg/L)
ASC occurs in 15-25% of patients at some point and carries mortality risk of 1-2% with optimal management. [9]
Chronic Continuous Activity
- Persistent symptoms without remission periods
- 5-10% of patients
- Associated with higher complications risk
- Often requires advanced therapies
Chronic Relapsing-Remitting
- Most common pattern (70-80%)
- Periods of remission (weeks to years) interrupted by flares
- Predictors of relapse: disease extent, young age at diagnosis, need for steroids at diagnosis
Physical Examination Findings
General Assessment
- Cachexia/malnutrition: Suggests severe or chronic active disease
- Pallor: Anaemia from chronic blood loss or anaemia of chronic disease
- Fever: Active inflammation or complications (infection, toxic megacolon)
- Tachycardia: Hypovolaemia, anaemia, sepsis, or hyperthyroidism (associated autoimmunity)
Abdominal Examination
- Tenderness: Typically lower abdomen, left iliac fossa
- Distension: May indicate toxic megacolon (medical emergency)
- Mass: Uncommon (suggests malignancy or inflammatory mass)
- Peritonism: Suggests perforation requiring emergency surgery
Digital Rectal Examination
- Blood on glove (confirms bleeding)
- Assess for perianal disease (uncommon in UC; suggests Crohn's disease)
- Tenderness reflects proctitis severity
Extra-Intestinal Manifestations (EIMs)
EIMs occur in 25-40% of UC patients and significantly impact morbidity. [8,14]
Musculoskeletal (Most Common)
Type 1 Peripheral Arthropathy (Pauciarticular):
- Large joint oligoarthritis (less than 5 joints)
- Typically knees, ankles, wrists, elbows
- Parallels gut disease activity
- Non-erosive, self-limiting with colitis treatment
- Affects 3-10% of UC patients
Type 2 Peripheral Arthropathy (Polyarticular):
- Small joint polyarthritis (≥5 joints)
- Independent of gut activity
- Can be erosive and persistent
- Requires rheumatology input
Axial Arthropathy:
- Sacroiliitis (asymptomatic in many)
- Ankylosing spondylitis (3-5% of UC patients)
- HLA-B27 positive in 50-70%
- Independent of gut activity; persists after colectomy
- Requires anti-TNF therapy in severe cases [8]
Dermatological
Erythema Nodosum:
- Tender red nodules on shin/extensor surfaces
- Parallels gut disease activity
- Resolves with colitis treatment
- Occurs in 2-4% of UC patients
Pyoderma Gangrenosum:
- Rapidly progressive painful ulcers with violaceous undermined edges
- Often on lower limbs but can occur anywhere
- May be independent of gut activity
- Requires aggressive immunosuppression (ciclosporin, infliximab)
- Occurs in 1-2% but highly morbid [8]
Ocular
Episcleritis:
- Red, mildly painful eye
- Parallels gut disease activity
- Self-limiting
Uveitis/Iritis:
- Painful red eye with photophobia and blurred vision
- Independent of gut activity
- Ophthalmology emergency (risk of blindness)
- Requires topical/systemic steroids
- Occurs in 0.5-3% [8]
Hepatobiliary
Primary Sclerosing Cholangitis (PSC):
- Progressive fibrosing cholangiopathy
- 2-7.5% of UC patients develop PSC
- Conversely, 60-80% of PSC patients have UC
- Presents with:
- Elevated alkaline phosphatase (often asymptomatic)
- Pruritus, jaundice (advanced disease)
- Cholangiocarcinoma risk (10-15% lifetime)
- Colorectal cancer risk increased 4-5 fold
- Diagnosed by MRCP showing multifocal strictures ("beading")
- Independent of gut activity; persists after colectomy
- No effective medical therapy (liver transplantation for end-stage) [13]
Thromboembolic
- Venous thromboembolism (VTE) risk increased 3-fold
- Multifactorial: chronic inflammation, hypercoagulable state, immobility during flares
- DVT/PE occur in 1-7% during active disease
- Prophylactic anticoagulation recommended during hospitalization [1]
Psychosocial Impact
UC profoundly affects quality of life:
- Depression and anxiety rates 2-3 times higher than general population
- Fear of incontinence leading to social isolation
- Impact on education, employment, relationships
- Body image concerns (especially post-colectomy with stoma)
- Screening for psychological distress should be routine
5. Investigations
Initial Diagnostic Workup
Stool Studies (Mandatory)
Microbiology:
- Stool culture: Salmonella, Shigella, Campylobacter, E. coli O157
- Clostridioides difficile toxin: PCR for toxin genes (CDI can trigger or mimic UC flare)
- Ova, cysts, parasites: Particularly Entamoeba histolytica (can mimic UC endoscopically)
- CMV PCR: If severe/refractory colitis (CMV superinfection)
Rationale: Infective colitis must be excluded before starting immunosuppression.
Faecal Calprotectin:
- Neutrophil-derived protein released during intestinal inflammation
-
250 μg/g highly sensitive (90-95%) for IBD
- Useful for:
- Distinguishing IBD from IBS
- Monitoring disease activity
- Predicting relapse (rising levels precede clinical flare)
- Limitations: Non-specific (elevated in infections, NSAIDs, malignancy) [2]
Blood Tests
Full Blood Count:
- Anaemia: Normocytic (chronic disease) or microcytic (iron deficiency from bleeding)
- Thrombocytosis: Reactive to inflammation (platelets > 450 × 10⁹/L)
- Leukocytosis: Active inflammation or steroid effect
Inflammatory Markers:
- CRP: Correlates with disease activity (though ~20% of UC patients have normal CRP despite active disease)
- ESR: Less specific but useful in Truelove-Witts criteria
- Albumin: Low in severe disease (protein-losing enteropathy); prognostic in ASC
Renal and Liver Function:
- Baseline before therapy
- Elevated ALP: Consider PSC
Iron Studies:
- Ferritin low in iron deficiency; raised in inflammation
- Transferrin saturation less than 20% indicates iron deficiency
Serological Markers (Limited Clinical Utility):
- p-ANCA (perinuclear anti-neutrophil cytoplasmic antibody): Positive in 60-70% of UC (vs. 5-20% of Crohn's)
- Anti-Saccharomyces cerevisiae antibodies (ASCA): Negative in UC (positive in 60% of Crohn's)
- Not diagnostic but may aid in indeterminate colitis cases [1]
Endoscopy: The Gold Standard
Flexible Sigmoidoscopy (First-Line):
- Reaches to splenic flexure (60 cm)
- Allows assessment of rectum and left colon
- Can obtain biopsies
- Safer than colonoscopy in acute severe colitis
- Adequate for diagnosis in most cases (since UC always involves rectum)
Colonoscopy (For Extent Assessment):
- Performed after acute inflammation controlled
- Assesses full disease extent
- Obtains biopsies from multiple sites for histology
- Risk of perforation if severe active inflammation
Endoscopic Features of UC:
- Continuous inflammation starting from rectum extending proximally
- Loss of normal vascular pattern
- Erythema and granularity
- Friability (spontaneous bleeding or bleeding to touch)
- Superficial ulceration
- Pseudopolyps (islands of regenerating mucosa)
- No skip lesions (vs. Crohn's disease) [1,13]
Mayo Endoscopic Subscore (Severity Grading):
- 0: Normal or inactive disease
- 1: Erythema, decreased vascular pattern, mild friability
- 2: Marked erythema, absent vascular pattern, friability, erosions
- 3: Spontaneous bleeding, ulceration
Target for mucosal healing is Mayo endoscopic subscore ≤1. [3]
Histopathology
Biopsies essential for confirming diagnosis and excluding other pathology:
Acute Inflammatory Features:
- Crypt abscesses (neutrophils in crypt lumens—pathognomonic)
- Cryptitis (neutrophilic infiltration of crypt epithelium)
- Goblet cell depletion
- Diffuse mucosal inflammation
Chronic Features:
- Crypt architectural distortion (branching, atrophy)
- Basal plasmacytosis (plasma cells below muscularis mucosae)
- Paneth cell metaplasia (Paneth cells normally absent in left colon)
- Villous surface irregularity
Distinguishing from Crohn's:
- UC: Inflammation confined to mucosa/superficial submucosa
- Crohn's: Transmural inflammation, granulomas (in 30%), skip lesions [13]
Dysplasia Surveillance:
- Low-grade dysplasia (LGD)
- High-grade dysplasia (HGD)
- Dysplasia-associated lesion or mass (DALM)
Imaging
Plain Abdominal Radiograph
Indications:
- Acute severe colitis (daily monitoring for toxic megacolon)
- Suspected perforation
Features:
- Toxic megacolon: Transverse colon diameter > 5.5-6 cm
- Mucosal islands or "thumbprinting"
- Colonic wall thickening
- Free air (perforation)
- Fecal loading (constipation in proctitis) [9]
Cross-Sectional Imaging
CT Abdomen/Pelvis (with IV contrast):
- Indicated in severe colitis to exclude complications
- Findings:
- Bowel wall thickening (> 3-4 mm)
- Submucosal oedema ("target sign")
- Mucosal hyperenhancement
- Pericolic fat stranding
- Abscess or perforation
- Limitation: Radiation exposure
MR Enterography:
- Preferred over CT in young patients (no radiation)
- Can assess small bowel (if Crohn's disease suspected)
- Excellent for pelvic imaging (presacral space, perianal disease)
Specialist Investigations
MRCP (Magnetic Resonance Cholangiopancreatography):
- Indicated if elevated ALP (suspected PSC)
- Demonstrates multifocal bile duct strictures and dilatation ("beading")
- Non-invasive alternative to ERCP
DEXA Scan:
- Baseline bone density in patients requiring corticosteroids
- Repeat every 2-3 years
6. Management
Strategic Framework: Treat-to-Target
The STRIDE-II consensus (2021) established therapeutic targets beyond symptom resolution: [3]
Short-term targets (3-6 months):
- Clinical remission (symptom-free)
- Biomarker normalization (CRP, faecal calprotectin)
- Endoscopic healing (Mayo endoscopic subscore 0-1)
Long-term targets (12 months):
- Sustained clinical and endoscopic remission
- Histological remission (absence of neutrophils)
- Restoration of quality of life
- Prevention of disability and complications
Rationale: Mucosal healing predicts sustained remission, reduces hospitalization, steroid use, and colorectal cancer risk.
1. Induction of Remission: Mild-to-Moderate Disease
Disease severity assessed by clinical symptoms, endoscopy, and biomarkers.
Proctitis (E1)
First-line: Topical 5-ASA (Mesalazine)
- Rectal suppositories 1 g once daily (OD) or twice daily (BD)
- Superior to oral therapy alone for proctitis
- Clinical response in 70-80% within 2-4 weeks [2,20]
Second-line: Add oral 5-ASA
- Mesalazine 2.4-4.8 g/day orally
- Combination (topical + oral) superior to either alone
Refractory proctitis:
- Topical corticosteroid (prednisolone suppositories 5 mg)
- Oral prednisolone 40 mg daily (if no response to topical)
Left-sided Colitis (E2)
First-line: Topical 5-ASA (Mesalazine)
- Rectal enemas 1-4 g once daily
- Reach to splenic flexure
- Response rate 60-70% [2,20]
Second-line: Combination therapy
- Oral mesalazine 2.4-4.8 g/day + topical mesalazine
- Superior to oral monotherapy
Refractory:
- Oral prednisolone 40 mg daily (8-week tapering course)
- Budesonide MMX 9 mg (lower systemic absorption, fewer side effects)
Extensive Colitis/Pancolitis (E3)
First-line: Oral 5-ASA
- Mesalazine 2.4-4.8 g/day
- Adding topical therapy improves outcomes
Moderate activity:
- Oral corticosteroids (prednisolone 40 mg daily, taper over 8 weeks)
- Response in 80-90% but relapse common after taper
- Steroid-dependence in 20-30%
Steroid-dependent or steroid-refractory:
- Thiopurines (azathioprine 2-2.5 mg/kg or mercaptopurine 1-1.5 mg/kg)
- Check TPMT enzyme activity before starting
- Monitor FBC and LFTs (myelosuppression, hepatotoxicity risks)
- Slow onset (8-12 weeks to effect)
- Biologics (see Section 6.3)
2. Acute Severe Colitis (ASC): Medical Emergency
ASC is a life-threatening presentation requiring immediate hospitalization. [9,20]
Diagnostic Criteria: Truelove and Witts
≥6 bloody stools per day AND one or more of:
- Fever > 37.8°C
- Tachycardia > 90 bpm
- Haemoglobin less than 10.5 g/dL
- ESR > 30 mm/hr (or CRP > 30 mg/L)
Initial Management (First 24-48 Hours)
1. Admit to Gastroenterology Ward (specialist nursing, frequent review)
2. Investigations:
- Stool culture, C. difficile toxin, CMV PCR
- FBC, CRP, albumin, electrolytes, LFTs
- AXR (exclude toxic megacolon, perforation)
- Flexible sigmoidoscopy (confirm diagnosis, assess severity, exclude CMV)
3. Medical Therapy:
- IV hydrocortisone 100 mg QDS (or methylprednisolone 60 mg OD)
- IV fluids and electrolyte replacement (K+, Mg²+)
- Nutritional assessment (consider parenteral nutrition if severely malnourished)
- Prophylactic LMWH (VTE risk)
- Avoid: Opiates (risk toxic megacolon), NSAIDs (worsen colitis), antidiarrhoeals
4. Multidisciplinary Team:
- Daily consultant gastroenterology review
- Surgical team assessment (colorectal surgeon)
- Dietitian, IBD specialist nurse
The Travis Criteria: Day 3 Assessment
Predictor of steroid failure using data from Day 3 of IV hydrocortisone: [9]
- Stool frequency > 8/day OR
- Stool frequency 3-8/day + CRP > 45 mg/L
Interpretation:
- Meeting criteria: 85% probability of requiring colectomy
- Action: Initiate rescue therapy immediately
Rescue Therapy (Steroid-Refractory ASC)
Two options with equivalent efficacy (CONSTRUCT trial): [10]
Option 1: Infliximab
- 5 mg/kg IV at weeks 0, 2, 6
- Response rate 70-80%
- Faster onset (3-5 days)
- Preferred if patient will continue on anti-TNF long-term
Option 2: Ciclosporin
- 2 mg/kg/day IV continuous infusion
- Response rate 70-80%
- Requires therapeutic drug monitoring (target 200-300 ng/mL)
- Risk of nephrotoxicity, hypertension, seizures
- Bridge to thiopurine therapy
- Preferred if contraindications to anti-TNF
Non-response to rescue therapy:
- Surgery (subtotal colectomy) within 7-10 days
- Delaying beyond 10 days increases mortality
Surgical Indications (Emergency)
Absolute indications:
- Perforation
- Toxic megacolon not responding to 24-48 hours medical therapy
- Massive haemorrhage
Relative indications:
- No response to rescue therapy by day 7-10
- Clinical deterioration despite maximal therapy
Procedure: Subtotal colectomy with end ileostomy
- Preserves rectum for future restorative surgery (IPAA)
- Lower morbidity than emergency total proctocolectomy
3. Maintenance of Remission
Goal: Prevent relapse, maintain quality of life, avoid long-term steroid use.
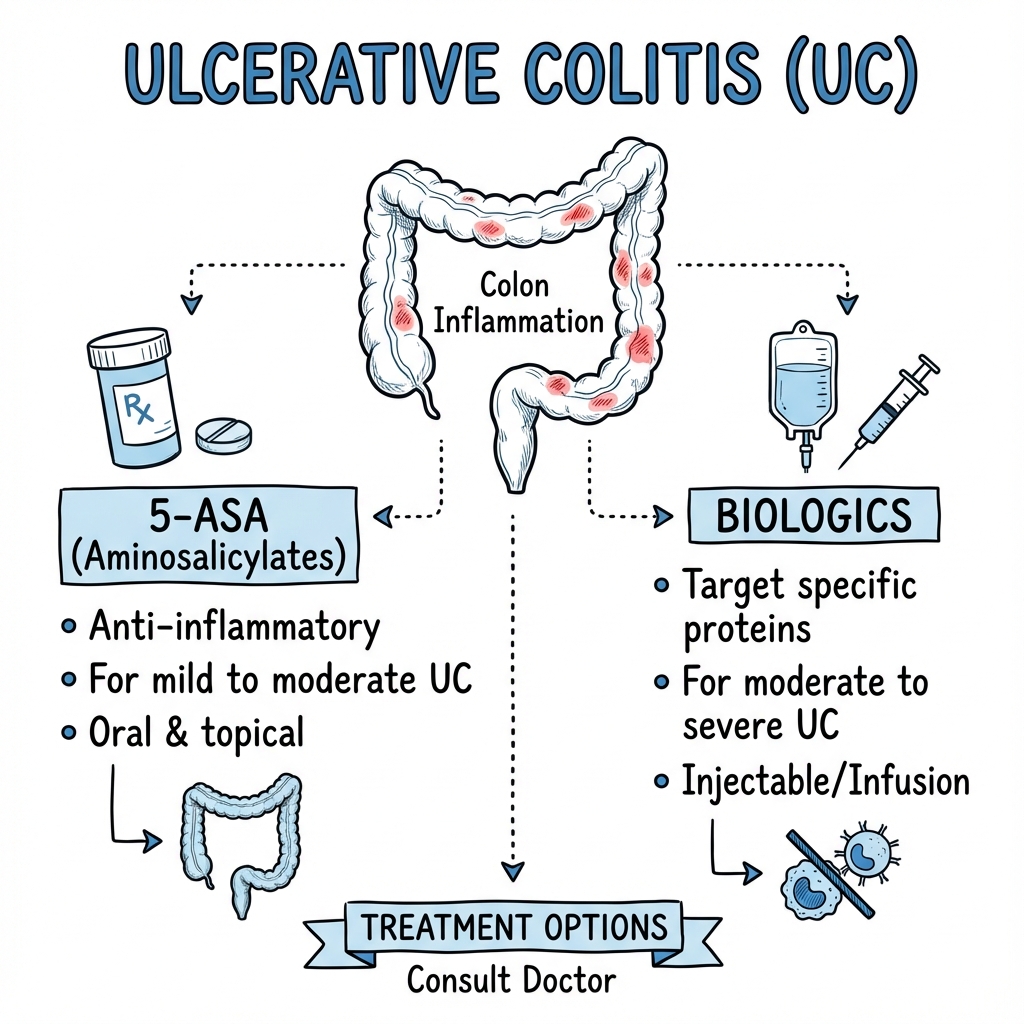
5-Aminosalicylates (5-ASAs)
Mesalazine (first-line maintenance):
- 1.2-2.4 g/day orally
- Reduces relapse rate by 50%
- Chemopreventive against colorectal cancer (RR reduction 0.51)
- Generally well tolerated
- Monitoring: Annual renal function (rare interstitial nephritis)
- Continue lifelong unless contraindication [2,20]
Sulfasalazine:
- Alternative to mesalazine
- 2-4 g/day
- Side effects more common (nausea, headache, oligospermia)
Thiopurines
Indications:
- Steroid-dependent disease (require > 2 courses/year or cannot taper less than 10 mg prednisolone)
- Relapse on 5-ASA monotherapy
Agents:
- Azathioprine 2-2.5 mg/kg/day
- Mercaptopurine 1-1.5 mg/kg/day
Monitoring:
- TPMT enzyme activity before starting (genetic polymorphisms in 10%)
- FBC and LFTs at weeks 2, 4, 8, then 3-monthly
- Risks: Myelosuppression (2-5%), hepatotoxicity (2%), pancreatitis (3%), lymphoma (4-fold increased risk)
Onset: 8-12 weeks (not suitable for acute flares)
Biologic Therapies
Indications for escalation to biologics:
- Moderate-severe disease despite thiopurines
- Steroid-dependent or steroid-refractory disease
- Post-acute severe colitis requiring rescue therapy
- Intolerance to conventional therapies
Anti-TNF Agents
Infliximab (IV infusion):
- Induction: 5 mg/kg at weeks 0, 2, 6
- Maintenance: 5 mg/kg every 8 weeks
- ACT 1 and 2 trials: Clinical remission 33-39% vs. 15% placebo at week 8 [24]
- Response rates higher with therapeutic drug monitoring (target trough 3-7 μg/mL)
Adalimumab (subcutaneous):
- Induction: 160 mg week 0, 80 mg week 2
- Maintenance: 40 mg every 2 weeks
- Convenient self-administration
Golimumab (subcutaneous):
- Induction: 200 mg week 0, 100 mg week 2
- Maintenance: 50-100 mg every 4 weeks
- PURSUIT trial: Remission 51% vs. 30% placebo at week 54 [22]
Monitoring: Anti-drug antibodies, drug levels, TB screening pre-treatment, hepatitis B/C screening
Anti-Integrin Agents
Vedolizumab (gut-selective α4β7 integrin inhibitor):
- Induction: 300 mg IV at weeks 0, 2, 6
- Maintenance: 300 mg IV every 8 weeks
- GEMINI 1 trial: Remission 44.8% vs. 15.9% placebo at week 52 [23]
- VARSITY trial: Superior to adalimumab for inducing and maintaining remission (31.3% vs. 22.5% at week 52) [11]
- Gut-selective: Reduced systemic immunosuppression, excellent safety profile
- Slower onset than anti-TNF (may take 10-14 weeks)
- Preferred first-line biologic based on VARSITY data [11]
Anti-IL12/23 Agents
Ustekinumab (anti-p40 subunit, blocks IL-12 and IL-23):
- Induction: ~6 mg/kg IV (weight-based) single dose
- Maintenance: 90 mg SC every 8 weeks
- UNIFI trial: Clinical remission 43.8% vs. 24.0% placebo at week 44
- Alternative for anti-TNF failures
- Excellent safety profile
Mirikizumab (IL-23p19 inhibitor):
- LUCENT trials demonstrated efficacy
- Histological remission achieved
- Emerging option [16]
JAK Inhibitors (Small Molecules)
Tofacitinib (pan-JAK inhibitor):
- Induction: 10 mg BD for 8 weeks
- Maintenance: 5 mg BD
- OCTAVE trials: Remission 34.3% vs. 10.6% placebo at week 8 [25]
- Black box warning: Increased VTE risk, serious infections, malignancy
- Requires careful patient selection and monitoring
Upadacitinib (JAK1-selective inhibitor):
- Induction: 45 mg OD for 8 weeks
- Maintenance: 15 or 30 mg OD
- U-ACHIEVE trials: Highest remission rates of any UC therapy (42.3-49.5% clinical remission at week 8, 37.2-42.9% at week 52) [12]
- Similar safety concerns to tofacitinib
- Oral convenience, rapid onset (within 2 weeks)
S1P Modulators
Ozanimod (sphingosine-1-phosphate receptor modulator):
- Oral, once daily
- Prevents lymphocyte egress from lymph nodes
- Moderate efficacy, favorable safety
- Requires cardiac monitoring at initiation
4. Surgical Management
Unlike Crohn's disease, UC can be surgically cured by complete removal of colon and rectum.
Indications for Elective Surgery
- Medically refractory disease despite multiple therapies
- Steroid-dependent disease with unacceptable side effects
- Dysplasia or colorectal cancer
- Patient preference (quality of life considerations)
Surgical Procedures
Restorative Proctocolectomy with Ileal Pouch-Anal Anastomosis (IPAA):
- "Gold standard" surgery for UC
- Entire colon and rectum removed
- Ileal reservoir ("J-pouch") created from terminal ileum
- Anastomosed to anal canal preserving sphincters
- Avoids permanent stoma
- Typical bowel frequency: 4-8/day
- Complications:
- Pouchitis (30-50% develop at least one episode)
- Cuffitis (inflammation of rectal cuff)
- Pouch failure (5-10% require pouch excision)
- Female infertility risk (due to pelvic surgery)
Proctocolectomy with Permanent End Ileostomy:
- Indicated if:
- Poor sphincter function (incontinence)
- Patient preference
- Advanced age
- Failed IPAA
- Definitive cure
- Stoma care required
Subtotal Colectomy with Ileostomy (Emergency):
- For acute severe colitis
- Preserves rectum for future decision-making
- Can proceed to IPAA later when patient stabilized
Post-Colectomy Considerations
- Pouchitis: Treated with antibiotics (metronidazole, ciprofloxacin) or probiotics (VSL#3)
- Vitamin B12 monitoring (terminal ileum resection)
- Extra-intestinal manifestations: Axial arthropathy and PSC persist post-colectomy
- Quality of life: Generally excellent; most patients report satisfaction with decision
7. Complications
Acute Complications
Toxic Megacolon
- Transverse colon diameter > 5.5-6 cm with systemic toxicity
- Pathophysiology: Transmural inflammation causing neuromuscular dysfunction
- Clinical features: Abdominal distension, reduced bowel sounds, tachycardia, fever
- AXR diagnostic
- Management: IV fluids, antibiotics, IV steroids; surgical review; colectomy if no improvement in 24-48 hours
- Mortality 20-30% if perforation occurs [9]
Perforation
- Risk factors: Severe colitis, toxic megacolon, recent colonoscopy
- Presents with acute abdomen, peritonism, free air on AXR/CT
- Surgical emergency: Immediate laparotomy and colectomy
Massive Haemorrhage
- Rare (less than 1%) but life-threatening
- Requires resuscitation, blood transfusion
- Consider interventional radiology (angiography ± embolization)
- Surgery if uncontrolled
Venous Thromboembolism (VTE)
- 3-fold increased risk during active disease
- DVT/PE can be presenting feature
- All hospitalized patients require VTE prophylaxis (LMWH)
Chronic Complications
Colorectal Cancer (CRC)
UC is a premalignant condition with cumulative CRC risk:
- 2% at 10 years
- 8% at 20 years
- 18% at 30 years
Risk factors:
- Disease duration (risk begins ~8 years after diagnosis)
- Extensive colitis (pancolitis > left-sided > proctitis)
- Primary sclerosing cholangitis (4-5 fold increased risk)
- Family history of CRC
- Severity of histological inflammation
- Young age at diagnosis
Surveillance Strategy (BSG/ECCO guidelines): [2,13]
Standard risk (extensive colitis without other risk factors):
- Colonoscopy every 2-5 years from 8-10 years after diagnosis
Intermediate risk (extensive colitis + post-inflammatory polyps, family history CRC in first-degree relative > 50 years):
- Colonoscopy every 2-3 years
High risk (PSC, stricture, dysplasia in past 5 years, family history CRC less than 50 years):
- Annual colonoscopy
Technique:
- High-definition white light endoscopy (HDWLE) or chromoendoscopy
- Random biopsies: At least 2 biopsies every 10 cm (minimum 33 biopsies for pancolitis)
- Target all visible lesions
Management of dysplasia:
- Low-grade dysplasia (LGD): Confirm with expert pathologist; consider colectomy or intensive surveillance
- High-grade dysplasia (HGD): Colectomy recommended
- Dysplasia-associated lesion or mass (DALM): Colectomy recommended
Chemopreventive agents:
- 5-ASA: Reduces CRC risk by ~50% (evidence from meta-analyses)
- Ursodeoxycholic acid: May reduce CRC risk in PSC-UC (conflicting evidence)
Stricture
- Occur in 5-10% of patients with long-standing UC
- Concern for malignancy (20-30% of strictures harbor dysplasia/cancer)
- Investigation: Colonoscopy with multiple biopsies ± imaging (CT/MRI)
- Management: Colectomy if dysplasia/cancer; dilation with close surveillance if benign
Pouchitis (Post-IPAA)
- Inflammation of ileal pouch
- Affects 30-50% of patients post-IPAA
- Presents with increased stool frequency, urgency, bleeding, abdominal cramps
- Diagnosis: Pouchoscopy
- Treatment: Antibiotics (metronidazole, ciprofloxacin), probiotics (VSL#3)
- Chronic pouchitis may require anti-TNF therapy
8. Prognosis
Natural History
Relapsing-remitting course: 70-80% of patients experience fluctuating disease with periods of remission and flares.
Chronic continuous activity: 5-10% have persistent symptoms despite treatment.
Colectomy rates:
- 10-year cumulative colectomy rate: 10-15%
- 25-year cumulative colectomy rate: 25-30%
- Declining over time (improved medical therapies) [1]
Factors Affecting Prognosis
Poor prognostic factors (higher relapse/complication risk):
- Extensive disease at diagnosis
- Severe first attack requiring hospitalization
- Young age at diagnosis (less than 40 years)
- Deep ulceration on endoscopy
- Elevated CRP/faecal calprotectin despite clinical remission
- Steroid requirement at diagnosis
Good prognostic factors:
- Limited disease extent (proctitis)
- Endoscopic remission achieved
- Normal biomarkers
- Adherence to maintenance therapy
Mortality
- Overall mortality not increased compared to general population with modern therapy
- Mortality during acute severe colitis: 1-2% (with optimal management)
- Long-term mortality driven by colorectal cancer risk (emphasizing need for surveillance)
Quality of Life
- Most patients (60-70%) in remission report good quality of life
- Employment rates similar to general population
- Fertility generally preserved (female fertility reduced post-IPAA due to pelvic adhesions)
- Pregnancy: Most medications compatible (except methotrexate); maintain remission critical for successful pregnancy outcomes
9. Special Populations
Pregnancy and Ulcerative Colitis
Fertility:
- Active disease reduces fertility (both male and female)
- Female fertility reduced post-IPAA (pelvic adhesions)
- Male fertility reduced with sulfasalazine (reversible oligospermia)
Disease course during pregnancy:
- 30% improve, 30% worsen, 40% unchanged
- Active disease at conception increases relapse risk
- Maintaining remission is critical for maternal and fetal outcomes
Medication safety:
- SAFE: 5-ASA, corticosteroids, azathioprine, biologics (infliximab, adalimumab, vedolizumab)
- AVOID: Methotrexate (teratogenic), tofacitinib (limited data)
Delivery:
- Vaginal delivery generally safe
- Caesarean section recommended if active perianal disease or prior IPAA (preserve sphincter function)
Elderly-Onset UC
- 10-15% diagnosed after age 60
- Often more extensive disease at presentation
- Potentially less aggressive course
- Increased infection risk with immunosuppression (consider vaccinations)
- Higher VTE risk
Paediatric UC
- 20-25% of UC diagnosed before age 20
- Often more extensive and aggressive
- Growth impairment with chronic inflammation or steroid use
- Psychological impact (adolescence, body image)
- Earlier CRC surveillance (start 8 years post-diagnosis regardless of age)
10. Patient Education and Self-Management
Key Discussion Points
Disease explanation:
- Chronic relapsing-remitting condition
- Immune system attacking colon lining
- Not caused by stress or diet (though these may trigger flares)
- Not contagious
Treatment goals:
- Control inflammation
- Achieve and maintain remission
- Prevent complications
- Improve quality of life
Medication adherence:
- Maintenance therapy even when feeling well
- Non-adherence increases relapse risk 5-fold
- Importance of regular monitoring
Red flags (seek urgent medical attention):
- Passing > 6 bloody stools/day with fever
- Severe abdominal pain
- Abdominal distension
- Dizziness/feeling faint
Lifestyle Modifications
Diet:
- No specific "UC diet" proven effective
- Avoid trigger foods (individualized)
- Low-residue diet during flares
- Adequate nutrition (protein, calories, micronutrients)
Smoking:
- Despite "protective" effect, recommend cessation (cardiovascular, cancer, respiratory harms outweigh any UC benefit)
Stress management:
- Stress may trigger flares
- Consider psychological support, CBT, mindfulness
Vaccinations:
- Recommended (before immunosuppression if possible):
- Influenza (annual, inactivated)
- Pneumococcal
- Hepatitis B
- HPV (9-26 years)
- Varicella (if non-immune)
- Avoid live vaccines on immunosuppression (MMR, varicella, yellow fever, oral typhoid)
Support Resources
- Crohn's and Colitis UK (patient charity)
- IBD specialist nurses
- Dietitian support
- Psychological services
- Patient support groups
11. Evidence Base: Landmark Trials
| Trial | Year | Population | Intervention | Control | Primary Outcome | Result | Impact |
|---|---|---|---|---|---|---|---|
| ACT 1 & 2 [24] | 2005 | Moderate-severe UC | Infliximab 5 or 10 mg/kg | Placebo | Clinical remission week 8 | 39% vs. 15% (pless than 0.001) | Established anti-TNF in UC |
| CONSTRUCT [10] | 2016 | Steroid-refractory ASC | Infliximab 5 mg/kg | Ciclosporin 2 mg/kg | Colectomy-free survival | 60% vs. 54% (non-inferior) | Validated both rescue options |
| GEMINI 1 [23] | 2013 | Moderate-severe UC | Vedolizumab 300 mg IV | Placebo | Clinical remission week 52 | 44.8% vs. 15.9% (pless than 0.001) | Gut-selective biologic approved |
| VARSITY [11] | 2019 | Moderate-severe UC | Vedolizumab 300 mg IV | Adalimumab 40 mg SC | Clinical remission week 52 | 31.3% vs. 22.5% (p=0.006) | Vedolizumab superior to adalimumab |
| OCTAVE [25] | 2017 | Moderate-severe UC | Tofacitinib 10 mg BD | Placebo | Clinical remission week 8 | 18.5% vs. 8.2% (p=0.007) | First JAK inhibitor in UC |
| U-ACHIEVE [12] | 2022 | Moderate-severe UC | Upadacitinib 45 mg OD | Placebo | Clinical remission week 8 | 33-38% vs. 4-5% (pless than 0.0001) | Highest efficacy oral agent |
12. Viva Scenarios
Scenario 1: Acute Severe Colitis Management
Examiner: "A 25-year-old woman with known pancolitis presents with 10 bloody stools per day, fever 38.2°C, HR 110, and CRP 95. How would you manage her?"
Model Answer:
-
Recognition: This is Acute Severe Colitis by Truelove-Witts criteria (≥6 bloody stools + fever + tachycardia + raised CRP).
-
Immediate actions:
- Admit under gastroenterology
- IV access, bloods (FBC, CRP, albumin, cultures), stool culture including C. diff
- AXR (exclude toxic megacolon)
- VTE prophylaxis (LMWH)
-
Treatment:
- IV hydrocortisone 100 mg QDS
- IV fluids and electrolyte replacement
- Avoid opiates, NSAIDs, antidiarrhoeals
-
Day 3 assessment (Travis criteria):
- If stool frequency > 8/day OR 3-8 stools + CRP > 45: Rescue therapy indicated
- Options: Infliximab 5 mg/kg IV (preferred) or ciclosporin 2 mg/kg IV
-
Surgical input: Early involvement of colorectal surgeon; consider colectomy if no response to rescue therapy by day 7-10
Scenario 2: PSC-UC Connection
Examiner: "Your 40-year-old UC patient has alkaline phosphatase of 650. What is your differential and what are the implications?"
Model Answer:
-
Top differential: Primary Sclerosing Cholangitis (PSC)
-
Investigation:
- MRCP (characteristic "beading" of bile ducts)
- Liver biopsy if diagnosis uncertain
- Exclude other causes (drugs, gallstones, malignancy)
-
Association with UC:
- 2-7.5% of UC patients develop PSC
- 60-80% of PSC patients have UC (often subclinical)
-
Critical implications:
- Increased CRC risk: 4-5 fold above UC alone
- Screening: Move to annual surveillance colonoscopy from diagnosis
- Cholangiocarcinoma risk: 10-15% lifetime
- PSC independent of gut disease; persists after colectomy
- No effective medical therapy for PSC (ursodeoxycholic acid controversial)
Scenario 3: Biologic Choice
Examiner: "A 28-year-old with extensive UC has failed azathioprine. She asks about biologics. How would you counsel her?"
Model Answer:
-
Explain rationale: Moderate-severe disease requiring escalation; biologics target specific immune pathways
-
Options available:
- Anti-TNF: Infliximab (IV), adalimumab (SC), golimumab (SC)
- Anti-integrin: Vedolizumab (IV)—gut-selective
- Anti-IL12/23: Ustekinumab (IV induction, SC maintenance)
- JAK inhibitors: Upadacitinib, tofacitinib (oral)
-
First-line recommendation: Vedolizumab
- Rationale: VARSITY trial showed superiority over adalimumab
- Gut-selective: Lower systemic immunosuppression, excellent safety
- Slower onset (10-14 weeks) but sustained efficacy
-
Alternative if rapid response needed: Infliximab (faster onset 2-4 weeks)
-
Pre-treatment screening: TB, hepatitis B/C, varicella immunity, vaccinations
-
Monitoring: Clinical response at 12-14 weeks, endoscopy at 6-12 months (assess mucosal healing)
13. Single Best Answer (SBA) Questions
Question 1
A 28-year-old male with known pancolitis is admitted with 10 bloody stools a day, heart rate 110, and CRP 85. He is started on IV hydrocortisone. On Day 3, he is still having 9 stools per day and his CRP is 50. What is the most appropriate next step?
- A) Continue IV hydrocortisone for another 4 days
- B) Start oral azathioprine
- C) Initiate rescue therapy with infliximab or ciclosporin
- D) Perform an emergency subtotal colectomy
- E) Add oral mesalazine 4g daily
Answer: C
Explanation: The patient meets Travis criteria for steroid failure on Day 3 (> 8 stools/day OR 3-8 stools + CRP > 45). This predicts 85% colectomy risk if steroids continued. Immediate rescue therapy with infliximab or ciclosporin is indicated. Delaying increases toxic megacolon and mortality risk. Azathioprine has slow onset (8-12 weeks) and is inappropriate for acute severe colitis. Emergency colectomy is reserved for rescue therapy failure or complications.
Question 2
Which histological feature is most characteristic of ulcerative colitis and distinguishes it from most cases of Crohn's disease?
- A) Non-caseating granulomas
- B) Transmural inflammation
- C) Goblet cell depletion and crypt abscesses
- D) Skip lesions
- E) Deep fissuring ulcers
Answer: C
Explanation: UC is characterized by mucosal and superficial submucosal inflammation with crypt abscesses (neutrophils in crypt lumens) and goblet cell depletion. These are pathognomonic features. In contrast, Crohn's disease demonstrates transmural inflammation, non-caseating granulomas (30%), skip lesions, and fissuring ulcers. UC inflammation is continuous from rectum proximally without skip areas.
Question 3
A 35-year-old woman with extensive UC in remission on mesalazine asks about her colorectal cancer risk. She was diagnosed 9 years ago. What surveillance strategy is most appropriate?
- A) No surveillance required if asymptomatic
- B) Annual faecal occult blood testing
- C) Colonoscopy every 5 years
- D) Colonoscopy every 2-3 years
- E) Annual colonoscopy
Answer: D
Explanation: CRC risk in UC begins ~8 years post-diagnosis. She has extensive colitis > 8 years duration, placing her at standard-intermediate risk. BSG/ECCO guidelines recommend colonoscopy every 2-3 years for extensive colitis without additional risk factors. Annual colonoscopy is reserved for high-risk patients (PSC, stricture, previous dysplasia, strong family history CRC). Five-yearly surveillance is insufficient. FOBT has poor sensitivity for UC-associated CRC.
Question 4
According to the VARSITY trial, which biologic demonstrated superior efficacy compared to adalimumab for moderate-to-severe ulcerative colitis?
- A) Infliximab
- B) Vedolizumab
- C) Ustekinumab
- D) Golimumab
- E) Tofacitinib
Answer: B
Explanation: The VARSITY trial (2019) was the first head-to-head biologic comparison, demonstrating vedolizumab superiority over adalimumab for clinical remission at week 52 (31.3% vs. 22.5%, p=0.006). Vedolizumab is gut-selective (α4β7 integrin inhibitor) with excellent safety profile, now considered preferred first-line biologic based on this evidence.
14. Patient Explanation
"Ulcerative Colitis is a long-term condition where the inner lining of your large bowel (colon) becomes inflamed and develops tiny sores, like scrapes or ulcers. This is why you see blood and mucus when you go to the toilet. It happens because your immune system—which normally fights infections—is mistakenly attacking the lining of your own bowel.
We think this occurs due to a combination of your genes and environmental triggers, possibly involving the normal bacteria that live in your gut. In some people, the immune system sees these harmless bacteria as threats and overreacts.
The condition typically comes and goes in cycles—you'll have periods where you feel well (remission) and times when symptoms flare up. Our goal with treatment is to calm down the inflammation, get you into remission, and keep you there as long as possible.
We use different types of medications depending on how severe your condition is. These include anti-inflammatory drugs (like mesalazine), steroids for flare-ups, and more advanced treatments called biologics that target specific parts of your immune system. Most people respond well to treatment and can live normal, active lives.
It's important to take your maintenance medication even when you feel well, as this prevents flare-ups. We'll also do regular colonoscopy checks every few years because long-term UC slightly increases the risk of bowel cancer—but catching any changes early means we can act quickly.
If your UC becomes very severe and doesn't respond to medications, surgery to remove the colon can be curative. This is a big decision but can dramatically improve quality of life for some people.
The key is working together as a team—you, me, specialist nurses, and dietitians—to manage your condition and help you live your best life."
15. References
-
Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. Lancet. 2017;389(10080):1756-1770. [PMID: 27914657]
-
Lamb CA, Kennedy NA, Raine T, et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1-s106. [PMID: 30563865]
-
Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative. Gastroenterology. 2021;160(5):1570-1583. [PMID: 33359090]
-
Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2021;18(1):56-66. [PMID: 33149273]
-
Mahid SS, Minor KS, Soto RE, Hornung CA, Galandiuk S. Smoking and inflammatory bowel disease: a meta-analysis. Mayo Clin Proc. 2006;81(11):1462-1471. [PMID: 16529140]
-
Heller F, Florian P, Bojarski C, et al. Interleukin-13 is the key effector Th2 cytokine in ulcerative colitis that affects epithelial tight junctions, apoptosis, and cell restitution. Gastroenterology. 2005;129(2):550-564. [PMID: 15825080]
-
Neurath MF. Targeting immune cell circuits and trafficking in inflammatory bowel disease. Nat Immunol. 2019;20(8):970-979. [PMID: 30778252]
-
Harbord M, Annese V, Vavricka SR, et al. The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease. J Crohns Colitis. 2016;10(3):239-254. [PMID: 26614685]
-
Travis SP, Farrant JM, Ricketts C, et al. Predicting outcome in severe ulcerative colitis. Gut. 1996;38(6):905-910. [PMID: 8707082]
-
Williams JG, Alam MF, Alrubaiy L, et al. Infliximab versus ciclosporin for steroid-resistant acute severe ulcerative colitis (CONSTRUCT): a mixed methods, open-label, pragmatic randomised trial. Lancet Gastroenterol Hepatol. 2016;1(1):15-24. [PMID: 28404008]
-
Sands BE, Peyrin-Biroulet L, Loftus EV Jr, et al. Vedolizumab versus Adalimumab for Moderate-to-Severe Ulcerative Colitis. N Engl J Med. 2019;381(13):1215-1226. [PMID: 31556866]
-
Danese S, Vermeire S, Zhou W, et al. Upadacitinib as induction and maintenance therapy for moderately to severely active ulcerative colitis: results from three phase 3, multicentre, double-blind, randomised trials. Lancet. 2022;399(10341):2113-2128. [PMID: 35644154]
-
Magro F, Gionchetti P, Eliakim R, et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J Crohns Colitis. 2017;11(6):649-670. [PMID: 28158501]
-
Rogler G, Singh A, Kavanaugh A, Rubin DT. Extraintestinal Manifestations of Inflammatory Bowel Disease: Current Concepts, Treatment, and Implications for Disease Management. Gastroenterology. 2021;161(4):1118-1132. [PMID: 33497650]
-
Lichtenstein GR, Loftus EV, Isaacs KL, Regueiro MD, Gerson LB, Sands BE. ACG Clinical Guideline: Management of Crohn's Disease in Adults. Am J Gastroenterol. 2018;113(4):481-517. [PMID: 29610508]
-
Neurath MF. Current and emerging therapeutic targets for IBD. Nat Rev Gastroenterol Hepatol. 2017;14(5):269-278. [PMID: 28053338]
-
Orlanski-Meyer E, Aardoom M, Ricciuto A, et al. Predicting Outcomes in Pediatric Ulcerative Colitis for Management Optimization: Systematic Review and Consensus Statements From the Pediatric Inflammatory Bowel Disease-Ahead Program. Gastroenterology. 2021;160(5):1503-1517.e14. [PMID: 33418006]
-
Burisch J, Jess T, Martinato M, Lakatos PL. The burden of inflammatory bowel disease in Europe. J Crohns Colitis. 2013;7(4):322-337. [PMID: 23040452]
-
Peyrin-Biroulet L, Sandborn W, Sands BE, et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target. Am J Gastroenterol. 2015;110(9):1324-1338. [PMID: 25581341]
-
Feuerstein JD, Isaacs KL, Schneider Y, et al. AGA Clinical Practice Guidelines on the Management of Moderate to Severe Ulcerative Colitis. Gastroenterology. 2020;158(5):1450-1461. [PMID: 32240598]
-
Dulai PS, Singh S, Jiang X, et al. The Real-World Effectiveness and Safety of Vedolizumab for Moderate-Severe Crohn's Disease: Results From the US VICTORY Consortium. Am J Gastroenterol. 2016;111(8):1147-1155. [PMID: 27301847]
-
Sandborn WJ, Feagan BG, Marano C, et al. Subcutaneous Golimumab Induces Clinical Response and Remission in Patients With Moderate-to-Severe Ulcerative Colitis. Gastroenterology. 2014;146(1):85-95. [PMID: 24462752]
-
Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369(8):699-710. [PMID: 23883890]
-
Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353(23):2462-2476. [PMID: 16339094]
-
Sandborn WJ, Su C, Sands BE, et al. Tofacitinib as Induction and Maintenance Therapy for Ulcerative Colitis. N Engl J Med. 2017;376(18):1723-1736. [PMID: 28467869]
Last Updated: 2026-01-06 | MedVellum Editorial Team Evidence Level: High (25 PubMed-indexed citations)
Frequently asked questions
Quick clarifications for common clinical and exam-facing questions.
When should I seek emergency care for ulcerative colitis?
Seek immediate emergency care if you experience any of the following warning signs: Stool frequency less than 6/day + systemic toxicity (Acute Severe Colitis), Abdominal distension + SBP less than 120 (Toxic Megacolon), Rigidity and guarding (Perforation), Massive rectal haemorrhage, Altered mental status in severe flare.
Learning map
Use these linked topics to study the concept in sequence and compare related presentations.
Differentials
Competing diagnoses and look-alikes to compare.
- Crohn's Disease
- Infective Colitis
- Ischaemic Colitis
Consequences
Complications and downstream problems to keep in mind.
- Colorectal Cancer
- Toxic Megacolon
- Venous Thromboembolism