EM · Procedural & diagnostic ED skills
Front-of-neck access and the emergency surgical airway
Also known as Emergency surgical airway · Cricothyroidotomy · Scalpel-bougie-tube cricothyroidotomy · Surgical cricothyroidotomy · Front-of-neck access · FONA · CICO rescue
Front-of-neck access in the ED — the scalpel-bougie-tube cricothyroidotomy for the cannot-intubate, cannot-oxygenate (CICO) event. The indication is the declared CICO state after every non-surgical lifeline (face mask, supraglottic airway, endotracheal tube) has failed. The anatomy is the cricothyroid membrane between the thyroid cartilage above and the cricoid ring below. The technique is the six-step sequence — laryngeal handshake, transverse stab incision through skin and membrane with a size 20 scalpel, turn the blade 90 degrees, pass the bougie caudally, railroad a size 6.0 mm cuffed endotracheal tube, confirm with sustained waveform capnography. The complications are bleeding, posterior tracheal wall injury, oesophageal injury, false passage and delayed tube displacement. The differential is the rescue oxygenation lifelines (face mask ventilation, supraglottic airway) and the alternative FONA technique (narrow-bore needle cricothyroidotomy with jet ventilation) — each distinguished by its place in the algorithm and its failure modes. ACEM Fellowship, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
3 MCQs with explanations
Target exams
Red flags
Related topics
- Upper airway obstruction in the emergency department
- The primary survey (ABCDE) — the trauma assessment framework
- Procedural sedation in the emergency department
- Local anaesthesia and topical agents
- Paediatric trauma — the modified approach
- Major trauma resuscitation — the team-based systematic approach
- Trauma team leadership
Front-of-neck access — FONA — is the emergency surgical airway performed through the anterior neck when every non-surgical route to oxygenate the patient has failed. It is the final common act of the difficult-airway algorithm and the one procedure in emergency medicine that cannot be deferred: once the cannot-intubate, cannot-oxygenate (CICO) state is declared, the brain has minutes of oxygen reserve, and the only route left to the trachea is through the front of the neck.[1][2] The Fellowship candidate must master three things an examiner will press — the indication (the declared CICO state, defined precisely), the technique (the scalpel-bougie-tube cricothyroidotomy, recited step-by-step), and the rationale for choosing the scalpel technique over the needle cricothyroidotomy that failed repeatedly in the national audits.[2] The procedure is rare — many emergency physicians will go a career without performing one on a patient — and precisely because it is rare it must be rehearsed until it is automatic, for the one occasion it is needed.[3][4]
Definition and the CICO endpoint

Front-of-neck access is the umbrella term for any surgical airway placed through the anterior neck — the surgical (open) cricothyroidotomy, the percutaneous dilational cricothyroidotomy, and the narrow-bore needle cricothyroidotomy with transtracheal jet ventilation. The technique specified by the contemporary difficult-airway algorithms for the adult is the scalpel-bougie-tube surgical cricothyroidotomy — a transverse stab through the cricothyroid membrane, a bougie railroaded into the trachea, and a cuffed endotracheal tube passed over the bougie.[1]
The indication is the cannot-intubate, cannot-oxygenate state, and the candidate must define it precisely because the threshold determines everything that follows. CICO is declared when the patient cannot be intubated by the best available laryngoscopist after the capped attempts (three best attempts per lifeline), and cannot be oxygenated by face mask, supraglottic airway, or endotracheal tube — the conjunction, not either alone. The saturation is falling, the apnoea is uncorrected, and the non-surgical lifelines are exhausted. A patient who is being oxygenated — however poorly — through a supraglottic airway is not yet a CICO; the surgical airway is reserved for the conjunction of failed intubation and failed oxygenation.[1][3]
The declaration of CICO is itself a named, examinable step. The clinician announces it aloud to the team — the verbal act that ends the perseverance with the upper airway and shifts the team to the surgical rescue, that assigns the operator who will perform the cricothyroidotomy, and that triggers the call for surgical and senior help. The recurring, avoidable failure of the 4th National Audit Project (NAP4) was that the surgical airway came too late: the teams persevered with a failing technique, attempted a needle cricothyroidotomy that failed and cost minutes, or simply did not declare the CICO while the saturation fell into the range from which death and brain injury follow.[2][3]
Indications
The indication is the declared CICO state in the adult. The clinical scenarios that produce a CICO in the emergency department cluster into a few recognisable patterns, and the candidate should be able to name them because the scenario shapes the preparation.[1][4]
Trauma is the commonest ED context: the maxillofacial trauma that distorts the upper airway and makes both intubation and mask ventilation impossible (the crushed larynx, the retropharyngeal haematoma, the severe facial burns that close the airway faster than expected), the penetrating neck injury with expanding haematoma, and the head-injured patient with blood and vomit in the airway and a cervical collar restricting laryngoscopy. Obstruction is the second pattern — the acute epiglottitis or deep neck space infection that occludes the glottis, the inhaled foreign body that cannot be retrieved, the angioedema or supraglottic oedema that closes the supraglottis, and the upper-airway tumour or haemorrhage. Can't intubate in the critically ill is the third: the physiologically difficult airway of the shocked, hypoxaemic or arrested patient who desaturates within seconds of induction, in whom repeated attempts at laryngoscopy traumatically swell the airway and convert a recoverable airway into a CICO.[3][4]
The unifying test across these scenarios is the same: every non-surgical lifeline has failed and the saturation is falling. The CICO is reached not as a single event but as the end of a spiral — each failed attempt desaturates the patient further, oedemas the tissues, and narrows the time to the next attempt — which is exactly why the algorithm caps attempts and why the disciplined early declaration is the sign the system is working rather than an admission of defeat.[1]
Contraindications
There is no absolute contraindication to performing an emergency surgical airway in the declared CICO state — the alternative to the cricothyroidotomy is death, and a contraindication that weighs against death is not a contraindication. The Fellowship answer to the contraindication question is therefore that the procedure has none in the genuine CICO; the candidate who lists contraindications in the CICO has misunderstood the indication.[1][2]
The relative considerations are the factors that change the technique or the timing, not the decision. Age is one: in the child (typically under 8 years, or under the age and size thresholds specified by the paediatric difficult-airway guidance) the cricothyroid membrane is small, the larynx is high and anterior, and the formal surgical cricothyroidotomy is technically harder — the narrow-bore needle cricothyroidotomy with jet ventilation remains the recommended paediatric rescue, recognising its own failure modes. Pre-existing laryngeal pathology is another: the patient with an obstructing laryngeal tumour, a crushed larynx, or an acute laryngeal infection may have anatomy that pushes the operator toward a formal tracheostomy rather than a cricothyroidotomy when time and expertise allow, though in the true CICO the cricothyroidotomy is still performed because it is faster. Coagulopathy and anticoagulation increase bleeding but do not defer the cut; the operator anticipates the bleeding and controls it once the airway is secure.[2]
The practical contraindication that the viva rewards is the one that distinguishes the CICO from the airway that is difficult but not lost: the patient who can still be oxygenated by any non-surgical route is not a CICO, and the scalpel is not yet indicated. The discipline is to declare the CICO the moment the threshold is crossed — neither too early (cutting a patient who could have been oxygenated) nor too late (the recurring fatal error).[1][3]
Relevant anatomy and landmarks
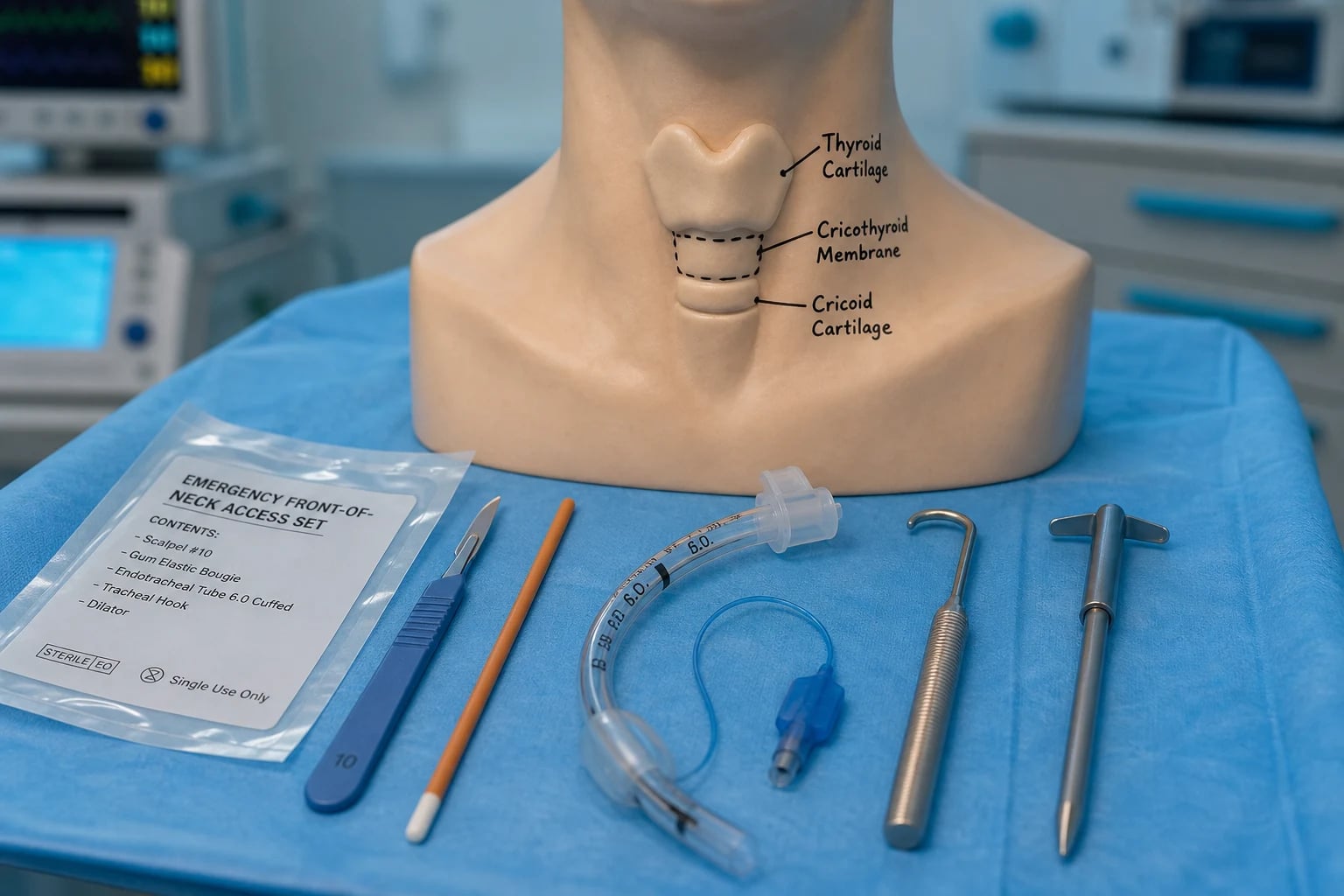
The cricothyroid membrane is the target of the surgical airway, and the candidate must describe its relations with the precision of a primary-viva anatomy answer. The membrane is a fibroelastic sheet stretching between the lower border of the thyroid cartilage above and the upper border of the cricoid cartilage below. It is subcutaneous and palpable in most adults, lying on average 1 to 2 cm below the laryngeal prominence (the Adam's apple), and it measures approximately 9 to 10 mm in vertical height and 22 to 30 mm in transverse width in the adult — the dimensions that govern tube size and that explain why a size 6.0 mm cuffed tube is the recommended default.[5]
The relations that matter surgically are three. The cricoid cartilage is the only complete ring of the trachea — the firm, circumferential landmark that is felt below the membrane and that anchors the lower edge of the target. The thyroid cartilage is the prominent, shield-shaped cartilage above, whose inferior border forms the upper edge of the membrane. The posterior tracheal wall is the structure most at risk: it is the membranous (non-cartilaginous) wall of the trachea, lying immediately behind the airway lumen, and the structure that the over-advancing scalpel, bougie or tube can perforate to enter the oesophagus.[2]
The vascular relations explain the bleeding complications. The cricothyroid artery runs transversely across the upper part of the membrane, a branch of the superior thyroid artery that anastomoses across the midline; a high transverse incision (too close to the thyroid cartilage) cuts it. The anterior jugular veins run longitudinally in the subcutaneous tissue lateral to the midline; a paramedian incision cuts them, which is why the incision is strictly midline. The isthmus of the thyroid gland overlies the second to fourth tracheal rings below the cricoid — relevant to the formal tracheostomy but below the cricothyroidotomy target. The recurrent laryngeal nerve ascends in the tracheo-oesophageal groove and is at risk in a lateral or deep dissection, though rarely injured in the midline stab.[2]
The laryngeal handshake is the landmark technique that identifies the membrane and stabilises the larynx in the midline. The non-dominant hand grasps the thyroid cartilage with the thumb and middle finger at its superior cornua and slides the index finger down the anterior surface to feel the soft depression between the prominent thyroid cartilage above and the firm cricoid ring below — that depression is the cricothyroid membrane. The handshake fixes the larynx (which is mobile and may be displaced in trauma or obesity), brings it forward in the obese neck, and maintains the midline so that the incision is true.[1]
Equipment — the CICO kit
The CICO kit is small, defined, and must be stored in a consistent marked location (a red bag or a marked drawer) so the team can find it under stress. The audit found kits were sometimes present but not found because storage was inconsistent; the modern standard is that the kit is brought to the bedside the moment the airway is recognised as difficult, not when the CICO is declared.[2][1]
The CICO kit — the minimum contents
The adjuncts support the technique. A tracheal hook may maintain the opening once the incision is made, lifting the thyroid cartilage cephalad and stabilising the tract for the bougie — useful when the tract tends to close. A Trousseau dilator may open the membrane, though the modern technique favours the bougie and the tube over the dilator, which is harder to place under stress. A size 6.0 mm cuffed tube is the default because it fits the cricothyroid membrane and is compatible with a standard bougie — the Cork cricothyroidotomy study confirmed that the optimum tube is the size that admits a standard bougie and that oversized tubes (7.5 or 8.0 mm) tear the membrane and the cricoid cartilage.[5] A surgical airway set (for the conversion to a formal tracheostomy once the patient is stable) and a synture tracheostomy or formal tracheostomy tray complete the kit for the definitive airway.[1]
The kit is checked on the routine equipment check, and the expiry of the single-use components is tracked. The DAS standard is that the kit and the technique are rehearsed in simulation so that, on the one occasion it is needed, the team performs it from memory — the simulation drills build both the procedural skill (the scalpel-bougie sequence on realistic tissue) and the non-technical skill (the declaration, the leadership, the communication) that determine the outcome.[1][3]
Patient preparation, positioning and consent
In the genuine CICO there is no time for formal consent — the procedure is performed under the emergency exception, and the candidate states this explicitly. Preparation is reduced to the seconds that buy the cut: oxygen left running at 100 per cent via whatever device is in place, suction on and within reach, the neck prepped if seconds allow (chlorhexidine or povidone-iodine, but not at the cost of delay), and the team briefed in a single sentence — "I am performing an emergency surgical airway, this is CICO."[1]
Positioning is the one preparation step that materially changes the technical success. Neck extension brings the larynx forward and the cricothyroid membrane closer to the skin, improving palpation and access — the head is extended on the neck, with a bolster under the shoulders if the anatomy allows and the cervical spine is not injured. In the trauma patient with a suspected cervical injury, manual in-line stabilisation is maintained but the neck is still extended as far as the stabilisation permits, because the trade-off favours the surgical airway over the cord. In the obese patient the membrane may be impalpable even in full extension — the larynx is buried in subcutaneous fat and falls posteriorly — and the preparation must anticipate the impalpable membrane with the vertical exploratory incision (described below).[3][4]
The consent conversation, when it is possible, is brief and honest: the procedure is life-saving, the alternative is death, the risks are bleeding, injury to the back of the trachea and the oesophagus, and the need for a later definitive airway. In the anticipated difficult airway (the planned front-of-neck access for the known obstructed airway) the consent and the preparation are fuller, and the local anaesthetic may be infiltrated if the patient is awake and time permits.[2]
Differential — the oxygenation lifelines versus the surgical airway
The first decision in the failing airway is not which surgical technique but whether the surgical airway is yet indicated — the differential is the set of non-surgical oxygenation lifelines that must be exhausted before the scalpel, and the alternative FONA technique that the modern algorithms have largely retired for the adult. The Fellowship candidate must distinguish each by its place in the algorithm and its failure modes, because reaching for the scalpel too early is an error, and reaching for a needle cricothyroidotomy in the obese adult is the error the audit documented.[1][2]
Two-person face mask ventilation (Plan C)
- The final non-surgical lifeline before the cut — oropharyngeal or nasopharyngeal airway, two-person jaw thrust, 100 per cent oxygen
- Oxygenation maintained even if intubation has failed; if adequate, STOP and wake or proceed, do not persist with repeated laryngoscopy
- Fails in the obese, the obstructed airway, the facial trauma — the scenarios that progress to CICO
- Not a surgical airway; the bridge that delays or avoids the cut
Supraglottic airway — i-gel, LMA Supreme (Plan B)
- The single best rescue attempt when intubation fails; second-generation devices seal better and protect against aspiration
- Oxygenates the majority of cannot-intubate situations; may serve as a conduit for fibreoptic intubation
- Fails in the distorted upper airway (oedema, tumour, blood, the closed glottis), the obese, and the high-pressure lung
- Not a definitive airway; a failed supraglottic attempt in the desaturating patient is the trigger to move to the cut
Scalpel-bougie-tube cricothyroidotomy (Plan D — the adult default)
- The DAS-specified adult default — transverse stab, bougie, size 6.0 mm cuffed tube
- Fast, works in the obese neck, provides a cuffed definitive airway that seals and protects
- Bleeding, posterior wall and oesophageal injury, false passage; technically demanding under stress
- Performed the moment CICO is declared; rehearsed in simulation until automatic
Needle cricothyroidotomy (narrow-bore cannula + jet ventilation)
- The historical adult default, now largely retired for the adult after NAP4
- Failed repeatedly in the obese — kinking, dislodgement, a cannula too short to reach the trachea; jet ventilation requires a patent upper airway for exhalation and causes barotrauma
- Retains a role in the paediatric airway (the small membrane, the high anterior larynx) as the recommended rescue
- Reaching for a needle set in the obese adult costs the time the brain cannot spare
The discriminating decision is oxygenation: a patient who can be oxygenated by face mask or supraglottic airway is not yet a CICO and the scalpel is not yet indicated, while a patient who cannot be oxygenated by any non-surgical route is a CICO and the scalpel is the act. The alternative FONA technique — the needle cricothyroidotomy — is distinguished from the scalpel-bougie technique by its failure modes in the adult (kinking, dislodgement, barotrauma, no cuffed airway) and by its retained role in the child, where the small cricothyroid membrane makes the formal surgical technique harder.[2][3]
Stepwise technique — the scalpel-bouogie-tube cricothyroidotomy

The technique is performed in a fixed six-step sequence, and the discipline is that each step is completed before the next is begun, with no improvisation and no deviation. The sequence is the DAS 2015 specification, rehearsed in simulation until it is automatic, and it is the technique the viva expects described step-by-step.[1][6]
The scalpel-bougie-tube cricothyroidotomy, in six steps
- Position and the laryngeal handshake. Extend the neck (if the cervical spine allows). With the non-dominant hand, grasp the thyroid cartilage with the thumb and middle finger and slide the index finger down to palpate the soft cricothyroid membrane between the prominent thyroid cartilage above and the firm cricoid ring below. This fixes the larynx in the midline and brings it forward. If the membrane is impalpable (the obese or traumatically distorted neck), make a vertical midline skin incision from the laryngeal prominence downward and palpate through the incision to find the membrane by feel — then proceed.
- Transverse stab incision through skin and cricothyroid membrane in a single motion, with a size 20 scalpel blade held vertically in the midline, advanced with a deliberate downward motion until it pops into the airway (a distinct give). The blade is kept in place to maintain the tract. In the impalpable neck, make the transverse membrane incision through the vertical skin incision, palpating the membrane with the non-dominant index finger.
- Turn the blade 90 degrees to open the tract, or insert a tracheal hook to lift the thyroid cartilage cephalad and stabilise the opening. Do not withdraw the blade before the bougie is placed — the tract is lost the moment the blade comes out.
- Pass the bougie caudally (toward the feet) through the incision, angled at 45 degrees, into the trachea. Confirm tracheal position by the characteristic tracheal clicks and a hold-up at the carina — the same confirmation used at laryngoscopy.
- Railroad a size 6.0 mm cuffed endotracheal tube over the bougie, through the incision and into the trachea, advancing gently to avoid tearing the membrane. The cuff is inflated with 5 to 10 mL of air. Remove the bougie. A size 6.0 mm tube is the default because it fits the cricothyroid membrane and admits a standard bougie — larger tubes (7.5 or 8.0 mm) tear the membrane and the cricoid cartilage.
- Confirm tracheal placement with sustained waveform capnography from the first breath — four to six rising traces confirm the tube is in the trachea, not a false passage. Ventilate with 100 per cent oxygen. Secure the tube, resuscitate the haemodynamics, and arrange the conversion to a formal tracheostomy once the patient is stable — the cricothyroidotomy is a rescue, not the definitive airway. [1]
The two structural errors are to withdraw the blade before the bougie is placed (the tract is lost) and to railroad an oversized tube that tears the membrane. The Cork cricothyroidotomy study established the equipment rationale — the optimum tube is the size that admits a standard bougie, and the size 6.0 mm cuffed tube with a compatible bougie is the pairing that the kit is built around.[5] The military comparison of two open surgical cricothyroidotomy techniques confirmed that the bougie-assisted technique is faster and more successful than the purely incision-and-dilation technique under stress, which is the evidence base for the modern default.[6]
Drug considerations and local anaesthesia
In the genuine CICO there is no time for pharmacology — the patient is arrested or imminently arrested, and the cut is performed without drugs. The drug considerations arise in two settings the viva may probe: the anticipated difficult airway in which the front-of-neck access is planned and prepared in advance, and the paediatric or awake patient in whom local anaesthesia is feasible if the airway is not yet lost.[1]
In the anticipated difficult airway, if the patient is awake and cooperative and the surgical airway is being performed electively (the known obstructing tumour, the planned conversion), local anaesthetic may be infiltrated. Lidocaine 1 per cent with adrenaline (3 mg/kg plain, 7 mg/kg with adrenaline, calculated before drawing up) is infiltrated subcutaneously over the cricothyroid membrane, with care to avoid intravascular injection and to stay within the weight-based maximum. The adrenaline produces vasoconstriction that aids the bloodless field, though it does not reduce the bleeding from the cricothyroid artery if the incision is too high. Topical anaesthesia of the tracheal mucosa (2 to 4 mL of lidocaine 4 per cent injected through the membrane into the trachea) blunts the cough reflex when the tube is passed.[1]
In the paediatric or the awake patient, ketamine (1 to 2 mg/kg intravenously) provides dissociative anaesthesia that preserves the airway reflexes, the tone and the blood pressure — the agent of choice when sedation is needed for an airway procedure in the haemodynamically compromised. The trap is that any sedation in the obstructed airway can precipitate complete obstruction — the sedationist must be ready to proceed to the surgical airway immediately if the airway is lost, and the surgical set must be open at the bedside before the sedative is given. In the genuine CICO, the rule is simple: oxygen on, suction on, scalpel in hand, no drugs.[2]
Why scalpel-bougie over needle cricothyroidotomy
The choice of the scalpel-bougie technique as the adult default is the single most important post-NAP4 change in the teaching of the front-of-neck access, and the viva expects the rationale set out in full. The needle cricothyroidotomy — a large-bore cannula inserted through the cricothyroid membrane and connected to a high-pressure jet ventilator — was for decades the taught technique, and the audit found that it failed repeatedly in the adult, and especially in the obese, in the very crisis it was meant to rescue.[2]
The mechanisms of the needle failure are the substance of the viva answer. The cannula kinks or dislodges — the rigid needle and the soft cannula bend at the membrane, and the ventilation is lost the moment the patient moves or the airway pressure rises. The cannula cannot be placed in the obese neck — the standard adult cannula is too short to reach the trachea through the thick subcutaneous fat, and the operator cannot confirm the intratracheal position. The jet ventilation requires a patent upper airway for exhalation — and the CICO state is, by definition, the state in which the upper airway is obstructed, so the jetted gas inflates the lungs but cannot escape, producing tension pneumothorax and subcutaneous emphysema in the very patient who can least tolerate it. And the needle provides no cuffed airway — it cannot seal the trachea against aspiration, and it cannot ventilate the high-pressure lung (the bronchospasm, the pulmonary oedema, the ARDS) that often accompanies the CICO.[2][1]
The scalpel-bougie-tube cricothyroidotomy answers each of these failures. The scalpel makes an incision that admits the bougie and the tube directly, and there is no cannula to kink or dislodge. The incision is through the skin and the membrane in one motion, and it works in the obese neck because the tract is created, not cannulated — the bougie and the tube follow the tract into the trachea regardless of the subcutaneous fat. The cuffed endotracheal tube provides a definitive airway that seals the trachea, protects against aspiration, and permits the high ventilating pressures the difficult lung requires. The success rate of the scalpel-bougie technique in the case series and the simulation literature is high, and the Australian emergency department experience confirmed that the open surgical technique is the one that succeeds when it is needed.[4][6]
The needle cricothyroidotomy retains a limited role in the paediatric airway, where the cricothyroid membrane is small and the formal surgical airway is technically harder, and the narrow-bore cannula is the recommended rescue in the child below the defined age or size threshold. It is not the adult default, and the candidate who reaches for a needle cricothyroidotomy set in the obese adult has not absorbed the post-NAP4 teaching.[1]
Complications
The complications are divided into the procedure-related (the immediate technical injuries) and the disease-related (the consequences of the hypoxic insult that preceded the cut).[2][4]
The immediate procedure-related complications begin with bleeding — the cricothyroid artery (a high incision), the anterior jugular veins (a paramedian incision) and the subcutaneous vessels all bleed, and the bleeding obscures the field at the worst moment. The prevention is the midline incision below the upper edge of the membrane, and the management is direct pressure and the rapid placement of the tube (which tamponades much of the bleeding once the cuff is inflated). Posterior tracheal wall injury is the over-advancing scalpel or bougie that perforates the membranous posterior wall into the oesophagus — the prevention is the controlled stab and the caudal, 45-degree angle of the bougie, and the consequence is the oesophageal injury that may need surgical repair. Oesophageal injury follows the posterior wall perforation and may present late as mediastinitis. False passage — the tube placed in the subcutaneous tissue or the pretracheal space rather than the trachea — is detected by the flat capnography trace and corrected by re-siting the tube through the tract. Tracheal and laryngeal injury (the torn cricoid cartilage, the fractured tracheal ring) follows the oversized tube or the forceful railroad, and may cause long-term stenosis.[2]
The delayed complications include tube displacement (the uncuffed or poorly secured tube that falls out), subglottic stenosis (the late sequel of the tube and the injury through the cricoid), infection of the wound, and the laryngeal damage that affects the voice and the swallow. The disease-related complications are the hypoxic brain injury, the aspiration pneumonitis, and the cardiovascular instability (the arrhythmia, the arrest) that followed the CICO itself — these are the consequences of the delay, and the reason the early declaration is the single most important determinant of outcome.[2][4]
The complications and their prevention
Pitfalls and practical tips
The pitfalls invert the structure, and the Fellowship candidate must name them because they are the recurring failures the audits found. Delaying the declaration of CICO while a fourth, hopeless laryngoscopy is attempted — the fixation error that the audit found most often, and the single most lethal error. Reaching for a needle cricothyroidotomy set in the obese adult — it fails (kinking, dislodgement, barotrauma) and costs the time the brain cannot spare. Making a blind transverse skin cut in the obese, impalpable neck — risks the anterior jugular veins and the wrong level; the vertical exploratory incision is the rescue. Withdrawing the blade after the stab, losing the tract before the bougie is placed. Railroading an oversized tube (a 7.5 or 8.0 mm) that tears the cricothyroid membrane and the cricoid cartilage. Failing to confirm with capnography — the chest that moves is not the trachea; a flat trace means a false passage.[2][3]
The practical tips are the mirror. Bring the CICO kit to the bedside the moment the airway is recognised as difficult — not when the CICO is declared. Use the laryngeal handshake to fix the larynx and identify the membrane. In the impalpable neck, make the vertical incision first and palpate through it. Keep the blade in, turn it 90 degrees, and railroad the bougie alongside it. Pass the bougie caudally at 45 degrees and confirm with clicks and hold-up. Use the size 6.0 mm cuffed tube — the size that fits the membrane and admits the bougie. Confirm with sustained waveform capnography from the first breath, four to six rising traces. Declare the CICO aloud, assign the operator, and call for surgical help — the verbal declaration that ends the perseverance and shifts the team to the rescue.[1][5]
The cognitive barrier is the human factor the training must overcome. The audit found that the teams did not fail the technique so much as they failed to move — the reluctance to abandon the upper airway, the cognitive tunnel of the failing laryngoscopy, the hope that one more attempt would succeed. The Vortex and the post-NAP4 teaching address this directly: the structured declaration, the assigned role, the rehearsed drill, and the explicit permission to perform the cut the moment the threshold is crossed. The simulation is the method that builds the muscle memory and the non-technical skill, and the Fellowship answer acknowledges that the cognitive readiness to cut is as examinable as the technique itself.[3]
Post-procedure care and disposition
Once the tube is placed and confirmed, the immediate priorities are to ventilate with 100 per cent oxygen, to resuscitate the haemodynamics (the CICO patient is typically hypoxic, hypercarbic and often cardiovascularly unstable — fluid, vasopressor and the correction of the metabolic acidosis), and to exclude the tension pneumothorax that may have developed from the obstructed airway or the jet ventilation if a needle was attempted first.[1]
The cricothyroidotomy is a rescue airway, not a definitive one, and the disposition is the conversion to a formal tracheostomy once the patient is stable and the surgical help is present. The timing of the conversion depends on the stability — the unstable patient is taken to theatre or the intensive care unit with the cricothyroidotomy in situ, and the conversion is performed when the physiology has recovered; the stable patient has the conversion performed semi-electively within 24 to 48 hours. The cricothyroidotomy is converted rather than left because the tube through the cricothyroid membrane risks subglottic stenosis (the cricoid is the narrowest part of the airway and the injured cricoid scars and narrows), and because the formal tracheostomy is more secure and more comfortable for the prolonged ventilation.[2]
The post-procedure monitoring is the full intensive-care set — continuous capnography, pulse oximetry, ECG and the blood pressure — and the observation for the delayed complications (the tube displacement, the bleeding, the infection, the mediastinitis of the oesophageal injury). The patient is admitted to the intensive care unit; the disposition from the emergency department is the resuscitation bay to theatre or to the ICU, never the ward. The handover to the receiving team includes the indication for the surgical airway, the technique used, the time of the cut, the confirmation method, and the plan for the definitive airway.[4]
Special populations
The child is the population in whom the technique diverges from the adult. The paediatric larynx is high and anterior, the cricothyroid membrane is small, and the formal surgical cricothyroidotomy is technically harder — the narrow-bore needle cricothyroidotomy with jet ventilation remains the recommended paediatric rescue, recognising its own failure modes (the same kinking, dislodgement and barotrauma, mitigated by the smaller cannula that fits the small membrane). The paediatric difficult-airway guidance specifies the age and size thresholds at which the surgical technique becomes the preferred rescue, and the Fellowship candidate states that the paediatric airway is managed with senior anaesthetic and ENT involvement from the outset, with the surgical airway prepared but the needle technique as the default in the younger child.[1]
The obese patient is the population in whom the adult technique is most tested. The thick subcutaneous fat buries the membrane, the larynx falls posteriorly, and the palpation that the technique depends on may fail — the vertical exploratory incision is the rescue, and the ultrasound identification of the membrane (where time and equipment allow, in the anticipated difficult airway) is the modern adjunct. The audit found the obese patient over-represented in the failed needle cricothyroidotomies, and the obese neck is the setting in which the scalpel-bougie technique most clearly outperforms the needle.[3][4]
The trauma patient brings the additional constraints of the cervical spine and the distorted anatomy. Manual in-line stabilisation is maintained, the neck is extended as far as the stabilisation permits, and the operator anticipates the blood, the oedema and the anatomical distortion. The penetrating neck injury with the expanding haematoma and the maxillofacial trauma with the distorted upper airway are the classic trauma CICO scenarios, and the surgical airway is performed with the understanding that the anatomy may not be the textbook anatomy. The pregnant patient at term is the physiologically difficult airway — the reduced functional residual capacity, the increased oxygen consumption and the engorged upper airway shorten the safe apnoea time and bring the CICO faster; the technique is unchanged, the preparation is earlier.[1]
Evidence and the regional guidelines
The contemporary framework rests on the Difficult Airway Society 2015 guidelines for the management of the unanticipated difficult intubation in adults, which specify the four-tier algorithm (Plans A through D) and the scalpel-bougie-tube cricothyroidotomy as the Plan D default, performed the moment the CICO is declared.[1] The evidence for the choice of technique comes from the 4th National Audit Project (NAP4) of the Royal College of Anaesthetists and the Difficult Airway Society, which documented the major complications of airway management and found that the needle cricothyroidotomy failed repeatedly in the adult (especially the obese), that the surgical airway came too late, and that capnography was repeatedly misused — the three lessons drawn directly into the modern algorithm.[2]
The Vortex approach of Chrimes and colleagues is the cognitive overlay that addresses the team and the human-factor dimension of the crisis — three lifelines (face mask, supraglottic airway, endotracheal tube) converging on a central CICO zone, each given a maximum of three best attempts, with the structured declaration and the move to the cut the moment the zone is reached. The "lost in transition" analysis of the cognitive barrier to moving from the upper airway to the neck is the contemporary addition to the post-NAP4 teaching — the recognition that the failure is often cognitive (the reluctance to move) rather than technical.[3]
The equipment evidence comes from the Cork cricothyroidotomy study, which established that the optimum tube size is the size that admits a standard bougie and that the size 6.0 mm cuffed tube is the default pairing — the oversized tube that does not fit the bougie or the membrane is the recurring equipment error.[5] The technique evidence comes from the military comparison of the open surgical cricothyroidotomy techniques, which confirmed the speed and the success of the bougie-assisted technique over the purely incision-and-dilation technique under stress.[6] The emergency department evidence comes from the Australian major trauma centre series, which described the real-world experience of the emergency surgical airway in the ED and confirmed that the open surgical technique is the one that succeeds when it is needed, and that the early declaration and the rehearsed drill are the determinants of the outcome.[4]
ANZ practice note. In Australian and New Zealand emergency departments, the front-of-neck access is taught and rehearsed as the DAS 2015 scalpel-bougie-tube cricothyroidotomy — the size 20 blade, the bougie, the size 6.0 mm cuffed tube, and the sustained waveform capnography. The CICO kit is a departmental stock item, stored in a consistent marked location and checked on the routine equipment check. The simulation programme is the method that maintains the skill, and the ACEM and the ANZCA jointly promote the structured difficult-airway training that builds both the procedural and the non-technical competence. The needle cricothyroidotomy is reserved for the paediatric airway; the adult default is the scalpel-bougie-tube. The conversion to the formal tracheostomy is the disposition once the patient is stable and the surgical help is present. [1]
SAQs — exam practice
SAQ — Declared CICO in the obese maxillofacial trauma patient
10 minutes · 10 marks
A 55-year-old obese man (BMI 38) is brought to the resuscitation bay after a high-speed motorcycle crash with severe maxillofacial trauma. He is bleeding from the mouth and nose with subcutaneous emphysema across the face and neck. Two experienced laryngoscopists have each made three best attempts at laryngoscopy — blood and distorted anatomy, no view (Cormack-Lehane grade 4). A size 4 i-gel and two-person face-mask ventilation with oropharyngeal and nasopharyngeal airways have failed to oxygenate: the chest does not move, the saturation is 72 per cent and falling, and he has bradyed to 42 bpm. The cricothyroid membrane cannot be palpated through the subcutaneous fat. You are the airway doctor.
SAQ — Scalpel-bougie-tube cricothyroidotomy: the technique and its pitfalls
10 minutes · 10 marks
A 40-year-old woman with known hereditary angioedema presents to the emergency department with rapid-onset stridor and tongue swelling after a dental procedure. Intramuscular adrenaline 0.5 mg, icatibant 30 mg subcutaneously and nebulised adrenaline 5 mg have been given without improvement. She is desaturating despite high-flow nasal cannulae at 60 L per minute and FiO2 of 1.0, and is becoming drowsy. After induction the saturations fall to 60 per cent, the larynx is completely obscured by oedema, neither intubation nor a supraglottic airway is possible, and CICO is declared. The cricothyroid membrane is palpable. You are performing the scalpel-bougie-tube cricothyroidotomy.
Exam pearls
- Define CICO precisely — cannot intubate (best laryngoscopist, three best attempts) AND cannot oxygenate (face mask, supraglottic airway, endotracheal tube) — the conjunction, not either alone.
- The declaration is a named, examinable step — announce it aloud, assign the operator, call for surgical and senior help; the recurring NAP4 failure was performing the cut too late.
- The six-step sequence — laryngeal handshake, transverse stab with a size 20 blade, turn the blade 90 degrees, pass the bougie caudally, railroad a size 6.0 mm cuffed tube, confirm with sustained capnography.
- The impalpable obese membrane — make a vertical midline skin incision to explore, palpate through it, then the transverse membrane cut; a blind transverse skin cut risks the anterior jugular veins and the wrong level.
- Why not needle — kinking, dislodgement, a cannula too short for the obese neck, jet ventilation against an obstructed upper airway causing barotrauma, and no cuffed airway; the needle retains a role in the child.
- Size 6.0 mm cuffed tube — the size that fits the cricothyroid membrane and admits a standard bougie; larger tubes tear the membrane and the cricoid cartilage.
- Confirm with sustained waveform capnography — chest movement alone is not confirmation; a flat trace means a false passage and mandates re-siting the tube.
- The cricothyroidotomy is a rescue, not a definitive airway — convert to a formal tracheostomy once the patient is stable, to avoid the subglottic stenosis of the injured cricoid. [1]
Red flags
[1]References
- [1]Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, Patel A, O'Sullivan EP, Woodall NM, Baker I; Difficult Airway Society intubation guidelines working group. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults Br J Anaesth, 2015.PMID 26556848
- [2]Cook TM, Woodall N, Frerk C; Fourth National Audit Project. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments Br J Anaesth, 2011.PMID 21447489
- [3]Chrimes N, Higgs M, Rehak A, Brindley PG, Auerbach M, Lagasse J, Kleiman-Adams C, Couper K, Gatward J, Blink F, Groombridge C, Anandan S, Utley R, Lynn-McHale D, Toft B, Kerry A, Nixon P, Nickson CP. Lost in transition: the challenges of getting airway clinicians to move from the upper airway to the neck during an airway crisis Br J Anaesth, 2020.PMID 32475685
- [4]Groombridge CJ, FitzGerald M, Sassen R, et al. Emergency surgical airway experience from an Australian major trauma centre emergency department Scand J Trauma Resusc Emerg Med, 2025.PMID 40506752
- [5]McCaul CL, O'Neill AF, Harney JF, Casey WF, Cashman J, O'Connor HM, O'Donoghue R, O'Loughlin C, O'Hora L, Harmon D, et al. Equipment for cricothyroidotomy: optimum tube size needs a compatible bougie. Comment on Br J Anaesth 2021; 127: 479-86 Br J Anaesth, 2021.PMID 34565521
- [6]Mabry RL, Nichols MC, Shiner DC. A comparison of two open surgical cricothyroidotomy techniques by military medics using a cadaver model Ann Emerg Med, 2014.PMID 24094476