EM · Paediatric resuscitation
The sick child and paediatric resuscitation
Also known as The sick child · Paediatric resuscitation · Paediatric cardiac arrest · Paediatric basic life support · Broselow tape
The sick child is any infant or child with actual or potential physiological failure, and paediatric resuscitation is the structured, weight-based response. Children differ from adults at every step: they compensate with a rising heart rate and intense vasoconstriction while the blood pressure holds, so hypotension is a late and pre-terminal sign; they consume oxygen at twice the adult rate and desaturate within seconds; and every drug, every fluid and every shock is dosed per kilogram, estimated with the Broselow tape or the formula weight equals age plus four times two. The structured approach is airway with cervical-spine control, breathing with oxygen and bag-valve-mask ventilation, then circulation with intra-osseous access, a 10 mL per kilogram fluid bolus and adrenaline 10 micrograms per kilogram. The paediatric arrest is usually asphyxial rather than cardiac, is managed with 15 to 2 cardiopulmonary resuscitation for two rescuers, the two-thumb encircling technique in the infant, and 4 joules per kilogram defibrillation, and runs through shockable and non-shockable loops that mirror the adult algorithm with weight-based doses. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Related topics
- Paediatric sepsis and septic shock (the septic child in the emergency department)
- Paediatric trauma — the modified approach
- Paediatric fever and serious bacterial illness (the febrile child in the emergency department)
- Neonatal emergencies (the sick neonate in the emergency department)
- Cardiac arrest and advanced life support
- Fluid resuscitation in the emergency department
The sick child is any infant or child whose physiology is failing or about to fail, and paediatric resuscitation is the structured, weight-based response that the Fellowship candidate must lead from the foot of the bed. Children are not small adults: they conceal decompensation until very late, they consume oxygen at twice the adult rate, and every intervention is dosed per kilogram of a weight that is often unknown. The examinable core is four things held together — a structured airway-breathing-circulation approach applied with cervical-spine control, weight-based dosing from the Broselow tape, the intra-osseous route when the veins collapse, and a paediatric arrest algorithm that is asphyxial in origin and uses 15 to 2 cardiopulmonary resuscitation. The 2020 American Heart Association paediatric guidelines and the 2024 International Liaison Committee on Resuscitation consensus are the two contemporary frameworks that govern this approach.[1][2]

Why the child differs — anatomy, physiology and pharmacology
The child differs from the adult in three examinable ways that change every decision at the bedside. Anatomically, the airway is anterior and the tongue is proportionally large, so the infant obstructs easily and the head must be in the neutral (not sniffing) position; the occiput is large, which flexes the neck in the supine child and is the reason a shoulder roll is used. The ribs are compliant and the intercostal muscles fatigue, so respiratory distress becomes respiratory failure quickly. Physiologically, cardiac output is heart rate multiplied by stroke volume, and the infant's stroke volume is fixed by a stiff, poorly compliant ventricle — so the only lever available to maintain output is heart rate, and the child compensates for shock with tachycardia and intense peripheral vasoconstriction rather than a rising stroke volume. Blood pressure is held normal until 25 to 30 per cent of circulating volume is lost, and hypotension is a late, pre-terminal sign. Oxygen consumption is roughly twice the adult rate per kilogram and the functional residual capacity is lower, so a child desaturates within seconds of apnoea — pre-oxygenation buys less time than in the adult, and bradycardia during intubation is hypoxia until proven otherwise.[1][2]
[1]Quantifying the differences — blood volume, body water, metabolic rate
The numbers anchor the clinical behaviour. A child carries a smaller absolute but larger weight-corrected blood volume: roughly 80 to 90 mL per kilogram in the infant against 70 mL per kilogram in the adult, so a 5-kg baby has only about 400 mL of circulating volume — a 100 mL haemorrhage is a 25 per cent loss and a disaster. Total body water is a larger fraction of body weight in the infant (around 75 per cent) than the adult (around 60 per cent), with a proportionally larger extracellular compartment that distributes fluid faster and is the basis of the higher maintenance requirement and the faster dehydration in gastroenteritis. The metabolic rate is roughly double the adult's per kilogram — oxygen consumption sits at 6 to 8 mL/kg/min in the infant against 3 to 4 mL/kg/min in the adult — and the functional residual capacity is low relative to that consumption, which is why an infant desaturates within 30 to 60 seconds of apnoea while a well-pre-oxygenated adult may hold several minutes. The infant kidney handles a large water and sodium load poorly (low glomerular filtration rate, low bicarbonate threshold), the immature liver conjugates drugs more slowly, and the large body-surface-to-mass ratio loses heat fast — a cold child becomes an acidotic, coagulopathic child, so active warming is part of the resuscitation. [1]
Airway & anatomy
- Tongue disproportionately large — fills the oropharynx, the commonest cause of soft-tissue obstruction in the unconscious infant
- Large occiput flexes the neck in supine — neutral position (or shoulder roll) opens the airway; "sniffing" is an adult concept
- Larynx high and anterior (C3–C4 in the infant vs C6 in the adult), epiglottis long and floppy — favour a straight (Miller) blade under 2 yr
- Narrowest point is the cricoid ring (not the vocal cords) below 8–10 yr — historically the rationale for an uncuffed tube; a cuffed tube now fits if cuff pressure is monitored under 20–25 cmH₂O
- Adenoidal tissue bleeds — avoid nasopharyngeal airways and nasal intubation in the small infant
Breathing & oxygen
- Compliant ribs + fatiguing intercostals — distress converts to failure in minutes; work of breathing is the key vital sign
- Lower FRC and double the metabolic rate — SpO₂ falls within 30–60 s of apnoea; pre-oxygenation buys less time
- Trachea short and straight — a main-stem (right) intubation is easily missed; confirm tube depth at the mid-trachea and verify with capnography
- Compliant chest wall — severe recession precedes hypoxia; the silent chest is pre-arrest
Circulation & volume
- Fixed stroke volume (stiff ventricle) — cardiac output is heart-rate-dependent; bradycardia = low output
- Intense vasoconstriction holds BP until 25–30% of volume lost — hypotension is pre-terminal
- Blood volume 80–90 mL/kg (infant) — a small absolute bleed is a large percentage loss
- Total body water ~75% of weight (infant) vs ~60% (adult) — faster distribution, faster dehydration, higher maintenance need
Neurology & metabolism
- Open fontanelle (to ~18 months) and sutures — raised ICP may bulge the fontanelle before papilloedema; head circumference is a vital sign
- Lower glycogen stores + higher metabolic demand — hypoglycaemia is common in the unwell child; check glucose early
- Immature thermoregulation + large surface area — hypothermia worsens acidosis and coagulopathy; actively warm
- Seizures may be subtle or febrile; the threshold for an ECG (to exclude SVT) in the tachycardic infant is low
Recognition of the sick child — PEWS and ABCDE
The Fellowship-level skill is not running the arrest but recognising the child forty-five minutes before it. Two tools do this work: the structured ABCDE primary survey, applied identically to the trauma and medical child, and the Paediatric Early Warning Score (PEWS), a track-and-trigger system that converts age-corrected vital-sign deviation into an escalating response. Neither replaces the senior clinician's gestalt — the "this child looks wrong" instinct — but both objectify it so a nurse or a junior doctor can trigger escalation without waiting for a code. The premise is that decompensation is rarely sudden; it travels a predictable trajectory of rising heart and respiratory rate, falling perfusion, and altered conscious level, and the deteriorating trajectory is visible in the vital signs long before the arrest.[7]
ABCDE — the primary survey applied to the child
The ABCDE framework is the universal discriminator: every step addresses the threat to life that kills first, and each step carries its own shortlist of immediately reversible causes. It is applied with cervical-spine control in the injured or unwitnessed-collapse child and is re-run after every intervention. [1]
ABCDE assessment of the deteriorating child
A — Airway (with cervical-spine control)
Assess patency: listen for stridor, gurgling, grunting; look for chest-wall and abdominal see-saw movement. Open with chin lift, or jaw thrust if cervical-spine injury is possible (never head-tilt). Insert an oropharyngeal airway (sized corner-of-mouth to angle-of-jaw) in the unconscious child; avoid nasopharyngeal airways in the infant (adenoidal bleeding) and in base-of-skull fracture. Suction blood, secretions, vomit and any foreign body. A child who can speak or cry has a patent airway — for now.
B — Breathing
Rate against age-corrected thresholds (over 60 in the neonate, over 40 in the toddler, over 30 in the school-age child); effort (recession, nasal flare, grunting, head bobbing); symmetry; and oxygenation. Give high-flow oxygen 15 L/min via a mask with reservoir to any child in distress or shock. Watch for the rising rate that then falls while effort rises — the exhausted child about to arrest. Support with bag-valve-mask ventilation if inadequate, one breath every 3–5 s raising the chest wall only.
C — Circulation
Heart rate against age (infant 160, pre-school 140, school-age 120 are upper normal); pulse quality (central vs peripheral); capillary refill (press the sternum, over 3 s is abnormal); skin colour and temperature (cool, mottled, prolonged refill = compensated shock); and blood pressure against 70 + (2 × age). Treat hypotension as pre-terminal. Two IV attempts or 90 s, then intra-osseous. Bedside glucose always.
D — Disability
AVPU (Alert, Voice, Pain, Unresponsive) as the rapid screen, paediatric GCS for the formal score; pupillary size and reactivity; posture (a stiff, extended, or asymmetric posture suggests raised ICP or a post-ictal state); and blood glucose — hypoglycaemia is silent, common and corrected with 5 mL/kg of 10% dextrose. A painful stimulus that the child localises is reassuring; one that it withdraws from or does not respond to is deterioration.
E — Exposure (with temperature control)
Fully expose to examine (the rash of meningococcaemia, the surgical abdomen, the missed injury), then re-cover and actively warm. Core temperature: hypothermia worsens acidosis, coagulopathy and mortality; hyperthermia raises intracranial pressure and is treated. Take the opportunity to weigh (or length-measure for the Broselow tape) and to look for the non-accidental injury.
PEWS — turning the vital signs into an escalation
The Paediatric Early Warning Score operationalises the ABCDE findings into a reproducible number. Variants exist — Bedside PEWS, the Royal College of Paediatrics PEWS, the Children's Early Warning Score — but all score the same domains against age-corrected thresholds: heart rate, respiratory rate, respiratory effort (or oxygen need), blood pressure, capillary refill, and conscious level. A rising score, or a single markedly deranged parameter, triggers a graded response — bedside review, senior review, and a paediatric alert or rapid-response team.[7] The validation literature shows that a high PEWS predicts paediatric intensive-care admission and in-hospital arrest hours in advance, and that routine PEWS recording reduces ward arrests; the score is therefore mandatory on every paediatric inpatient observation set, and the Fellowship candidate should be able to compute and interpret one at the bedside.
[1] [1]Weight estimation and equipment sizing
Every drug, fluid, and shock in paediatric resuscitation is weight-based, and the commonest source of error is the wrong weight. Estimate it at the moment the child arrives, before any drug is drawn up. The Broselow tape is the length-based reference standard: the child is laid flat alongside the colour-coded tape, and the colour zone at the heel gives the weight plus the drug doses, fluid volumes, and equipment sizes for that length. Its accuracy is good in the well-nourished child but drifts in obesity, and a human-factors comparison found the tape less error-prone than age-formula mental arithmetic under stress, which is why it remains the recommended bedside tool.[4][5] Where the tape is unavailable, the age-formula weight applies to the child aged one to ten years: weight in kilograms equals age plus four, times two. A 3-year-old is therefore 14 kg, a 6-year-old 20 kg. The cuffed endotracheal tube is now standard in the infant and child over 28 days and over 3 kg, sized at the internal diameter equal to age divided by four plus four millimetres. The intra-osseous needle is sized to the patient (15 gauge for the infant, 15 gauge proximal tibia), and the laryngoscope blade is straight (Miller) in the infant under two and curved (Macintosh) in the older child.[1]
The weight-formula toolbox — and where each breaks down
No weight estimation is perfect; the Fellowship candidate should know three formulae and where each fails. The classic APLS formula weight = (age + 4) × 2 holds well from 1 to 10 years in well-nourished children but, as Luscombe and Owens showed, increasingly underestimates the modern (heavier) child above 5 years, which is why the updated Luscombe–Owens formula — weight = (age × 3) + 7 for 6-to-12-year-olds — was derived.[8] The Best Guess formula (Australian, age-segmented) performs better in overweight cohorts, and the Broselow tape is the most robust bedside tool but drifts in the obese or very tall child and in non-Caucasian populations where body habitus differs. The pragmatic answer in the resus bay is to cross-check two methods — Broselow tape plus an age formula — and to use the higher estimate when they diverge, because underdosing a resuscitation drug is generally more dangerous than a slight overdose, with the critical exception of adrenaline where precision matters most. When the parents are present, a recently documented weight (outpatient, clinic, or parental estimate for a child under one) is more accurate than any formula and should be sought.[4][8]
(age + 4) × 2
- The classic APLS formula for 1–10 yr — a 4-yr-old is 16 kg, a 6-yr-old is 20 kg
- Easy mental arithmetic under stress; the default when the Broselow tape is unavailable
- Underestimates the modern heavier child above ~5 yr — the reason Luscombe–Owens superseded it for older children
- Fails in the under-1 (use ½ × [age in months + 9] / 2 for infants, or a parental/clinic weight)
(age × 3) + 7 (Luscombe–Owens)
- The updated formula for the 6–12-yr-old — better fit for the modern, heavier child
- Derived because the old APLS formula under-estimated in this age band
- A 6-yr-old is 25 kg, a 9-yr-old is 34 kg — the recalibration is clinically meaningful for drug dosing
- Use the Broselow tape as the cross-check; both are estimations, neither replaces a true weight when available
Broselow tape
- Length-based colour-coded tape — the bedside reference standard; gives weight, drugs, fluids and equipment in one read
- Least error-prone under stress in human-factors studies; standard in every Australasian resus bay
- Drifts in obesity (under-estimates) and in very tall, thin children (over-estimates)
- Cross-check with an age formula when the two diverge — the larger estimate is usually safer for fluids and most drugs
Parental / documented weight
- For the under-1, a parental estimate or a recent clinic weight is the most accurate of all
- A known weight always supersedes an estimate — ask the carer if the child is known to the service
- Beware the outdated chart weight in a child who has lost or gained fluid rapidly
- Document the source of the weight (tape, formula, parental) on the drug chart so the team can re-check
Luscombe & Owens — the ageing APLS formula (Arch Dis Child 2007)
Archives of Disease in Childhood
PMID 17213259
Key finding
A retrospective review of 100,003 children aged 1–16 weighing them against the then-current APLS formula (age + 4) × 2. The formula under-estimated weight by a mean of 18.8 per cent in 10-year-old girls and 6.9 per cent in 5-year-old boys, with the discrepancy worsening steadily with age — the modern child is heavier than the formulae assumed.
Practice change
Demonstrated that the classic weight formula had drifted with secular trends in childhood body habitus, and provided the updated (age × 3) + 7 formula for older children — a reminder that the dose is only as good as the weight it is built on.<Cite id='8' />
The structured approach — airway with cervical-spine control
The structured approach is airway, breathing, circulation, disability, exposure, applied in that order because each step addresses the threat to life that kills first, with cervical-spine control maintained throughout in the injured or unwitnessed-collapse child. Airway is assessed for patency and opened with gentle airway manoeuvres — chin lift or jaw thrust if cervical-spine injury is possible, never head-tilt. An oropharyngeal airway, sized from the corner of the mouth to the angle of the jaw, is inserted in the unconscious child; a nasopharyngeal airway is avoided in the infant (the adenoids bleed) and in any suspected base-of-skull fracture. Suction the blood, secretions and vomit. If the airway cannot be maintained, a definitive airway is required — bag-valve-mask ventilation is the bridge, and rapid sequence intubation with a cuffed tube and a cardiovascular-stable induction (ketamine 1 to 2 mg per kilogram with rocuronium 1 mg per kilogram) is the definitive act. Manual in-line stabilisation of the cervical spine is held throughout, and the child is log-rolled only when the spine is cleared or imaging is needed.[1]
[1]The definitive airway — cuffed or uncuffed tube, and why it changed
Tube selection is a perennial exam question because the teaching has shifted. The traditional APLS teaching was an uncuffed endotracheal tube for the child under eight (some texts, under ten) years, on the grounds that the cricoid ring is the narrowest part of the paediatric airway (the adult narrowest point is the glottis), so a tube that passes the cords fits the cricoid snugly without a cuff — and a cuff at the subglottic cricoid risks mucosal ischaemia and subsequent subglottic stenosis. Modern practice has moved to the cuffed tube as standard in the infant over 3 kg and the older child, including in resuscitation, on the evidence that cuffed tubes reduce leak, reduce the need for tube exchange, lower the rate of reintubation, and do not increase post-extubation stridor provided cuff pressure is monitored and kept below 20 to 25 cmH₂O.[1] The examinable reconciliation is: a cuffed tube is acceptable and now preferred in the resuscitation setting, but the cuff pressure must be checked — an unmonitored, over-inflated cuff in a child is the harm the old teaching protected against. The tube internal diameter follows the formula age/4 + 4 mm (e.g. 4 mm at 1 yr, 5.5 mm at 6 yr, 6.5 mm at 10 yr), with a tube one half-size larger and one half-size smaller available at the bedside. A straight (Miller) blade is used under two years (the long, floppy epiglottis is lifted directly), and a curved (Macintosh) blade above.
Uncuffed tube (traditional)
- Historical APLS default for the under-8 (or under-10) child — the cricoid is the narrowest point and self-seals
- No cuff-pressure monitoring needed; no risk of cuff-induced subglottic ischaemia
- Higher leak, more tube exchanges, higher reintubation rate than cuffed in modern series
- Still preferred in the neonate and small infant under 3 kg, and in units without cuff manometers
Cuffed tube (modern standard)
- Now standard in resuscitation for the infant over 3 kg and the older child — reduced leak, fewer exchanges, lower reintubation
- Mandatory cuff-pressure monitoring — keep under 20–25 cmH₂O to avoid subglottic mucosal ischaemia and later stenosis
- Particularly valuable in poor lung compliance (ARDS, pneumonia) where an adequate tidal volume demands an airtight seal
- Size by age/4 + 4 mm ID; have a half-size up and a half-size down ready
Breathing, oxygen and bag-valve-mask ventilation
Breathing is assessed for rate, effort, symmetry and oxygenation against age-corrected thresholds — a respiratory rate above 60 in the neonate, above 40 in the toddler, above 30 in the school-age child is abnormal, as is a rising rate that then falls while effort increases (the exhausted child about to arrest). Look for the recession, the grunt, the nasal flare and the head bobbing. High-flow oxygen is given to any child in respiratory distress or shock via a mask with a reservoir at 15 litres per minute, because a normal saturation in a working child does not exclude the early desaturation that follows. When breathing is inadequate, bag-valve-mask ventilation is the immediate rescue: a correctly sized mask sealing nose and mouth, the one-hand C-E grip, a slow squeeze delivering a tidal volume that just raises the chest wall, at 12 to 20 breaths per minute (one breath every three to five seconds) for the apnoeic or inadequately breathing child. Avoid gastric insufflation — cricoid pressure is not routine in paediatric basic life support, and orogastric decompression follows intubation. Pre-oxygenase for three minutes where possible, but accept that a child desaturates within 30 to 60 seconds and move quickly. Treat the reversible respiratory causes as they are found — a bronchodilator for the wheeze, adrenaline for the croup or anaphylaxis, a dextrose for the hypoglycaemic seizure.[1][2]
Circulation, intra-osseous access and fluid resuscitation
Circulation is assessed from the heart rate, the pulse quality, the capillary refill, the skin colour and temperature, and the blood pressure interpreted against the age-corrected threshold. A systolic blood pressure below 70 plus twice the age in years for a child under ten, or below 90 for the child over ten, defines hypotension — but by the time the pressure falls the child is already in decompensated, pre-arrest shock, so recognise the compensated phase first from the tachycardia, the mottled cool skin, the capillary refill over three seconds and the altered conscious level. Establish intravenous access early and deliberately: two attempts or 90 seconds, and if they fail, place an intra-osseous needle without further delay in the proximal tibia, distal femur or proximal humerus — the intra-osseous route delivers drugs, fluid and blood as effectively as a central line and is the standard paediatric rescue access. Send the bloods through the first line, including a bedside glucose. The fluid bolus is 10 mL per kilogram of a balanced crystalloid (Hartmann's or Plasma-Lyte) over five to ten minutes, reassessed against the heart rate, the capillary refill, the blood pressure, the conscious level and the liver size before any repeat; titrate up to 40 to 60 mL per kilogram in the first hour in shock, stopping at the first sign of overload — hepatomegaly, a gallop, a rising work of breathing. Adrenaline 10 micrograms per kilogram intravenously or intra-osseously (0.1 mL per kilogram of 1 in 10,000) is the shock dose for symptomatic bradycardia and refractory shock, and it is given while the reversible cause is sought.[1]
The weight-based resuscitation doses
Fluid resuscitation — the bolus, the volume, and the FEAST warning
The fluid bolus is weight-based, but the volume is aetiology-dependent, and the Fellowship candidate must hold three numbers. The standard APLS bolus is 20 mL/kg of a balanced crystalloid (Hartmann's or Plasma-Lyte) for uncomplicated shock, given over 5 to 10 minutes and reassessed against heart rate, capillary refill, blood pressure, conscious level and liver size before any repeat, titrating up to 40 to 60 mL/kg in the first hour and stopping at the first sign of overload — hepatomegaly, a gallop, a rising work of breathing. In septic shock, many protocols use cautious 10 mL/kg aliquots after the FEAST trial demonstrated excess mortality with aggressive bolus fluid in resource-limited African children with severe infection — a finding tempered by the differing resource setting but enough to mandate reassessment between every bolus and a low threshold for early vasoactive support rather than escalating fluid.[6] In suspected cardiogenic shock (the gallop, the hepatomegaly, the myocarditic infant), the aliquot is 5 mL/kg — a full 20 mL/kg bolus precipitates pulmonary oedema. Blood products for haemorrhagic shock are given at 10 to 20 mL/kg of packed red cells, or a paediatric massive-transfusion ratio of red cells to plasma to platelets approximating whole blood. The discipline is the same in all three: titrate, reassess, and stop at overload.[1][6]
FEAST — fluid bolus increased mortality in African children with severe infection (NEJM 2011)
New England Journal of Medicine
PMID 21615299
Key finding
A randomised controlled trial of 3,141 children with severe febrile illness and impaired perfusion in resource-limited African centres, comparing bolus albumin or saline against no bolus (maintenance only). Fluid bolus increased 48-hour mortality from 6.2 per cent (no bolus) to 10.6 per cent (albumin) and 10.5 per cent (saline) — an absolute excess of around 4 percentage points, largely from cardiovascular collapse.
Practice change
The most influential paediatric resuscitation trial of the decade. It did not abolish fluid boluses in well-resourced septic shock, but it changed the culture from large blind boluses to cautious, reassessed aliquots (10 mL/kg), an early vasoactive agent, and an intolerance of fluid overload. The lesson is generalisable: titrate every bolus against the perfusion signs, and do not chase a number.<Cite id='6' />
Differential diagnosis — the deteriorating child
The differential in the deteriorating child is generated through the structured approach rather than at the end of it, because each letter of the primary survey carries its own shortlist of immediately reversible causes. The Fellowship candidate must hold the common and the dangerous causes simultaneously and treat as the search proceeds. [1]
Sepsis
- The leading medical cause of paediatric decompensation — fever or hypothermia, tachycardia, mottled skin, prolonged capillary refill, altered conscious level
- Recognise from the Phoenix criteria and the perfusion signs; the blood pressure holds until late
- Fluid 10 mL/kg titrated, ceftriaxone 50 to 75 mg/kg within the hour, adrenaline for refractory shock
- The archetype of the decompensating medical child — see the dedicated paediatric sepsis topic
Lower respiratory failure
- Bronchiolitis, asthma, pneumonia — the rising respiratory rate that then falls with rising effort signals exhaustion and impending arrest
- Wheeze, recession, grunting, hypoxia; the silent chest in asthma is pre-arrest
- Oxygen, bronchodilator, escalation to high-flow nasal cannula, non-invasive ventilation or intubation before collapse
- A child who is tiring is intubated before the arrest, not after it
Upper airway obstruction
- Croup, epiglottitis, bacterial tracheitis, foreign body — stridor, drooling, tripoding, the toxic-looking child
- Inspiratory stridor at rest, recession, the sitting-forward posture
- Keep the child calm, nebulised adrenaline for croup, humidified oxygen, avoid upsetting the epiglottitic child, senior airway help
- Croup and anaphylaxis are the two reversible causes to treat in the first minute
Anaphylaxis
- Sudden onset after an allergen — urticaria, angioedema, stridor, wheeze, hypotension
- Biphasic; a history of allergy, food, drug or sting
- Adrenaline 10 micrograms per kilogram intramuscularly (0.01 mL/kg of 1 in 1,000), fluid, repeat adrenaline every five minutes
- A shocked child with a rash is not always sepsis — the timing and the urticaria distinguish anaphylaxis
Cardiogenic / arrhythmia
- Myocarditis, congenital heart disease, supraventricular tachycardia — a gallop, hepatomegaly, a heart rate above 220 in the infant with no variability
- SVT is a fixed narrow-complex tachycardia; a febrile infant at 240 is SVT until proven otherwise
- Cautious 5 mL/kg fluid aliquots in suspected cardiogenic shock, vagal manoeuvres then adenosine 100 mcg/kg for SVT
- A bolus in cardiogenic shock causes pulmonary oedema — examine for the gallop first
Metabolic — hypoglycaemia and DKA
- Hypoglycaemia is common in the unwell child and causes altered conscious level and seizures; DKA causes dehydration, acidosis and altered mentation
- Check the bedside glucose in every sick or seizing child
- 5 mL/kg of 10 per cent dextrose for hypoglycaemia; the DKA pathway with careful fluid and insulin for acidosis
- Never attribute altered conscious level to a behavioural cause until the glucose is checked
Investigations in parallel with resuscitation
Investigations run in parallel with — never before — the airway, the oxygen and the first fluid bolus, and the single most important bedside test is the glucose. A point-of-care glucose is checked in every sick, seizing or arrested child, because hypoglycaemia is common, dangerous and easily corrected with 5 mL per kilogram of 10 per cent dextrose. A venous or capillary blood gas gives the immediate lactate, the pH and the base deficit, and a rising lactate after fluids predicts mortality; the gas also screens the potassium, the sodium and the haemoglobin. A full blood count, CRP, electrolytes, liver function and coagulation are drawn when a line is available; blood cultures are taken before the antibiotic whenever they do not delay it, and a urinalysis is obtained by catheter or suprapubic aspirate, never by bag, in the unwell child. A chest radiograph is taken for respiratory signs or an occult source. The paediatric early warning score operationalises the vital-sign deviation into a track-and-trigger escalation, and a child who triggers on two or more age-corrected vital signs is presumed sick until the workup proves otherwise. The lumbar puncture is deferred — never the antibiotic — in the shocked or comatose child and performed once resuscitated.[1]
The paediatric cardiac arrest algorithm
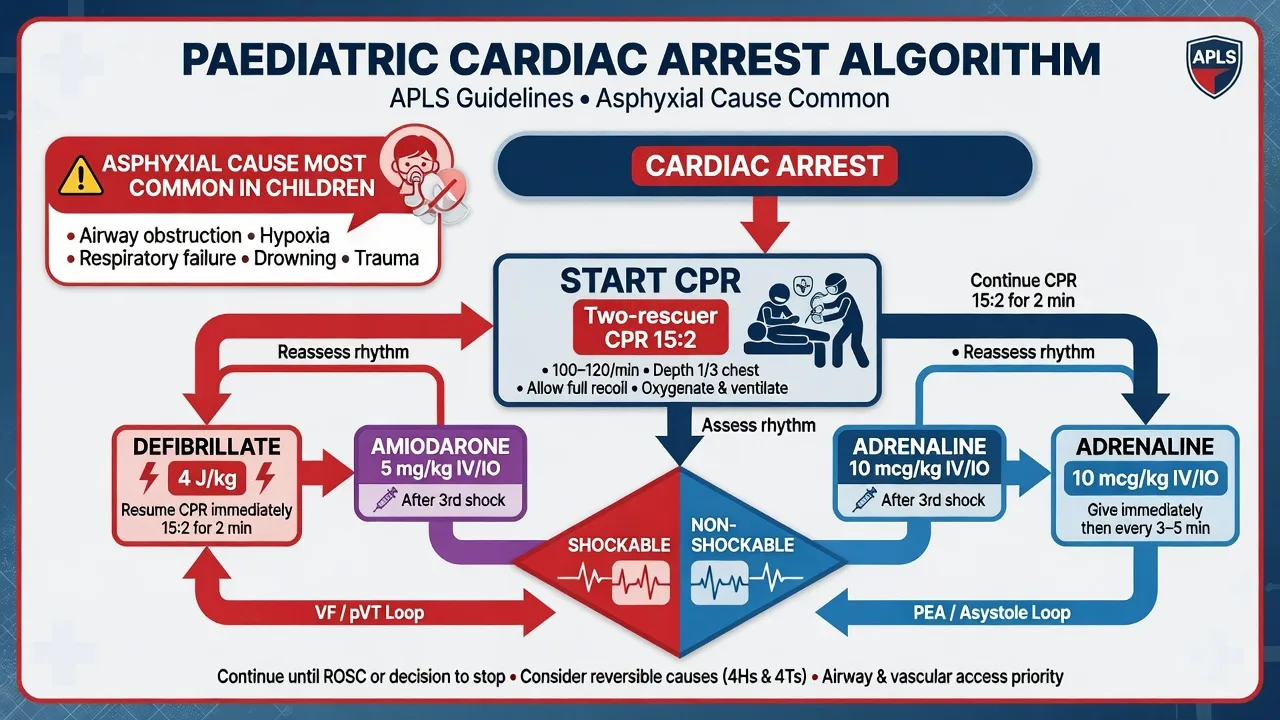
The paediatric cardiac arrest algorithm runs through two loops — shockable (ventricular fibrillation or pulseless ventricular tachycardia) and non-shockable (asystole or pulseless electrical activity) — built around two-minute cycles of high-quality cardiopulmonary resuscitation with a rhythm analysis and a drug at each cycle, identical in structure to the adult algorithm but with paediatric ratios, depths and doses. The arrest in a child is overwhelmingly asphyxial in origin — a primary cardiac cause accounts for less than ten per cent — which is why ventilations are central, why the ratio is 15 to 2 for two rescuers, and why the outcome turns on early oxygenation as much as on compressions.[1][3]
Why the arrest is asphyxial — the cause profile
The aetiology of paediatric cardiac arrest is the single most important departure from adult resuscitation, and it drives every ratio, dose and priority in the algorithm. In the adult, the arrest is overwhelmingly primary cardiac — an ischaemic arrhythmia in a diseased myocardium — and compression-only CPR works because the heart still holds oxygenated blood. In the child, the arrest is overwhelmingly asphyxial or circulatory — the heart is healthy and stops only after progressive hypoxia, hypercarbia and acidosis have exhausted the myocardium — so the oxygen reservoir is depleted at the moment of arrest and ventilations are essential. The common causes, in descending frequency, are SIDS and apparent life-threatening events (ALTEs), drowning and submersion, foreign-body airway obstruction (choking), severe sepsis, lower-airway respiratory failure (severe asthma, bronchiolitis, pneumonia), and trauma; primary cardiac causes (cardiomyopathy, myocarditis, congenital-heart-disease arrhythmia, commotio cordis, the inherited channelopathies) account for fewer than ten per cent, but they are the subgroup in which a shockable rhythm appears and early defibrillation is decisive.[1][3]
SIDS / ALTE
- Peak age 2–4 months; the archetypal out-of-hospital infant arrest
- Cause of death unexplained after investigation, but most "near-miss" events in the ED are an unrecognised infection (sepsis, RSV), a metabolic disorder, or non-accidental injury — investigate, do not assume SIDS
- Resuscitate per the paediatric algorithm; a sub-sample of apparent SIDS has a treatable cause found only on workup
Drowning / submersion
- The second commonest paediatric arrest cause; hypoxia is the mechanism, primary cardiac is rare
- Five initial rescue breaths then 15:2 CPR; prolonged resuscitation and rewarming are warranted — the cold, hypoxic submerged child may recover after a long arrest ("they are not dead until warm and dead")
- Cervical-spine precautions in a diving injury; check glucose (cold children run low)
Foreign-body obstruction (choking)
- A leading cause of death in the toddler — nuts, grapes, coins, balloons; the obstruction is silent, not the noisy choking of films
- If conscious: back blows, chest thrusts (infant) or abdominal thrusts (child); if unconscious: CPR, look in the mouth before each breath, Magill forceps under direct vision — never blind finger sweeps
- A high index of suspicion in the sudden, witnessed collapse of a previously well toddler eating or playing with small objects
Severe sepsis
- Progressive shock, cold mottled peripheries, then a bradycardic, asystolic or PEA arrest
- The arrest is the end of unrecognised or under-resuscitated shock — fluid, early adrenaline (vasoactive, not just arrest dose), and antibiotics are simultaneous with the algorithm
- Meningococcaemia, pneumococcal sepsis, and the immunocompromised host are the dangerous subgroups
Trauma
- Hypovolaemic, obstructive (tension pneumothorax, tamponade), or neurogenic (catastrophic brain injury) — primary cardiac arrest is uncommon
- Adrenaline is not routinely effective in the hypovolaemic traumatic arrest; control the catastrophic haemorrhage, splint, decompress, and transfuse early in the paediatric massive-transfusion ratio
- A traumatic paediatric arrest has a poor prognosis but survivable causes (tension pneumothorax, hypovolaemia) must be sought and corrected
Primary cardiac (rare)
- Under ten per cent of paediatric arrests — cardiomyopathy, myocarditis, congenital-heart arrhythmia, commotio cordis, the channelopathies (long-QT, CPVT)
- The subgroup in which VF or pulseless VT is the presenting rhythm — early defibrillation at 4 J/kg is decisive
- A family history of sudden death or a prolonged QT on the post-arrest ECG prompts the inherited-channelopathy workup
Dispatcher-assisted conventional CPR — better neurological outcome in children (JAHA 2014)
Journal of the American Heart Association
PMID 24785780
Key finding
A population-based observational study of paediatric out-of-hospital cardiac arrests comparing dispatcher-assisted conventional CPR (compressions plus rescue breaths) against dispatcher-assisted compression-only CPR. Conventional CPR was associated with significantly better one-month favourable neurological outcome, particularly in the asphyxial (non-cardiac) arrests that dominate the paediatric population.
Practice change
The clinical-justification evidence for the 15:2 ratio and the priority given to ventilations in paediatric arrest — unlike the adult, where compression-only is equivalent or superior, the child's arrest is oxygen-driven and conventional CPR with breaths saves brains.<Cite id='9' />
Cardiopulmonary resuscitation. The compression-to-ventilation ratio is 15 to 2 for two rescuers and 30 to 2 for a single rescuer, reflecting the asphyxial aetiology: the child needs more breaths than the adult because the arrest was oxygen-driven. Compressions are delivered at 100 to 120 per minute to a depth of at least one-third the anteroposterior diameter of the chest — roughly 4 centimetres in the infant and 5 centimetres in the child — with full recoil between compressions and minimal interruption (pauses kept below five seconds and confined to the rhythm check and the shock). The two-thumb encircling hands technique is used for the infant when two rescuers are present, the rescuer's hands encircling the chest and compressing the lower third of the sternum; it generates higher systolic pressure and more consistent depth than the two-finger technique and is the recommended method. The compressor is rotated every two minutes to prevent fatigue. [1]
Shockable rhythms — VF and pulseless VT. Defibrillate immediately at 4 joules per kilogram, resume cardiopulmonary resuscitation for two minutes without pausing for a pulse check, then reassess. If VF or pVT persists, repeat the shock at 4 joules per kilogram and resume; after the third shock, give adrenaline 10 micrograms per kilogram (0.1 mL per kilogram of 1 in 10,000) intravenously or intra-osseously every three to five minutes and amiodarone 5 mg per kilogram, with a second amiodarone dose after the fifth shock if needed. The cycle continues until a perfusing rhythm returns or the resuscitation is stopped. [1]
Non-shockable rhythms — asystole and PEA. These are managed with continuous cardiopulmonary resuscitation, adrenaline 10 micrograms per kilogram every three to five minutes, and an unremitting search for a reversible cause. PEA in a child is almost always a manifestation of a reversible cause — hypoxia, hypovolaemia, hypoglycaemia, hypothermia, tension pneumothorax, tamponade, toxins or thrombosis — and bedside ultrasound during the rhythm check is invaluable. Asystole carries the worst prognosis but may still reflect a correctable profound hypoxia.[1][2]
[1]Definitive resuscitation drugs and doses
The paediatric resuscitation drugs are the adult drugs at weight-based doses, and the candidate who reaches for the adult ampoule will overdose the child. Adrenaline is the workhorse: 10 micrograms per kilogram intravenously or intra-osseously (0.1 mL per kilogram of 1 in 10,000) every three to five minutes in the arrest and for symptomatic bradycardia, and 10 micrograms per kilogram intramuscularly (0.01 mL per kilogram of 1 in 1,000) for anaphylaxis, repeated every five minutes. Amiodarone 5 mg per kilogram is given for refractory VF or pulseless VT after the third shock (a second dose after the fifth); lidocaine 1 mg per kilogram is the alternative. Fluid is 10 mL per kilogram of balanced crystalloid reassessed after each bolus for shock, with blood products at 10 mL per kilogram for haemorrhagic shock. Dextrose — 5 mL per kilogram of 10 per cent dextrose — treats hypoglycaemia, which must be checked and never assumed. Sodium bicarbonate 1 mL per kilogram of 8.4 per cent is reserved for hyperkalaemia or the tricyclic-antidepressant arrest, not given routinely. The rapid sequence induction for the intubated sick child uses ketamine 1 to 2 mg per kilogram or propofol 2 to 4 mg per kilogram (reduced in shock) with rocuronium 1 mg per kilogram or suxamethonium 1.5 mg per kilogram, with a fluid bolus or vasopressor running because induction in the shocked child drops the pressure. The weight-based chart, the Broselow tape, and the printed drug card exist to prevent the dosing error that is the commonest cause of paediatric drug-related harm.[1][4]
Model answer — a 6-year-old, 20 kg child arrests into ventricular fibrillation
A 6-year-old, 20 kg child collapses in the resuscitation bay and the monitor shows ventricular fibrillation. Call the arrest team, start cardiopulmonary resuscitation at 15 to 2 with the two-thumb encircling technique (the child is small enough for an encircling approach if the compressor's hands fit; otherwise the heel of one hand at the lower sternum), compress at 100 to 120 per minute to a depth of 5 centimetres. Attach the defibrillator and deliver the first shock at 4 joules per kilogram — 80 joules biphasic. Resume cardiopulmonary resuscitation immediately for two minutes without a pulse check, then reassess the rhythm. If VF persists, repeat the shock at 4 joules per kilogram. After the third shock, give adrenaline 10 micrograms per kilogram — 200 micrograms (2 mL of 1 in 10,000) intravenously or intra-osseously — every three to five minutes, and amiodarone 5 mg per kilogram — 100 mg — intravenously. Establish intra-osseous access if the intravenous route is not secured within 90 seconds. Search for and treat the cause at every cycle — in a child, hypoxia, hypovolaemia and the arrhythmogenic cardiomyopathy or congenital heart lesion are high on the list. Treat the bedside glucose. [1]
Differences from the adult — the Fellowship answer
The Fellowship examiner rewards a candidate who can articulate, point by point, how the sick child differs from the sick adult, because the adult algorithm applied unchanged to a child is dangerous. The differences fall into four groups. Recognition differs: children run a higher heart rate for age and a lower, age-corrected blood pressure, so a heart rate of 140 is normal in a two-year-old and alarming in an adult, and the hypotension threshold is 70 plus twice the age in years rather than a fixed 90 — and the pressure falls last, so recognition rests on the perfusion signs, not the cuff reading. The arrest differs: it is asphyxial rather than cardiac, so the ratio is 15 to 2 for two rescuers (not 30 to 2), ventilations are central (compression-only is inferior in children), and the two-thumb encircling technique replaces the two-handed adult compression. The doses differ: adrenaline is 10 micrograms per kilogram (not 1 mg), defibrillation is 4 joules per kilogram (not 150 to 200 J), amiodarone is 5 mg per kilogram (not 300 mg), and fluid is 10 mL per kilogram (not a 500 mL saline bolus) — every dose is calculated against a weight estimated from the Broselow tape. The technique differs: the airway is anterior and the larynx high and anterior, the infant occiput flexes the neck, the straight-blade laryngoscope is preferred under two, and the cuffed tube is now standard. The dispatcher-assisted conventional cardiopulmonary resuscitation data confirm that conventional CPR with ventilations outperforms compression-only CPR in children, which is the evidence base for the 15 to 2 ratio.[1][3]
APLS and PALS versus adult ALS — the side-by-side
The Advanced Paediatric Life Support (APLS, ANZ/UK) and Pediatric Advanced Life Support (PALS, AHA) courses are structurally identical to each other and mirror the adult ALS algorithm in shape, but they diverge in five examinable ways. The Fellowship candidate must be able to draw the comparison, because applying the adult algorithm unchanged to a child is the single most dangerous error in paediatric resuscitation.[1]
Aetiology & ratio
- Adult: primary cardiac arrest, compression-only CPR equivalent — ratio 30:2
- Child: asphyxial arrest (over 90%), ventilations essential — ratio 15:2 for two rescuers, 30:2 only for a lone rescuer
- Both: 100–120 compressions/min, depth ≥⅓ AP chest diameter, full recoil, minimise pauses (under 5 s)
Doses (per kg)
- Adult: adrenaline 1 mg, amiodarone 300 mg, fluid bolus 500 mL–1 L, defib 150–200 J
- Child: adrenaline 10 mcg/kg (0.1 mL/kg of 1:10,000), amiodarone 5 mg/kg, fluid 10–20 mL/kg, defib 4 J/kg
- The adult ampoule overdoses the child — every dose is read off the Broselow tape or weight card
Compression technique
- Adult: two hands, lower sternum, depth 5–6 cm
- Infant: two-thumb encircling hands technique (two rescuers), depth ~4 cm
- Small child: heel of one hand; older child: two hands as in the adult
Airway & tube
- Adult: oral/nasal ETT, cuffed, Macintosh blade, sniffing position
- Child: oral preferred; high anterior larynx; straight (Miller) blade under 2 yr; cuffed now standard with cuff pressure under 25 cmH₂O
- Shoulder roll for the large occiput; pre-oxygenation buys only 30–60 s — expect early desaturation and bradycardia
Reversible causes
- Adult & child both: the 4 Hs (hypoxia, hypovolaemia, hypo/hyperkalaemia, hypothermia) and 4 Ts (tension pneumothorax, tamponade, toxins, thrombosis)
- Child adds: hypoglycaemia (check bedside glucose every arrest) — and PEA is almost always a reversible cause, search aggressively
- Traumatic arrest: adrenaline is not routinely effective in hypovolaemia — control the bleed and transfuse
Running the paediatric arrest algorithm — the two-minute loop
1 — Call for help and start high-quality CPR
Summon the resuscitation team. Start CPR at 15:2 (two rescuers) or 30:2 (lone rescuer), 100–120/min, depth ≥⅓ AP chest diameter (~4 cm infant, 5 cm child), full recoil. Two-thumb encircling hands for the infant. Attach the defibrillator and oxygen without interrupting compressions. Give five initial rescue breaths in the asphyxial arrest (drowning, hanging, asthma).
2 — Rhythm check and defibrillate if shockable
After 2 min, pause briefly (under 5 s) and assess the rhythm. VF or pulseless VT → defibrillate at 4 J/kg and resume CPR immediately for 2 min — do not check a pulse between shock and CPR. Asystole or PEA → resume CPR without a shock. Rotate the compressor every 2 min to prevent fatigue.
3 — Vascular access and the first adrenaline
Secure IV access within 90 s, or place an intra-osseous needle in the proximal tibia. Check the bedside glucose. Give adrenaline 10 mcg/kg (0.1 mL/kg of 1:10,000) IV/IO every 3–5 min (i.e. roughly every other cycle). Treat hypoglycaemia with 5 mL/kg of 10% dextrose.
4 — The third shock and amiodarone
After the third shock (still VF/pVT), give adrenaline 10 mcg/kg IV/IO and amiodarone 5 mg/kg IV/IO; flush. Continue CPR. A second amiodarone dose (5 mg/kg) follows the fifth shock. Lidocaine 1 mg/kg is the alternative where amiodarone is unavailable.
5 — Search and treat the reversible cause every cycle
Run the 4 Hs and 4 Ts at every rhythm check — hypoxia first in a child, then hypovolaemia, hypoglycaemia, hypothermia, tension pneumothorax, tamponade, toxins, thrombosis. Bedside ultrasound during the pause is invaluable for tamponade, volume and contractility. The child in PEA almost always has a correctable cause — find it.
6 — ROSC, stop, or escalate
On return of spontaneous circulation, optimise oxygenation (target SpO₂ 94–98%, avoid hyperoxia), normocapnia, normotension, normoglycaemia and normothermia, and transfer to PICU with targeted-temperature management. Prolong the resuscitation in the hypothermic, asphyxial (drowning) or toxin-reversible arrest — the child may recover after a long arrest. Stop only when the senior clinician is satisfied that reversible causes are exhausted.
Subtypes and special scenarios

The arrest and the resuscitation are modified by the cause. The asphyxial arrest (submersion or drowning, hanging, choking, severe asthma) prioritises five initial rescue breaths and effective ventilation — the outcome turns on restoring oxygenation, and the resuscitation is prolonged because the hypoxic, hypothermic child may recover after a long arrest. The septic-shock arrest follows unrecognised or under-resuscitated shock; the child is cold, mottled and hypotensive, and the resuscitation combines the arrest algorithm with fluid, adrenaline and antibiotics. The submersion arrest in cold water may benefit from prolonged resuscitation and rewarming. The congenital-cardiac and cardiomyopathy arrest is the small subgroup with a primary cardiac cause — VF and pulseless VT are more likely here, and early defibrillation is decisive. The trauma arrest is managed with simultaneous catastrophic-haemorrhage control, splintage and the paediatric trauma modifications, and adrenaline is not routinely effective in the hypovolaemic traumatic arrest. The neonatal arrest in the first 28 days follows the neonatal resuscitation algorithm — airway and breaths first, a higher initial fraction of inspired oxygen, and compressions at 3 to 1 once effective ventilation is established — and is covered in the neonatal emergencies topic.[1][2]
Complications and pitfalls
The complications are those the resuscitation is designed to prevent — hypoxic brain injury, multisystem organ failure, the post-arrest myocardial stunning — plus the iatrogenic: fluid overload with pulmonary oedema from over-aggressive boluses, and the drug error from a wrong weight. The pitfalls mirror the inversions of the protocol. The first is applying adult doses to a child — adrenaline 1 mg, defibrillation at 200 J, a 500 mL saline bolus — which overdoses and harms; the Broselow tape and the weight-based card prevent it. The second is compression-only CPR in a child — because paediatric arrest is asphyxial, omitting ventilations worsens outcome, and the ratio is 15 to 2. The third is delaying intra-osseous access while chasing collapsing veins; the intra-osseous needle is placed after two attempts or 90 seconds. The fourth is not checking the bedside glucose in the sick, seizing or arrested child — hypoglycaemia is silent, common and corrected with 5 mL per kilogram of 10 per cent dextrose. The fifth is mistaking exhaustion for compensation — the rising respiratory rate that then falls with rising effort is the exhausted child about to arrest, and the threshold to intubate is the failing effort, not the arrested child. The sixth is fixation on the rhythm at the expense of the reversible-cause search, the commonest human-factor failure in the failing paediatric resuscitation.[1][3]
Prognosis and disposition
Survival from paediatric out-of-hospital cardiac arrest sits around 7 to 10 per cent to hospital discharge overall, and rises to 30 to 40 per cent for in-hospital arrest, with good neurological outcome strongly predicted by a witnessed event, early bystander conventional cardiopulmonary resuscitation, and a shockable first rhythm. The asphyxial arrests dominate the out-of-hospital group, and their outcome turns on the quality of the early ventilation — which is the clinical justification for the 15 to 2 ratio and the priority given to the initial rescue breaths.[1][3] Every child who is resuscitated from arrest or who is in shock requiring fluid, vasoactive support or intubation is admitted to paediatric intensive care, with the retrieval service engaged early — the deteriorating or arrested child is retrieved to a centre that can deliver paediatric intensive care, not held in a peripheral emergency department beyond the first hour. The disposition from the emergency department is therefore a decision about timing and transport: stabilise the structured bundle, secure the airway and the access, start the vasoactive agent, control the temperature, and hand over to the retrieval and intensive-care teams with a documented timeline of the resuscitation. The parents are informed and supported by the senior clinician throughout.[1]
Special populations
The neonate under 28 days is managed on the neonatal resuscitation algorithm, not the paediatric one — airway and breaths first, compressions at 3 to 1 only after effective ventilation, and a higher initial inspired oxygen (21 per cent for the term baby, titrated up) — and sepsis in this age group uses cefotaxime plus ampicillin, not ceftriaxone. The bronchiolitic infant tires and hypercapnia mounts; the threshold for high-flow nasal cannula, non-invasive ventilation or intubation is the rising carbon dioxide and the failing effort, not a fixed oxygen threshold. The cyanotic congenital-heart-disease infant may desaturate because of a duct-dependent lesion, and a prostaglandin E1 (alprostadil) infusion at 0.01 to 0.05 micrograms per kilogram per minute keeps the ductus open until definitive repair; the differential of a desaturating infant includes this duct-dependent lesion. The immunocompromised or neutropenic child is treated as sick on arrival at any appearance, with broadened empiric antibiotics. The under-vaccinated child brings Haemophilus influenzae type b back into the organism list. The child with a difficult airway — the syndromic child, the crou-py epiglottitic child, the foreign-body obstruction — needs senior airway help summoned at the moment of recognition, not at the moment of collapse.[1]
[1] [1]Evidence and regional guidelines
The contemporary framework is the 2020 American Heart Association Guidelines for Pediatric Basic and Advanced Life Support (Topjian and colleagues), which set the structured approach, the 15 to 2 ratio, the two-thumb encircling technique, the 4 joules per kilogram defibrillation energy, the adrenaline and amiodarone doses, and the reversible-cause search used throughout this topic.[1] The 2024 International Liaison Committee on Resuscitation Consensus on Science with Treatment Recommendations (Greif and colleagues) integrates the most recent global evidence and underpins the regional guidelines.[2] The dispatcher-assisted conventional CPR outcome data (Goto, 2022) is the contemporary evidence base for the conventional CPR-with-ventilations approach over compression-only CPR in children, supporting the 15 to 2 ratio.[3] The weight-estimation literature (O'Leary, 2017, in an Australian cohort, and Abdel-Rahman, 2017, on the human-factors performance of the estimation tools) underpins the Broselow tape and the age-formula weight as the bedside standards.[4][5]
ANZ practice note. The Australian Resuscitation Council and New Zealand Resuscitation Council (ANZCOR) guidelines govern Australasian practice and align with the International Liaison Committee on Resuscitation consensus, adopting the 15 to 2 ratio, the 4 joules per kilogram defibrillation energy, the two-thumb encircling technique, and the weight-based drug doses from the Broselow tape or the age-formula weight. The state paediatric retrieval services retrieve every child in shock or after arrest to a paediatric intensive-care centre, and the weight-based drug cards and Broselow tapes are standard equipment in every Australasian emergency department resuscitation bay. [1]
SAQ — Septic shock and the weight-based resuscitation
10 minutes · 10 marks
A 3-year-old boy is brought to the resuscitation bay with a 12-hour fever, lethargy and a mottled, cool periphery. The heart rate is 180, the respiratory rate is 40, the capillary refill is 5 seconds, and the blood pressure is 78 over 50. The bedside glucose is 4.2 mmol per litre.
SAQ — The asphyxial paediatric arrest and the weight-based algorithm
10 minutes · 10 marks
A 6-year-old, 20 kg child collapses in the resuscitation bay three minutes after a near-drowning. The monitor shows a slow, wide-complex rhythm at 30 per minute with no palpable pulse. The child is apnoeic and cyanosed.
Exam pearls
- The blood pressure falls last in a child — recognise the tachycardia, the mottled skin, the capillary refill over three seconds and the altered conscious level first; a normal blood pressure does not exclude shock.
- Weight before any drug: Broselow tape, or weight in kilograms equals age plus four times two for the one-to-ten-year-old.
- Two rescuers means 15 to 2; one rescuer means 30 to 2. Paediatric arrest is asphyxial — ventilations matter, so compression-only is inferior and is not routine.
- Two-thumb encircling for the infant, heel of one hand for the small child, two hands for the older child; depth is at least one-third the chest (about 4 cm infant, 5 cm child).
- Defibrillate at 4 joules per kilogram; adrenaline 10 micrograms per kilogram; amiodarone 5 milligrams per kilogram — the adult doses overdose the child.
- Intra-osseous after two failed intravenous attempts or 90 seconds — never let difficult veins delay the resuscitation.
- Bradycardia in the deteriorating child is hypoxia — ventilate with 100 per cent oxygen first; the rate recovers.
- Check the bedside glucose in every sick, seizing or arrested child — hypoglycaemia is corrected with 5 mL per kilogram of 10 per cent dextrose.
- PEWS is a track-and-trigger, not a diagnosis — a child who triggers on two or more age-corrected vital signs is presumed sick until the workup proves otherwise; escalate before the blood pressure falls.
- The standard APLS fluid bolus is 20 mL/kg reassessed; cautious 10 mL/kg aliquots in septic shock (FEAST) and 5 mL/kg in suspected cardiogenic shock — titrate to perfusion, stop at hepatomegaly.
- The cuffed tube is now standard over 3 kg provided cuff pressure is monitored under 25 cmH₂O; tube internal diameter = age/4 + 4 mm; straight (Miller) blade under 2 yr, curved (Macintosh) above.
- Paediatric arrest aetiology is asphyxial over 90 per cent of the time — SIDS, drowning, choking, sepsis, trauma; primary cardiac (cardiomyopathy, myocarditis, channelopathy, commotio cordis) is the rare subgroup where VF/pVT appears and early defib at 4 J/kg is decisive.
- The desaturating neonate under 6 weeks has a duct-dependent lesion until proven otherwise — start prostaglandin E1 0.01–0.05 mcg/kg/min and anticipate apnoea.
- A child desaturates within 30–60 s of apnoea — pre-oxygenate, move fast, and ventilate before any drug; the adult two-minute window does not apply.
- The under-one-month febrile baby gets cefotaxime plus ampicillin, not ceftriaxone (bilirubin displacement) — full septic screen, low threshold to investigate. [1]
Red flags
[1]References
- [1]Topjian AA, Raymond TT, Atkins D, et al. Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Circulation, 2020.PMID 33081526
- [2]Greif R, Olasveengen TM, Semeraro F, et al. 2024 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Pediatric Life Support; Neonatal Life Support; Education, Implementation, and Teams; and First Aid Task Forces Resuscitation, 2024.PMID 39549953
- [3]Goto Y. Dispatcher-assisted conventional cardiopulmonary resuscitation and outcomes for paediatric out-of-hospital cardiac arrests Resuscitation, 2022.PMID 34648920
- [4]O'Leary F, Peat J, Hayen A, et al. Estimating the weight of ethnically diverse children attending an Australian emergency department: a prospective, blinded, comparison of age-based and length-based tools including Mercy, PAWPER and Broselow Arch Dis Child, 2017.PMID 27799153
- [5]Abdel-Rahman SM, Jacobsen R, Watts JL, et al. Comparative Performance of Pediatric Weight Estimation Techniques: A Human Factor Errors Analysis Pediatr Emerg Care, 2017.PMID 28777773
- [6]Maitland K, Kiguli S, Opoka RO, et al. Mortality after fluid bolus in African children with severe infection N Engl J Med, 2011.PMID 21615299
- [7]Parshuram CS, Hutchison J, Middaugh M, et al. Development and initial validation of the Bedside Paediatric Early Warning System score Crit Care, 2009.PMID 19678924
- [8]Luscombe MD, Owens BD, Burke D. Weight estimation in resuscitation: is the current formula still valid? Arch Dis Child, 2007.PMID 17213259
- [9]Goto Y, Funada A, Goto Y. Impact of dispatcher-assisted bystander cardiopulmonary resuscitation on neurological outcomes in children with out-of-hospital cardiac arrests: a prospective, nationwide, population-based cohort study J Am Heart Assoc, 2014.PMID 24785780