Paeds · child-safety-and-social-paediatrics
Abusive head trauma
Also known as Shaken baby syndrome · Non-accidental head injury · Inflicted traumatic brain injury · Shaken impact syndrome · Inflicted neurotrauma
Fellowship guide to abusive head trauma in infants and young children: the inflicted shaking-with-or-without-impact mechanism, the clinical picture of encephalopathy with subdural and retinal haemorrhage, the PediBIRN screen and Maguire discriminating features, the imaging and skeletal-survey workup, safeguarding from minute zero, the medical mimics and the triad debate, and the ANZ, UK and US guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the four-month-old brought in "not behaving normally", limp and grunting, whose parent says he rolled off a low bed an hour ago — but who, on the scan, has a thin inter-hemispheric subdural bleed, cerebral oedema, and a healing rib fracture that nobody mentioned. That gap between the story offered and the injury found is the heart of abusive head trauma, and it is where your clinical reasoning has to start. [1] [3]
AHT is the term the American Academy of Pediatrics adopted in 2009 to replace "shaken baby syndrome", and reaffirmed in its 2020 clinical report, because the older name implied a single mechanism and a single set of findings that the evidence does not support. The diagnosis is not "shaking did this"; it is "this child has inflicted head injury", made on the balance of the history, the examination and the investigations together. [1] [2]
The mechanism is violent, repeated rotational acceleration of the head, usually from shaking, often with an impact at the end of the movement — a force that exceeds anything a short household fall can generate in an infant whose neck is weak and whose brain is soft and water-rich. [1] [2]
Why this matters at fellowship level is that AHT is one of the commonest causes of traumatic brain injury and traumatic death in infants, it carries a heavy burden of lifelong disability, and missing it returns a child to a dangerous home while overcalling it harms a family and breaks trust. Your job is a careful, documented, multi-source assessment, with safeguarding running from minute zero. [3] [9]
Classification
There is no single lesion that is abusive head trauma. It is a constellation, so the useful way to classify it is by the injury domains that together raise the probability of inflicted injury, each scored on its own merits rather than collapsed into a label. [4] [5]
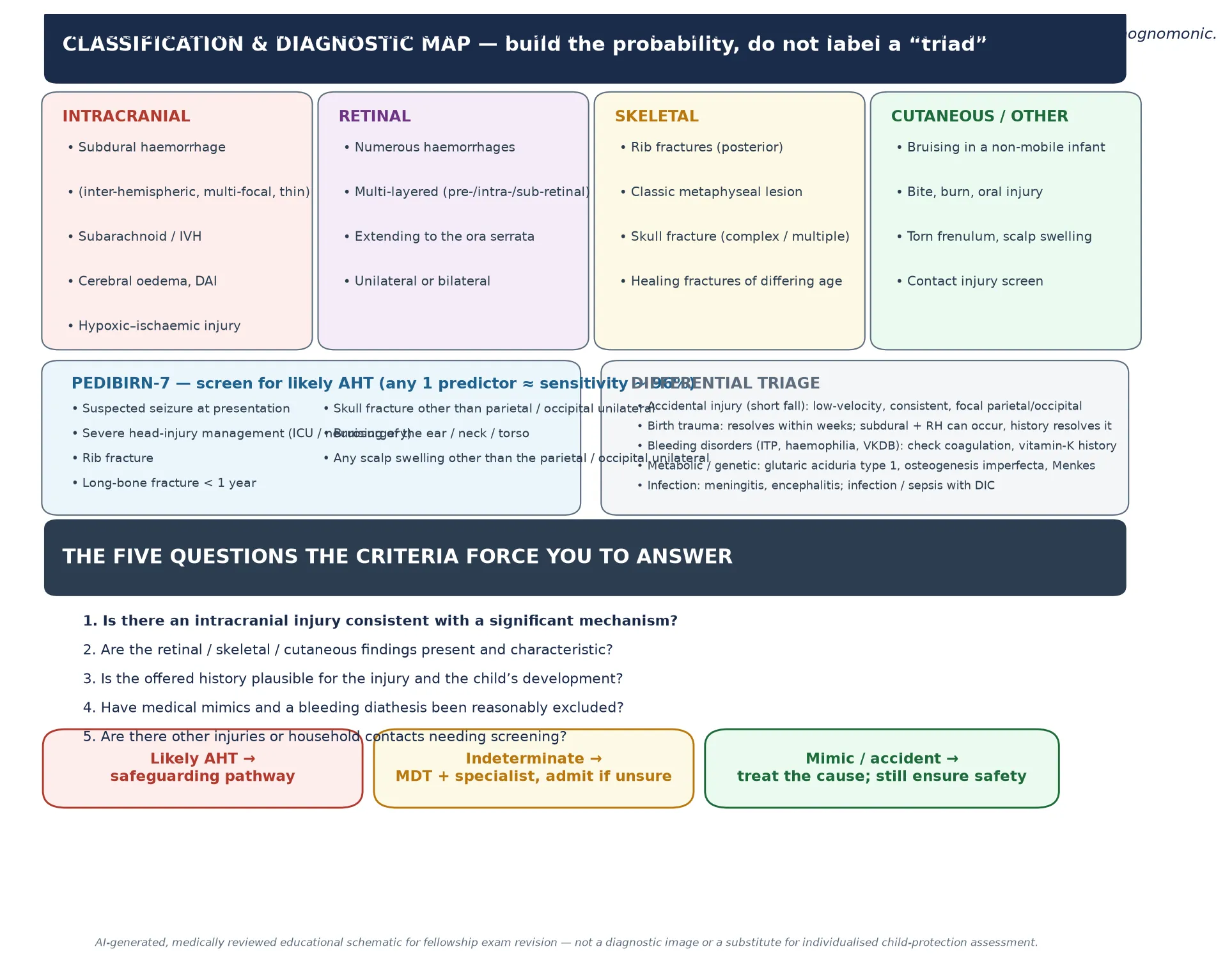
The intracranial domain includes subdural haemorrhage (especially multi-focal, inter-hemispheric or thin convexity bleeds), subarachnoid and intraventricular blood, diffuse cerebral oedema, diffuse axonal injury, and hypoxic–ischaemic change. The retinal domain is judged by the number, layer and extent of haemorrhages. The skeletal domain looks for high-specificity inflicted-injury markers such as posterior rib fractures, classic metaphyseal lesions, and fractures of differing ages. The cutaneous domain records bruising, bites, burns and oral injury, particularly in a child who is not yet mobile. [4] [5]
Intracranial injury
brain imaging
- Subdural bleed — multi-focal, inter-hemispheric, thin
- Subarachnoid / intraventricular blood
- Cerebral oedema, diffuse axonal injury
- Hypoxic–ischaemic change; atrophy over time
Retinal haemorrhage
dilated ophthalmology
- Numerous, too many to count
- Multi-layered: pre-, intra- and sub-retinal
- Extending to the ora serrata
- Unilateral or bilateral; highly supportive
Skeletal injury
skeletal survey
- Posterior / multiple rib fractures
- Classic metaphyseal lesion (corner fracture)
- Complex or multiple skull fracture
- Fractures of differing ages (healing)
Cutaneous / occult
skin + other
- Bruising in a non-mobile infant (TEN-4)
- Bite, burn, torn frenulum, oral injury
- Abdominal / thoracic occult injury
- Contact-injury screen of the home
A second, operational classification is the PediBIRN-7 screen, derived and validated in the paediatric intensive-care setting to flag head-injured infants who need an AHT workup. The presence of any one of seven predictors carries a high sensitivity for likely AHT, which is why it is a trigger to investigate, not a rule that proves abuse on its own. [6]
The numbers that anchor your viva
Epidemiology & Risk Factors
AHT most often strikes the most vulnerable infants. Population-based work places the peak incidence in the first year of life, with the highest risk in the two-to-four-month window that coincides with the normal peak of infant crying — the crying that overwhelms a carer who then shakes the child. [3]
The Keenan population-based study remains the foundational incidence estimate for inflicted traumatic brain injury in young children, and later work has confirmed that the burden falls overwhelmingly on infants and that the economic and disability cost is large. The Miller disability-adjusted life-year analysis quantified AHT as one of the costliest single categories of paediatric injury in the under-fives. [3] [9]
Risk amplifiers cluster around the child, the carer and the context. Child factors include young age, male sex, prematurity, low birth weight, and disability or colic. Carer factors include young parental age, single parenthood, mental-health or substance-use problems, domestic violence, and a carer who is not the biological parent. Contextual factors include socioeconomic stress, social isolation, prior child-welfare contact, and a household where intimate-partner violence is present. [1] [3]
Pathophysiology
The teaching model links the force applied to the anatomy of the infant to the pattern of injury you see on imaging and examination. The force is violent, repeated rotational acceleration of the head from shaking, with or without impact, that exceeds by far the force generated by a short household fall. [1]
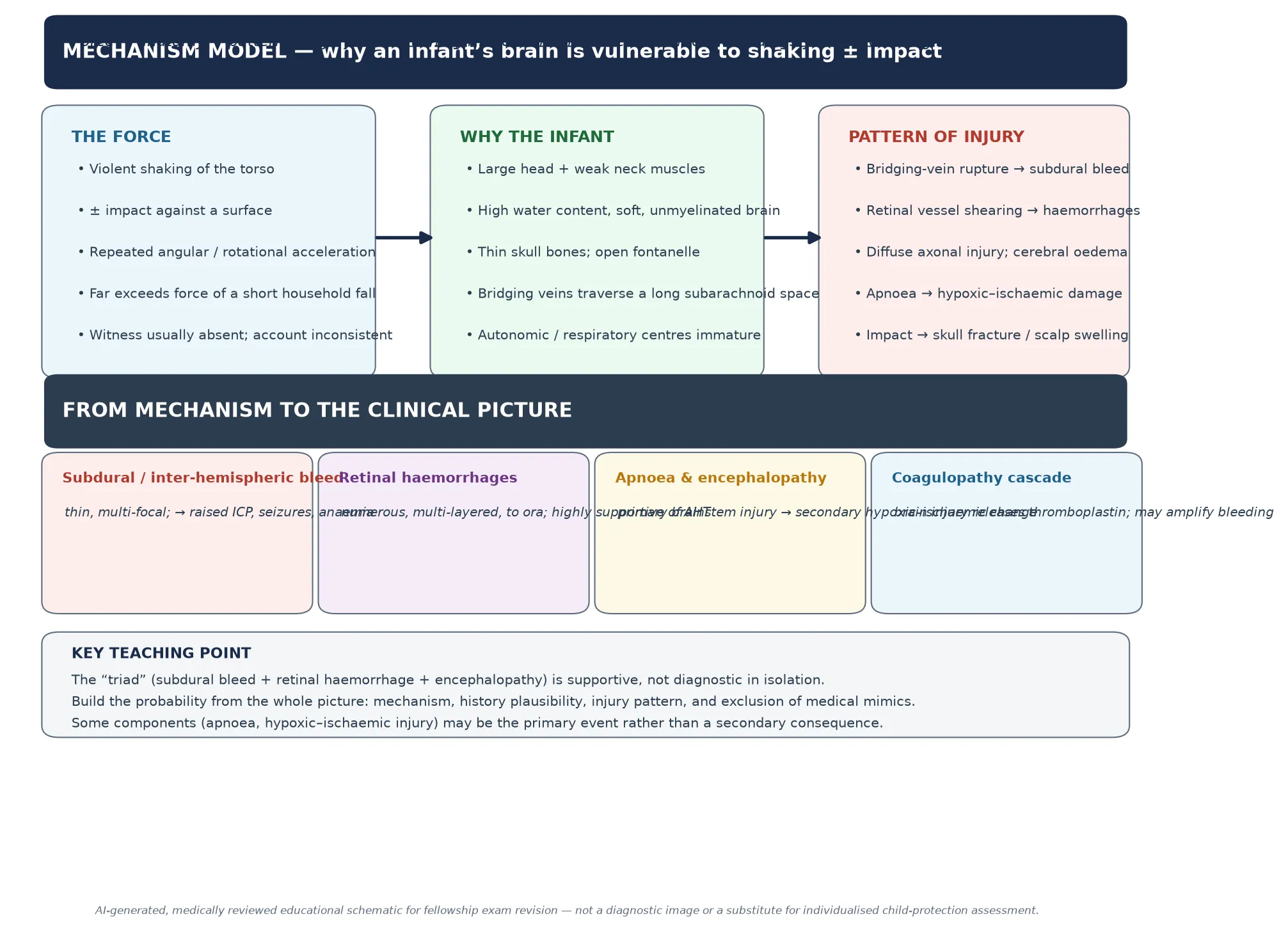
The infant's anatomy is the key to why the same force that would bruise an adult devastates a baby: a large heavy head on weak neck muscles, an unmyelinated brain with high water content, a thin and compliant skull, and bridging veins that traverse a long subarachnoid space before reaching the venous sinuses. When the head whips back and forth those veins stretch and tear, producing a thin subdural bleed, while rotational shearing injures axons and the retinal vessels. [1] [10]
The injury cascade that follows explains the clinical picture. Bridging-vein rupture gives the subdural haemorrhage; retinal vascular shearing gives the characteristic numerous, multi-layered retinal haemorrhages; diffuse axonal injury and cerebral oedema drive the encephalopathy; and apnoea from primary brainstem injury produces the secondary hypoxic–ischaemic damage that dominates the long-term outcome. The Kemp work on apnoea and brain swelling highlighted how often respiratory compromise is a central, not a peripheral, event in non-accidental head injury. [12]
A common pitfall is to assume each finding is a direct mechanical consequence of shaking in a simple chain. The evidence now supports a more complex model in which primary traumatic injury, apnoea-driven hypoxia, and a secondary coagulopathy cascade (brain injury releases thromboplastin) interact, which is why dating injuries and reading the whole pattern matters more than matching one finding to one force. [1] [12]
Clinical Presentation
The child in front of you rarely arrives with a label. An infant may present with non-specific, apparently minor symptoms — irritability, vomiting, poor feeding, lethargy — that look like a viral illness, or with an apparent life-threatening event, a seizure, or collapse. The discriminator is that the story does not fit the severity of the brain injury, and that the child is in the high-risk age band. [1] [11]
The Bechtel study, which compared accidental and abusive head-injured infants in hospital, found that the features that separated inflicted from accidental injury were the severity of the encephalopathy, the presence of retinal haemorrhages, the pattern of skeletal injury, and a history that was absent, inconsistent or implausible for the child's developmental stage. The lesson for the bedside is that the history is part of the data, not background. [11]
| Presentation story | Do not stop here | Must still map |
|---|---|---|
| 'Rolled off the bed' | A short fall rarely causes a serious intracranial injury in an infant | Mechanism plausibility, neuroimaging, retina, skeleton, skin |
| 'Just a viral illness' | Irritability, vomiting and lethargy can be the only sign of a subdural bleed | GCS, fontanelle, head circumference, seizures, full workup if any red flag |
| 'Stopped breathing briefly' | An ALTE / BRUE in an infant may be the presentation of inflicted injury | Neuroimaging, retina, coagulation, skeletal survey, screen contacts |
| 'He fell while I was holding him' | The account often changes between tellings or between informants | Document verbatim, obtain collateral, repeat the history |
| 'No idea how this happened' | An absent history for a serious injury is itself a red flag | Full inflicted-injury workup and safeguarding pathway |
On examination the brain-injured infant may be encephalopathic, floppy, pale or shocked, with a full or tense fontanelle, a rising head circumference, a low Glasgow Coma Scale score, focal or generalised seizures, apnoea or irregular breathing. The skin exam may reveal bruising in a non-mobile child — recall the TEN-4-FACES rule, that bruising on the Torso, Ear, or Neck in any infant under 4 years, or any bruising in a non-mobile infant, is a sentinel finding. [1]
Retinal haemorrhages are not visible without dilation by an ophthalmologist, which is why you must not declare "no retinal haemorrhages" on a bedside look alone — it is a request, not an examination. The Binenbaum natural-history study showed that retinal haemorrhages from head trauma resolve on a predictable timescale, which is why prompt, documented, dilated ophthalmology with imaging is part of the standard workup and of dating. [10]
Differential Diagnosis
Build the differential in three piles so you neither anchor on abuse nor dismiss it: accidental injury that mimics the imaging, medical conditions that bleed, and the rare metabolic or genetic mimics. The aim is not to "prove" abuse but to estimate the probability of inflicted injury against plausible alternatives, using the history, the injury pattern and focused tests. [4] [15]
A short fall — from a bed, a change table or a carer's arms — can produce a simple, single parietal or occipital skull fracture and a small extra-axial bleed, but it very rarely produces the multi-focal, inter-hemispheric subdural bleed, cerebral oedema and numerous retinal haemorrhages of AHT. The Piteau systematic review set out the clinical and radiographic features that associate with abusive versus non-abusive head trauma, and the discriminators are the ones to memorise for viva. [5]
Accidental injury
- Short fall: simple linear parietal/occipital fracture
- Consistent, witnessed, developmentally plausible story
- Single-pattern injury, no occult fractures
- Resolves the diagnosis with the history
Birth trauma
- Subdural and retinal haemorrhages can occur with vaginal delivery
- Usually asymptomatic; resolves within weeks
- Resolved by the history and the rapid clearance of RH
- Becomes a mimic mainly in the first few weeks
Bleeding disorders
- Vitamin-K deficiency bleeding (especially if declined)
- Haemophilia, ITP, rare factor deficiencies, DIC
- Does not explain fractures or the history
- Coagulation, FBC, vitamin-K history, PT/APTT
Metabolic / genetic / other
- Glutaric aciduria type 1 (subdural + macrocephaly)
- Osteogenesis imperfecta (fractures, blue sclerae)
- Menkes disease; rare vascular malformations
- Meningitis / encephalitis; sepsis with DIC
The most important rule of the differential is that a medical mimic does not exclude abuse — a child with a bleeding disorder or a metabolic condition can also be abused, and a coagulopathy can be both a mimic and a consequence of brain injury. Document the mimics you considered and excluded, and let the child-protection team and the specialists reason together rather than declaring the case closed on a single test. [15]
Clinical & Bedside Assessment
The assessment is a structured, multi-source process, not a single examination. You need the history from every carer who looks after the child, the developmental history, the social history, and collateral from the referring clinician and any witnesses, because the consistency and plausibility of the account is itself diagnostic information. [1] [2]
The examination documents the airway, breathing and circulation first, then a careful skin search in good light (record every bruise on a body map), the head and fontanelle, the head circumference plotted over time, a full neurological examination including the GCS, an abdominal and oral examination, and a search for the high-specificity inflicted-injury markers. Every finding is contemporaneously documented, with photographs where the local protocol allows, because this record may become evidence. [1]
Use the PediBIRN-7 rule as a structured trigger: in an acutely head-injured infant, the presence of suspected seizure at presentation, severe head injury requiring intensive care or neurosurgery, rib fracture, long-bone fracture in an infant, a skull fracture that is not a simple unilateral parietal/occipital fracture, bruising of the ear, neck or torso, or scalp swelling beyond a simple parietal/occipital swelling should trigger the full AHT workup. [6]
Investigations
The investigation strategy has three aims: to characterise the brain injury and treat it, to search for additional inflicted injuries, and to exclude reasonable medical mimics. These run in parallel with safeguarding, not after it. [1] [5]
Neuroimaging leads the workup. A non-contrast CT head is the first-line investigation in any infant with altered responsiveness, seizures, a low GCS, a fontanelle abnormality or any red flag, because it identifies haemorrhage, midline shift and cerebral oedema that need urgent neurosurgical or intensive-care action. MRI brain follows, ideally within days, to define the full injury map — diffuse axonal injury, hypoxic–ischaemic change, and the number and character of subdural collections — and to help date the bleeds through signal evolution and the presence of membranes. [1] [5]
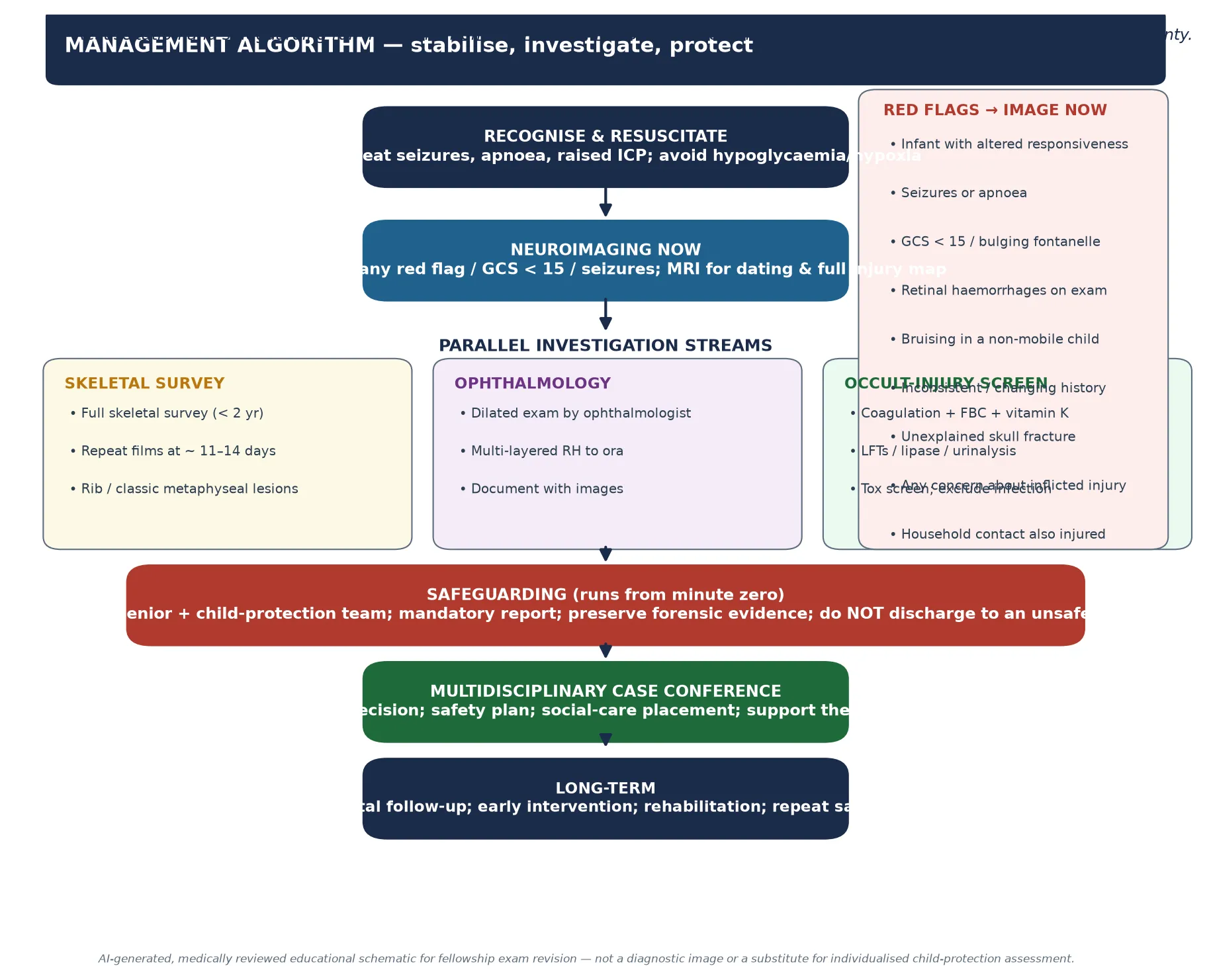
A skeletal survey is indicated in every suspected case and in any child under two years with a suspicious injury, performed to a standardised protocol of multiple views and repeated at about eleven to fourteen days to reveal fractures that were occult on the initial films. The Wood study confirmed the utility and the yield of skeletal surveys in young injured children, particularly for the high-specificity inflicted-injury fractures that change the probability of AHT. [14]
Dilated ophthalmology by an ophthalmologist, with imaging, documents the number, layer and extent of retinal haemorrhages and their distribution to the ora serrata — the pattern most supportive of inflicted injury. A laboratory occult-injury screen includes a coagulation profile and full blood count, a vitamin-K history, liver and pancreatic markers (to find occult abdominal injury), a urinalysis, and infection and toxicology screens where indicated. [1] [10]
The standard workup, run in parallel
CT head now for any red flag or low GCS; MRI within days to map and date the injury.
Skeletal survey to protocol, repeated at ~ 11–14 days to surface occult fractures.
Dilated ophthalmology with imaging; document number, layer and extent of retinal haemorrhages.
Coagulation, FBC and vitamin-K assessment; liver and pancreatic markers, urinalysis, infection and toxicology screens.
Screen siblings and household contacts for occult injury through the child-protection team.
Contemporaneous documentation of every finding and every history account; preserve evidence.
Management — Resuscitation
Resuscitation is exactly the same as for any critically brain-injured child: protect the airway, support breathing and circulation, and treat the treatable causes of secondary brain injury — hypoxia, hypotension, hypoglycaemia, seizures and raised intracranial pressure. The difference is that safeguarding begins at the same moment, not after the child is stabilised. [1]
Manage seizures with the standard paediatric anticonvulsant pathway and treat raised intracranial pressure with neuroprotection, head positioning and urgent neurosurgical input for a surgical lesion. Involve paediatric intensive care and neurosurgery early, because the brain-injured infant can deteriorate quickly from cerebral oedema or an expanding bleed. [1]
The safeguarding bundle runs alongside: inform the consultant and the child-protection team from the start, do not allow the child to be discharged to the care of a suspected perpetrator, preserve clothing and any potential evidence, and make the mandatory report required by your jurisdiction. Treat the family with respect and without accusation — your role is to investigate and protect, and an adversarial stance damages both the child and the assessment. [1] [2]
Management — Definitive & Stepwise
Once the child is stabilised, definitive management is a coordinated, multidisciplinary process. The medical job is to complete the investigation set, treat the injuries, and reach a careful, documented conclusion about the probability of inflicted injury; the safeguarding job is to secure the child, assess and support the family, and plan a safe disposition. [1]
The decision about the probability of AHT is made by the team, not a single clinician, weighing the mechanism plausibility, the injury pattern across all four domains, the exclusion of medical mimics, and the social context. Use the Maguire pooled-analysis discriminating features and the PediBIRN screen as the evidence base for that estimate, and record your reasoning explicitly. [4] [6]
AHT-SAFE
Hold a multidisciplinary case conference with the child-protection team, social care, the police where the local protocol requires it, and the treating clinicians, to agree the level of concern and the safety plan. Screen siblings and household contacts for occult injury — the Lindberg study showed a real prevalence of abusive injuries in contacts of physically abused children, which is why contact screening is standard. [7]
Plan the disposition around safety first: the child must not return to a setting where further injury is possible, which may mean a safe carer, out-of-home care, or a prolonged inpatient stay while the assessment and the social-care plan are completed. Arrange neurodevelopmental follow-up, early-intervention services, and rehabilitation from the outset, because the outcome of AHT is dominated by long-term disability. [9] [13]
Specific Subtypes & Scenarios
The well-looking infant with an incidental subdural bleed is one of the hardest scenarios. A small subdural collection found on imaging done for another reason, in a well infant, forces a careful search for birth trauma, a bleeding disorder, a metabolic mimic such as glutaric aciduria type 1, and a hidden inflicted-injury pattern — not an automatic diagnosis of abuse, but never a dismissal of it either. [15]
The infant with retinal haemorrhages alone must be assessed in context, because retinal haemorrhages can occur with birth trauma (and clear within weeks), with severe accidental injury, with a bleeding disorder, and with raised intracranial pressure. The pattern most supportive of inflicted injury is numerous, multi-layered haemorrhages extending to the ora serrata, and the absence of that pattern does not exclude AHT. [10]
Rebleeding into a known subdural collection is often raised in court as evidence of a "second event" or of extreme fragility. The evidence does not support the idea that trivial handling rebleeds a subdural; rebleeding is uncommon and, when it occurs, usually reflects the natural evolution of a significant initial injury rather than a new inflicted event. [1] [15]
Hymel 2014 — Pediatrics (PMID 25404722)
Multicentre derivation-and-validation cohort in a paediatric ICU
Key finding
The PediBIRN predictors identified likely AHT with high sensitivity, supporting their use as a structured trigger for the full inflicted-injury workup.
Practice change
Use the screen to decide who to investigate, not to prove abuse; the diagnosis is a team judgement on the whole picture.
The contact-screening scenario is a frequent examination stem: an infant is diagnosed with AHT, and you are asked what to do about the siblings. The answer is a structured screen for occult injury — history, examination, and imaging as age-appropriate — coordinated through the child-protection team, because occult inflicted injury in contacts is common enough to mandate it. [7]
Complications & Pitfalls
The complications of AHT are dominated by its outcome. Mortality is high — around a fifth of recognised cases die, and many survivors are left with cognitive, visual, seizure, motor and behavioural disability that becomes apparent only as the child grows and misses developmental milestones. [3] [13]
The Keenan three-year neurodevelopmental follow-up found that early traumatic brain injury left a substantial burden of cognitive and behavioural impairment, which is why surveillance, early intervention and rehabilitation must be planned from the time of diagnosis, not deferred until problems declare themselves. [13]
The most damaging pitfall is the opposite of the one candidates fear. The classic error is to miss AHT by attributing an infant's encephalopathy to a viral illness, a short fall or a feeding problem, returning the child to a dangerous home where a recurrence — often fatal — follows. The discriminating move is to image the brain of any infant with an unexplained altered mental state and to look for the injury domains. [1] [11]
The second pitfall is overcalling AHT on a single finding or a fixed "triad" without excluding mimics or weighing the history, which harms the family and is vulnerable in court. The RCPCH critique of the triad is required reading precisely because it forces a disciplined, whole-picture assessment rather than a label-based one. [15]
[15]Prognosis & Disposition
AHT carries one of the heaviest prognostic burdens in paediatrics. Alongside the high mortality, survivors face a high probability of permanent disability — cognitive impairment, epilepsy, visual impairment, cerebral palsy-type motor deficits, and behavioural disorders — and the full extent often emerges only over years of neurodevelopmental follow-up. [3] [13]
The factors that worsen prognosis are the severity of the initial encephalopathy, the extent of hypoxic–ischaemic injury on MRI, the need for intensive care or neurosurgery, the presence of seizures, and social factors that limit access to rehabilitation and early intervention. Plan follow-up with developmental medicine, neurology, ophthalmology and allied health from the outset. [13]
Disposition is safety-led. The child must not be discharged to the care of a suspected perpetrator; the options, agreed with the child-protection team and social care, are placement with a safe carer, out-of-home care, or an inpatient stay while the assessment completes. The treating team also owes the family honesty, support and a non-judgemental stance, and an accurate, well-documented report that may be used in child-protection or criminal proceedings. [1] [2]
A relapse-prevention and family-support plan is part of the disposition: identify the triggers (infant crying, parental stress, isolation), link the family to support services, and ensure that any return home is planned and supervised so that the child is not placed back at risk. Prevention at the population level — parent education about infant crying and the danger of shaking — has been shown to reduce AHT incidence. [8]
Special Populations
Infants under six months are the highest-risk group because of their complete dependence, their crying peak, and the immaturity of their brain and neck; a low threshold for imaging and the full workup is essential. Children with disability or neurodevelopmental difference are over-represented both as victims and as children whose symptoms are misattributed, and they need an assessment calibrated to their baseline. [1] [3]
Siblings and household contacts of a child with confirmed or suspected AHT must be screened for occult injury, because the prevalence of inflicted injury in contacts is high enough to make this standard practice rather than an optional extra. The Lindberg contact-prevalence study underpins this recommendation. [7]
Indigenous, refugee and socio-economically disadvantaged families experience higher rates of the stressors that drive AHT, and they deserve a culturally safe, non-stigmatising assessment that distinguishes the violence from the context. Children in out-of-home care and those known to child-protection services carry elevated risk and need vigilant follow-up. [1]
Rural and remote settings face thin access to ophthalmology, skeletal-survey expertise and child-protection teams, which makes telehealth, retrieval and clear referral pathways part of the standard of care — the workup should not be compromised by geography. [1]
Evidence, Guidelines & Regional Differences
| Region | Guideline / position | Naming | Reporting |
|---|---|---|---|
| ANZ | RACP / state child-protection guidance; trauma-informed MDT | Non-accidental head injury, inflicted neurotrauma, AHT | Mandatory reporting to child protection; varies by state |
| UK | RCPCH child-protection evidence; triad used with caution | Abusive head trauma / non-accidental head injury | Mandatory reporting duties under safeguarding legislation |
| US | AAP 2020 clinical report (Narang) replacing the 2009 Christian report | Abusive head trauma | State mandatory-reporting laws; CAPTA |
| Canada / RCPSC | CPS and provincial child-protection guidance | AHT / inflicted head injury | Provincial mandatory reporting |
The evidence backbone you should be able to name starts with the Keenan population-based incidence study and the AAP clinical reports (the 2009 Christian report that renamed SBS to AHT, and the 2020 Narang report that reaffirmed it). The Maguire pooled analysis quantified the discriminating clinical features, the Piteau systematic review did the same for the radiographic features, and the Hymel PediBIRN studies gave a validated screening rule. [1] [4] [5]
The live controversy is not whether AHT exists — it does, and it kills and disables infants — but how rigorously the diagnosis is built and how honestly it is presented in court. The RCPCH critique of the triad, and the history of overturned convictions, demand that paediatricians present a probability grounded in the whole picture, exclude mimics, document meticulously, and never overstate the certainty of any single finding. [15]
The prevention evidence is encouraging: hospital-based parent-education programs about infant crying and the dangers of shaking, such as the Dias program, have been associated with reductions in AHT incidence, which is why universal parent education in the maternity and early-infancy period is a recommended population-level intervention. [8]
Exam Pearls
The single move that saves lives is the lowest-threshold one: when an infant's brain does not match the story, image the brain and start the workup. When the workup is equivocal, keep the child safe while the team decides — a few days of cautious admission is far cheaper than a recurrence. [1] [11]
And when you teach this topic, teach the discipline of the assessment rather than the label: a careful, documented, multi-source evaluation that weighs mechanism, injury pattern, mimics and context is what protects the child and stands up in court. [1] [15]
References
- [1]Narang SK, Fingarson A, Lukefahr J, et al. Abusive Head Trauma in Infants and Children. Pediatrics, 2020.PMID 32205464
- [2]Christian CW, Block R, Committee on Child Abuse and Neglect, et al. Abusive head trauma in infants and children. Pediatrics, 2009.PMID 19403508
- [3]Keenan HT, Runyan DK, Marshall SW, et al. A population-based study of inflicted traumatic brain injury in young children. JAMA, 2003.PMID 12902365
- [4]Maguire SA, Kemp AM, Lumb RC, et al. Estimating the probability of abusive head trauma: a pooled analysis. Pediatrics, 2011.PMID 21844052
- [5]Piteau SJ, Ward MG, Barrowman NJ, et al. Clinical and radiographic characteristics associated with abusive and nonabusive head trauma: a systematic review. Pediatrics, 2012.PMID 22778309
- [6]Hymel KP, Willson DF, Boos SC, et al. Validation of a clinical prediction rule for pediatric abusive head trauma. Pediatrics, 2014.PMID 25404722
- [7]Lindberg DM, Shapiro RA, Blood EA, et al. Prevalence of abusive injuries in siblings and household contacts of physically abused children. Pediatrics, 2012.PMID 22778300
- [8]Dias MS, Smith K, DeGuehery K, et al. Preventing abusive head trauma among infants and young children: a hospital-based, parent education program. Pediatrics, 2005.PMID 15805350
- [9]Miller TR, Steinbeig R, Waidyanatha R, et al. Disability-adjusted life-year burden of abusive head trauma at ages 0-4. Pediatrics, 2014.PMID 25404725
- [10]Binenbaum G, Mirza-George N, Christian CW, et al. The natural history of retinal hemorrhage in pediatric head trauma. J AAPOS, 2016.PMID 27079593
- [11]Bechtel K, Stoessel K, Leventhal JM, et al. Characteristics that distinguish accidental from abusive injury in hospitalized young children with head trauma. Pediatrics, 2004.PMID 15231923
- [12]Kemp AM, Stoodley N, Cobley C, et al. Apnoea and brain swelling in non-accidental head injury. Arch Dis Child, 2003.PMID 12765909
- [13]Keenan HT, Hooper SR, Wetherington CE, et al. Neurodevelopmental consequences of early traumatic brain injury in 3-year-old children. Pediatrics, 2007.PMID 17332181
- [14]Wood JN, Fakeye O, Feudtner C, et al. Use and Utility of Skeletal Surveys to Evaluate for Occult Fractures in Young Injured Children. Acad Pediatr, 2019.PMID 30121318
- [15]Debelle GD, Maguire S, Coltman T, et al. Abusive head trauma and the triad: a critique on behalf of RCPCH of 'Traumatic shaking: the role of the triad in medical investigations of suspected traumatic shaking'. Arch Dis Child, 2018.PMID 29510999