Paeds · child-safety-and-social-paediatrics
Strangulation, suffocation and asphyxial injury
Also known as Asphyxial injury · Mechanical asphyxia · Accidental suffocation and strangulation in bed · Inflicted suffocation · Non-accidental asphyxia
Fellowship guide to strangulation, suffocation and asphyxial injury in infants and children: the three mechanisms (neck compression, airway oronasal occlusion, chest restriction) and their shared endpoint of cerebral hypoxia; the infant-vulnerability anatomy and the petechial-haemorrhage reality check; recognition of the collapsed child in a sleep or hazard space, the resuscitation and scene-preservation response, the safe-sleep ABCs and product-hazard prevention, the hardest forensic question of accidental overlay versus inflicted suffocation, and the ANZ, UK and US guideline and reporting differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the seven-month-old brought to the emergency department cold and blue after being found face-down in the soft bedding of the parental bed during a feed, or the three-year-old found dangling by the neck from a looped window-blind cord in the bedroom. Both children share the same mechanism of harm — oxygen stopped reaching the brain — and both are examples of the preventable, time-critical, often fatal category of injury this topic covers. [1] [3]
Asphyxia is the failure of oxygen delivery to the tissues, and in childhood it happens when an external force blocks the airway, compresses the neck, or restricts chest movement. Strangulation is external pressure on the neck; suffocation (also called smothering) is obstruction of the external airway or entrapment in an oxygen-depleted space; and compression asphyxia is restriction of chest expansion. Each can be accidental, inflicted, or — rarely — the result of self-harm in older children. [6]
Why this matters at fellowship level is that asphyxial injury is one of the leading causes of accidental death in infants and young children in high-income countries, it is largely preventable through safe-sleep and product-safety measures, and it sits at the uneasy boundary between an accident and child abuse where the scene, the history and the body findings decide the conclusion. Your job is to recognise it instantly, resuscitate while you preserve evidence, and reason carefully about whether the story fits. [1] [4]
Classification
There is no single lesion that is asphyxia — the useful way to classify these injuries is by the mechanism that produced the oxygen failure, because the mechanism dictates both the immediate resuscitation and the prevention message. Sort every case into one of three mechanism families, then judge whether it is accidental or inflicted against the story. [6]
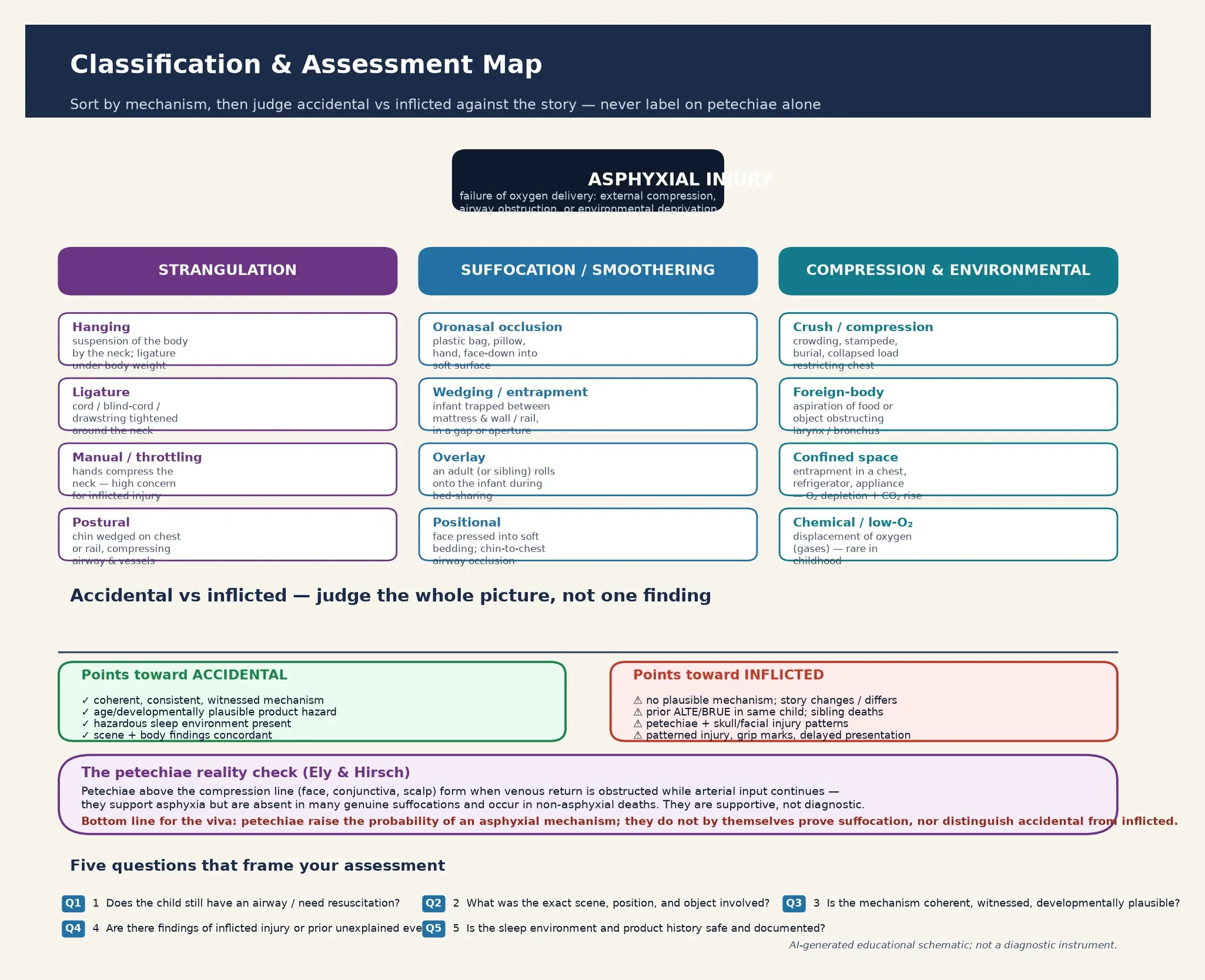
The first family is neck compression (strangulation) — hanging, where the body weight tightens a ligature; ligature strangulation from a window-blind cord, drawstring or rope; manual throttling, which carries a high index of concern for inflicted injury; and postural strangulation, where the chin wedges against a rail or the chest, folding the airway closed. The second family is suffocation and smothering — oronasal occlusion by a plastic bag, pillow or hand; wedging and entrapment, where an infant is trapped between a mattress and a wall or in a cot gap; overlay, where an adult or sibling rolls onto the infant during bed-sharing; and positional suffocation, where the face presses into soft bedding. [6]
The third family is compression and environmental asphyxia — crush from crowding or a collapsed load that restricts chest expansion; foreign-body obstruction of the larynx or bronchus; confined-space entrapment in a chest, refrigerator or appliance; and, rarely, chemical or low-oxygen environments that displace oxygen. These boundaries overlap at the bedside, which is why you name the most plausible mechanism and then test it against the scene and the history rather than forcing the case into a single box. [5] [6]
Neck compression
strangulation
- Hanging — body weight tightens a ligature
- Ligature — blind cord, drawstring, rope
- Manual / throttling — high concern for inflicted
- Postural — chin wedged on chest or rail
Suffocation / smothering
airway obstruction
- Oronasal occlusion — bag, pillow, hand
- Wedging / entrapment — mattress-to-wall, cot gap
- Overlay — adult rolls onto bed-sharing infant
- Positional — face pressed into soft bedding
Compression & environmental
chest / space
- Crush — crowding, burial, collapsed load
- Foreign body — food or object in airway
- Confined space — chest, refrigerator, appliance
- Low-O₂ — oxygen displacement (rare)
A second, operational classification matters as much as the mechanism: every case is either accidental, inflicted, or indeterminate, and the indeterminate group is the one that demands the most disciplined work because the body alone often cannot separate accidental overlay from deliberate suffocation. Build that judgement from the scene, the history, the findings and the context together, and present a probability rather than a verdict. [7]
Epidemiology & Risk Factors
Asphyxia strikes the most vulnerable children in the most ordinary places — the cot, the parental bed, the bedroom with the window blind, the high chair, the toy box. In high-income settings, accidental suffocation and strangulation, particularly in the sleep environment, is one of the commonest causes of injury death in infants beyond the neonatal period, and the reported rate has risen over the last two decades as classification shifted deaths out of SIDS and into the asphyxia category. [3] [4]
The Erck Lambert national-trends analysis traced sudden unexpected infant death in the United States from 1990 to 2015 and showed that as SIDS rates fell after the back-to-sleep campaigns, the proportion of deaths attributed to accidental suffocation and strangulation in bed rose — partly a genuine signal of hazardous sleep environments and partly a reclassification of deaths that would once have been labelled SIDS. The Carlberg study mapped the maternal and infant characteristics that cluster with ASSB and found the burden fell on infants in unsafe sleep settings, with soft bedding, prone sleeping, bed-sharing, and exposure to smoke. [3] [4]
The numbers that anchor your viva
Risk amplifiers cluster around the child, the sleep environment, and the product. Child factors include young age, low birth weight, prematurity, and any condition that limits the ability to extricate from a hazardous position. Sleep-environment factors include prone and side sleeping, soft bedding and pillows, sofa-sharing, bed-sharing with an impaired or smoking adult, and overcrowding. Product factors include looped window-blind cords, drawstrings on clothing, gaps in cots and bunk-bed rails, and chest or appliance entrapment. [1] [10]
Pathophysiology
The teaching model links the force applied to the anatomy of the child to the injury you see. The force is any external compression, obstruction, or restriction that stops oxygen reaching the brain; the endpoint is cerebral hypoxia and, if it persists, hypoxic–ischaemic injury or death. The speed of the collapse reflects how little reserve an infant has. [6]
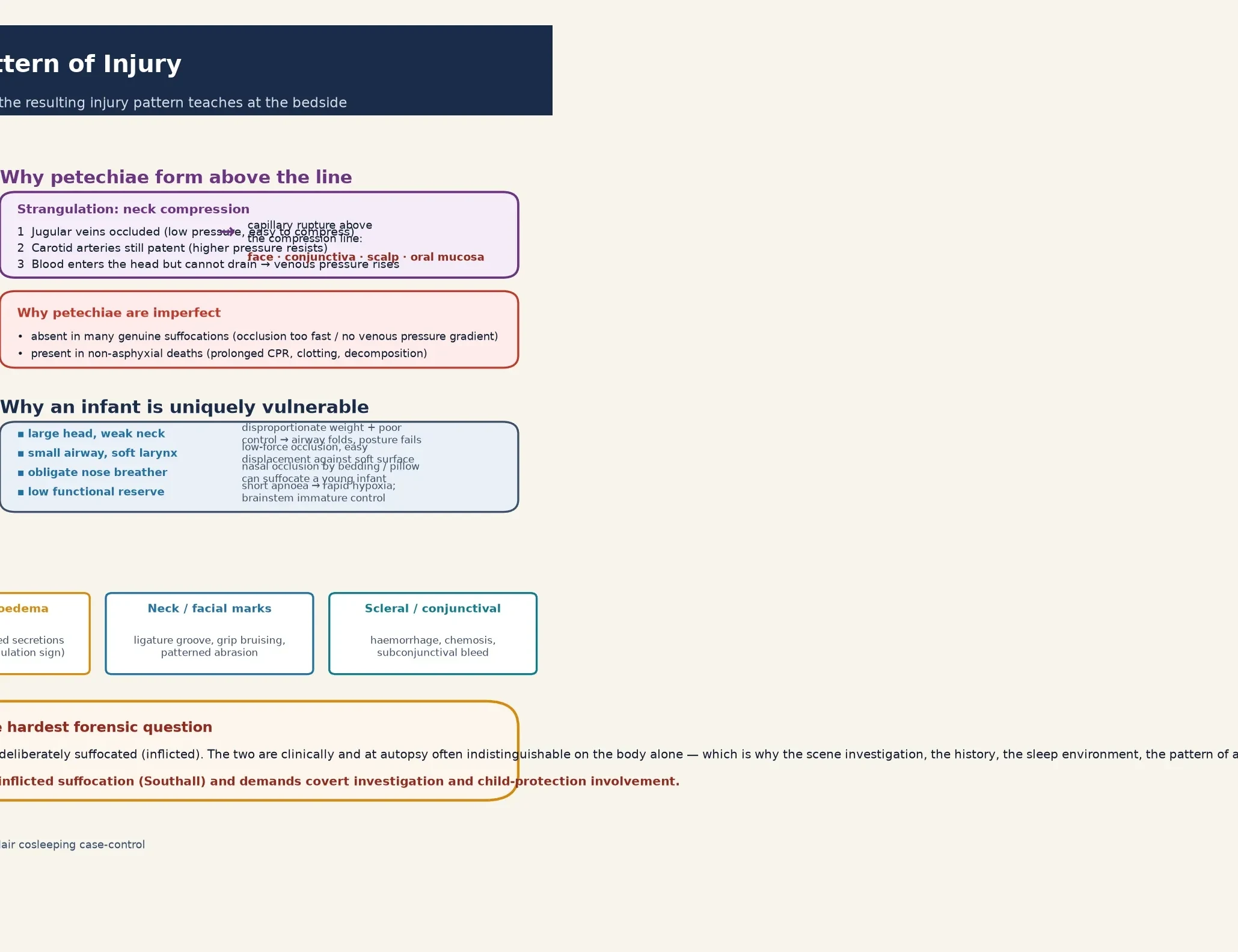
The infant's anatomy is the key to why the same force that an adult shrugs off kills a baby: a disproportionately large heavy head on weak neck muscles, a small and compliant airway that occludes against a soft surface, obligate nasal breathing in the first months of life, and a low functional reserve that turns a short apnoea into rapid, profound hypoxia. When the face presses into soft bedding the nose and mouth occlude; when the neck compresses the venous return fails before the airway; and when the chest is restricted the lungs cannot expand. [6]
The injury cascade that follows explains the clinical picture. Reduced ventilation raises carbon dioxide and lowers oxygen; tissue hypoxia develops fastest in the brain, with its high metabolic demand and immature autoregulation; and neuronal injury, cerebral oedema and brainstem failure produce the altered responsiveness, seizure, apnoea and collapse you find at the scene. The Ely and Hirsch review of asphyxial deaths and petechiae set out why petechial haemorrhages form — when neck compression obstructs the thin-walled jugular veins while the higher-pressure carotid arteries keep delivering blood, venous pressure rises and capillaries rupture above the compression line, giving the face, conjunctival, scalp and oral-mucosal petechiae that support an asphyxial mechanism. [6]
A common pitfall is to assume the body findings will always tell you what happened. The harder truth is that accidental overlay and inflicted suffocation are often clinically and at autopsy indistinguishable on the body alone, which is why the scene investigation, the sleep environment, the history and any prior unexplained events — not the autopsy in isolation — decide the question. [7] [8]
Clinical Presentation
The child in front of you usually arrives already collapsed, and the story of where and how they were found is the single most important piece of data. An infant may be brought in pale, floppy, apnoeic or seizing after being found in a sleep space; a toddler may arrive with neck marks, stridor, or a hoarse voice after a cord or drawstring event; and a child with a foreign body may present with the abrupt choking, coughing and cyanosis of acute airway obstruction. [1] [5]
The features that separate an asphyxial collapse from sepsis, a cardiac arrhythmia or a metabolic crisis are the context and the scene: a child found unconscious in a sleep space, under bedding, beside a window cord, or in an entrapment hazard, with petechiae on the face and conjunctiva, frothy pulmonary oedema, neck or facial marks, or a pattern of injury that points to a specific mechanism. The lesson for the bedside is that the scene report and the carer account are clinical data of the first rank, not background. [6] [7]
| Presentation story | Do not stop here | Must still map |
|---|---|---|
| 'Found not breathing in bed' | Bed-sharing, soft bedding, or overlay may be the mechanism | Scene detail, sleep position, who else was present, prior events |
| 'Cord round the neck' | A looped blind-cord hanging can arrest within minutes | Neck marks, airway and cervical injury, neurology, time to retrieval |
| 'Choked on food, now blue' | Acute laryngeal obstruction can present as sudden collapse | Airway patency, foreign-body removal, aspiration risk, neurology |
| 'Just stopped breathing' | An ALTE / BRUE in an infant may mask inflicted suffocation | Scene, history consistency, prior events, sibling deaths, safeguarding |
| 'No idea how this happened' | An absent history for a collapse in a hazard space is a red flag | Full scene reconstruction, child-protection team, forensic documentation |
On examination the asphyxiated child may be apnoeic, cyanosed, shocked or in cardiorespiratory arrest, with altered responsiveness, seizure activity, or a low Glasgow Coma Scale score that reflects hypoxic–ischaemic encephalopathy. The skin and head exam may reveal facial and conjunctival petechiae, a ligature groove or grip bruising on the neck, patterned abrasions, and signs of other inflicted injury. The airway may reveal an obstructing foreign body, stridor, or frothy secretions, and the chest may show poor expansion from compression or a coexisting injury. [6]
Differential Diagnosis
Build the differential around the collapsed child so you neither anchor on asphyxia nor miss it: non-asphyxial causes of sudden collapse, the specific asphyxial mechanism, and the question of inflicted injury. The aim is to identify the reversible cause at the bedside and to reason carefully about the mechanism once the child is stable. [1] [7]
A severe infection — sepsis, meningitis or pneumonia — can present as a sudden collapse with respiratory failure and must be treated empirically while you gather the scene history. A cardiac arrhythmia or cardiomyopathy, including the channelopathies, can produce sudden collapse in an infant or older child and is excluded by an ECG and cardiac evaluation. A metabolic crisis, an intentional or accidental poisoning, and a seizure can each mimic an asphyxial presentation, which is why a glucose, a blood gas and a toxicology screen belong in the early workup of any unexplained collapse. [1]
Non-asphyxial collapse
- Sepsis, meningitis, pneumonia — treat empirically
- Cardiac arrhythmia, cardiomyopathy — ECG
- Metabolic crisis, hypoglycaemia — glucose, gas
- Poisoning, seizure — tox screen, history
Asphyxial mechanism
- Sleep-space overlay, wedging, soft bedding
- Neck compression — cord, drawstring, hanging
- Foreign-body airway obstruction
- Confined-space or compression entrapment
Inflicted injury
- Induced or inflicted suffocation (Southall)
- Story that shifts or is implausible
- Prior unexplained apnoea or sibling death
- Patterned injury, grip marks, coexisting abuse
The most important rule of the differential is that an alternative diagnosis does not exclude asphyxia or abuse — a child with a channelopathy can also be suffocated, and a coexisting infection does not explain petechiae above a compression line. Document the causes you considered and excluded, and let the scene, the history, the investigations and the child-protection team reason together before any conclusion is communicated. [7]
Clinical & Bedside Assessment
The assessment is a structured, scene-aware process that begins the moment the child is found. Take the history from every carer who was present, focusing on the exact time, place, position, sleep arrangement, who else was in the bed or room, and the sequence from discovery to the call for help — because the consistency and plausibility of the account is itself diagnostic and forensic information. [1] [7]
The examination documents the airway, breathing and circulation first, then a careful search for the asphyxial signs — facial and conjunctival petechiae, neck marks and ligature grooves, patterned abrasions, frothy pulmonary oedema, and a foreign body in the airway — alongside a full top-to-toe assessment for coexisting inflicted injury. Every finding is contemporaneously documented, with photographs where the local protocol allows and before the scene is disturbed, because this record may become evidence in a child-protection or coronial process. [6]
Use the scene reconstruction as a structured part of the assessment: what was the sleep surface, the position, the bedding, the room, and the objects present? Was there a looped window-blind cord, a drawstring, a plastic bag, a gap in the cot, or an unsafe shared surface? The Blair case-control study of hazardous cosleeping in south-west England showed that the modifiable risk factors — soft bedding, sofa-sharing, bed-sharing with an adult who had drunk alcohol or smoked, and prone positioning — cluster in the deaths and are the ones a careful scene history will surface. [8]
Investigations
The investigation strategy has three aims: to support the resuscitation and identify reversible causes, to characterise the injury and exclude mimics, and to contribute to the forensic and safeguarding assessment. These run in parallel, not after the child is stable. [1]
Bedpoint investigations include a blood gas and lactate to gauge the severity of hypoxia and acidosis, a glucose to exclude hypoglycaemia, and an ECG to screen for a cardiac cause of collapse. Sepsis, metabolic and toxicology screens run where the presentation is unexplained, because an alternative diagnosis must be sought and treated empirically even when the scene points to asphyxia. [1]
Neuroimaging with a CT head is indicated for any child with altered responsiveness, a seizure, a low Glasgow Coma Scale, or focal neurological signs, to identify cerebral oedema, hypoxic–ischaemic change or a coexisting intracranial injury. A full inflicted-injury workup — skeletal survey, ophthalmology and a coagulation screen — runs in parallel whenever the story is implausible or the findings suggest abuse, because the asphyxial presentation may be one part of a wider inflicted-injury pattern. [7]
The standard workup, run in parallel
Blood gas, lactate and glucose at the bedside; ECG to screen for a cardiac cause.
Sepsis, metabolic and toxicology screens where the collapse is unexplained; treat empirically.
CT head for any neurological sign or low GCS; MRI later to map hypoxic–ischaemic injury.
Inflicted-injury workup — skeletal survey, dilated ophthalmology, coagulation — when the story is implausible.
Scene documentation and reconstruction with police and child-protection input; preserve objects.
Contemporaneous, verbatim documentation of every history account and every examination finding.
The forensic investigation of an unexpected death is not the treating clinician's job alone — it is a statutory child-death review that integrates police scene examination, paediatric review, social-care assessment and, where indicated, a post-mortem to a standardised sudden-unexpected-death protocol. Your contribution is the contemporaneous clinical record, the verbatim history and the honest communication of uncertainty. [7] [8]
Management — Resuscitation
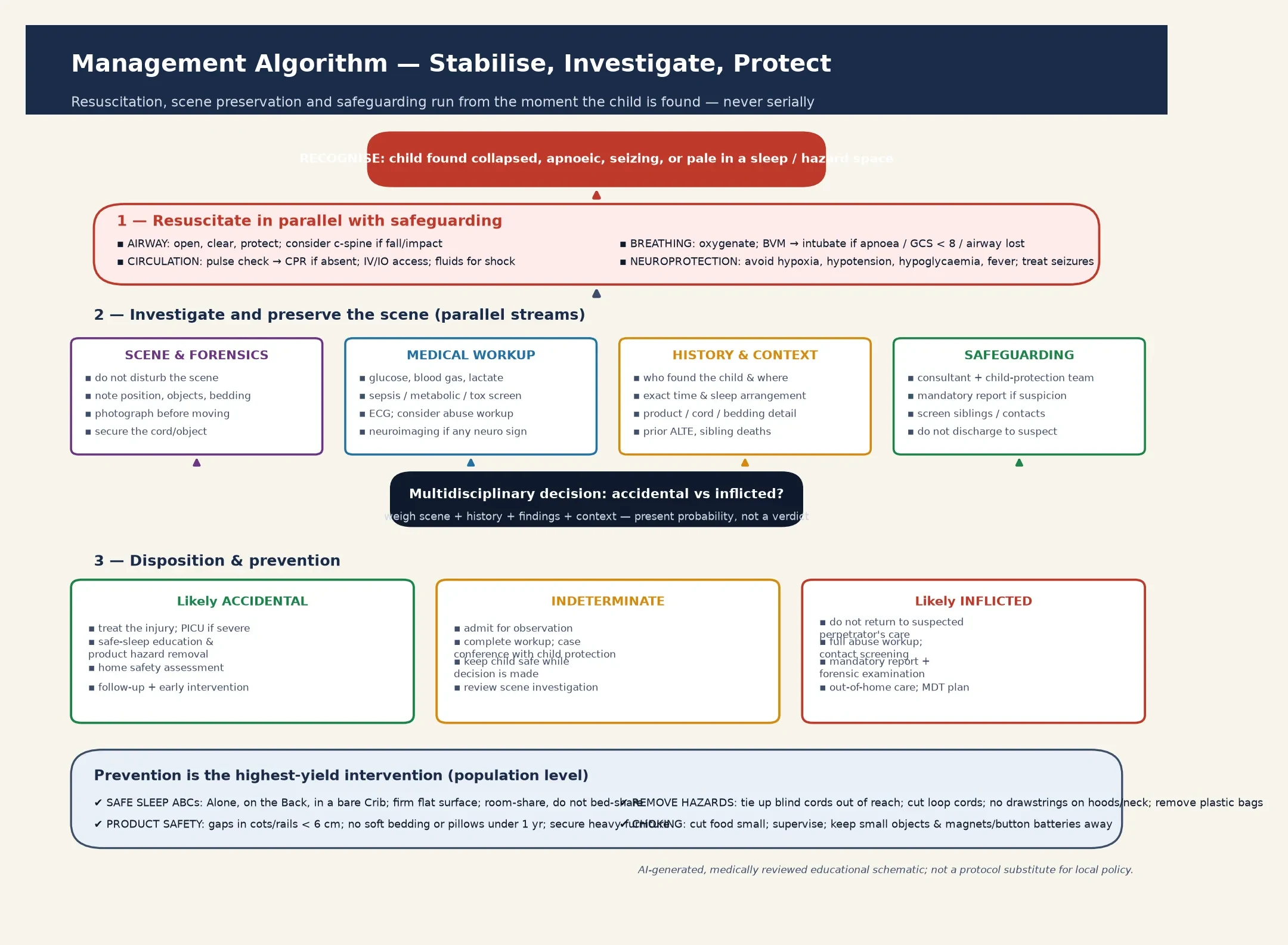
Resuscitation is exactly the same as for any critically hypoxic child: open and protect the airway, support breathing and circulation, and treat the reversible causes of secondary brain injury — hypoxia, hypotension, hypoglycaemia, fever and seizures. The difference is that scene preservation and safeguarding begin at the same moment, not after the child is stabilised. [1]
Manage the airway by clearing any obstruction, removing a foreign body if one is present, and supporting ventilation with bag-valve-mask ventilation, escalating to intubation for apnoea, a falling consciousness level or an unprotected airway. Begin cardiopulmonary resuscitation immediately if there is no pulse, and seek the cause in parallel — a glucose, a blood gas, and a search for sepsis and a cardiac rhythm disturbance. Involve paediatric intensive care early, because the asphyxiated child can deteriorate quickly from cerebral oedema or a secondary arrest. [1]
The safeguarding and scene-preservation bundle runs alongside: do not disturb or "tidy" the scene, note and photograph the position, the bedding and the objects before anything is moved, secure the cord or product involved, and inform the consultant and the child-protection team from the first minute. Make the mandatory report required by your jurisdiction, and treat the family with respect and without accusation — your role is to resuscitate, to investigate and to protect, and an adversarial stance damages both the child and the assessment. [7]
Management — Definitive & Stepwise
Once the child is stabilised, definitive management is a coordinated, multidisciplinary process. The medical job is to complete the investigation set, treat the injuries, and reach a careful, documented conclusion about the probability of an accidental versus an inflicted mechanism; the safeguarding job is to secure the child, assess and support the family, and plan a safe disposition. [1] [7]
The decision about the mechanism is made by the team, not a single clinician, weighing the scene, the history, the injury pattern, the exclusion of mimics and the social context. Where the picture is clear and concordant — a witnessed cord event with a matching ligature mark, or a coherent overlay story in a known hazardous bed-sharing setting — the conclusion may be straightforward. Where it is not, keep the child safe while the multidisciplinary review and the statutory child-death process complete, and present a probability rather than a verdict. [7] [8]
ASPHYX
Hold a multidisciplinary case review with the child-protection team, social care, the police where the local protocol requires it, and the treating clinicians, to agree the level of concern and the safety plan. Screen siblings and household contacts for occult injury and for a history of unexplained events — because recurrent or witnessed apnoea in the same child, or a sibling death, raises induced or inflicted suffocation, the entity the Southall covert-video work brought to light, and demands a higher level of child-protection involvement. [7]
Plan the disposition around safety first: the child must not return to a setting where further injury is possible, which may mean a safe carer, out-of-home care, or an inpatient stay while the assessment and the social-care plan are completed. For the survivor, arrange neurodevelopmental follow-up, early-intervention services and rehabilitation from the outset, because the outcome of significant hypoxic–ischaemic injury is dominated by long-term disability. [1]
Specific Subtypes & Scenarios
The sleep-related suffocation in an infant is the commonest and the most preventable scenario. An infant found face-down in soft bedding, wedged between a mattress and a wall, or overlaid during bed-sharing presents the core safe-sleep lesson: back to sleep on a firm flat surface, in a bare cot, room-sharing without bed-sharing, and away from smoke, soft bedding and impaired adults. The AAP 2022 recommendations and their evidence base are the documents you must be able to summarise. [1] [2]
The window-blind-cord strangulation is a classic, devastating, and preventable toddler-and-preschool scenario. A looped cord tightens around the neck as the child slips or leans, producing rapid unconsciousness from carotid and jugular compression; the mortality is high and the prevention is mechanical — fit cordless blinds or tension devices, cut looped cords, and keep cots and furniture away from windows. The product-safety and regulatory response, including moves toward cordless window-covering standards, is part of the prevention evidence. [1]
Blair 2009 — BMJ (PMID 19826174)
Case-control study of SIDS in south-west England, comparing sleep environments
Key finding
The highest risk attached to sofa-sharing, bed-sharing with an adult who had drunk alcohol or smoked, and soft bedding — factors amenable to change through a targeted safe-sleep message.
Practice change
Tailor prevention to the hazardous cosleeping environments the data identify, rather than a blanket prohibition that families ignore.
The foreign-body airway obstruction spans the choking infant to the older child with an inhaled object. Acute laryngeal obstruction presents with sudden coughing, choking, stridor and cyanosis, and the response is back-blows and chest thrusts for the infant, abdominal thrusts for the older child, with urgent airway removal if obstruction persists. The Lorenzoni systematic review of non-food foreign bodies aspirated by children characterised the objects — magnets, button batteries, coins, beads and small toy parts — that drive the prevention message to keep small objects out of reach. [5] [9]
The induced or inflicted suffocation scenario is the one no clinician can afford to miss. An infant with recurrent, witnessed, or unexplained apnoea, a story that changes between tellings, or a sibling death, raises fabricated, induced or inflicted suffocation — the entity the Southall covert-video study documented, in which a carer obstructs the infant's airway and produces life-threatening events that resolve only when the child is removed from the carer's care. The threshold for child-protection involvement and covert investigation is low, because the mortality of missed inflicted suffocation is high. [7]
Complications & Pitfalls
The complications of asphyxial injury are dominated by its outcome. Death at the scene is common, and survivors of significant hypoxic–ischaemic injury face a high probability of permanent disability — cognitive impairment, epilepsy, cerebral-palsy-type motor deficits, visual impairment and behavioural disorders — that often emerges only over years of neurodevelopmental follow-up. [1]
The most damaging pitfall is the opposite of the one candidates fear. The classic error is to miss inflicted suffocation by attributing a collapse or a death to SIDS, an accident or a near-miss without examining the scene, the history and the pattern of injury — returning the child to a dangerous home where a recurrence, often fatal, follows. The discriminating move is to treat every unexplained infant collapse as a safeguarding event from the first minute and to reconstruct the scene. [7]
The second pitfall is overcalling asphyxia or abuse on petechiae alone, which the Ely and Hirsch review explicitly warns against. Petechiae support an asphyxial mechanism but are absent in many genuine suffocations and present in non-asphyxial deaths, so they never prove suffocation and never, on their own, distinguish accidental from inflicted. The disciplined clinician builds the probability from the whole picture — scene, history, findings, context — and presents it honestly. [6]
[7]Prognosis & Disposition
Asphyxial injury carries one of the heaviest prognostic burdens in child safety. The outcome is driven by the duration and severity of the hypoxic insult, the time to retrieval and effective resuscitation, and the presence of secondary brain injury — cerebral oedema, hypoxic–ischaemic change and seizure. Children who present in cardiorespiratory arrest, or who need prolonged intensive care, face the worst outlook. [1]
The factors that worsen prognosis are a long downtime, the need for cardiopulmonary resuscitation, a low initial Glasgow Coma Scale, refractory seizures, and social factors that limit access to rehabilitation and early intervention. Plan follow-up with developmental medicine, neurology, and allied health from the outset, because the full extent of the disability often emerges only over years. [1]
Disposition is safety-led. The child must not be discharged to the care of a suspected perpetrator; the options, agreed with the child-protection team and social care, are placement with a safe carer, out-of-home care, or an inpatient stay while the assessment completes. For every case — accidental or otherwise — the discharge must include a concrete prevention plan: remove the hazard, teach the safe-sleep ABCs, and arrange home-safety and follow-up support so that the family leaves safer than it arrived. [1] [8]
A relapse-prevention and family-support plan is part of every disposition: identify the modifiable risk factors the Blair study highlighted — sofa-sharing, bed-sharing with an impaired or smoking adult, soft bedding, prone positioning — and address them with a culturally appropriate, judgement-free message in the family's own language. Population-level prevention — universal safe-sleep education, cordless window-covering standards, and product-safety regulation — has been shown to reduce asphyxial deaths and is the highest-yield intervention of all. [8]
Special Populations
Infants under six months are the highest-risk group because of their obligate nasal breathing, their inability to extricate from a hazardous position, and their low physiological reserve; a low threshold for safe-sleep counselling and scene assessment is essential. Premature and low-birth-weight infants carry elevated risk and need targeted safe-sleep teaching at discharge and beyond. [1] [10]
Children with disability or neurodevelopmental difference are over-represented both as victims of asphyxial events (impaired airway protection, seizure-related suffocation, unsafe sleep positioning) and as children whose collapse is misattributed; they need an assessment calibrated to their baseline and a prevention plan tailored to their abilities. The Vennemann German SIDS study confirmed that prematurity, prone sleeping and hazardous sleep environments amplify one another in the most vulnerable infants. [10]
Siblings and household contacts of a child with confirmed or suspected inflicted suffocation must be screened for occult injury and a history of unexplained events, because the recurrence risk in an unsafe setting is high. Indigenous, refugee and socio-economically disadvantaged families experience more crowded housing, shared and improvised sleep surfaces, and thinner access to safe products, and they deserve a culturally safe, non-stigmatising prevention message. [1] [7]
Rural and remote settings face thin access to intensive care, retrieval, child-protection teams and forensic services, which makes telehealth, clear retrieval pathways and a standardised scene-documentation checklist part of the standard of care — the response should not be compromised by geography. [1]
Evidence, Guidelines & Regional Differences
| Region | Guideline / position | Classification | Reporting |
|---|---|---|---|
| ANZ | RACP / state SUDI and child-death-review guidance | SUDI with ASSB subclassification | Mandatory reporting; statutory child-death review |
| UK | RCPCH child-protection evidence; statutory child-death review | SIDS vs explained asphyxial death | Mandatory reporting; rapid-response multi-agency review |
| US | AAP 2022 safe-sleep recommendations (Moon) | SUID, ASSB, SIDS categories | State mandatory-reporting laws; CAPTA |
| Canada / RCPSC | CPS and provincial joint-paediatric guidance | SUDI with scene investigation | Provincial mandatory reporting |
The evidence backbone you should be able to name starts with the AAP 2022 safe-sleep recommendations and their evidence base (Moon and the Task Force on SIDS), which reaffirm the back-to-sleep, firm-flat-surface, bare-cot, room-share-not-bed-share, no-soft-objects and avoid-smoke messages. The Erck Lambert national-trends analysis traced the SUID shift from SIDS to ASSB, the Carlberg study mapped the maternal-and-infant risk profile of ASSB, and the Blair case-control study identified the hazardous cosleeping factors amenable to change. [1] [4] [8]
The forensic and child-protection evidence turns on two papers. The Ely and Hirsch review of asphyxial deaths and petechiae is the reference for what petechiae do and do not prove, and the Southall covert-video study remains the landmark evidence that induced or inflicted suffocation is a real, lethal, and identifiable form of child abuse. The Lorenzoni systematic review characterises the non-food foreign bodies that drive choking prevention. [6] [7] [9]
The live controversy is not whether asphyxial injury exists — it does, and it kills and disables children — but how rigorously the accidental-versus-inflicted question is built, and how honestly it is presented. The history of deaths reclassified from SIDS to asphyxia, and of inflicted suffocation missed until a sibling died, demands that paediatricians present a probability grounded in the scene, the history, the findings and the context — never a verdict built on a single sign. [6] [7]
Exam Pearls
The single move that saves lives is the most preventable one: when an infant's death or collapse traces to an unsafe sleep environment or an unretrieved hazard, the prevention message — delivered in the family's own language, without judgement, and before the next baby arrives — is what breaks the cycle. When the picture is unclear, keep the child safe while the team and the child-death review decide. [1] [7]
And when you teach this topic, teach the discipline of the scene: a careful, documented, multi-agency reconstruction that weighs mechanism, history, findings and context is what protects the child, what honours the family, and what stands up in a coronial or child-protection process. [6] [7]
References
- [1]Moon RY, Carlin RF, Hand I, Task Force on Sudden Infant Death Syndrome and the Committee on Fetus and Newborn Sleep-Related Infant Deaths: Updated 2022 Recommendations for Reducing Infant Deaths in the Sleep Environment. Pediatrics, 2022.PMID 35726558
- [2]Moon RY, Carlin RF, Hand I, Task Force on Sudden Infant Death Syndrome Evidence Base for 2022 Updated Recommendations for a Safe Infant Sleeping Environment to Reduce the Risk of Sleep-Related Infant Deaths. Pediatrics, 2022.PMID 35921639
- [3]Carlberg MM, Shapiro-Mendoza CK, Goodman M Maternal and infant characteristics associated with accidental suffocation and strangulation in bed in US infants. Matern Child Health J, 2012.PMID 21769585
- [4]Erck Lambert AB, Parks SE, Shapiro-Mendoza CK National and State Trends in Sudden Unexpected Infant Death: 1990-2015. Pediatrics, 2018.PMID 29440504
- [5]Committee on Injury, Violence, and Poison Prevention Prevention of choking among children. Pediatrics, 2010.PMID 20176668
- [6]Ely SF, Hirsch CS Asphyxial deaths and petechiae: a review. J Forensic Sci, 2000.PMID 11110181
- [7]Southall DP, Plunkett MC, Banks MW, Falkov AF, Samuels MP Covert video recordings of life-threatening child abuse: lessons for child protection. Pediatrics, 1997.PMID 9346973
- [8]Blair PS, Sidebotham P, Evason-Coombe C, Edmonds M, Heckstall-Smith EM, Fleming P Hazardous cosleeping environments and risk factors amenable to change: case-control study of SIDS in south west England. BMJ, 2009.PMID 19826174
- [9]Lorenzoni G, Vertuani M, D'Agnolo D, et al. Characterization of Non-Food Foreign Bodies Aspirated by Children: A Systematic Review of the Literature. Children (Basel), 2023.PMID 37892372
- [10]Vennemann MM, Bajanowski T, Brinkmann B, Jorch G, Yudkin P, Mitchell EA, GeSID Study Group Sleep environment risk factors for sudden infant death syndrome: the German Sudden Infant Death Syndrome Study. Pediatrics, 2009.PMID 19336376