Paeds · ent-hearing-and-oral-health
Facial swelling and odontogenic infection
Also known as Dental abscess · Periapical abscess · Odontogenic cellulitis · Ludwig angina · Facial cellulitis of dental origin
Fellowship guide to paediatric facial swelling of dental origin, from a localised periapical abscess through spreading odontogenic cellulitis to Ludwig angina and deep neck space infection: the principle that every spreading odontogenic infection has a source tooth that must be drained or extracted, because antibiotics alone fail without source control; the polymicrobial anaerobic microbiology and the empirical intravenous regimens (ampicillin-sulbactam, clindamycin with metronidazole, ceftriaxone plus metronidazole); the fascial-plane anatomy (buccinator, mylohyoid, submandibular and sublingual spaces) that determines whether pus tracks into the cheek, the floor of mouth or the neck; and the airway-threat red flags of Ludwig angina — bilateral submandibular swelling, woody floor of mouth induration, tongue elevation, drooling and trismus — that make securing the airway the first and most important step.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Related topics
Overview & Definition
Picture the five-year-old who arrives with a swollen cheek, a low fever and a two-day history of toothache that the family put down to sweets. The swelling is firm, warm and tender, and the child holds the jaw stiff. The fellowship task is to recognise this as an odontogenic infection — an infection that began in a tooth — and to judge how far it has spread, because the difference between a dental abscess that needs a day-case extraction and Ludwig angina that needs an emergency airway is a clinical judgement you make at the bedside. [1] [6]
An odontogenic infection is one that arises from the teeth or their supporting structures — most often as the end result of untreated dental caries, but occasionally from periodontal disease or dental trauma. The chain runs from enamel caries through dentine to the dental pulp, where it causes irreversible pulpitis; once the pulp necroses, infection escapes through the root apex into the periapical tissues to form a periapical abscess, and from there it can erode the cortical bone and track through the fascial planes of the face and neck. [1] [4]
What lifts this topic to fellowship level is the principle of source control and the anatomy of fascial spread. An abscess is a collection of pus under pressure, and antibiotics cannot sterilise a closed space — the offending tooth must be extracted or undergo endodontic treatment and the pus drained. Where the pus tracks is determined by the muscle attachments of the jaw, which dictates whether the child develops a cheek swelling, a floor-of-mouth infection, or Ludwig angina with its threat to the airway. Recognising the source, draining the collection, and protecting the airway are the three skills that earn marks and save lives. [2] [4]
Classification
Classify paediatric odontogenic infection by depth of spread and the fascial space involved, because this determines whether the child needs a dental extraction as a day case or an emergency airway in theatre. Keeping the layers separate prevents the two great errors: discharging a child whose infection has already spread beyond the tooth, and missing the child whose floor-of-mouth swelling is Ludwig angina. [1] [2]
By depth, the spectrum has four layers. A localised dentoalveolar abscess is confined to the periapical tissues and overlying mucosa — a gum swelling, a tender tooth, and a well child. A spreading odontogenic cellulitis has breached the cortical bone and entered the soft tissues of the face, producing a firm, tender, warm and erythematous facial swelling with regional lymphadenopathy and systemic features. A localised fascial space infection occupies a named space such as the buccal, canine, submasseteric or infratemporal space, often as a drainable collection. A deep space infection — submandibular, sublingual and submental spaces together (Ludwig angina), or parapharyngeal and retropharyngeal spread — threatens the airway and the mediastinum. [4] [1]
By the space involved, the pattern of facial swelling localises the source. Buccal space infection swells the cheek; canine (infraorbital) space infection swells the upper lip and nasolabial fold and threatens the periorbital tissues; submental space infection swells the region under the chin; and submandibular and sublingual space infection swells the floor of the mouth and the submandibular region. When the submandibular, sublingual and submental spaces are involved together and bilaterally, the diagnosis is Ludwig angina. [2] [4]
The numbers that anchor your viva
A practical distinction the exam rewards is between primary (deciduous) and permanent teeth. Most paediatric odontogenic infections in the under-tens arise from primary molars, and the offending tooth is extracted rather than endodontically treated; infections of permanent teeth in older children and adolescents are managed with both extraction and root-canal options depending on the tooth and the child. Knowing which dentition the child is in shapes the surgical plan. [1] [6]
Epidemiology & Risk Factors
Dental caries is the most prevalent chronic disease of childhood worldwide, and odontogenic infection is its commonest serious complication. Untreated caries progresses to pulpitis, periapical abscess and facial cellulitis in a predictable chain, which is why the burden of odontogenic infection tracks closely with the burden of untreated caries in a population. The PUFA index — recording the visible Pulpal involvement, Ulceration, Fistula and Abscess from untreated caries — was developed to quantify exactly these advanced consequences, and it shows that a substantial fraction of young children in disadvantaged communities already have pus-forming dental disease. [8] [6]
The risk factors divide into those that cause the caries and those that delay its treatment. Frequent sugar consumption, inadequate brushing and lack of fluoride, early colonisation by cariogenic bacteria (often transmitted from a primary caregiver), and infant feeding practices such as prolonged bottle or breast feeding at night all drive caries. Limited access to dental care, cost barriers, remote living and low health literacy delay treatment until infection has spread — which is why odontogenic infection is as much a disease of health inequity as of microbiology. [8] [6]
Ludwig angina itself is uncommon in children compared with adults, but it does occur — most often in a child or adolescent with poor dentition, typically arising from a second or third mandibular molar. The risk of needing intensive care for a paediatric deep neck infection rises with younger age, greater depth of spread, immunocompromise and delayed presentation, which is why the threshold to admit and observe a young child with a spreading odontogenic infection is low. [2] [3]
The microbiology explains both the treatment and the danger. Odontogenic infections are polymicrobial, mixing oral aerobes (viridans streptococci, the Streptococcus anginosus or milleri group) with anaerobes (Prevotella, Porphyromonas, Fusobacterium, Peptostreptococcus). The anaerobic component produces gas, tissue destruction and the characteristic foul odour, and it is the reason that empirical therapy must cover anaerobes — a regimen active against streptococci alone will fail. [5] [10]
Pathophysiology
The teaching model runs from the tooth surface to the deep fascia, and it hinges on the anatomy of the jaw — specifically the muscle attachments that dictate where pus tracks once it perforates the cortical bone. [4] [1]
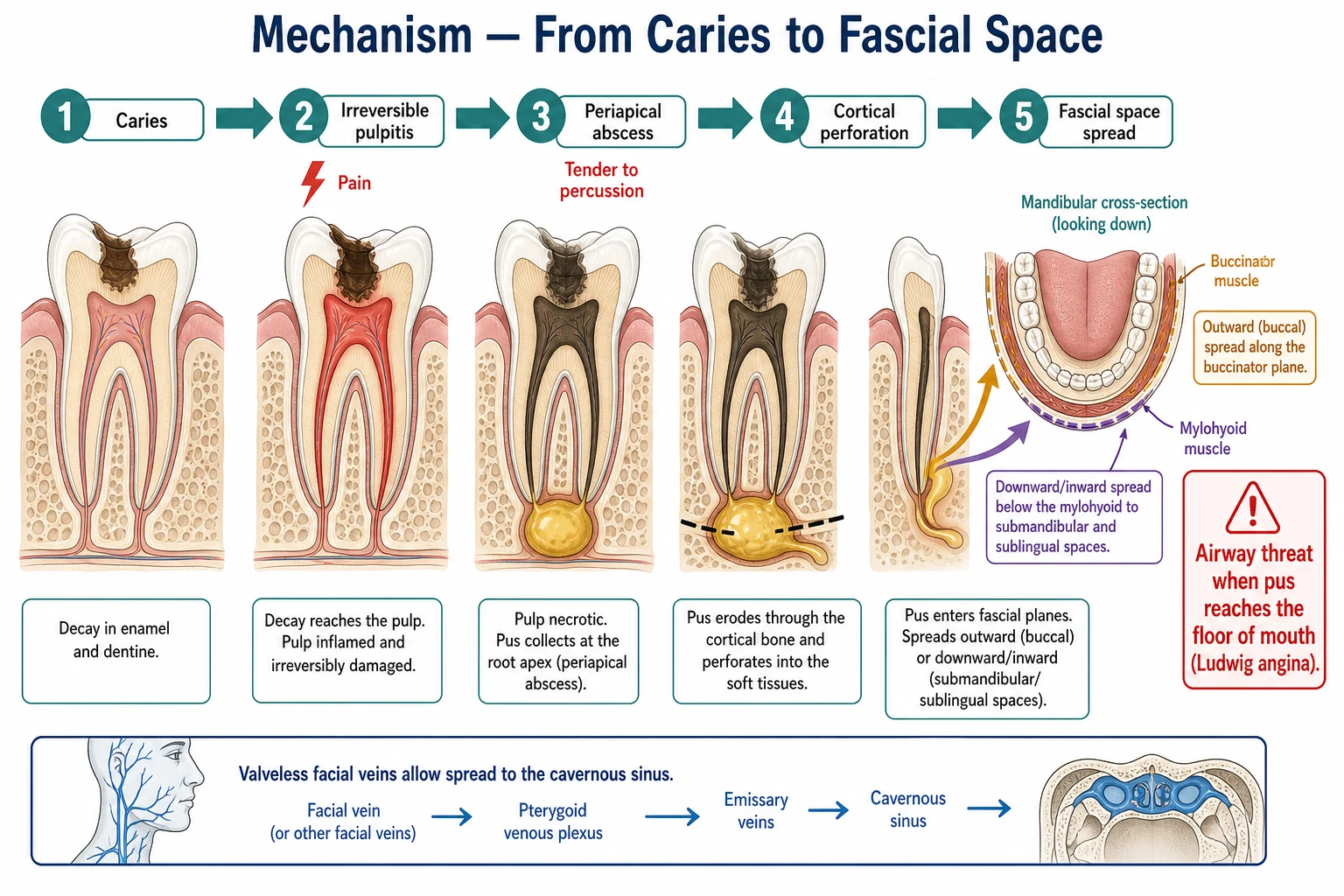
The chain begins with carious destruction of enamel and dentine, which allows bacteria to reach the dental pulp. Early pulpitis is reversible and painful, but as infection progresses the pulp becomes necrotic and the pain may paradoxically settle — a dangerous calm before the abscess forms. Bacteria then escape through the root apex into the periapical tissues, setting up an acute apical periodontitis and, as neutrophils accumulate and pus collects under pressure, a periapical abscess. The tooth becomes tender to percussion, mobile, and painful on biting. [1] [4]
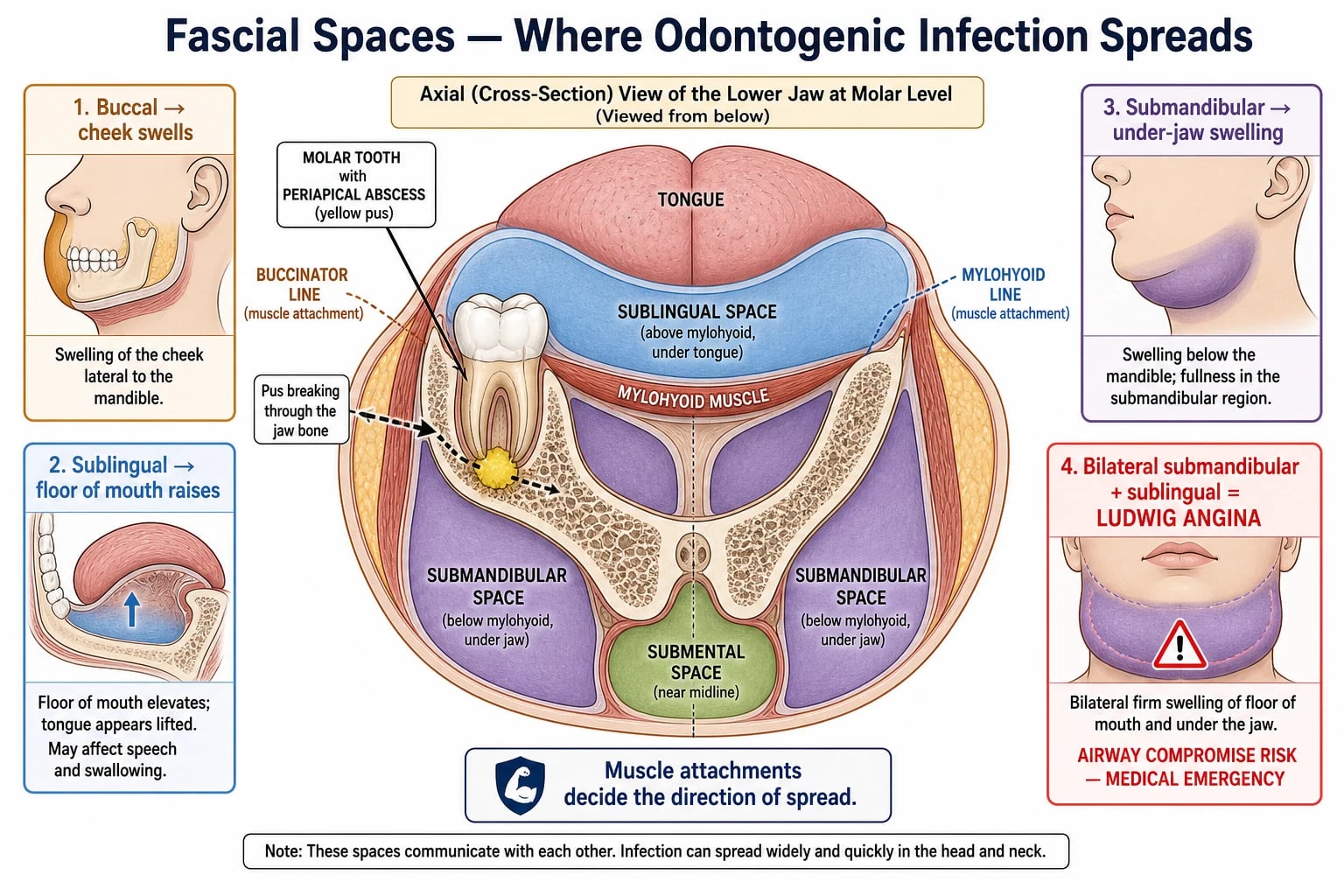
From the periapical region, pus takes the path of least resistance through the cancellous bone. Whether it perforates the buccal or the lingual cortex — and therefore whether it presents as a cheek swelling or a floor-of-mouth swelling — is determined by the relationship of the root apex to the buccinator and mylohyoid muscle attachments on the mandible. Apices lying above the mylohyoid line (the attachment of mylohyoid) track into the buccal or sublingual space; apices below it track into the submandibular space. Maxillary teeth can track into the canine space, the buccal space, or — dangerously — towards the maxillary sinus and orbit. [4] [2]
Ludwig angina is the pathophysiological endpoint that earns the most exam attention. It is a rapidly spreading, bilateral cellulitis — not a single abscess — of the submandibular, sublingual and submental spaces. The infection is typically odontogenic, most often from a mandibular molar, and it produces a woody, brawny induration of the floor of the mouth (because these are closed fascial spaces and the inflammation is a cellulitis rather than a fluctuant collection). The tongue is elevated and pushed upwards and backwards, the floor of the mouth becomes raised and double-ridged, and the airway is progressively obstructed at the tongue base — the mechanism of the drooling, trismus and airway compromise that define the emergency. [2] [9]
A second dangerous pathway is venous spread into the cavernous sinus. The veins of the face — around the upper lip, canine fossa and nose — drain via the ophthalmic veins into the cavernous sinus, and these veins are valveless, so infection can propagate retrogradely. An upper anterior tooth infection that reaches the canine space can therefore produce septic cavernous sinus thrombosis, with proptosis, chemosis, cranial nerve palsies (especially the abducens) and systemic sepsis. The same valveless venous plexus allows infection to spread between the deep neck spaces and down into the mediastinum. [7] [4]
Clinical Presentation
The classic story begins with toothache — often several days of throbbing pain in a carious tooth, worse on biting or with hot and cold — followed by the insidious onset of facial or jaw swelling. The child may have a low-grade fever, malaise and refusal to eat or drink because swallowing and chewing hurt. By the time the family presents, the swelling is usually the dominant feature, and the dental origin may need to be actively sought. [6] [1]
| Picture | Bedside findings | Immediate response |
|---|---|---|
| Localised periapical abscess | Tender tooth, localised gum or facial swelling, well child, low or no fever | Dental review for extraction or endodontic treatment; analgesia; antibiotics only if spreading |
| Spreading odontogenic cellulitis | Firm, warm, tender facial swelling beyond one space; regional nodes; fever and malaise | Identify source tooth; oral or IV antibiotics covering anaerobes; admit if young or unwell |
| Canine space infection | Upper lip and infraorbital swelling; risk of orbital and cavernous sinus spread | Urgent dental and maxillofacial review; IV antibiotics; watch for eye signs |
| Ludwig angina | Bilateral submandibular swelling, woody floor of mouth, raised tongue, drooling, trismus, muffled voice | Emergency: airway first; do not lay flat; anaesthetics, ENT and OMFS; IV antibiotics; theatre |
| Cavernous sinus thrombosis | Proptosis, chemosis, ophthalmoplegia, cranial nerve palsies, toxic | Critical emergency: IV antibiotics, imaging, neurosurgery and ophthalmology |
The localising signs map onto the fascial space involved. A buccal space infection produces a swelling of the cheek that is firm and tender, often with overlying erythema, and the child may be unable to open the mouth fully because of pain and muscle spasm. A canine space infection from a maxillary anterior tooth swells the upper lip and the infraorbital region, and because of the valveless venous drainage the clinician must actively look for early eye signs — eyelid oedema, chemosis or pain on eye movement — that herald orbital or cavernous sinus involvement. [6] [7]
A submandibular or sublingual space infection presents with swelling under the jaw and in the floor of the mouth, drooling, dysphagia and a muffled voice. The child may hold the mouth open to maintain the airway and sit leaning forward. When the submandibular, sublingual and submental spaces are involved together and bilaterally, the picture is Ludwig angina: a firm, bilateral, board-like swelling of the floor of the mouth, a raised and displaced tongue, marked trismus, drooling of saliva, and progressive airway obstruction. [2] [9]
[2] [3]A trap to avoid is the child whose swelling has been treated with oral antibiotics without a dental assessment and who returns with persistent or worsening infection. An established abscess cannot be sterilised by antibiotics alone; persistence means the source tooth has not been managed and the pus has not been drained. A second trap is mistaking odontogenic cellulitis for a non-dental cause — periorbital or orbital cellulitis, salivary gland infection or lymphadenitis — and so missing the source tooth entirely. The dental examination is part of the assessment of every facial swelling in a child. [1] [6]
Differential Diagnosis
Sort the differential into three groups: the non-dental causes of facial swelling, the spreading complications of odontogenic infection, and the deeper mimics. The aim is to identify the source tooth early while maintaining a low threshold to look deeper when the picture does not fit a simple dental abscess. [6] [4]
Odontogenic cellulitis
the core diagnosis
- Tender tooth, caries, firm warm facial swelling
- Polymicrobial oral flora; anaerobic component
- Source control — drainage or extraction — is curative
- Antibiotics for spreading or systemic infection
Periorbital / orbital cellulitis
- Swelling around the eye, often from sinus disease
- Eye signs (proptosis, ophthalmoplegia) = orbital
- Dental cause less common but canine space can spread
- Imaging and IV antibiotics; ophthalmology
Sialadenitis / ranula
- Salivary gland swelling, often unilateral
- Associated with dehydration or stone
- No offending tooth; rises with meals for parotid
- Hydration, massage, sialogogues; treat the cause
Angioedema / allergic
- Rapid onset, non-tender, periorbital and lip swelling
- No fever, no tooth pain, often urticarial
- May compromise airway — assess urgently
- Antihistamine, adrenaline if airway threat
Ludwig angina
- Bilateral submandibular, woody floor of mouth
- Raised tongue, drooling, trismus
- Airway emergency
- Expert airway, IV antibiotics, theatre drainage
Periorbital and orbital cellulitis are the most important mimics when the swelling is around the eye. Periorbital (preseptal) cellulitis is usually from skin or sinus origin and the eye itself is normal; orbital (postseptal) cellulitis is more serious, produces proptosis, ophthalmoplegia and pain on eye movement, and usually arises from ethmoid sinusitis. The reason it matters here is that an upper-tooth canine-space infection can spread towards the orbit, so a child with apparent periorbital cellulitis needs the dentition examined and, if there is any eye sign, urgent imaging. [7] [6]
Acute bacterial sialadenitis (parotitis or submandibular sialadenitis) presents with a tender swelling of the salivary gland, often in a dehydrated child, with pus from the duct on massage and no offending tooth. A ranula is a salivary retention cyst in the floor of the mouth that can mimic sublingual infection but is non-tender and fluctuant without systemic features. Cervical lymphadenitis produces a tender swelling of a lymph node rather than a fascial space, usually without trismus or floor-of-mouth change. Allergic angioedema comes on rapidly, is non-tender and non-pyrexic, and often involves the lips and periorbital tissues; it can compromise the airway and needs urgent assessment. [6] [1]
Among the rarer but dangerous mimics, septic cavernous sinus thrombosis presents with cranial nerve signs, proptosis and chemosis, and is a complication rather than a separate entity — it is most often seeded from an upper-face or dental source through the valveless ophthalmic veins. Recognising it early is essential because it carries a high mortality and needs immediate imaging and broad intravenous therapy. [7]
Clinical & Bedside Assessment
Assessment of a child with facial swelling begins with the airway and the depth of spread, not with the tooth. A child who is drooling, holding the mouth open, sitting forward, or who has stridor or a muffled voice is assessed as a Ludwig or deep space emergency first and a dental problem second. Keep the child in a position of comfort — usually upright and leaning forward — and do not force an intraoral examination until the airway is secure. [2] [3]
The history should establish the timeline of toothache and swelling, any previous dental problems or treatment, the child's immune and vaccination status, and the social context — access to a dentist, remoteness, and the family's ability to return if things worsen. Ask specifically about rapid progression, difficulty swallowing, drooling and any breathing difficulty, because these shift the child into the emergency pathway. [6] [1]
Examination is both extraoral and intraoral. Extraorally, assess the extent, warmth, tenderness and fluctuance of the swelling, the regional lymph nodes, and the airway. Intraorally — in a cooperative and stable child — inspect for the offending tooth: caries, a tender and mobile tooth, localised gingival swelling, or a draining sinus tract on the gum. Palpate the floor of the mouth for the woody induration of Ludwig angina and check for trismus by assessing mouth opening. The single most common error is to examine the face but not the mouth and teeth, and so miss the source. [4] [1]
Deliberately avoid the common errors: laying a child with Ludwig angina flat for examination, which can precipitate complete airway obstruction; forcing a throat or intraoral examination in a child with a compromised airway; prescribing oral antibiotics for a spreading infection without identifying or referring for the source tooth; and failing to reassess a child whose cellulitis is not improving on antibiotics, which signals an undrained collection. The discipline is airway, source, spread — in that order. [2] [5]
Investigations
Odontogenic infection is, in most cases, a clinical diagnosis combined with a dental assessment. The role of investigation is to confirm the source tooth, to define a deep space collection for surgical planning, and to assess severity in the unwell child. [1] [4]
For a localised abscess or spreading cellulitis in a well child, a dental radiograph (a panoramic orthopantomogram, or an intraoral periapical film) confirms the offending tooth and the periapical pathology, and no other imaging is needed. Blood tests are not routinely useful in the well child, although a full blood count and CRP may be taken in the unwell child to track response to treatment. [4] [6]
| Test | When to use it | What it tells you |
|---|---|---|
| Dental radiograph (OPG or periapical) | Most cases — to identify the source tooth | Confirms caries, periapical abscess and the offending tooth |
| Contrast CT of the neck and face | Suspected deep space infection or Ludwig angina | Defines the collection, the spaces involved and airway compromise; guides drainage |
| Ultrasound | Selected superficial collections; some centres | Can identify a drainable collection; operator and child dependent |
| Blood cultures | Toxic or septic child; before antibiotics if possible | Identifies bacteraemia; positive in a minority |
| Full blood count, CRP | Unwell or admitted child; tracks response | Supports severity assessment and response to therapy |
When a deep space infection or Ludwig angina is suspected, the investigation of choice — once the airway is secure — is contrast-enhanced computed tomography (CT) of the neck and face. CT defines the collection, its size, the fascial spaces involved, the extent of airway compromise, and any mediastinal extension or cavernous sinus involvement. It also distinguishes a drainable abscess from cellulitis, which guides the decision to operate. Airway safety always takes precedence over imaging — a child with a threatened airway should not be sent to the scanner unaccompanied or without a plan for securing the airway. [2] [3]
Blood cultures should be taken in the toxic or septic child, preferably before antibiotics are given, although they are positive in only a minority because the infection is usually localised. In suspected cavernous sinus thrombosis, contrast CT or MR venography of the orbits and cavernous sinus confirms the diagnosis and is performed as soon as the child is stabilised. [7] [3]
Management — Resuscitation
For the child with a spreading or deep space odontogenic infection, the priority shifts from the routine dental pathway to airway protection, sepsis management and surgical planning. The first step is to assess and secure the airway: a child with drooling, stridor, a raised floor of mouth or a displaced tongue is managed in a position of comfort, kept calm, and assessed by an anaesthetist with ENT and oral-maxillofacial surgery at the bedside. Do not lay the child flat and do not instrument the oropharynx or floor of mouth without airway expertise, because either can precipitate complete airway obstruction. [2] [9]
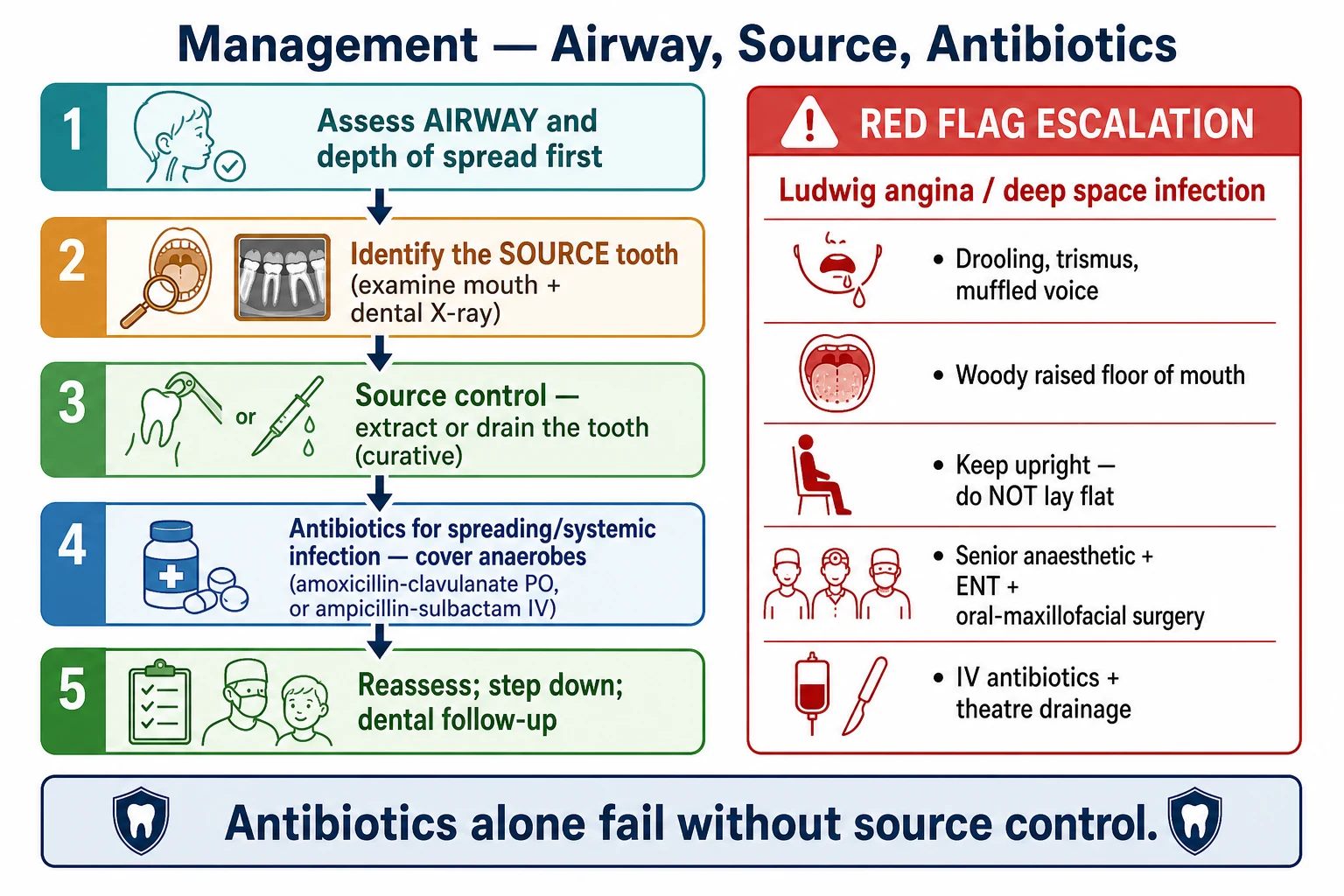
Obtain intravenous access, take blood cultures and inflammatory markers, and start broad-spectrum intravenous antibiotics covering oral aerobes and anaerobes. Empirical regimens include ampicillin-sulbactam, or clindamycin (with metronidazole added for deeper pelvic-style anaerobic cover), or ceftriaxone plus metronidazole — adjusted to local resistance patterns and guidelines. A child with signs of sepsis is resuscitated with intravenous fluids and managed by the paediatric sepsis pathway; the Phoenix sepsis score of two or more identifies the child needing escalation. [5] [2]
The airway in Ludwig angina deserves specific emphasis because it is where deaths occur. Intubation is anatomically difficult — the tongue is displaced, the floor of mouth is distorted, and there is often blood and pus — so the airway is secured by senior anaesthetic help, often with awake fibre-optic intubation, and a surgical airway (cricothyroidotomy or tracheostomy) must be immediately available as a backup. The child is taken to theatre for drainage and extraction once the airway is controlled. [2] [9]
For the much larger group of well children with localised infection, resuscitation simply means analgesia and antipyretics — paracetamol and ibuprofen, weight-based and regular — and encouragement of oral fluids. Good pain relief is also the key to a cooperative child who can undergo a dental examination and extraction. [6]
Management — Definitive & Stepwise
The definitive management of odontogenic infection rests on a single principle that overrides all others: source control. An established abscess is a collection of pus under pressure in a closed space, and antibiotics cannot sterilise it. The offending tooth must be extracted or undergo endodontic treatment, and any collection must be drained surgically. Antibiotics are adjuncts for spreading cellulitis or systemic infection, not substitutes for drainage. [1] [4]
Grading the severity to drive the pathway
Emergency
Ludwig angina or deep space infection; airway risk; IV antibiotics, contrast CT, theatre drainage and extraction
Step one — airway and severity. Assess the airway and the depth of spread first. A child with drooling, trismus, a raised floor of mouth or a muffled voice is managed as a Ludwig or deep space emergency with senior airway help. A well child with a localised swelling is managed electively or urgently according to the degree of spread. [2] [3]
Step two — identify and control the source. Locate the offending tooth by dental examination and radiograph. For a primary tooth, the source is usually extracted; for a permanent tooth, endodontic (root canal) treatment or extraction is chosen depending on the tooth and the child. Any fluctuant collection is incised and drained. This is the step that cures the infection; antibiotics without it will fail. [1] [4]
Drugs in paediatric odontogenic infection
Step three — antibiotics for spreading or systemic infection. For a well child with a drained localised abscess, antibiotics are often unnecessary after source control. For spreading cellulitis or systemic features, give oral amoxicillin-clavulanate or amoxicillin plus metronidazole; for moderate to severe or deep space infection, give intravenous ampicillin-sulbactam, or clindamycin (with metronidazole for deepest cover), or ceftriaxone plus metronidazole. Antibiotics are reviewed daily and stepped down to oral as the child improves and the source is controlled. [5] [10]
The stepwise pathway
Assess the airway and depth of spread first; escalate drooling, trismus, raised floor of mouth or a muffled voice as Ludwig or deep space infection.
Identify the offending tooth by dental examination and radiograph; map the swelling to its fascial space.
Control the source — extract or endodontically treat the tooth and drain any collection; this is curative.
Give antibiotics only for spreading cellulitis or systemic infection; cover oral aerobes and anaerobes.
For Ludwig angina — secure the airway with senior help, give IV antibiotics, and take to theatre for drainage and extraction.
Reassess daily; step down to oral antibiotics once the source is controlled and the child improves; arrange dental follow-up.
Step four — the role of corticosteroids and adjuncts in Ludwig angina. High-dose corticosteroids (for example dexamethasone) are used in some centres to reduce oedema and improve trismus and airway patency, but the evidence is limited and their use remains controversial; they are an adjunct rather than a substitute for airway control, antibiotics and drainage. The decision is made by the treating surgical and intensive-care team and is not routine. [9]
DRAIN
Specific Subtypes & Scenarios
Ludwig angina is the subtype most often examined. It is a bilateral, rapidly spreading cellulitis of the submandibular, sublingual and submental spaces, usually from a mandibular molar, producing the characteristic woody floor-of-mouth induration, raised and displaced tongue, drooling, trismus and progressive airway obstruction. The infection is a cellulitis in a closed fascial space rather than a drainable abscess, which is why the floor of mouth feels hard rather than fluctuant. Management is airway first, broad-spectrum intravenous antibiotics, and surgical decompression and extraction in theatre; mortality has fallen from over fifty per cent in the pre-antibiotic era to around eight per cent with modern airway and surgical care. [2] [9]
Facial cellulitis of odontogenic origin is the common paediatric presentation — a school-age child with a carious molar, a firm tender facial swelling and a low fever. The key is to recognise the dental source, which is easily missed when the swelling dominates the picture, and to arrange dental extraction and oral antibiotics rather than antibiotics alone. A child who is young, systemically unwell, or unable to tolerate oral intake is admitted for intravenous antibiotics and source control. [6] [1]
Bridwell, Gottlieb, Koyfman 2021 — Am J Emerg Med (PMID 33383265)
Evidence-based narrative review of Ludwig angina
Key finding
Ludwig angina is a rapidly progressive bilateral cellulitis of the submandibular, sublingual and submental spaces; airway protection is the priority, with broad-spectrum antibiotics (ampicillin-sulbactam first-line, clindamycin plus a third-generation cephalosporin as an alternative) and early surgical drainage. Corticosteroids are used adjunctively in some centres but the evidence is limited.
Practice change
The modern management of Ludwig angina combines early airway security, anaerobe-covering intravenous antibiotics and surgical source control — the principles that have reduced mortality from over fifty per cent to single digits.
Canine space and cavernous sinus involvement from a maxillary anterior tooth is the subtype that threatens the eye and brain. Swelling of the upper lip and infraorbital region, with any eye sign, demands urgent imaging for orbital or cavernous sinus extension. Septic cavernous sinus thrombosis presents with proptosis, chemosis, ophthalmoplegia (especially lateral gaze palsy from abducens involvement), cranial nerve signs and systemic sepsis, and it is managed with broad intravenous antibiotics, imaging and multidisciplinary care. [7]
Immunocompromised children — those on chemotherapy, post-transplant, or with primary immunodeficiency — may present with atypical or rapidly progressive infection, a broader microbial differential including resistant organisms and fungi, and less localising signs. The threshold for intravenous antibiotics, imaging and surgical consultation is lower, and microbiological sampling is more aggressive. [3] [5]
Complications & Pitfalls
The complications of odontogenic infection divide into local, deep space and distant. Local complications include tooth loss, facial scarring and the formation of a chronic sinus tract or periapical granuloma. Deep space complications are the airway and life threats: Ludwig angina itself, parapharyngeal and retropharyngeal spread, and descending necrotising mediastinitis. Distant complications include septic cavernous sinus thrombosis, orbital cellulitis and brain abscess, and bacteraemic sepsis. [4] [7]
| Complication | Recognise it by | Key action |
|---|---|---|
| Ludwig angina | Bilateral submandibular swelling, woody floor of mouth, raised tongue, drooling, trismus | Airway first; IV antibiotics; theatre drainage and extraction |
| Parapharyngeal / retropharyngeal spread | Neck stiffness, torticollis, toxic appearance, deep neck fullness | Contrast CT neck; IV antibiotics; surgical drainage if large or failing |
| Descending necrotising mediastinitis | Chest pain, septic shock, mediastinal air or fluid | Emergency surgical drainage of neck and mediastinum; ICU |
| Cavernous sinus thrombosis | Proptosis, chemosis, ophthalmoplegia, cranial nerve palsies | IV antibiotics, imaging (CT or MR venography), multidisciplinary care |
| Orbital cellulitis | Proptosis, pain on eye movement, ophthalmoplegia | Imaging; IV antibiotics; ophthalmology and ENT |
| Bacteraemia / sepsis | High fever, tachycardia, poor perfusion, altered mentation | Paediatric sepsis pathway; cultures; IV antibiotics and source control |
The danger of each complication rises with its rarity and depth. Descending necrotising mediastinitis occurs when infection tracks from the deep neck spaces down the danger space into the mediastinum, and it carries a mortality of twenty-five to forty per cent even with aggressive surgery. Cavernous sinus thrombosis remains lethal in a substantial fraction of cases despite antibiotics. Each is prevented by the same discipline: identify the source early, drain the pus, cover anaerobes, and escalate the airway-threat signs without delay. [2] [7]
The fellowship-level pitfalls are where marks are lost. The first is treating a spreading infection with antibiotics alone without source control — the single most common and most dangerous error. The second is missing the source tooth by examining the face but not the mouth. The third is laying a child with Ludwig angina flat or forcing an intraoral examination, which can precipitate airway obstruction. The fourth is mistaking odontogenic cellulitis for periorbital or salivary disease and so delaying dental referral. Each is prevented by the same sequence: airway, source, spread. [1] [2]
Prognosis & Disposition
The prognosis of a localised periapical abscess treated with extraction or drainage is excellent: pain resolves rapidly once the tooth is managed and the pus is drained, and the child recovers fully within days. Spreading cellulitis treated with source control and appropriate antibiotics also resolves well, with the child becoming afebrile and the swelling settling over forty-eight to seventy-two hours. [1] [6]
Disposition is decided by the depth of spread and the airway. A well child with a drained localised abscess or controlled cellulitis is managed as a day case or outpatient with dental follow-up. A child with spreading cellulitis, young age, systemic features or poor oral intake is admitted for intravenous antibiotics and source control. A child with Ludwig angina or deep space infection is managed in theatre and then in high-dependency or intensive care, because the airway can deteriorate and because these children need close observation after surgical decompression. [2] [3]
[2] [1]Ludwig angina, historically lethal, now survives in the great majority of children when the airway is secured early and surgical source control is prompt. The long-term outlook for the dentition depends on the underlying caries and access to ongoing dental care — which is why every episode of odontogenic infection should end with a dental follow-up plan and, where appropriate, a preventive oral-health programme. For disadvantaged and remote children, the corrective is sustained dental access, not repeated emergency surgery. [8] [9]
Special Populations
Aboriginal and Torres Strait Islander children, and children in remote Australia and the Pacific, carry a far higher burden of untreated caries and its complications than the general population. They present later, with more advanced infection, and they are over-represented among children needing theatre and intensive care for odontogenic infection. The response is both immediate — prompt recognition, source control and anaerobe-covering antibiotics — and structural: culturally safe, publicly funded oral health programmes, fluoridation, and improved access to dental care. [8] [6]
Young children, particularly preschoolers, are at higher risk of rapid progression and airway compromise because their airways are small and their fascial spaces are compact, and they may not localise or report pain reliably. The threshold to admit and observe a preschool child with a spreading odontogenic infection is low, and dental treatment often requires general anaesthesia because the child cannot cooperate. [3] [1]
Immunocompromised children — on chemotherapy, post-transplant, or with primary immunodeficiency — may have muted signs, atypical organisms and rapid progression. They need a lower threshold for imaging, intravenous antibiotics and surgical consultation, and broader microbiological sampling. Children with disability or who are unable to cooperate with dental examination usually need management under general anaesthesia for both assessment and treatment. [3] [5]
Adolescents with erupting third molars are a specific group at risk of pericoronitis and its spread into the submandibular and sublingual spaces, and they may present with the early features of Ludwig angina. A painful, swollen gum over a partially erupted wisdom tooth with trismus in an adolescent warrants dental assessment and close observation. [2] [4]
Evidence, Guidelines & Regional Differences
| Region | Guideline / source | Empirical emphasis | First-line antibiotics |
|---|---|---|---|
| ANZ | RCH Melbourne, Therapeutic Guidelines | Source control first; admit young or unwell children; anaerobe cover | Amoxicillin-clavulanate orally; ampicillin-sulbactam or clindamycin IV |
| UK | NICE / CKS, SIGN | Dental referral for source; antibiotics only for spreading infection | Amoxicillin or amoxicillin-clavulanate; metronidazole if deeper |
| North America | AAOMS Parameters of Care | Surgical source control; airway in Ludwig; broad IV cover | Ampicillin-sulbactam; clindamycin plus cephalosporin |
| Remote / Indigenous | National oral health guidance | Lower threshold to admit; access and prevention focus | As above; ensure dental follow-up and preventive care |
The evidence backbone rests on clinical and surgical series rather than large randomised trials, which is appropriate for a condition defined by anatomy and source control. The 2024 Oral and Maxillofacial Surgery Clinics review of paediatric odontogenic infections (Teal and colleagues) provides the contemporary framework for classification and management in children. The evidence-based review of Ludwig angina (Bridwell and colleagues, 2021) establishes the modern ED approach — airway first, broad-spectrum anaerobe-covering antibiotics, early surgical drainage — and documents the fall in mortality. The review of paediatric deep neck infection and the risk of needing intensive care (Perina and colleagues, 2022) quantifies the factors that predict severity in children. [1] [2] [3]
The antimicrobial evidence is summarised in the update on antimicrobial therapy in odontogenic infection (Caruso and colleagues, 2022) and the general review of antibiotic therapy in dentistry (Ahmadi and colleagues, 2021), which support the empirical regimens above and emphasise stewardship — antibiotics for spreading or systemic infection, not for a well child with a drained abscess. The narrative review of corticosteroids in Ludwig angina (Tami and colleagues, 2020) captures the live controversy around adjunctive steroids. The review of septic cavernous sinus thrombosis (Caranfa and Yoon, 2021) and the PUFA index (Monse and colleagues, 2010) complete the picture of complication and epidemiology respectively. [5] [10] [9] [7] [8]
The live areas of nuance are the choice between ampicillin-sulbactam and clindamycin-based regimens (guided by local resistance and allergy), the role of corticosteroids in Ludwig angina, the duration of intravenous therapy, and the threshold for CT in deep space infection. A fellowship candidate shows depth by naming the principle of source control and the airway-first approach rather than reciting a single antibiotic. [2] [1]
Exam Pearls
The single discipline that keeps children safe is the same one that earns fellowship marks: find the source tooth and drain or extract it, cover anaerobes when the infection is spreading, and treat the child with drooling, trismus and a raised floor of mouth as Ludwig angina — an airway emergency managed by senior teams in theatre, not by antibiotics alone in the community. [1] [2]
And when you teach this topic, teach it as a model of source control and airway vigilance — a common childhood infection where the modern default is dental extraction and targeted antibiotics, but where the rare child whose dental abscess has become Ludwig angina depends on you having looked at the floor of the mouth and secured the airway before anything else. [6] [3]
References
- [1]Teal L, Sheller B, Susarla HK. Pediatric Odontogenic Infections. Oral Maxillofac Surg Clin North Am, 2024.PMID 38777729
- [2]Bridwell R, Gottlieb M, Koyfman A, Long B. Diagnosis and management of Ludwig's angina: An evidence-based review. Am J Emerg Med, 2021.PMID 33383265
- [3]Perina V, Szaraz D, Harazim H, et al. Paediatric Deep Neck Infection—The Risk of Needing Intensive Care. Children (Basel), 2022.PMID 35883963
- [4]Bertossi D, Barone A, Iurlaro A, et al. Odontogenic Orofacial Infections. J Craniofac Surg, 2017.PMID 27930461
- [5]Caruso SR, Yamaguchi E, Portnof JE. Update on antimicrobial therapy in management of acute odontogenic infection in oral and maxillofacial surgery. Oral Maxillofac Surg Clin North Am, 2022.PMID 34728145
- [6]Giunta Crescente C, Soto de Facchin M, Acevedo Rodriguez AM. Medical-dental considerations in the care of children with facial cellulitis of odontogenic origin. A disease of interest for pediatricians and pediatric dentists. Arch Argent Pediatr, 2018.PMID 30016031
- [7]Caranfa JT, Yoon MK. Septic cavernous sinus thrombosis: A review. Surv Ophthalmol, 2021.PMID 33831391
- [8]Monse B, Heinrich-Weltzien R, Benzian H, Holmgren C, van Palenstein Helderman W. PUFA—an index of clinical consequences of untreated dental caries. Community Dent Oral Epidemiol, 2010.PMID 20002630
- [9]Tami A, Othman S, Sudhakar A, Bell RB, Garg M. Ludwig's angina and steroid use: A narrative review. Am J Otolaryngol, 2020.PMID 32035654
- [10]Ahmadi H, Ebrahimi A, Ahmadi F. Antibiotic therapy in dentistry. Int J Dent, 2021.PMID 33574843