Paeds · mental-behavioural-and-psychosomatic
Conduct disorder and antisocial behaviour
Also known as Conduct disorder · Antisocial behaviour in children · Disruptive behaviour disorder · Aggressive behaviour in children · CD
Fellowship guide to conduct disorder and antisocial behaviour in children: the rights-violation definition, the Moffitt developmental taxonomy, the callous-unemotional specifier, the biopsychosocial coercion-loop model, and a NICE CG158 stepped-care ladder built on evidence-based parenting programmes (Incredible Years, Triple P, PCIT, MST) rather than medication, with ANZ/UK/US guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the ten-year-old who has been suspended twice for fighting, whose teacher describes cruelty to younger children at lunchtime, and whose mother — exhausted and frightened — tells you he steals from her purse and will not come home until midnight. The defining feature is not that he is "naughty" or even that he is angry; it is that his behaviour crosses a line into violating the rights of others or breaking major social rules, and that it does so persistently and outside the developmental norm. [4]
Conduct disorder is a behavioural syndrome, not a single broken circuit, and it sits at the severe end of the disruptive-behaviour spectrum that runs from ordinary boundary-testing, through oppositional defiant disorder, to frank rights-violating conduct. What makes it a disorder is the triad of persistence (at least twelve months, with at least one symptom in the past six months), pervasiveness (more than one setting, or clearly impairing), and severity (the rights of others or major norms are actually violated, not merely bent). [4]
The reason the definition matters in clinic is that it tells you where to look next. A child whose behaviour fits conduct disorder needs an assessment of risk to self and others, a search for comorbidity (especially ADHD, which is the commonest travelling partner, and trauma), a developmental history that places the child on the Moffitt taxonomy, and a plan that almost always begins with the family rather than the child alone. [1] [4]
Classification
Conduct problems sort into a small number of clinically important shapes, and each shape changes what you do. The most useful first cut is the disruptive-behaviour spectrum: oppositional defiant disorder is the angry, defiant, argumentative child who has not yet crossed into aggression or rights violation; conduct disorder is the child who has; and antisocial personality disorder is the possible adult endpoint — never diagnosed under eighteen, but predicted by persistent childhood-onset conduct disorder. [4]
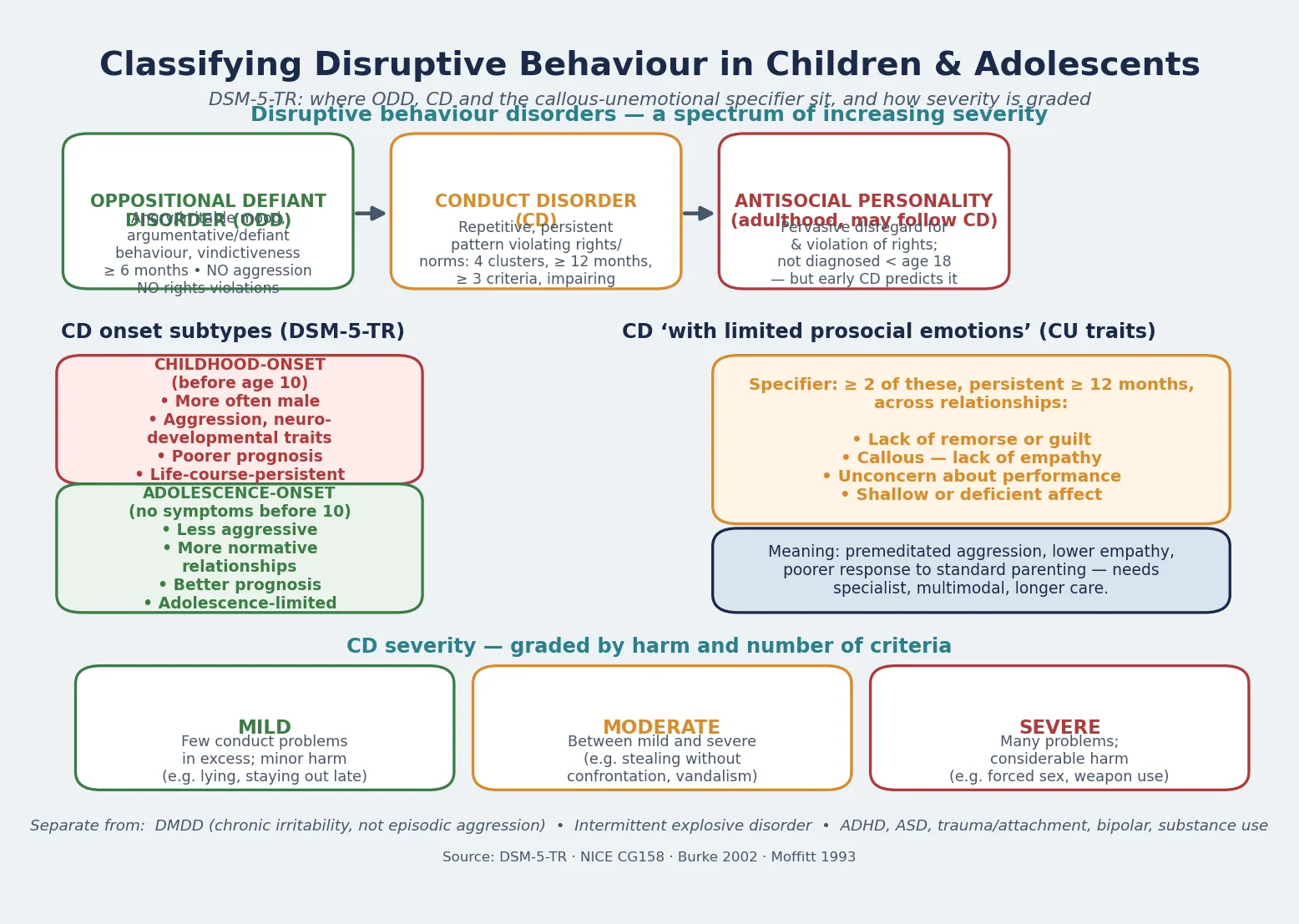
Within conduct disorder itself, DSM-5-TR distinguishes two onset subtypes that carry different prognoses. Childhood-onset conduct disorder (at least one symptom before age ten) is more often seen in boys, is more aggressive and neurodevelopmentally loaded, and tracks with Moffitt's life-course-persistent trajectory and a poorer adult outcome. Adolescence-onset conduct disorder (no symptoms before ten) is less aggressive, tends to retain normative social bonds, and aligns with the adolescence-limited trajectory that usually desists as maturity and adult roles arrive. [1] [4]
The single most prognostically important specifier is "with limited prosocial emotions," applied when a child shows at least two of the following persistently across relationships for twelve months or more: lack of remorse or guilt, callous lack of empathy, unconcern about performance at school or home, and shallow or deficient affect. These are the callous-unemotional (CU) traits, and their presence marks a more severe, premeditated, stable and treatment-resistant form of conduct disorder that demands specialist multimodal care rather than a community parenting group alone. [4]
Severity is then graded by the number of conduct problems beyond the minimum and the degree of harm: mild (few problems, minor harm such as lying or staying out late), moderate (an intermediate number, such as stealing without confrontation or vandalism), and severe (many problems with considerable harm, such as forced sex, cruelty, weapon use, or breaking and entering). [4]
Epidemiology & Risk Factors
Conduct disorder is among the commonest mental-health diagnoses of middle childhood and adolescence, and its burden falls hardest on the children already carrying the most adversity. Community surveys put the prevalence of conduct disorder at roughly two to five percent of children and adolescents, rising with age and more frequent in boys before adolescence; the Erskine global-burden analysis ranked conduct disorder among the leading contributors to disability in young people, with high comorbidity and a large unmet-treatment gap. [3] [4]
Headline numbers for viva
Risk amplifiers cluster at every level of the child's ecology. At the child level they are male sex, a difficult and sensation-seeking temperament, neurodevelopmental vulnerability, and callous-unemotional traits; at the family level they are harsh, inconsistent or coercive parenting, abuse and neglect, parental mental illness or substance use, family violence, and parental antisocial behaviour; and at the community level they are poverty, neighbourhood instability, school failure and exclusion, and a deviant peer group. The children at highest risk are those in out-of-home care, the youth-justice system, and Indigenous and socioeconomically disadvantaged communities, where adversity, intergenerational trauma, and thin service access compound. [1] [4]
The reason this matters is that the risk profile is also the treatment profile: the same coercion, trauma, and instability that cause conduct disorder are the levers an intervention must move, which is why a parenting programme delivered into an unsafe or unsupported home will disappoint. [2] [5]
Pathophysiology
There is no single broken gene or circuit to name. The model that best fits the evidence is biopsychosocial and developmental: a child carrying a vulnerable temperament and neurobiology meets an adverse, coercive environment, and the interaction — reinforced over years — locks in a persistent antisocial trajectory. [1] [8]
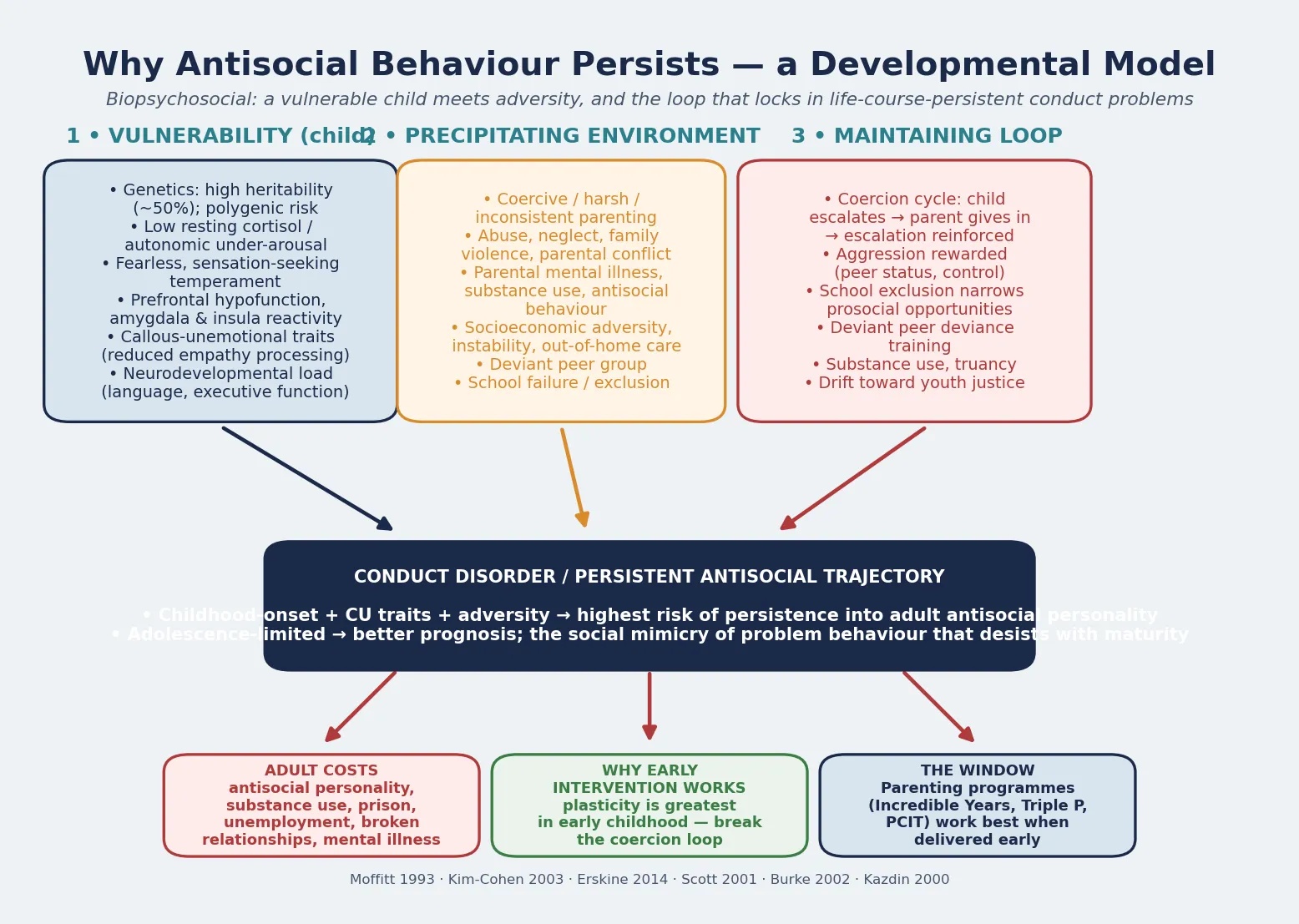
At the child level the threads are high heritability (around fifty percent), autonomic under-arousal with low resting cortisol (the fearless, stimulation-seeking child), reduced prefrontal inhibitory control with amygdala and insula differences, and — for the callous-unemotional subgroup — reduced processing of others' distress and fear. At the environment level the threads are harsh and inconsistent parenting, abuse, neglect and family violence, parental mental illness and substance use, socioeconomic adversity, school failure, and deviant peers. [1] [4]
The mechanism that turns these into a persistent problem is the coercion cycle: the child escalates, the exhausted parent gives in to end the conflict, and escalation is thereby reinforced and refined. Aggression is then further rewarded by peer status and control, school exclusion narrows prosocial opportunities, and the child drifts toward a deviant peer group, substance use, and the youth-justice system. This loop is the reason early childhood is the window of greatest leverage — brain plasticity and the still-forming parent-child relationship mean a parenting intervention delivered at four can prevent the trajectory that is much harder to shift at fourteen. [1] [5]
The developmental taxonomy ties this together. Moffitt's life-course-persistent form arises when neuropsychological vulnerability meets sustained adversity from early childhood; it is uncommon but carries the worst adult outcome, including antisocial personality, substance use, and imprisonment. The adolescence-limited form is far commoner, arises from social mimicry of antisocial peers against a near-normal temperament, and usually desists as adult roles and maturity arrive. Knowing which a child sits on is the single most useful prognostic judgement you make. [1] [8]
Clinical Presentation
The child in front of you rarely presents with "conduct disorder" as a complaint. What you see is behaviour that scares people: a parent who is frightened of her own child, a teacher who has given up, a school asking for help after a suspension, or a youth-justice worker requesting a developmental assessment. The behaviour falls into the four DSM-5-TR clusters — aggression to people and animals, destruction of property, deceit or theft, and serious violation of rules. [4]
The aggression cluster is the one that brings children to attention earliest: bullying, initiating fights, using a weapon, forcing someone into sexual activity, and physical cruelty to people or animals. The destruction cluster is fire-setting and deliberate property damage; the deceit cluster is breaking into a house or car, lying for goods or favours, and stealing; and the rule-violation cluster is staying out at night before age thirteen, running away from home, and being truant. The severity and the cluster mix change with age and trajectory. [4]
Preschool children rarely meet full criteria but show the precursors — severe, persistent aggression and defiance that do not respond to normal parenting — and these early-onset problems are the single best predictor of life-course-persistent conduct disorder, so they are the population in which evidence-based parenting programmes pay the largest dividend. School-age children present with fighting, cruelty, stealing, lying, truancy and school exclusion, often with comorbid ADHD and learning problems. Adolescents add rule-breaking that overlaps with offending — running away, staying out, substance use, and sexual aggression — and the adolescence-limited form is commonest here. [1] [4]
The comorbidity is the rule, not the exception, and it changes management. ADHD is the commonest travelling disorder and, untreated, both drives and maintains antisocial behaviour, so its recognition and treatment is one of the most effective things you can do for a child's conduct problems. Anxiety, depression, substance use, specific learning disorders, autism, and the sequelae of trauma and attachment disruption all coexist and must be assessed in parallel. [4] [8]
Differential Diagnosis
Build the differential in four piles so you do not anchor on the obvious label: behaviours that look like conduct disorder but are something else, things that travel with it, dangerous mimics, and the normal extremes of childhood defiance. Several are quickly separated by the quality and context of the behaviour. [4]
The discriminator you must never miss is trauma: a child whose aggression flares in response to perceived threat, who is hypervigilant, and who has a history of abuse, neglect, domestic violence, or disrupted attachments may be reacting to danger rather than choosing antisocial behaviour, and a punitive or purely behavioural plan will fail and may retraumatise. Equally, an adolescent with new, escalating, affectively driven risk-taking after puberty is not "just conduct disorder" until bipolar disorder, substance use, and an emerging psychotic illness have been considered. [4]
Finally, separate conduct disorder from the normal extremes of childhood and adolescence — ordinary boundary-testing, the moody withdrawal of early adolescence, and the rule-bending of peer-influenced teenagers — which are time-limited, responsive to consistent parenting, and do not violate the rights of others. [4]
Clinical & Bedside Assessment
The assessment is a structured, multi-informant interview, not a behaviour-rating score. You need the child, the parent or carer, the school, and — where relevant — youth justice and social care, because adolescents under-report antisocial behaviour and parents and teachers each see a different slice. The history establishes the nature, onset, persistence and severity of the conduct problems, the developmental trajectory, the comorbidities, and — above all — the ecological context of family, adversity and trauma that the plan must address. [4]
CASES
The mental state and behavioural examination documents the child's cooperativeness, empathy and remorse (or their absence), the presence of callous-unemotional features, any mood, anxiety, psychotic or manic content, and — in adolescents — substance use and suicidality. A standardised instrument such as the Eyberg Child Behaviour Inventory or the Strengths and Difficulties Questionnaire can support screening, severity grading and tracking, but it does not make the diagnosis; the diagnosis is clinical. [6] [4]
You must assess risk explicitly at every contact — risk to the child (from their own behaviour, from retaliation, from abuse at home), risk to others (siblings, peers, animals), and access to means such as weapons or fire. Document the risk assessment, the safeguarding considerations, and the multi-agency plan, and recognise that conduct problems emerging after abuse, neglect, or family violence are as much a safeguarding problem as a behaviour problem. [2] [4]
Investigations
There is no blood test or scan for conduct disorder. Investigations are about excluding mimics, mapping comorbidity, and finding the unmet developmental or health needs that drive the behaviour — not confirming a label. In a typical first assessment, focused history and examination are the core; tests are added when the picture points elsewhere. [4]
Where the history suggests it, screen for substance use, sexual-health needs, and the consequences of risk-taking behaviour, and consider a physical examination for the signs of abuse, neglect, or self-harm. The most important "investigation" in this condition is often a school visit or collateral — the teacher who sees the child every day will tell you more about onset, severity and the unmet need than any laboratory test. [4] [6]
Management — Resuscitation
"Resuscitation" for a behavioural disorder means safety first. Before you discuss a parenting programme or a therapy plan, you must answer one question: is this child — and are the people around this child — safe between now and the next contact? Weapon use, cruelty, sexual aggression, fire-setting, or escalating risk to others are behavioural emergencies that need a safeguarding review and a multi-agency plan the same day. [2] [4]
The immediate bundle is a named, written risk-and-safeguarding plan: the specific risks, the triggers, the adults responsible in each setting, the access-to-means restrictions (especially weapons and fire), and the named clinician and review date. Inpatient admission is rarely the answer for conduct disorder itself, and is reserved for acute comorbid crisis — active self-harm, suicidality, or a psychotic or affective illness — because a hospital ward neither treats nor contains antisocial behaviour well. [4]
Management — Definitive & Stepwise
Once safety is secured, treatment is stepped — the intensity matches the severity, and every plan is built around the family system, not imposed on the child alone. The NICE guideline on antisocial behaviour and conduct disorders in children is explicit about this ladder, and the evidence base is overwhelmingly psychosocial rather than pharmacological. [5] [9]
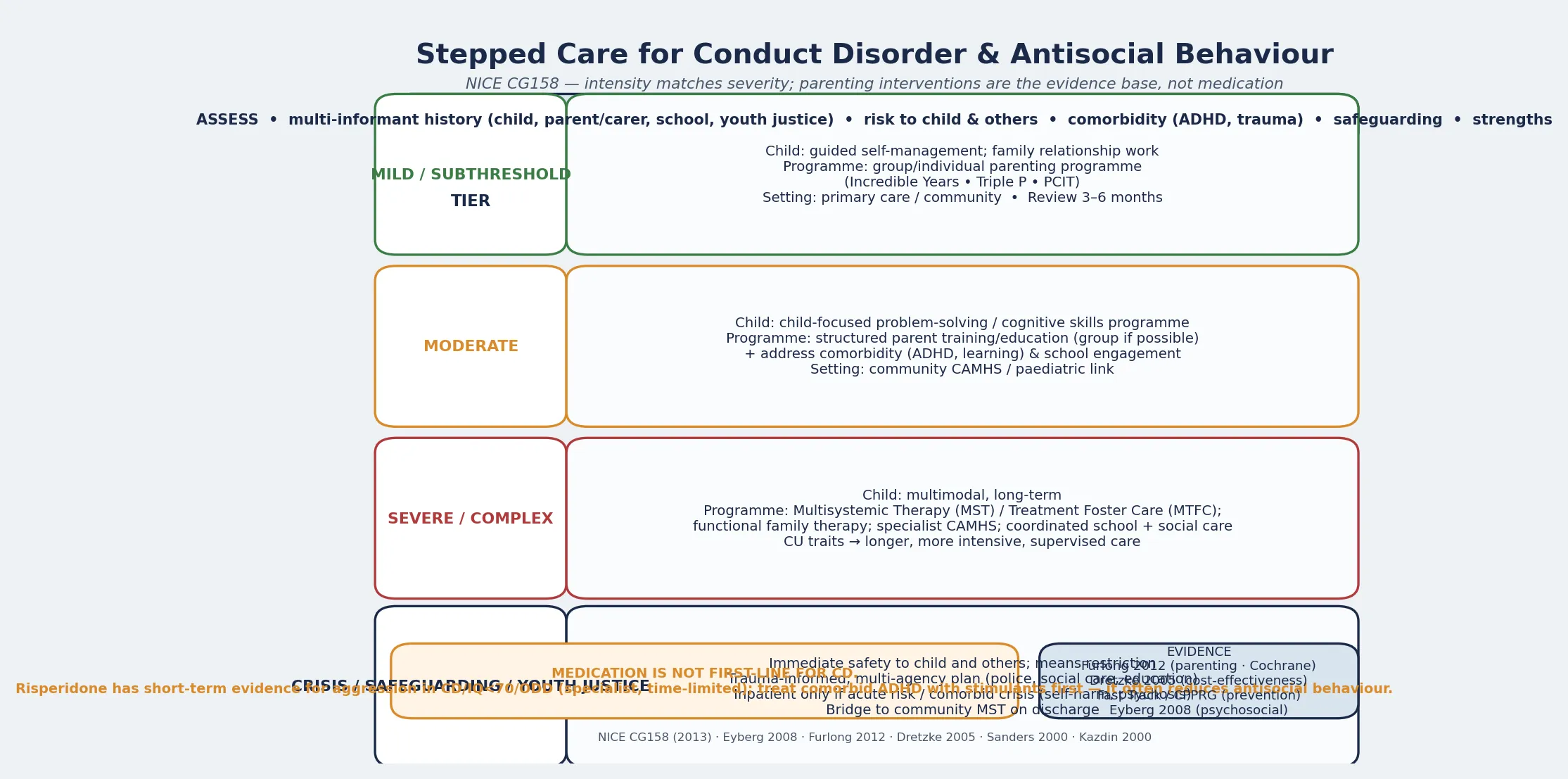
For mild or subthreshold problems, the first-line intervention is a group or individual parenting programme — the Incredible Years series, the Triple P (Positive Parenting Program), or Parent-Child Interaction Therapy (PCIT). The Cochrane review by Furlong and colleagues found that behavioural and cognitive-behavioural group-based parenting programmes produce clinically important reductions in child conduct problems in the three-to-twelve age range, and the Sanders trial of Triple P showed that even standard and self-directed delivery helps families of children with early-onset conduct problems. [5] [7]
For moderate conduct disorder, the ladder adds a structured parent-training or parent-education programme, ideally in a group, alongside a child-focused problem-solving or cognitive-skills programme, while comorbidity (ADHD, learning problems) and school engagement are addressed in parallel. The Dretzke health-technology assessment confirmed that parent-training programmes are both effective and cost-effective for conduct disorder and oppositional defiant disorder in children. [9] [6]
Stepped-care ladder (NICE CG158)
Mild / subthreshold → group or individual parenting programme (Incredible Years, Triple P, PCIT); guided child self-management; primary-care or community setting; review at 3–6 months
Moderate → structured parent training/education (group where possible) + child problem-solving/cognitive skills programme; treat comorbid ADHD and learning needs; community CAMHS link
Severe / complex → multimodal, long-term: Multisystemic Therapy (MST), Multidimensional Treatment Foster Care (MTFC), or functional family therapy; specialist CAMHS; coordinated school + social care
Crisis / safeguarding / youth justice → safety first; multi-agency plan (police, social care, education); bridge to community MST on discharge
For severe and complex conduct disorder — and especially for children with callous-unemotional traits or those in the youth-justice system — the response is multimodal, intensive and long-term. Multisystemic Therapy and Multidimensional Treatment Foster Care work across the child's whole ecology (family, school, peers, community) and are designed for precisely this high-risk group; the Fast Track prevention trial demonstrated that early, sustained, multicomponent intervention can change long-term outcomes through to established adulthood. [6] [12]
Medication is not first-line for conduct disorder. The psychosocial evidence is stronger and the harms lower. Where medication is considered, it is for specific indications and usually under specialist supervision: treating comorbid ADHD with stimulant medication is often the single most effective pharmacological move, because uncontrolled ADHD both drives and maintains antisocial behaviour. Short-term risperidone has evidence for reducing aggression in children with conduct disorder or ODD and intellectual disability (IQ below about 70), but it is a specialist, time-limited decision with attention to weight gain, metabolic effects and sedation — never a substitute for the parenting and multimodal plan. [6] [10]
Specific Subtypes & Scenarios
Childhood-onset conduct disorder with callous-unemotional traits is the highest-risk, most treatment-resistant form: premeditated aggression, low empathy, and a strong association with the life-course-persistent trajectory and adult antisocial outcome. It needs specialist, multimodal, intensive and long-term care, with close risk management — and the family needs an honest, compassionate framing of severity without fatalism, because even this group can improve with sustained intervention. [1] [4]
Adolescence-onset conduct disorder is commoner and more hopeful: the behaviour is driven by peer influence and developmental context against a more normal temperament, and it usually desists as maturity and adult roles arrive. The task is to keep the young person safe, engaged in school, and connected to prosocial relationships through the window of risk, while addressing substance use, family conflict, and any comorbidity. [1] [8]
Conduct disorder with comorbid ADHD should have the ADHD treated effectively first or in parallel, because untreated ADHD sabotages every other intervention; this is one of the clearest evidence-based levers in the field. Conduct disorder following trauma or in out-of-home care must be managed with trauma-informed care — behaviour plans that ignore the abuse, neglect, or instability that drive the behaviour will fail and may retraumatise, and stability of placement and relationships is itself treatment. [4] [8]
Conduct disorder in the youth-justice system demands a developmental and trauma-informed lens: screen for unmet neurodevelopmental need, speech and language disorder, acquired brain injury, and mental illness, all of which are over-represented and under-recognised, and bridge the young person into community multimodal care on release rather than abandoning the work at the gate. [2] [12]
Complications & Pitfalls
The harms of conduct disorder are real, measurable, and extend far beyond childhood. Untreated or undertreated conduct disorder carries elevated rates of school failure and dropout, substance use, mental illness, unemployment, broken relationships, imprisonment, and the progression to adult antisocial personality — and Scott's long-term follow-up found that the children with persistent antisocial behaviour went on to cost society roughly ten times more than their comparison peers across health, social, and criminal-justice services. [2] [8]
Scott et al., BMJ 2001
Key finding
Follow-up of children with antisocial behaviour into adulthood showed roughly ten-fold higher costs in crime, health and social services than comparison children \u2014 the economic case for early, evidence-based intervention.
The complications of treatment are smaller but real and must be discussed openly. Risperidone, when used, carries weight gain, metabolic effects and sedation, and must be monitored; stimulant treatment of comorbid ADHD needs attention to appetite, sleep and growth. The single largest pitfall is undertreatment driven by therapeutic nihilism — the false belief that conduct disorder is untreatable — which the evidence directly contradicts: parenting programmes and multimodal therapies work, and work best when delivered early. [5] [9]
The other classic errors are labelling rather than assessing (calling a traumatised child "conduct disordered" and missing the abuse), missing comorbid ADHD, prescribing medication in place of a parenting plan, and failing to engage the school and social-care system that surrounds the child. Each of these converts a treatable problem into a chronic one. [4] [10]
Prognosis & Disposition
The prognosis divides sharply along the developmental taxonomy. The life-course-persistent form — childhood-onset, with CU traits and heavy adversity — has the poorest outcome, with persistence into adult antisocial behaviour, substance use and imprisonment in a substantial minority; the adolescence-limited form usually desists as maturity and adult roles arrive, leaving a far better prognosis. The predictors of poor outcome are early onset, callous-unemotional traits, comorbidity, family adversity and conflict, school failure and exclusion, and a deviant peer group. [1] [8]
The Kim-Cohen follow-back study reinforced why early conduct problems matter across the life course: adult mental disorder is strongly foreshadowed by juvenile diagnoses, with conduct problems among the most predictive of adult antisocial and substance-use outcomes, so what looks like a childhood behaviour problem is often the first chapter of an adult trajectory the clinician can still change. [8]
Disposition is layered: mild problems are managed in primary care and the community with a parenting programme and a clear review date; moderate problems in community CAMHS with structured parent training and child skills work; severe, complex, or callous-unemotional presentations in specialist CAMHS with multimodal therapy such as MST or MTFC; and acute crisis, safeguarding concern, or comorbid psychiatric emergency in an inpatient or intensive community setting. A relapse-prevention and transition plan — early-warning signs, the intervention that worked, the adults who held the plan, and how to restart care — should be written with the family before any discharge. [4] [12]
Special Populations
Looked-after children and those in out-of-home care carry the highest rates of conduct problems because adversity, abuse and instability are their cause as much as their correlate; stability of placement, security of relationships, and trauma-informed care are themselves treatment, and a behaviour plan delivered into a chronically unstable home will fail. Young people in the youth-justice system need a developmental, trauma-informed and culturally responsive assessment — unmet neurodevelopmental need, speech and language disorder, acquired brain injury, and mental illness are over-represented and under-recognised. [2] [8]
Indigenous children — Aboriginal and Torres Strait Islander, Māori, and First Nations young people — carry the additional weight of intergenerational trauma, racism, socio-economic disadvantage, and often culturally unsafe services; engagement and outcome are improved by Indigenous-led, culturally responsive, community-based models of care rather than services imposed from outside. Children in socioeconomically disadvantaged families and rural and remote communities face thin access to evidence-based parenting programmes and specialist CAMHS, so school-based, telehealth-delivered and locally-supported interventions matter disproportionately. [4] [3]
Pre-school children are the population in which prevention pays the largest dividend: the Fast Track programme and the Incredible Years and Triple P trials all show that intervening early, when the coercion loop is still forming and plasticity is greatest, changes the trajectory that is far harder to shift in adolescence. [5] [12]
Evidence, Guidelines & Regional Differences
The disorder is global, but the service models, the parenting programmes that are funded, and the role of medication are regional. Name the guideline you are quoting and carry the differences explicitly. [4] [5]
United Kingdom / NICE (CG158) provides the most explicit stepped-care framework: child-focused programmes and group parenting programmes for those at risk or with mild problems, structured parent-training programmes for moderate-to-severe conduct disorder, and multimodal intervention (MST, MTFC) for severe and complex cases, with medication reserved for specific indications. Australia and New Zealand follow a similar evidence base and increasingly deliver Incredible Years and Triple P through primary care, schools and Aboriginal community-controlled services, with culturally adapted variants for Indigenous families. North America (AAP, AACAP) emphasises PCIT for younger children and MST/MTFC for severe adolescent conduct disorder, and treats comorbid ADHD vigorously. [5] [6] [9]
The strongest, most consistent evidence is for behavioural and cognitive-behavioural parenting programmes delivered in early childhood — the Furlong Cochrane review, the Sanders Triple P trials, the Eyberg evidence update, and the Dretzke economic evaluation all converge on this. The Fast Track prevention trial and its long-term follow-up demonstrate that sustained, multicomponent early intervention can change outcomes into established adulthood, which is the most powerful argument for investment in prevention. Where the evidence is weaker is in the pharmacotherapy of conduct disorder itself: outside comorbid ADHD and short-term risperidone for aggression in intellectual disability, drug treatment is not evidence-supported as a primary strategy. [5] [7] [12]
Exam Pearls
The high-yield facts examiners reward: the Moffitt taxonomy (life-course-persistent versus adolescence-limited) is the single most quotable framework; childhood-onset plus callous-unemotional traits is the worst prognosis and the one that needs specialist multimodal care; ADHD is the commonest comorbidity and treating it is one of the most effective interventions; parenting programmes are first-line and medication is not; risperidone is short-term, specialist, and mainly for aggression with intellectual disability; and the Fast Track trial is the landmark evidence that early prevention works into adulthood. [1] [5] [12]
The classic errors: calling a traumatised child "conduct disordered" and missing the abuse; missing comorbid ADHD; prescribing in place of a parenting plan; and under-treating because of therapeutic nihilism. The corrective in every case is to assess the ecology, treat the comorbidity, and deliver an evidence-based, stepped, family-centred plan — and to intervene early, where the leverage is greatest. [4] [10]
References
- [1]Moffitt TE Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychol Rev, 1993.PMID 8255953
- [2]Scott S, Knapp M, Henderson J, Maughan B Financial cost of social exclusion: follow up study of antisocial children into adulthood. BMJ, 2001.PMID 11473907
- [3]Erskine HE, Ferrari AJ, Nelson P, et al. The global burden of conduct disorder and attention-deficit/hyperactivity disorder in 2010. J Child Psychol Psychiatry, 2014.PMID 24447211
- [4]Burke JD, Loeber R, Birmaher B Oppositional defiant disorder and conduct disorder: a review of the past 10 years, part II. J Am Acad Child Adolesc Psychiatry, 2002.PMID 12410070
- [5]Furlong M, McGilloway S, Bywater T, et al. Behavioural and cognitive-behavioural group-based parenting programmes for early-onset conduct problems in children aged 3 to 12 years. Cochrane Database Syst Rev, 2012.PMID 22336837
- [6]Eyberg SM, Nelson MM, Boggs SR Evidence-based psychosocial treatments for children and adolescents with disruptive behavior. J Clin Child Adolesc Psychol, 2008.PMID 18444059
- [7]Sanders MR, Markie-Dadds C, Tully LA, Bor W The triple P-positive parenting program: a comparison of enhanced, standard, and self-directed behavioral family intervention for parents of children with early onset conduct problems. J Consult Clin Psychol, 2000.PMID 10965638
- [8]Kim-Cohen J, Caspi A, Moffitt TE, et al. Prior juvenile diagnoses in adults with mental disorder: developmental follow-back of a prospective-longitudinal cohort. Arch Gen Psychiatry, 2003.PMID 12860775
- [9]Dretzke J, Davenport C, Frew E, et al. The effectiveness and cost-effectiveness of parent training/education programmes for the treatment of conduct disorder, including oppositional defiant disorder, in children. Health Technol Assess, 2005.PMID 16336845
- [10]Kazdin AE Treatments for aggressive and antisocial children. Child Adolesc Psychiatr Clin N Am, 2000.PMID 11005009
- [11]Conduct Problems Prevention Research Group Kindergarten conduct problems are associated with monetized outcomes in adolescence and adulthood. J Child Psychol Psychiatry, 2024.PMID 37257941
- [12]Conduct Problems Prevention Research Group Fast Track Intervention Effects and Mechanisms of Action Through Established Adulthood. Prev Sci, 2025.PMID 39392546