Paeds · mental-behavioural-and-psychosomatic
Obsessive-compulsive disorder in children
Also known as OCD · Obsessive compulsive disorder · Paediatric OCD · Childhood-onset OCD · Obsessive-compulsive disorder
Fellowship guide to paediatric OCD: recognising the hidden obsession–compulsion cycle, multi-informant clinical diagnosis with CY-BOCS, differentials including autism, tics and anxiety, stepped CBT-with-ERP-first care with SSRI escalation, PANDAS/PANS controversy, family accommodation, regional pathway differences and exam pearls.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the eight-year-old who is late every morning because her shoelaces "do not feel right" until she reties them forty times, or the teenager who washes his hands until they bleed because a thought about germs will not leave him alone. These are not quirks or bad habits — they are the obsession–compulsion cycle that defines OCD, and children will often hide them for a long time before anyone asks the right question. [22] [17]
OCD in children is a common, treatable anxiety-spectrum disorder. Intrusive, unwanted thoughts, images or urges (obsessions) generate intense distress, and the child performs repetitive behaviours or mental acts (compulsions) to reduce that distress. The relief is brief, so the cycle repeats — often for more than an hour a day and across home, school and social life. The diagnosis is clinical, and the impairment is real even when the child looks "fine" in a brief clinic visit. [22] [9]
The single most important clinical habit is to ask directly. Children rarely volunteer their obsessions because they fear being judged or because they believe the thoughts are "crazy". A routine question — "Do you have any thoughts that bother you and keep coming back even when you don't want them?" — is the gateway that turns a hidden, disabling illness into a treatable one. [17] [22]
Classification
OCD is classified by the content of obsessions and compulsions and by severity and insight, not by separate disease subtypes. Common childhood themes include contamination with washing/cleaning, symmetry and exactness with ordering/repeating, doubt with checking, and forbidden or aggressive thoughts with mental rituals or reassurance-seeking. These themes overlap and shift over time, so a child rarely fits a single tidy box. [22] [17]
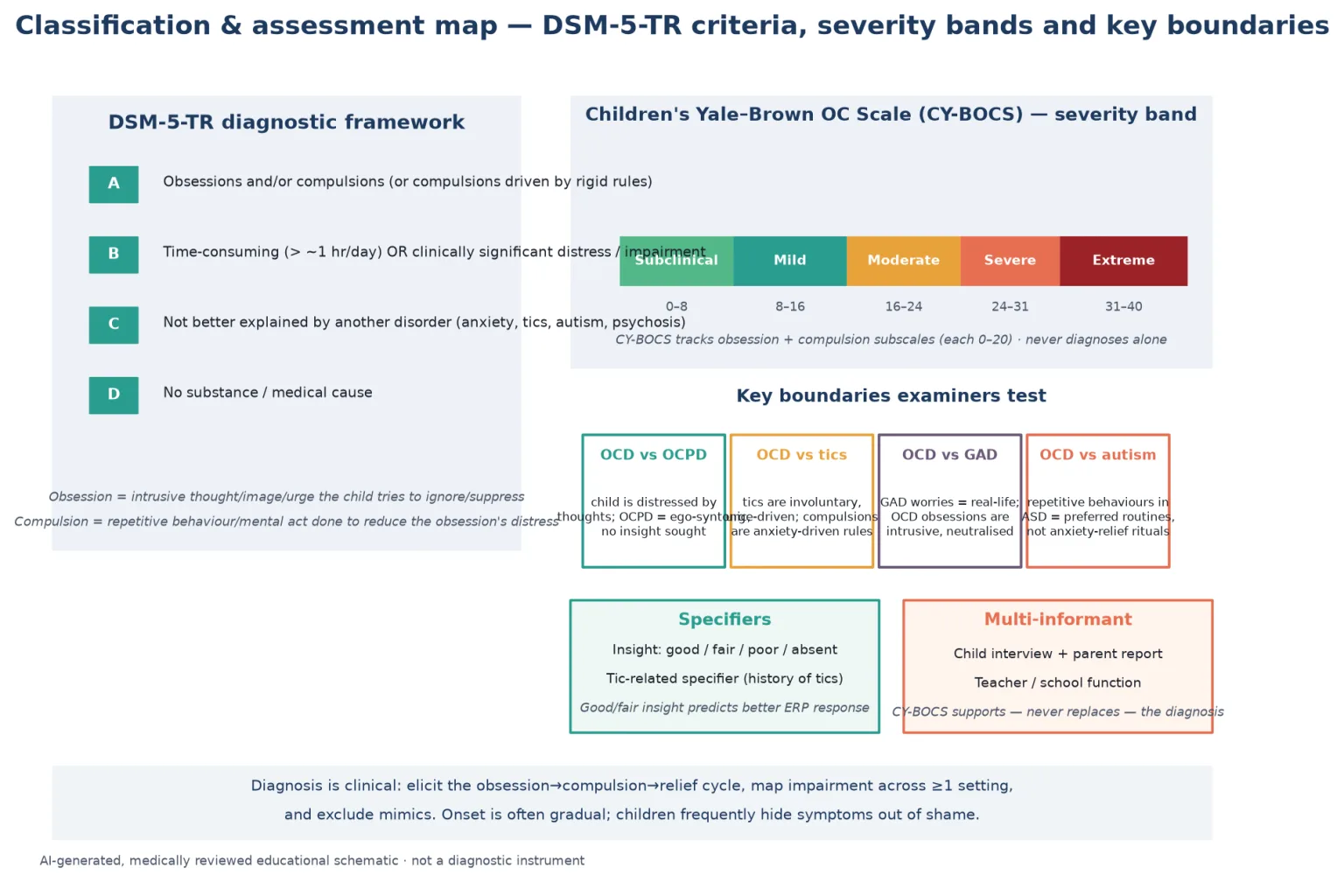
Diagnostic criteria framework (exam-level DSM-5-TR style). Criterion A requires obsessions and/or compulsions. Criterion B requires that they are time-consuming (more than about one hour per day) or cause clinically significant distress or impairment. Criterion C excludes better explanations such as another mental disorder, and Criterion D excludes a substance or medical cause. ICD-11 frames obsessive-compulsive disorder similarly and places it within an obsessive-compulsive and related disorders grouping that also covers body dysmorphic disorder, hoarding and hair-pulling. [22]
Contamination
Washing / cleaning
- Germ or dirt fears drive long handwashing
- Avoidance of toilets, doorknobs, shared items
- Skin breakdown from washing is a clue
- Often the most visible in clinic
Symmetry / exactness
Ordering / repeating
- Things must feel 'just right'
- Repeating actions until perfect
- Common in younger school-age children
- Drives lateness and task non-completion
Doubt / checking
Reassurance-seeking
- Did I lock the door? Hurt someone?
- Endless checking and asking
- Sleep severely disrupted
- Family drawn into the checking
Forbidden thoughts
Mental rituals
- Aggressive, sexual or religious intrusions
- Child may hide these most
- Counting, praying, neutralising silently
- High shame; ask gently and privately
Insight specifiers matter for treatment. A child may have good, fair, poor or absent/delusional insight into the irrationality of their obsessions. Good or fair insight predicts a stronger response to exposure-based therapy, while poor or absent insight raises the need to reconsider the diagnosis and to lean more on medication and family-supported treatment. The tic-related specifier flags children with a personal or family history of tics, who often have more symmetry/exactness symptoms and a different pharmacotherapy profile. [22] [17]
Epidemiology & Risk Factors
Childhood OCD is far more common than trainees expect. Community and epidemiological work places the point prevalence in children and adolescents around 1–3%, with a bimodal age of onset — one peak in prepubertal children (more often boys, more often with a family history or tic-related features) and a larger peak in adolescence. Early adolescent epidemiological study established OCD as one of the more prevalent anxiety-spectrum disorders of youth, not a rare curiosity. [9] [18]
Headline numbers for viva
Heritability is substantial. A family history of OCD, tics or anxiety disorder raises a child's risk, and twin studies support a strong genetic contribution alongside environmental and developmental modifiers. Prenatal and perinatal complications, streptococcal infection triggers (in a defined subgroup), psychosocial stress and trauma can influence onset or severity without being the sole cause. [17] [10]
Under-recognition and delayed treatment are the real public health problems here. Children hide symptoms, families accommodate them to keep the peace, and clinicians do not always ask — so the mean time from onset to effective treatment is measured in years. That delay worsens impairment, family conflict and school function, which is why direct, routine screening matters more than elaborate referral pathways. [17] [14]
Pathophysiology
You do not need a molecular monologue in clinic. You do need a working model that explains the symptoms and justifies the two treatment pillars. The most useful teaching model is the cortico-striato-thalamo-cortical (CSTC) circuit: hyperactivity or imbalance in loops connecting the orbitofrontal cortex, anterior cingulate, striatum (caudate) and thalamus is linked to the "sticking" of intrusive thoughts, over-detection of threat and persistence of rituals despite their irrationality. [17] [22]
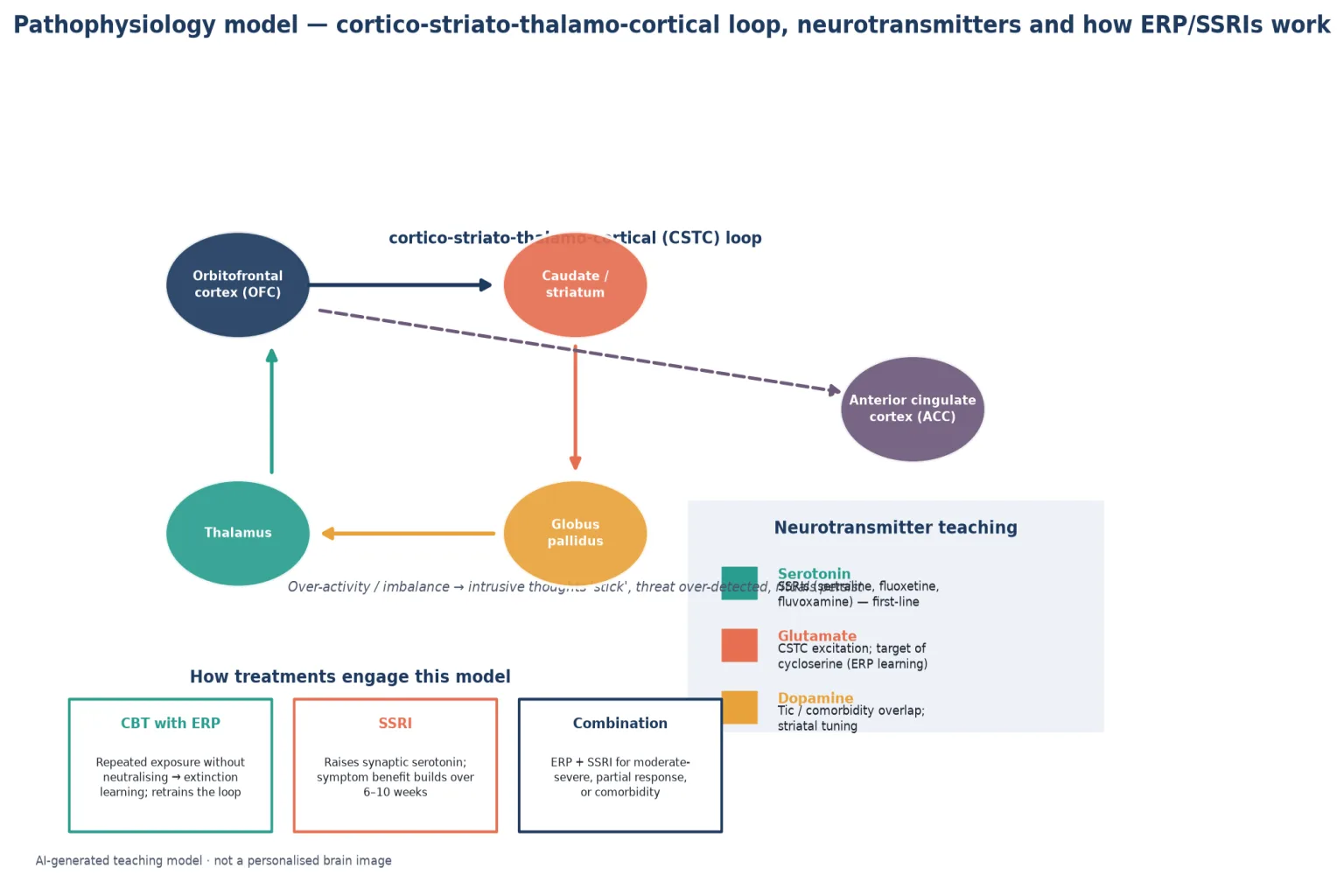
The neurotransmitter bridge to drug classes is serotonin: SSRIs (sertraline, fluoxetine, fluvoxamine) raise synaptic serotonin and reduce symptom severity over weeks, which is why benefit builds rather than arriving on day one. Glutamate signalling within the CSTC loop is increasingly important for understanding augmentation strategies such as D-cycloserine, which aims to enhance the extinction learning that exposure therapy depends on. Dopaminergic pathways explain some of the overlap with tic disorders. [4] [21]
Crucially, exposure and response prevention (ERP) retrains the circuit. By repeatedly confronting the fear-trigger without performing the neutralising ritual, the child learns that anxiety falls on its own and the feared catastrophe does not occur — a process of extinction learning that is the active ingredient of CBT. This is why ERP, not generic counselling or relaxation, is the evidence-first psychological treatment. [1] [3] [14]
Clinical Presentation
Children rarely present saying "I have obsessions". They present with the consequences of the cycle: school lateness, unfinished work, family arguments over "weird rules", bedtime that takes three hours, skin breakdown from washing, or a sudden drop in mood. The job is to recognise the obsession–compulsion pattern underneath the presenting complaint. [17] [22]
Younger children (preschool and early school-age). Presentations skew toward contamination, symmetry and "just right" feelings, often with magical thinking ("if I don't tap the wall, Mum will die"). Compulsions may look like play or habit at first, but the distress when interrupted is severe. Children may involve parents in rituals ("say it again, properly") and tantrum when the routine is disrupted. [17] [22]
School-age children. Washing, checking, repeating, re-reading and re-ordering dominate, and the academic cost becomes obvious — homework takes hours, tasks are unfinished, concentration is consumed by suppressing intrusive thoughts. Shame and secrecy grow, so the child may under-report. Teachers often notice concentration loss and avoidance before anyone names OCD. [17] [22]
Adolescents. Forbidden-thought content (aggressive, sexual, religious obsessions) becomes more prominent and is most likely to be hidden. Depression, self-harm and substance use can complicate the picture, and insight may fluctuate. Partial remission of childhood symptoms can still leave major functional impairment in study, friendships and family life. [15] [17]
| Presentation story | Do not stop here | Must still map |
|---|---|---|
| 'He is just very tidy' | Tidiness is preference; OCD is distress-driven and impairing | Time spent, distress if interrupted, functional cost |
| 'She washes a lot' | Handwashing alone is not diagnostic | Duration, skin condition, avoidance, contamination fear |
| 'Bad behaviour / tantrums' | Tantrums may be ritual-disruption distress | Trigger pattern, family accommodation, cycle |
| 'Depressed and withdrawn' | Depression may be secondary to hidden OCD | Screen obsessions directly and privately |
| 'Fussy eater' | Food refusal may hide contamination fears | Weight, avoidance pattern, fear content |
Differential Diagnosis
Build the differential in four piles: what looks like OCD but is something else, what coexists with OCD, what is dangerous to miss, and what is normal childhood behaviour. Normal childhood rituals — bedtime routines, superstitions, lining up toys — are common, time-limited, enjoyed rather than feared, and do not cause impairment. They do not need treatment. [17] [22]
Reversible mimics
- Normal developmental rituals (enjoyed, not impairing)
- Anxiety-driven avoidance without a neutralising ritual
- Medication or substance effects
- Recent stressor or trauma reaction
Common co-travellers
- Other anxiety disorders (GAD, separation, social)
- Tic disorders / Tourette syndrome
- ADHD and specific learning disorders
- Depression; autism spectrum disorder
Can't-miss alternatives
- Autism preferred routines vs OCD anxiety-rituals
- Primary psychotic disorder (delusions vs obsessions)
- PANDAS / PANS acute-onset subgroup
- Acquired basal-ganglia lesion (encephalitis, stroke)
The trickiest boundary is OCD versus the restricted, repetitive behaviours of autism. In autism, routines and sameness behaviours are usually preferred, enjoyable or self-regulating — the child gets upset when interrupted but is not driven by an intrusive fear. In OCD, the ritual is ego-dystonic, anxiety-driven and performed to neutralise a distressing obsession, and the child often wants to stop but cannot. Both can coexist, which is common, so ask what happens if you gently block the behaviour: an autism-driven routine produces dysregulation, while an OCD ritual produces mounting anxiety that the child describes as fear. [17] [22]
Tic disorders also overlap. Tics are sudden, brief, involuntary and preceded by a premonitory urge; compulsions are purposeful, rule-bound and aimed at reducing an obsession. A child can have both — the tic-related OCD specifier flags this group, who often have more symmetry/exactness symptoms and may respond preferentially to certain medications. [17] [22]
PANDAS/PANS describes a subgroup with dramatic, acute-onset OCD and/or eating restriction, often with accompanying urinary frequency, choreiform movements, anxiety and developmental regression. Whether streptococcal autoimmunity is a true, separable entity remains debated; the practical message is to recognise acute explosive onset, exclude other causes, and refer for specialist evaluation rather than treating with antibiotics or immunotherapy in routine general paediatric practice. [10] [11]
Clinical & Bedside Assessment
Structure every assessment the same way so you do not skip the cycle, the impairment or the comorbidity screen under time pressure. The history is the diagnosis — there is no confirmatory test. [22] [20]
Bedside OCD assessment sequence
Child and young person voice first
Ask about thoughts that 'keep coming back', secret worries, rituals and what happens if they are interrupted. Give private, stigma-free space.
Map the obsession–compulsion cycle
Elicit each obsession, the compulsion it drives, time per day, situational triggers and whether rituals involve family members.
Multi-setting impairment
Home, school, friendships, sleep, eating, bathing and family conflict. Gather teacher information where possible.
Comorbidity and red-flag screen
Anxiety, tics, ADHD, depression, autism traits, self-harm, suicidality, safeguarding and acute-onset neurological features.
Examination and severity baseline
Skin (washing injury), growth and weight (food avoidance), focused mental state, and CY-BOCS rating for severity tracking.
Synthesis and shared plan
Name OCD, explain the cycle, agree stepped ERP-based care, involve family in reducing (not feeding) accommodation, and set a review date.
CY-BOCS supports; it does not diagnose. The Children's Yale-Brown Obsessive Compulsive Scale quantifies severity across obsession and compulsion subscales (each scored 0–20), tracks response over time, and helps distinguish mild from moderate-to-severe illness for treatment stepping. A high score without the clinical cycle and impairment is a severity rating, not a diagnosis. Use it to measure change, not to replace the clinical interview. [20] [22]
Always ask about family accommodation — the ways parents modify their own behaviour to prevent or reduce the child's distress (providing reassurance, participating in rituals, avoiding triggers). Accommodation is well-intentioned but maintains the cycle and predicts poorer response, so it is both a clinical target and a family-engagement opportunity, not a failing to be judged. [14] [22]
Investigations
There is no diagnostic blood test, EEG or MRI for uncomplicated OCD. Investigations exist to exclude mimics, assess medical compromise from compulsions, and screen for medication safety. [22]
Consider targeted testing only when the history points there: a throat swab and anti-streptolysin-O titre when acute explosive onset suggests PANDAS/PANS (as part of specialist workup, not routine); neuroimaging when there are focal neurological signs, cognitive decline, seizures or an atypical acute presentation; and weight, BMI and skin assessment when contamination fears or food avoidance drive medical compromise. Before starting an SSRI, take a baseline weight, screen for bipolar symptoms (a personal or family history of mania), and document suicidal ideation — because SSRIs carry a youth suicidality warning that shapes monitoring, not because a blood test is required. [5] [22]
Management — Resuscitation
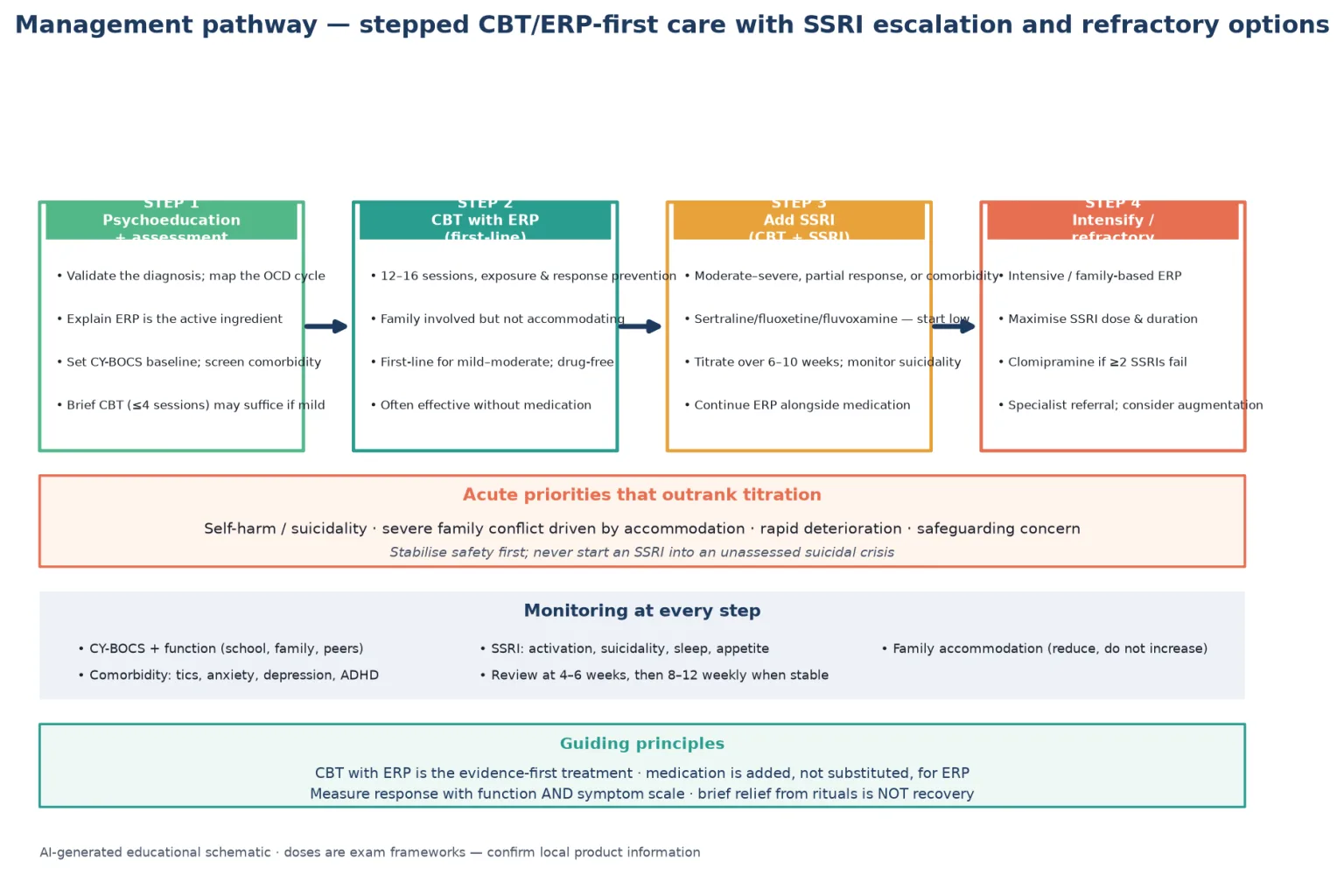
OCD itself is rarely the emergency, but several situations outrank titration. Acute suicidal crisis, severe self-harm from compulsions (e.g. caustic skin injury), food and fluid avoidance causing medical compromise, family violence driven by accommodation demands, and rapid deterioration with neurological features all require stabilisation before stepping OCD treatment. Do not start an SSRI into an unassessed suicidal or possibly bipolar landscape. [5] [22]
Management — Definitive & Stepwise
Match intensity to severity. Every family needs psychoeducation: OCD is a real, treatable anxiety-spectrum condition, the child is not "naughty", and the goal is to break the cycle rather than to feed it with accommodation. The evidence base consistently shows that cognitive–behavioural therapy with exposure and response prevention (CBT/ERP) is first-line, with SSRIs added for moderate-to-severe, partially responsive, or comorbid presentations. [22] [1] [3]
The stepped ladder
Step 1 — Psychoeducation and assessment. Validate the diagnosis, map the cycle, explain that ERP is the active ingredient, set a CY-BOCS baseline and screen comorbidity. For genuinely mild OCD, brief CBT (around four sessions) may be sufficient. [14] [22]
Step 2 — CBT with ERP (first-line). A full course of roughly 12–16 sessions of exposure and response prevention is first-line for mild-to-moderate paediatric OCD and is often effective without medication. Family is involved to reduce accommodation, not to enforce rituals. Meta-analytic evidence supports CBT as the strongest single intervention for paediatric OCD. [1] [3] [12]
Step 3 — Add an SSRI (CBT + SSRI). Combine ERP with an SSRI for moderate-to-severe illness, partial response to ERP alone, or significant comorbidity (depression, severe anxiety). Sertraline, fluoxetine and fluvoxamine all have paediatric OCD evidence; start low, titrate over 6–10 weeks toward an adequate dose, and monitor for activation, sleep disturbance and suicidality. The original POTS trial showed combination treatment was superior for some outcomes, and POTS II showed CBT augmentation of an SSRI improves outcomes over SSRI alone. [1] [2] [4] [7]
Step 4 — Intensify / refractory. For non-response after an adequate ERP course and at least two SSRI trials, escalate to intensive or family-based ERP, maximise SSRI dose and duration, consider clomipramine (a tricyclic with the strongest early paediatric evidence but a heavier side-effect profile), and refer to a specialist OCD service. Follow-up of initial CBT non-responders shows continued CBT and SSRI both help, so do not abandon ERP at the first failure. [8] [16] [22]
SSRIs — exam frameworks
| Agent | Typical exam framework | Key teaching points |
|---|---|---|
| Sertraline | Start low, titrate weekly toward response; paediatric OCD licensed in many jurisdictions | First SSRI with a paediatric OCD RCT (March 1998); monitor activation and suicidality [4] [5] |
| Fluoxetine | Start low, titrate toward response; also has paediatric OCD RCT evidence | Long half-life useful for missed doses; also approved for paediatric depression [6] |
| Fluvoxamine | Paediatric OCD evidence; titrate as tolerated | Useful alternative; gastrointestinal effects common [7] |
| Clomipramine | Tricyclic; ECG and cardiac monitoring; reserved for refractory | Strong early evidence (DeVeaugh-Geiss 1992) but heavier side-effect and overdose risk [8] |
The 2024 Pediatrics meta-analysis confirms that both pharmacotherapy and CBT outperform placebo, and combination treatment generally offers the best overall outcomes for moderate-to-severe paediatric OCD — but CBT/ERP is the most effective single component and should not be skipped. [19]
Monitoring schedule
At baseline and follow-up track CY-BOCS, functional impact (school, family, peers), family accommodation, comorbidity (tics, anxiety, depression, ADHD), and — for SSRIs — activation, sleep, appetite, weight and suicidality, especially in the first weeks and after dose changes. Review at 4–6 weeks after starting or changing treatment, then space visits to 8–12 weekly when stable. [5] [22]
Australian and New Zealand practice uses stepped care with GP mental health treatment plans and Better Access referrals for CBT, and specialist child and adolescent mental health services for moderate-to-severe or refractory OCD. SSRI initiation in children is usually a specialist or shared-care decision. Access to ERP-trained therapists is uneven, especially in rural and remote areas, so telehealth-delivered CBT is an emerging evidence-supported option. [14] [12]
Specific Subtypes & Scenarios
Mild OCD with good insight. Brief CBT or guided self-help with ERP may suffice; medication is usually unnecessary. Measure function, not just the scale score. [14] [22]
Moderate-to-severe OCD. Combine full CBT/ERP with an SSRI; the original POTS combination data and POTS II augmentation data support this. Reduce family accommodation as an explicit treatment target. [1] [2]
OCD with comorbid autism. Adapt ERP pacing, use visual supports and a structured approach, and avoid diagnostic overshadowing — both can be true. Specialist CAMHS involvement is often needed. [17] [22]
OCD with tics / Tourette syndrome. The tic-related specifier applies; these children often have symmetry/exactness symptoms. Treat the OCD with ERP, and address tics in parallel if they are impairing. [17] [22]
Acute explosive onset (PANDAS/PANS). Recognise the sudden, dramatic onset of obsessions/compulsions or eating restriction with urinary frequency, choreiform movements and regression; exclude infection and neurological causes; and refer for specialist evaluation. Routine antibiotic or immunomodulatory treatment is not standard general-paediatric practice. [10] [11]
Refractory OCD after adequate ERP and two SSRIs. Maximise dose and duration, consider clomipramine, escalate to intensive or family-based ERP, and refer to a specialist OCD service. Three-year outcome data show continued treatment helps even initial non-responders. [8] [16]
Adolescent with depression and self-harm. Treat safety first, address depression alongside OCD, and choose an SSRI with explicit suicidality monitoring. Involve CAMHS early. [5] [15]
Rural, remote or language-discordant family. Use telehealth-delivered CBT where evidence supports it, work with interpreters, and ensure equitable access to ERP rather than defaulting to medication-only care for logistical convenience. [14] [12]
Complications & Pitfalls
Classic errors: missing OCD because the child hides symptoms; mistaking rituals for autism-driven routines or "naughty behaviour"; diagnosing from a scale without eliciting the cycle; starting an SSRI without screening for suicidality or bipolar risk; feeding accommodation instead of reducing it; promising a quick cure; and abandoning ERP after one non-response when continued treatment helps. [17] [22]
Family accommodation is the most common hidden maintainer. Well-meaning parents provide reassurance, participate in rituals and avoid triggers to reduce the child's distress, but this prevents extinction learning and predicts poorer outcomes. Naming it as a treatment target — gently, without blame — is part of every management plan. [14] [22]
SSRIs carry a boxed warning for suicidality in youth. The sertraline pooled-analysis data showed that the absolute risk is small and that treatment benefit in paediatric OCD is substantial, but the warning shapes monitoring: document baseline suicidality, review early and after dose changes, and involve families in observation. Untreated OCD itself carries significant suicide and depression risk, so the risk-benefit balance favours treatment when OCD is impairing. [5] [15]
PANDAS/PANS is a pitfall in both directions: missing a genuine acute-onset presentation with treatable medical factors, or over-diagnosing it and subjecting children to unproven immunomodulatory or antibiotic regimens. The balanced stance is recognise, exclude, refer. [10] [11]
Prognosis & Disposition
Paediatric OCD is often chronic but highly treatable. With evidence-based care, a substantial proportion of children achieve remission or marked improvement; without it, symptoms persist, impair and entrench. Three-year follow-up of children treated with evidence-based therapies shows meaningful remission rates but also a real relapse risk, so maintenance CBT booster sessions and early review at any relapse signal are part of good care. [15] [16]
Predictors of a harder course include earlier onset, poor insight, severe baseline symptoms, comorbidity (especially depression and tics), family accommodation and psychosocial adversity. Define response by function — school attendance, friendships, family conflict, sleep and mood — not only the CY-BOCS score, because a child can be symptom-improved but still functionally impaired. [15] [22]
Disposition ranges from primary-care or GP-shared follow-up for mild, stable OCD to specialist CAMHS or OCD services for moderate-to-severe, comorbid or refractory illness. Transition planning to adult mental health services should begin before the young person falls out of paediatric care, because OCD often persists into adulthood and continuity of ERP and medication matters. [15] [17]
Special Populations
Children with autism or intellectual disability need adapted ERP (slower pacing, visual supports, structured sessions) and careful dual diagnosis without diagnostic overshadowing. Younger children benefit from family-based and developmentally adjusted ERP rather than adult-style protocols. Girls and adolescents with hidden forbidden-thought obsessions need active case-finding through private, stigma-free direct questioning. [17] [22]
Indigenous, migrant and refugee families need culturally safe assessment, interpreter use, and equity of access to ERP — not medication-only default care driven by therapist availability or language barriers. Children in out-of-home care and those experiencing family violence have higher rates of both trauma-driven intrusive thoughts and true OCD, so demand a careful cycle and impairment assessment rather than assuming all intrusions are trauma. Rural and remote families may use telehealth-delivered CBT, which has emerging evidence, but still need reliable access to ERP-trained clinicians. [14] [12] [22]
Evidence, Guidelines & Regional Differences
POTS one-liner. The original POTS trial showed that combination CBT plus sertraline produced the highest response rates in children and adolescents with OCD, while CBT alone and sertraline alone were both effective — establishing that ERP is the evidence-first pillar and medication is added, not substituted, for it. [1]
POTS II one-liner. Augmenting sertraline with CBT improved outcomes over sertraline alone, confirming that ERP adds value even when an SSRI is already in place. [2]
Suicidality one-liner. The pooled sertraline analysis found a small absolute suicidality risk that is outweighed by substantial treatment benefit in paediatric OCD — monitor actively, but do not let the warning deny effective treatment. [5]
Exam Pearls
CYCLE
Self-test: moderate-severe paediatric OCD plan
Psychoeducation + family involvement to reduce accommodation + full course of CBT with ERP (12–16 sessions) + SSRI (sertraline or fluoxetine, start low, titrate over 6–10 weeks toward response); monitor CY-BOCS, function, family accommodation, activation and suicidality; review at 4–6 weeks then 8–12 weekly. If refractory after adequate ERP and two SSRIs: maximise dose/duration, consider clomipramine with cardiac monitoring, intensive/family-based ERP, specialist OCD referral. [1] [2] [8] [22]
References
- [1]Pediatric OCD Treatment Study (POTS) Team Cognitive-behavior therapy, sertraline, and their combination for children and adolescents with obsessive-compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial. JAMA, 2004.PMID 15507582
- [2]Franklin ME Cognitive behavior therapy augmentation of pharmacotherapy in pediatric obsessive-compulsive disorder: the Pediatric OCD Treatment Study II (POTS II) randomized controlled trial. JAMA, 2011.PMID 21934055
- [3]Watson HJ Meta-analysis of randomized, controlled treatment trials for pediatric obsessive-compulsive disorder. Journal of child psychology and psychiatry, and allied disciplines, 2008.PMID 18400058
- [4]March JS Sertraline in children and adolescents with obsessive-compulsive disorder: a multicenter randomized controlled trial. JAMA, 1998.PMID 9842950
- [5]March JS Treatment benefit and the risk of suicidality in multicenter, randomized, controlled trials of sertraline in children and adolescents. Journal of child and adolescent psychopharmacology, 2006.PMID 16553531
- [6]Geller DA Fluoxetine treatment for obsessive-compulsive disorder in children and adolescents: a placebo-controlled clinical trial. Journal of the American Academy of Child and Adolescent Psychiatry, 2001.PMID 11437015
- [7]Geller DA Which SSRI? A meta-analysis of pharmacotherapy trials in pediatric obsessive-compulsive disorder. The American journal of psychiatry, 2003.PMID 14594734
- [8]DeVeaugh-Geiss J Clomipramine hydrochloride in childhood and adolescent obsessive-compulsive disorder--a multicenter trial. Journal of the American Academy of Child and Adolescent Psychiatry, 1992.PMID 1537780
- [9]Flament MF Obsessive compulsive disorder in adolescence: an epidemiological study. Journal of the American Academy of Child and Adolescent Psychiatry, 1988.PMID 3264280
- [10]Swedo SE Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases. The American journal of psychiatry, 1998.PMID 9464208
- [11]Swedo SE The pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection (PANDAS) subgroup: separating fact from fiction. Pediatrics, 2004.PMID 15060242
- [12]O'Kearney R Benefits of cognitive-behavioural therapy for children and youth with obsessive-compulsive disorder: re-examination of the evidence. Australian and New Zealand journal of psychiatry, 2007.PMID 17464701
- [13]Farrell LJ Efficacy of D-cycloserine augmented brief intensive cognitive-behavioural therapy for paediatric obsessive-compulsive disorder: A randomised clinical trial. Depression and anxiety, 2022.PMID 35084071
- [14]Farrell LJ Closing the Gap for Children with OCD: A Staged-Care Model of Cognitive Behavioural Therapy with Exposure and Response Prevention. Clinical child and family psychology review, 2023.PMID 37405675
- [15]Ivarsson T Remission and Relapse Across Three Years in Pediatric Obsessive-Compulsive Disorder Following Evidence-Based Treatments. Journal of the American Academy of Child and Adolescent Psychiatry, 2024.PMID 38070870
- [16]Skarphedinsson G Three-Year Follow-Up of children and adolescents with OCD Who Did Not Respond to Initial Cognitive-Behavioral Therapy (CBT): Outcomes of Continued CBT vs. Sertraline. European child & adolescent psychiatry, 2026.PMID 41854760
- [17]Leonard HL Obsessive-compulsive disorder. Child and adolescent psychiatric clinics of North America, 2005.PMID 16171700
- [18]Rapoport JL Childhood obsessive-compulsive disorder in the NIMH MECA study: parent versus child identification of cases. Methods for the Epidemiology of Child and Adolescent Mental Disorders. Journal of anxiety disorders, 2000.PMID 11918090
- [19]Steele DW Treatment of Obsessive-Compulsive Disorder in Children and Youth: A Meta-Analysis. Pediatrics, 2024.PMID 39639456
- [20]Scahill L Children's Yale-Brown Obsessive Compulsive Scale: reliability and validity. Journal of the American Academy of Child and Adolescent Psychiatry, 1997.PMID 9183141
- [21]McGuire JF Advances in the treatment of pediatric obsessive-compulsive d-cycloserine with exposure and response prevention. Neuropsychiatry (London), 2012.PMID 24174993
- [22]AACAP Practice parameter for the assessment and treatment of children and adolescents with obsessive-compulsive disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 2012.PMID 22176943
- [23]AACAP Practice parameters for the assessment and treatment of children and adolescents with obsessive-compulsive disorder. AACAP. Journal of the American Academy of Child and Adolescent Psychiatry, 1998.PMID 9785727